Article Text

Abstract
Background: Endoscopic treatment for gastro-oesophageal reflux disease (GORD) is rapidly emerging, but there is a great need for randomised controlled trials to evaluate the efficacy.
Design and setting: A single-centre, double-blind, randomised, sham-controlled trial of endoscopic gastroplication by the Endocinch suturing system.
Patients and interventions: 60 patients with GORD were randomly assigned to three endoscopic gastroplications (n = 20), a sham procedure (n = 20) or observation (n = 20). The research nurse and patients in the active and sham groups were blinded to the procedure assignment. After 3 months, open-label active treatment was offered to all patients.
Outcome measures: The primary outcome measures were proton pump inhibitor (PPI) use and GORD symptoms, and secondary measures were quality of life, 24-h oesophageal acid exposure, oesophageal manometry and adverse events. Follow-up assessments were performed at 3, 6 and 12 months.
Results: At 3 months, the percentage of patients who had reduced drug use by ⩾50% was greater in the active treatment group (65%) than in the sham (25%) or observation groups (0%) (p<0.02). Symptoms (heartburn and to a lesser extent regurgitation) improved more in the active group than in the sham group. Three Short Form-20 quality of life subscales (role function, general health and bodily pain perception) improved in the active group versus sham. Oesophageal acid exposure was modestly decreased after active treatment (p<0.02), but not significantly greater than after the sham procedure (p = 0.61). The active treatment effects on PPI use, symptoms and quality of life persisted after 6 and 12 months of open-label follow-up (n = 41), but 29% of patients were retreated in this period. No serious adverse events occurred.
Conclusions: Endoscopic gastroplication, using the Endocinch device, reduced acid-inhibitory drug use, improved GORD symptoms and improved the quality of life at 3 months compared with a sham procedure. The effects persisted up to 12 months. However, the reduction in oesophageal acid exposure was not greater after endoscopic treatment than after a sham procedure.
- ANOVA, analysis of variance
- GORD, gastro-oesophageal reflux disease
- IQR, interquartile range
- LOS, lower oesophageal sphincter
- OGJ, oesophagogastric junction
- PPI, proton pump inhibitor
- SF-20, Short Form-20
Statistics from Altmetric.com
- ANOVA, analysis of variance
- GORD, gastro-oesophageal reflux disease
- IQR, interquartile range
- LOS, lower oesophageal sphincter
- OGJ, oesophagogastric junction
- PPI, proton pump inhibitor
- SF-20, Short Form-20
Gastro-oesophageal reflux disease (GORD) is a common and chronic disorder with a considerable impact on a patient’s quality of life and healthcare utilisation resources.1–5 Medical and surgical treatment methods available to date are often sufficient but also cumbersome and expensive. Proton pump inhibitors (PPIs) are a safe and effective treatment for GORD,6 but many patients are not willing to accept a lifelong use of drugs. Patients who experience persistent symptoms despite daily drug use can be offered a laparoscopic fundoplication, which has proved to be safe and efficacious,7 but in a significant subset of these patients new symptoms arise postoperatively (eg, dysphagia and bloating).8,9 For these reasons, a minimally invasive endoscopic antireflux treatment could be an appealing alternative approach.
Recently, three endoscopic antireflux techniques have been developed: radiofrequency energy, copolymer injection and suturing.10 A common goal of these different therapeutic approaches is to improve the antireflux barrier function of the oesophagogastric junction (OGJ). Endoluminal treatments are designed to be carried out in an outpatient setting. Only a few investigators have studied the effectiveness of these types of treatment in a randomised sham-controlled fashion. Corley et al11 showed that radiofrequency energy delivered to the OGJ improved GORD symptoms and quality of life when compared with a sham procedure. However, there was no reduction in oesophageal acid exposure or drug use at 6 months. Devière et al12 conducted a randomised, sham-controlled, multicentre trial on the effectiveness of non-resorbable copolymer implantation (Enteryx (Boston Scientific Corporation, Natick, MA, USA)). Active treatment reduced GORD symptoms and PPI use, but again no significant effect on oesophageal acid exposure was found.
The endoscopic antireflux procedure used in the present study is endoluminal suturing with the Bard endoscopic suturing system (Endocinch (Bard Endoscopic Technologies, CR Bard, Billerica, MA, USA)) developed by Swain and Mills,13 which it is one of the most used endoscopic antireflux devices worldwide. The aim of endoscopic suturing is to place gastroplications at or just below the OGJ to reduce the frequency and volume of reflux of gastric contents into the oesophagus. The important advantages of this technique are its reversibility and titratability. Numerous authors have reported on the safety and feasibility of the procedure.14–17 Several open-label studies have shown promising short-term and medium-term results,14–16 but there is a need for a randomised comparative trial to show its efficacy over placebo. The objective of this research was to evaluate the therapeutic efficacy of endoscopic gastroplication in GORD compared with the sham procedure.
PATIENTS AND METHODS
We conducted a single-centre, randomised, double-blind trial of endoscopic gastroplication for the treatment of GORD, comparing three groups: active gastroplication, sham gastroplication and no treatment (observation). The study was approved by the medical ethics committee of the University Medical Centre Utrecht, Utrecht, The Netherlands.
Patients
Patients with typical persistent symptoms of GORD (heartburn or regurgitation) were recruited from the outpatient clinic of the Department of Gastroenterology at the University Medical Centre Utrecht (Utrecht, The Netherlands) and by an advertisement in a local newspaper.
All patients were at least partially responsive to PPI drugs and had been dependent on PPIs for at least 1 year. They were considered for non-medical treatment because of their unwillingness to take drugs lifelong, because of inadequate responsiveness to medical treatment, or because they experienced side effects due to drugs. Patients were included only when oesophageal pH results were compatible with the diagnosis of GORD—that is, oesophageal pH <4 >5% of the time or a symptom association probability >95%.18 Patients <18 years of age, with severe oesophageal motility disorder on manometry, hiatus hernia >3 cm in length, a history of thoracic or gastric surgery, reflux oesophagitis grade C or D (LA classification), Barrett’s epithelium, other severe comorbidities (including cardiopulmonary disease, portal hypertension, collagen diseases, morbid obesity and coagulation disorders), use of anticoagulant or immunosuppressive drugs, or a history of alcohol or drug misuse were excluded.
Patient assessment at baseline
To assess eligibility, patients underwent an upper endoscopy if not already performed in the past 2 years. Baseline values of the daily dose of PPI needed to achieve optimal symptom control were recorded for each patient during a run-in period of 1 month. During the last week of this period, patients discontinued acid-suppressive drugs and underwent stationary oesophageal manometry and 24-h ambulatory pH monitoring if not already performed in the past year. Questionnaires on GORD symptoms and quality of life assessments before treatment were also completed off medication.
Randomisation
After having obtained written informed consent, patients were randomly allocated to one of three groups: active treatment, sham treatment or no treatment (observation). The observation group was added to enable assessment of the magnitude of placebo effect of the sham procedure. Treatment status was assigned by using block randomisation. For each patient, a numbered envelope was drawn from a set of sealed envelopes containing the allocation on a card. The assignment was recorded in a computer database by an independent staff member. Shortly before each intervention the endoscopist was informed about the patient’s group assignment. Subsequent contact between the patient and the endoscopist was minimised. Patients randomised to active or sham treatment were blinded with regard to their assignments. A research nurse, blinded to the treatment assignments, contacted the patients and carried out subsequent outcome assessments.
Intervention
Endoscopic suturing was carried out to create a preset number of three gastroplications in all patients in the active treatment group. All procedures, both active and sham, were carried out by one and the same endoscopist (MPS). As described previously,14 the procedure was carried out using two video gastroscopes (type Olympus GIF-160 (Olympus Nederland BV, Zeeterwoude, The Netherlands)) and the endoscopic suturing device (Endocinch). After endoscopic placement of an oesophageal overtube, two stitches were placed adjacent to one other, using the same thread. The first gastroplication was positioned about 1.5–2 cm below the squamocolumnar line along the lesser curvature. The second endoscope was used to create the gastroplication by tightly pulling the sutures together and placing a suture anchor. A second gastroplication was placed 1 cm above the first, and a third gastroplication was placed at the level of the second along the greater curvature.
The sham procedure was carried out using the same equipment, but without the suturing needle and thread loaded. The endoscopist and two trained nurses carried out the same treatment routine as during active treatment for a duration of 40 min, including placement of an overtube, but no mucosal tissue was grasped or stitched. All procedures were carried out under deep sedation, with a combination of midazolam and pethidine administered intravenously. Oxygen saturation was monitored continuously during the procedure. After the procedure, patients were observed for a period of 4 h in the outpatient clinic. Blood pressure and heart rate were measured hourly. Before their departure, patients were seen by the research nurse, who was blinded to the type of treatment, to obtain general information on the recording and reporting of adverse events, the use of drugs and food intake. Patients assigned to the observation group received no interventional treatment.
Objectives
The hypotheses tested in this study were that active treatment would:
1. decrease the use of antisecretory drug;
2. decrease GORD symptoms;
3. improve quality of life; and
4. reduce oesophageal acid exposure.
Follow-up
Patients in the active and sham treatment groups were instructed to discontinue PPI drugs from day 5 after having undergone treatment. Patients in the observation group were off drugs as they had undergone pH monitoring. If symptoms returned, PPI treatment (maintenance or on demand) was restarted without consulting a doctor. Patients were free to increase or reduce the daily PPI dose as desired, depending on their GORD symptoms. Use of other antacids was discouraged. Drug use was recorded daily. One month after treatment, the research nurse contacted each patient by telephone to enquire about PPI consumption, present symptoms and the occurrence of adverse events (ie, sore throat, dysphagia, retrosternal pain and nausea).
After 3 months, GORD symptoms and quality of life questionnaires were completed, 1 week off drugs in all groups, and oesophageal manometry and ambulatory 24-h pH monitoring were repeated in the active and sham groups. Subsequently, patients were unblinded with regard to the treatment they had received. The number of patients responding to treatment was assessed, response being defined as a ⩾50% reduction in the use of PPIs. Patients from the sham and observation groups were offered open-label active treatment. In case of treatment failure in the active treatment group the patient was offered a repeat endoscopic treatment, consisting of the addition of one or more gastroplications. Follow-up was continued for up to 12 months after the gastroplication procedure.
Outcome measures
The primary end point at 1, 3, 6 and 12 months was the use of antisecretory drugs (daily PPI dose) and those at 3, 6 and 12 months were the symptom scores for heartburn and regurgitation. Symptoms were scored according to a 6-point scale measuring frequency (>5 times daily, 2–5 times daily, once daily, once weekly, once monthly or <1 monthly) and a 4-point scale measuring severity (not, mildly, moderately and very severe).8 GORD symptom scores were calculated by multiplying frequency and severity scores.
Secondary end points at 3 and 12 months were quality of life scores, and those at 3 months were oesophageal acid exposure characteristics (using 24-h pH monitoring) and lower oesophageal sphincter (LOS) pressure. The occurrence of adverse events was assessed at 1 month. Quality of life assessments were carried out using the 20-item Short-Form Health Survey (SF-20), which comprises six dimensions of quality of life: physical function, role function, social function, mental health, general health and bodily pain perception. After transformation of each individual scale to a 100-point scale, 0 represents the worst score and 100 the best. In bodily pain perception, however, a higher score is negative: the patient encounters more pain.
Oesophageal manometry and ambulatory pH monitoring
Manometry was carried out using a water-perfused catheter with a sleeve sensor (Dentsleeve, Mui Scientific, Ontario, Canada) connected to a pneumohydraulic perfusion pump. The catheter was passed transnasally into the stomach and the sleeve sensor was positioned at the central point of the lower oesophageal sphincter. Intraluminal oesophageal pressures were recorded at 5, 10 and 15 cm above the upper margin of the LOS. The manometric response to 10 standardised wet swallows was recorded. The residual pressure of the LOS during relaxations in response to wet swallows was measured. For pH monitoring, a pH glass electrode catheter was introduced into the oesophagus and positioned 5 cm above the upper margin of the LOS, determined during manometry. Data were stored in a digital data logger, using a sampling rate of 0.2 Hz. The intraoesophageal pH was measured for 24 h. Manometry and pH data were interpreted by independent (blinded) staff members.
Sample size
Power calculations before the study were aimed to detect the primary outcomes. Calculations were based on uncontrolled data gathered from previous studies.14,16 It was estimated that 54 patients had to be included (α = 0.05, β = 0.20), assuming that 70% in the treatment group, 20% in the placebo group and 0% in the observation group would respond (ie, ⩾50% improvement compared with baseline values). Six additional patients were enrolled to allow for dropouts.
Statistical analysis
Analyses were performed according to the intention-to-treat principle. Data are presented as mean (standard deviation (SD)) for normally distributed data and as median (interquartile range (IQR)) for non-normally distributed data.
Intraindividual differences between baseline and post-treatment values were analysed with the paired Student’s t test for normally distributed data or the Wilcoxon signed-ranks test for non-normally distributed data. Differences between the three groups were analysed with a one-way ANOVA (analysis of variance) for normally distributed data or a Kruskal–Wallis test for non-normally distributed data. If significant differences were found, multiple comparisons were made with Bonferroni correction. Comparisons involving only two groups (ie, open-label follow-up and analysis of the pH and manometry data) were analysed using the unpaired Student’s t test. Logistic regression analysis was used to explore the relationship between two variables (eg, the occurrence of adverse events and treatment outcome, or the change in oesophageal acid exposure and treatment response). Differences were considered significant when p<0.05.
RESULTS
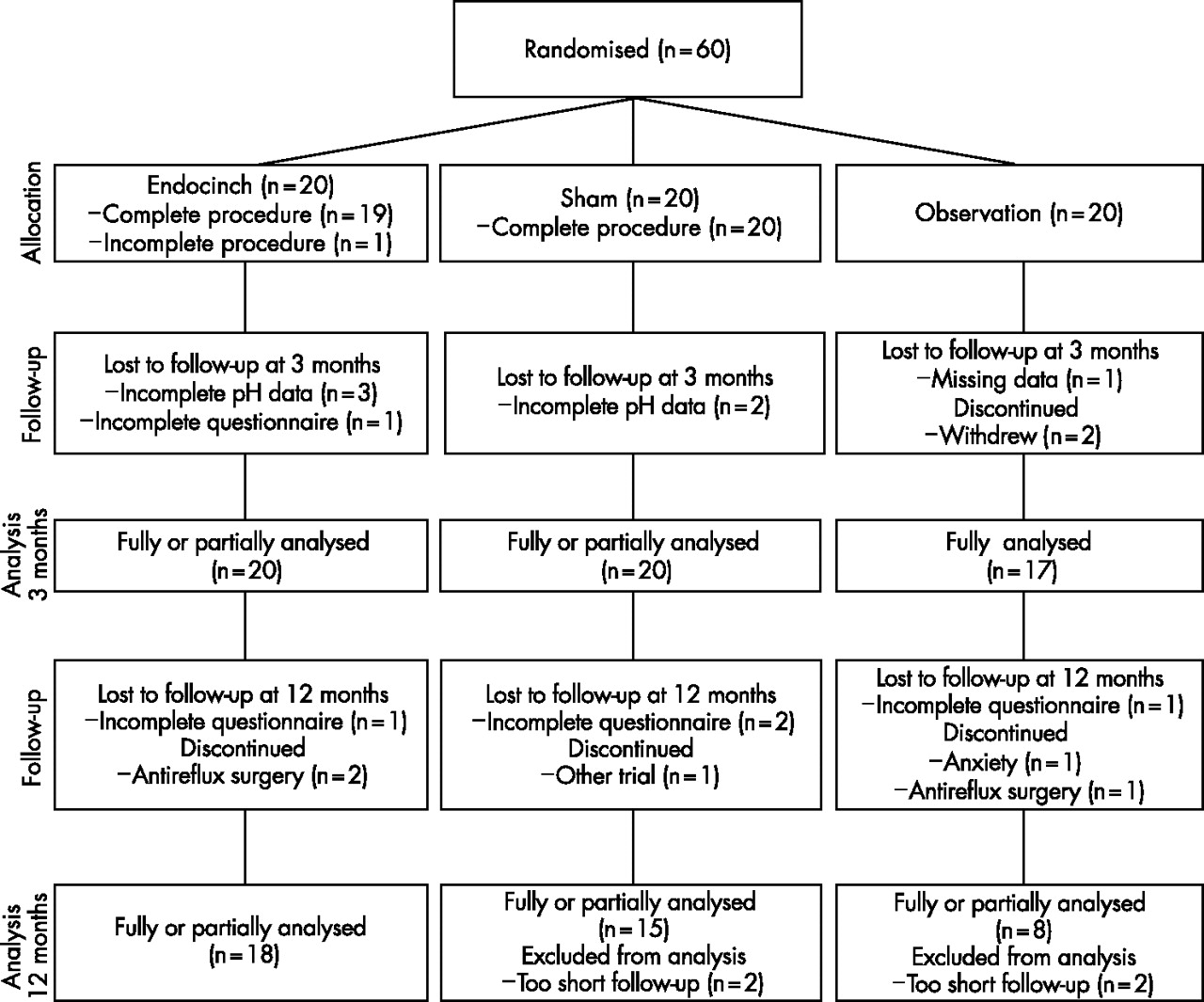
Sixty patients were enrolled between August 2003 and May 2005 (fig 1). All patients were randomly assigned without deviations from the randomisation protocol. Random variation resulted in patients undergoing sham treatment having slightly higher baseline quality of life score in the SF-20 subscale general health. No other significant differences were observed in baseline data between the three groups (table 1).
Baseline patient characteristics
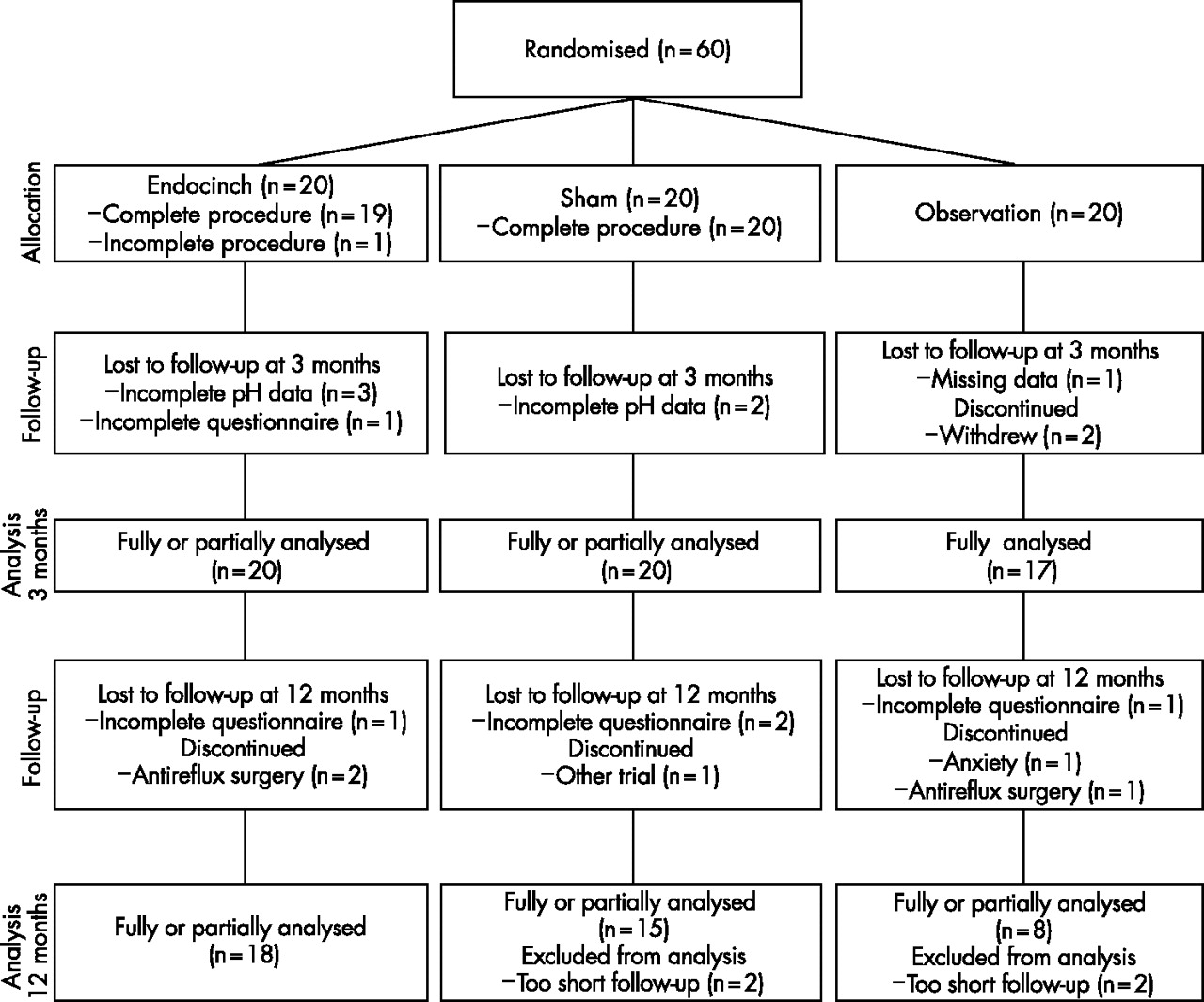
Flow diagram of trial.
In three patients from the observation group, no follow-up data were available: two patients withdrew from the trial before the 3-month evaluation and in one patient data were missing. One patient (randomised to active treatment) did not use PPIs but a H2-receptor antagonist; data on this patient were included when analysing drug use (use related to baseline values), with the exception of calculating the mean dose (mg) of PPIs. Partial or complete 3-month data were available for 57 patients.
Treatment
In one patient of the active treatment group, only two of the planned three gastroplications were placed, due to technical problems. The other 39 patients assigned to active or sham treatment underwent a technically successful and uneventful treatment procedure. Thus, 56 patients received the intended treatment (n = 19, active; n = 20, sham; n = 17, observation), but 57 were analysed according to the intention-to-treat principle. Patients in the active group (n = 20) were sedated with a mean dose of 14 (4) mg midazolam and 46 (11) mg pethidine. The mean procedure time, from start of endoscopy to removal of the endoscope, was 43 (11) min. In the sham group (n = 20), 12 (4) mg midazolam and 45 (10) mg pethidine was administered.
Crossover and retreatment
After 3 months, 30 patients from the sham and observation groups crossed over to active treatment (fig 1). The remaining seven patients from these groups received an alternative endoscopic or surgical treatment for GORD. Thus, a total of 50 patients received active treatment, of whom 41 were analysed after 1-year, open-label follow-up.
Within a year, 12 (29%) patients were retreated with a mean of 1.4 (0.5) extra plications, after a median period of 4.0 (3.25–5.0) months. In these patients 72% of sutures were still present, but only 19% were judged as functional.
Primary end points
Drug use
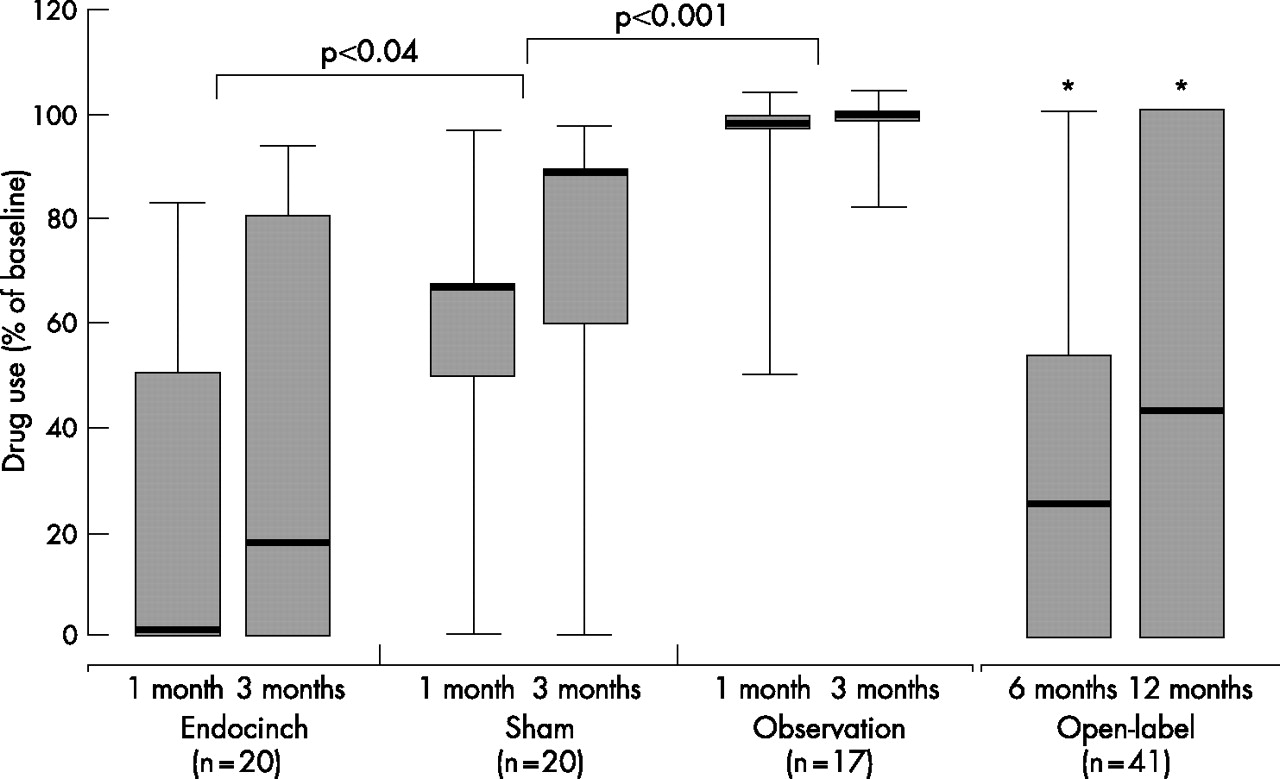
At 1 and 3 months, there was a significantly greater reduction in daily PPI use in active patients compared with sham patients (fig 2). When sham was compared with observation, PPI use was reduced in the sham group as well. At 3 months, 13 (65%) patients in the active group responded to intervention (⩾50% reduction in PPI use) compared with 5 (25%) patients in the sham group and none (0%) in the observation group (p = 0.011, active v sham; p = 0.05, sham v observation). In all, there were 8 (40%) patients in the active group and 1 (5%) patient in the sham group who had reduced PPI use by ⩾95% at 3 months (p = 0.02). The reduction of PPI use in the active treatment persisted at 6 and 12 months (fig 2), although an increase in drug use was noted over time (p = 0.48). At 6 months, the use of PPI reduced by ⩾50% in 32 of 41 (78%) patients, and by ⩾95% in 14 (34%) patients. At 12 months, ⩾50% and ⩾95% reductions were achieved in 68% and 29% of the patients, respectively.

Drug use, expressed as percentage of the baseline dose of antisecretory drugs. The horizontal lines of the boxes denote the 25th, 50th (median) and 75th centile values. Error bars denote the 0 and 100th centiles. p Values apply to between-group comparisons at 1 and 3 months. *p<0.001, compared with baseline.
After 1 year, the number of treatment failures was 25 of 45 (56%) patients (Kaplan–Meier analysis; fig 3).
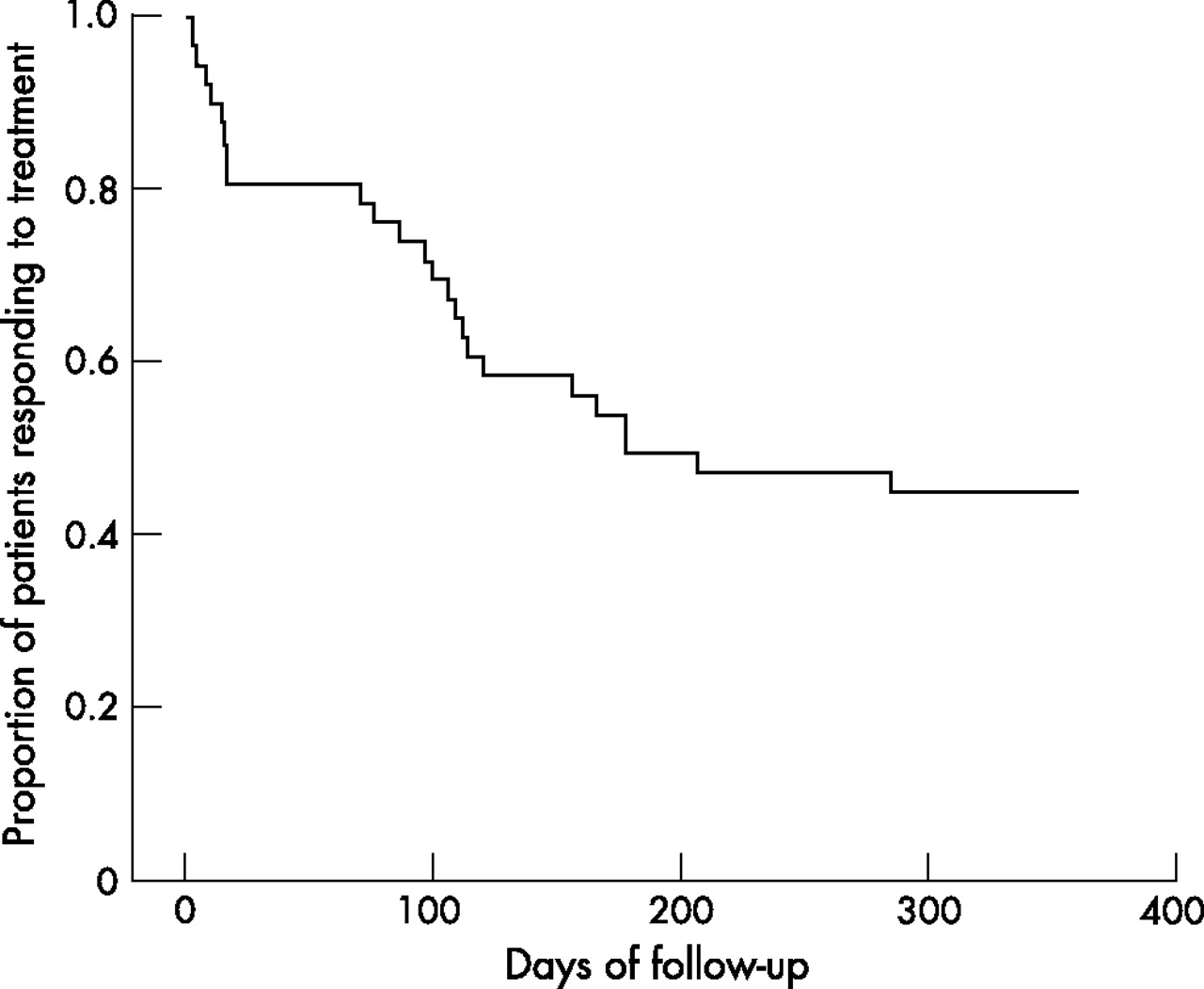
Kaplan–Meier analysis of proportion of patients (n = 45) responding to active treatment during 1-year follow-up. Treatment failures also included patients who chose to receive retreatment (n = 12) or an alternative antireflux treatment (n = 4), according to intention-to-treat analysis.
Symptoms
Heartburn frequency and scores decreased significantly after active treatment compared with sham treatment at 3 months (table 2, fig 4).
Treatment effects at 3 months

Heartburn and regurgitation scores (frequency×severity) before (grey bars) and after 3 months of follow-up (black bars). Data are means (SD). Statistical tests compared mean differences in absolute change from baseline values between groups, and, if significant, multiple comparisons were carried out.
The number of patients that were heartburn-free (frequency <1/month) was 8 (40%) in the active group, 1 (5%) in the sham group and none in the observation group (p = 0.02, active v sham). Regurgitation was also reduced after active treatment, although to a lesser extent, and was significant only for regurgitation frequency when compared with sham (table 2). Heartburn severity and scores slightly improved after observation at 3 months, but there were no significant differences between sham and observation. Symptom improvements were sustained during open-label follow-up (table 3), with 15 of 37 (41%) patients reporting no heartburn at 12 months.
Treatment effects at 6 and 12 months open-label follow-up
Secondary end points
Quality of life
Three months after active treatment, SF-20 quality of life scores were significantly improved in three subscales (role function, general health and bodily pain perception) compared with sham (table 2). No differences were observed in SF-20 scores between sham and observation at 3 months. After 6 and 12 months, the improvements in quality of life scores persisted (table 3).
Oesophageal acid exposure
At 3 months after the procedure, mean oesophageal acid exposure times were decreased in both the active group and, to a slightly lesser extent, the sham group (p = 0.02, active; p = 0.10, sham; table 4).
Treatment effects for pH metry and manometry at 3 months
No differences were seen between the two groups. Figure 5 shows the individual oesophageal acid exposure times. Acid exposure times normalised (pH <4 during <5% of time) in 5 of 17 (29%) evaluated patients of the active group and in 4 of 18 (22%) patients of the sham group (p = 0.71). Acid exposure times were reduced in 12 of 17 (71%) evaluated patients after active treatment and in 11 of 18 (61%) patients after the sham procedure (p = 0.73). No significant changes were found in numbers of reflux periods.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Individual 24-h oesophageal acid exposure values before and 3 months after procedure for the Endocinch and sham groups. Horizontal lines represent mean values.
Oesophageal manometry
No differences were seen in lower oesophageal sphincter pressure (table 4) or oesophageal body contractions (data not shown) when comparing the two treatment groups.
Adverse events
No major adverse events requiring clinical observation, blood transfusion or administration of drugs other than paracetamol (table 5) were seen.
Adverse events
All adverse events were mild and transient, resolving spontaneously within 1 week. Adverse events occurred more frequently in the active group, with the exception of experiencing a sore throat. One patient developed a subcutaneous haematoma as result of a misplaced intravenous line.
Subgroup analysis
Subgroup analysis was done to explore whether a response to treatment (⩾50% reduction in PPI use) was related to a decreased oesophageal acid exposure. A comparison of responders (n = 13, with 12 pH studies) versus non-responders (n = 7, with 5 pH studies) showed that there was a greater decrease in nightly acid exposure (−4.9% v 3.3%; p = 0.036) in responders, although there was no significant difference in total acid exposure time (−3.6% v −0.5%; p = 0.24).
To explore whether the occurrence of an adverse event was related to the outcome of treatment, logistic regression analysis of responders versus non-responders was carried out. Patients experiencing dysphagia after the procedure (transient; n = 10) were more likely to respond to treatment (odds ratio (OR), 13.5; 95% confidence interval (CI), 1.2 to 152.2; p = 0.035). In the group experiencing dysphagia (n = 10, nine pH studies) mean % acid exposure time after the procedure was reduced more compared with the group not experiencing dysphagia (n = 10, eight pH studies; −4.9% v −0.2%, p = 0.022).
DISCUSSION
This randomised trial showed that endoscopic gastroplication, using the Endocinch procedure, significantly reduced GORD symptoms, reduced the use of PPI drugs, and improved quality of life scores at 3 months compared with the sham procedure. The symptom heartburn was improved more than the symptom regurgitation. Oesophageal acid exposure, however, was not reduced more after active treatment than after the sham procedure.
The results of this sham-controlled trial confirm those of prior open-label studies showing that, in the short and intermediate term, endoscopic gastroplication improves GORD symptoms and quality of life, and reduces the use of acid-inhibitory drugs.14–16,19–21 However, the extent of the effect was less in this study than in open-label studies, with just 29% of patients of this study managing to stop use of drugs completely, compared with 50–70% at 3 months in open-label studies.16,19–21 Furthermore, the improvement in oesophageal acid exposure was not significantly greater than after sham treatment, emphasising the importance of a sham comparison.
All three main types of endoscopic GORD treatments (radiofrequency energy, injection and suturing) have now been evaluated by a randomised sham comparison.11,12 Interestingly, in all these three trials symptoms improved significantly as a result of endoscopic treatment, whereas oesophageal acid exposure failed to improve compared with the sham procedure. Although within-group comparisons showed a lower acid exposure after active treatment in the present study, between-group differences were far from significant, as even the sham group improved.
This discrepancy between improvement of GORD symptoms (and drug use) and a lack of improvement in oesophageal acid exposure raises various questions. Firstly, how does endoscopic gastroplication for GORD actually work? Is it merely the reduction in oesophageal acid exposure or does it alter reflux characteristics, such as the proximal extent of reflux in the oesophagus and the volume of the refluxate? Our study was not designed to answer these questions, but we included a subgroup analysis to compare responders with non-responders to further explore the role of oesophageal acid exposure. The definition of a responder (⩾50% reduction in PPI use) used is somewhat arbitrary but consistent with definitions used by other authors.12,17 The result, showing that responders had a greater reduction in acid exposure than non-responders, suggests that at least part of the effect of active treatment is due to a reduction in oesophageal acid exposure. However, the proportion of the decrease in acid exposure might well be a more important factor in symptomatic response than the absolute decrease in oesophageal acid exposure. We know from PPI studies that up to 50% of patients with GORD continue to have an abnormal oesophageal pH profile, despite complete symptom control on drugs.22 A reduction in the proximal extent of the refluxate or specific effects on different types of reflux episodes (acidic, weakly acidic, alkaline and gas–liquid composition) might also play a part. These issues can be dealt with by studies using intraluminal impedance monitoring. Another possible explanation for the treatment effect includes a decreased oesophageal visceroperception as a result of endoscopic gastroplication, as was recently shown in a small study.23
Thus, the pathogenesis of GORD is complex, and thereby the interpretation of oesophageal pH studies. In this respect, how can the improvement in oesophageal acid exposure after a sham procedure be explained? A possible explanation is that there is a difference in patient attitude during the pH study after the procedure compared with the baseline pH measurement. Most patients experience a 24-h ambulatory pH study off drugs as a bothersome investigation; in fact, more than the treatment procedure itself. For this reason, many participants will be less motivated to undergo a second measurement than the first, which would result in an attitude and behaviour leading to avoidance of activities associated with acid reflux during the second pH study. This “postprocedure motivation bias” is likely to occur in both the sham and the active treatment groups. If such a bias indeed has a role, the improvement of oesophageal pH after endoscopic treatment does not properly reflect the true effect of treatment. The net positive effect of endoscopic treatment on acid exposure will be even less pronounced than the data shown now. This type of bias could have played a part in all previously reported uncontrolled studies on endotherapy for GORD that included pH data.
It should be noted that there was an, albeit relatively small, number of dropouts from postprocedure measurements, most importantly three patients in the active group declining a postprocedure pH metry. By our definition, two of these patients were non-responders and one a responder, which may have slightly influenced the results in favour of active treatment.
One might argue that patients randomised to the active group were “unblinded” by the side effects they experienced as a result of the gastroplications (ie, dysphagia, local chest pain) and therefore would be biased towards a treatment effect.24 Indeed, subgroup analysis showed that this group of patients responded better to active treatment than the group without these side effects. However, their oesophageal acid exposure improved more as well, suggesting a true effect of treatment, not a bias effect. Thus, it seems that the occurrence of side effects, such as dysphagia, is an indication of effectively placed gastroplications and a predictor of success.
For this study, a design that included a third group of patients who received no active or sham treatment but who were followed up during ad libitum use of PPIs was chosen. The reason for including this group was to be able to assess the effect of the sham procedure on GORD symptoms. This three-arm design was justified by the fact that the observation group showed a spontaneous improvement in the symptom heartburn at 3 months, which—if present in the sham group—would have been falsely attributed to a sham effect.
A major concern regarding this procedure is its durability in the long term. For this reason we included a 1-year, open-label follow-up, after establishing the primary efficacy in a sham-controlled 3-month design. Treatment effects were reasonably consistent with the 3-month results, with only a marginal increase of drug use over time. However, we should take into account that 29% of patients again received treatment with one or two extra gastroplications. Promising long-term results, as published in previous reports,15,16,19 could therefore be only partly confirmed by the present study. We share concerns with other others with regard to the durability of the endoscopically placed sutures.17,25 Many sutures are lost or seem to be already loose at 2 or 3 months after the procedure,17,25 and a correlation between efficacy and presence of sutures has been established.26 Although we did not include a second, postprocedure gastroscopy in our protocol, a large percentage (81%) of non-functional (loose) sutures was seen during retreatment in non-responders. Probably, postprocedure results would have changed in favour of active treatment if all sutures had remained in place, but the present results reflect the current efficacy of this (imperfect) procedure. It is conceivable that placement of more than three sutures in individual patients, for example, those with larger hiatal openings, would improve the results. We chose, however, to adhere to a strict treatment protocol with a relatively high number of plications (ie, three), based on previous open-label results.16
In summary, this sham-controlled trial of endoscopic gastroplication for GORD showed that this procedure improves GORD symptoms, quality of life and drug use in about two thirds of the patients up to 12 months. However, the reduction in oesophageal acid exposure is modest and is not greater after active gastroplication than after sham treatment. The results emphasise that caution should be undertaken when interpreting the results of uncontrolled pH monitoring studies. The presence of transient dysphagia after the procedure seems to predict a favourable treatment outcome. The procedure was safe and could be carried out well in an outpatient setting under conscious sedation. Although this study confirmed that this method represents an attractive alternative treatment option for patients with uncomplicated GORD unwilling to take drugs, the procedure should be improved to increase the effect on oesophageal acid exposure (and probably the proportion of patients responding) and improve the durability of sutures. Widespread use of the endoscopic suturing device should probably be avoided until the technique is improved and efficacy on objective end points has been proved in a sham-controlled fashion.
Acknowledgments
We thank Elvire Muris and the other nurses who assisted in endoscopic suturing and who have diligently cared for the patients. We acknowledge the statistical support of Dr P Westers, Biostatistics Centre, University of Utrecht, Utrecht, The Netherlands.
REFERENCES
Footnotes
-
Published Online First 8 June 2006
-
Competing interests: HW was supported by a grant from Janssen-Cilag pharmaceuticals.