Article Text

Abstract
Objective Significant heterogeneity was observed in previous trials that assessed the efficacies of sequential therapy for 10 days (S10) versus triple therapy for 14 days (T14) in the first-line treatment of Helicobacter pylori. We aimed to compare the efficacy of S10 and T14 and assess the factors affecting their efficacies.
Design We conducted this open-label randomised multicentre trial in eight hospitals and one community in Taiwan. 1300 adult subjects with H pylori infection naïve to treatment were randomised (1:1) to receive S10 (lansoprazole and amoxicillin for the first 5 days, followed by lansoprazole, clarithromycin and metronidazole for another 5 days) or T14 (lansoprazole, amoxicillin and clarithromycin for 14 days). All drugs were given twice daily. Successful eradication was defined as negative 13C-urea breath test at least 6 weeks after treatment. Our primary outcome was the eradication rate by intention-to-treat (ITT) and per-protocol (PP) analyses. Antibiotic resistance was determined by agar dilution test.
Results The eradication rates of S10 and T14 were 87.2% (567/650, 95% CI 84.4% to 89.6%) and 85.7% (557/650, 95% CI 82.8% to 88.2%) in the ITT analysis, respectively, and were 91.6% (556/607, 95% CI 89.1% to 93.4%) and 91.0% (548/602, 95% CI 88.5% to 93.1%) in the PP analysis, respectively. There were no differences in compliance or adverse effects. The eradication rates in strains susceptible and resistant to clarithromycin were 90.7% and 62.2%, respectively, for S10, and were 91.5% and 44.4%, respectively, for T14. The efficacy of T14, but not S10, was affected by CYP2C19 polymorphism.
Conclusions S10 was not superior to T14 in areas with low clarithromycin resistance.
Trial registration number NCT01607918.
- HELICOBACTER PYLORI - TREATMENT
- ANTIBIOTIC THERAPY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Our previous trial showed a trend of superiority of sequential therapy for 10 days (S10) over triple therapy for 14 days (T14) by 4.7%, but the difference was not statistically significant.
A large trial from Latin America showed contradictory result that T14 was superior to S10.
A meta-analysis putting these trials together showed that S10 was not superior to T14, but there was significant and unexplained heterogeneity (I2=61%) because antibiotic susceptibility was done only in one trial.
What are the new findings?
This trial provides direct evidence with adequate power that S10 is not superior to T14 in areas with low clarithromycin resistance.
Our prediction model showed that whether S10 is superior to T14 depends on the prevalence of antibiotic resistance.
S10 appears to be superior to T14 in areas with high clarithromycin, but low metronidazole resistance and vice versa. Yet, both regimens fail to reach acceptable eradication rates in regions with high clarithromycin or high metronidazole resistance.
How might it impact on clinical practice in the foreseeable future?
These collectively suggested that sequential therapy given for 10 days is not enough and extending the treatment duration of sequential therapy might be indicated.
Introduction
In the face of rising antibiotic resistance, the eradication rate of standard triple therapy for 7–10 days for Helicobacter pylori has fallen below 80% in many countries.1 Extending the treatment duration of triple therapy to 14 days (T14) has been recommended.2 The use of a four-drug therapy, such as sequential therapy, is another strategy to overcome this problem.3 ,4 Several meta-analyses have shown that sequential therapy for 10 days (S10) was superior to triple therapy for 7 or 10 days.5–7 In addition, our previous study showed that sequential therapy for 14 days was superior to T14.8 However, whether S10 is superior to T14 remains controversial. In our previous study, we observed a trend of higher eradication rate (4.7%) of S10 than that of T14, but the difference was not significant.8 In contrast, a multinational study conducted in Latin America showed that T14 was superior to S10 by 5.6%.9 Yet, both regimens failed to achieve acceptable eradication rates in that region.9
Although a recent meta-analysis has shown that the efficacy of S10 was not different from that of T14, further large randomised trial is still necessary because of the following reasons. First, discrepancies (about 35%) between meta-analysis of randomised trials and subsequent large randomised trials were not uncommon, especially when significant heterogeneities were observed in the previous meta-analysis.10 In the previous meta-analysis by Gatta et al, unexplained significant heterogeneity (I2=61.1%) was observed.5 Second, of the seven trials included in that meta-analysis,5 only the trial from our group provided information on antibiotic susceptibility, which might be the most important factor leading to the heterogeneity.8 ,11 Therefore, further large randomised trial, which provides information on antibiotic resistance, is needed to identify the causes of the heterogeneity and to clarify when S10 would be the preferred regimen.
Emerging evidence suggests that eradication of H pylori has the potential to reduce the risk of gastric cancer.12–14 However, the optimal regimen for targeting the asymptomatic population within the community remains unclear. Previous studies, which evaluated the efficacies of anti-H pylori treatment, focused mainly on symptomatic subjects who were recruited from hospitals,1–8 ,15 while treatment of asymptomatic carriers in the community may be more vulnerable to the side effects, which are highly associated with the length and complexity of the antimicrobial regimen.16 As a result, their compliance may be reduced. However, no evidence currently exists to support this speculation, and it is unclear if the results based on hospital populations can be extrapolated to community populations.
To address these issues, we conducted a randomised trial to compare the efficacy of S10 with that of T14 in first-line therapy of H pylori infection by recruiting both community-based and hospital-based populations. We aimed to comprehensively evaluate the impact of antibiotic resistance on treatment efficacies and also provide a predictive model to estimate the results in areas with a different prevalence of antibiotic resistance.
Materials and methods
Trial design and settings
This multicentre open-label parallel randomised trial was conducted in eight hospitals (outpatient department) on the main island of Taiwan and in a community population residing in an offshore island (Matsu Island) from February 2012 to March 2014. The details of screen-and-treat for H pylori infection in the community population in Matsu Island (high risk for gastric cancer) have been previously reported.13 Our protocol was approved by the institutional review board of each participating unit. Study research staff recruited potential participants, and explained the purpose and eligibility requirements of the study to them. Written informed consent was obtained from each subject prior to enrolment. The ClinicalTrials.gov registration identifier is NCT01607918.
Participants
Subjects 20 years or more in age with documented H pylori infection (as described below) were eligible for enrolment. Subjects with any one of the following criteria were excluded from the study: (1) history of gastrectomy, (2) previous eradication therapy for H pylori, (3) pregnant or lactating women, (4) contraindication or previous allergic reaction to the study drugs, (5) use of antibiotics within 4 weeks and (6) severe concurrent diseases or malignancy.
Determination of H pylori status
In the hospital setting, H pylori status was determined by: (1) rapid urease test, (2) histology, (3) culture and (4) serology. Subjects with positive results in at least two of the above tests were eligible for enrolment (criterion 1). In the community setting, a single positive 13C-urea breath test (13C-UBT) was defined as H pylori infection (criterion 2),3 and those with positive 13C-UBT were invited to undergo endoscopic screening and biopsy for culture. The 13C-UBT, which contained 75 mg13C-urea, was dissolved in water and mixed with orange juice. Baseline and 30 min breath samples were assayed with an infrared spectrometer at the Taipei Institute of Pathology, and computer-generated results were produced. Positive results were defined as a delta value of ≥4 units and negative results as <2.5 units, with the sensitivity and specificity of 97.8% and 96.8%, respectively.17 For all participants, a follow-up 13C-UBT was performed at least 6 weeks after completion of treatment to confirm successful eradication. All subjects were asked to stop proton-pump inhibitors and histamine-2 blockers for at least 2 weeks prior to the 13C-UBT. Patients with inconclusive results received another 13C-UBT at least 2 weeks later until the results became conclusive. The technicians who performed the 13C-UBT assays by infrared spectrometer were blinded to the treatment regimens.
Randomisation and blinding
Eligible subjects were randomised in a 1:1 ratio to receive one of the following regimens: S10: lansoprazole 30 mg and amoxicillin 1 g for the first 5 days, followed by lansoprazole 30 mg, clarithromycin 500 mg, and metronidazole 500 mg for another 5 days (all given twice daily); or T14: lansoprazole 30 mg, amoxicillin 1 g and clarithromycin 500 mg for 14 days (all given twice daily). The permuted block randomisation sequence, with a block size of four, was computer generated. The sequence was concealed in an opaque envelope, and was kept by an independent research assistant at the National Taiwan University Hospital (NTUH) until treatment was assigned. All investigators were blinded to the randomisation sequence. After obtaining written informed consents from eligible subjects, the study nurses contacted the independent assistant at NTUH to obtain the next allocation number by phone in order to ensure adequate allocation concealment.
Outcomes
The primary end-point of the study was the eradication rates in the first-line therapy. The secondary end-points were the frequency of adverse effects and compliance. Intention-to-treat (ITT) and per-protocol (PP) analyses were performed in the assessment of the primary end-point. All randomised subjects were included in the ITT analysis. All protocol violators, such as subjects who failed to take at least 80% of their treatment drugs, or who had unknown post-treatment H pylori status, were excluded from the PP analysis. Subjects who did not return for a follow-up 13C-UBT were considered treatment failures. Subjects were informed of the common side effects associated with the study drugs before the therapy began; they were also asked to record these symptoms during treatment. In both settings (hospital and community), a standardised interview was arranged at the end of treatment when patients were questioned regarding the incidence of any adverse events and the drug compliance. The pills not taken by the patients were also counted. Compliance was considered low if less than 80% of pills were taken. Subgroup analyses were conducted according to the demographics, host genetic polymorphism, bacterial antibiotic resistance and the community/hospital-based populations.
Determination of host CYP2C19 polymorphism and genotypic/phenotypic antibiotic resistance of H pylori
The SEQUENOM MassARRAY System in the National Genotyping Center was used for genotyping of CYP2C19 polymorphism.18 PCR, with or without direct sequencing using the automatic sequencer (ABI PRISM 3100 Genetic Analyzer, Applied Biosystems), was used for the determination of genotypic antibiotic resistance, including 23S rRNA (clarithromycin resistance) and gyrA (levofloxacin resistance).19 ,20 The phenotypic antibiotic resistance was determined by the minimum inhibitory concentration on the agar dilution test. The resistance breakpoints for clarithromycin, metronidazole, amoxicillin and levofloxacin were defined as ≥1, ≥8, ≥0.5 and > 1 mg/L, respectively.8 ,20
Statistical analysis
Categorical data were compared using the χ2 test or Fisher's exact test, as appropriate. Continuous data were compared using the Student's t test and expressed as mean (SD). Regarding the sample size estimation, we hypothesised that there would be approximately a 6% difference in the eradication rates between the two studied regimens.8 Knowing that the eradication rate of T-14 was approximately 85%,8 ,21 our original sample size estimation was at least 500 for each group, given a power of 80% and a 0.05 two-side type 1 error, assuming a 10% loss to follow-up. Following an interim report, we decided to increase the sample size to a conservative estimate of 650 for each group, hoping to reach a power of 90% in the rejection of the null hypothesis. Multiple logistic regression analysis was performed to identify predictors of treatment failure. All p values were two-tailed, with the level of statistical significance set at 0.05. The statistical analyses were performed using the SPSS V.21.0 statistical software for Windows 7 (IBM, Armonk, New York, USA). All authors had access to the study data, and had reviewed and approved the final manuscript.
Ancillary analysis
We constructed a prediction model in order to explain the contradictory results in the literatures and to suggest the optimal regimens in areas with different prevalence of clarithromycin and metronidazole resistance. The data required for model generation was based on the eradication rates of S10 and T14 according to the antibiotic resistance, which was obtained from the present study and our prior study8 (see online supplementary table S1). The efficacy of sequential therapy and triple therapy can be predicted in an area with clarithromycin resistance rate of p and metronidazole rate of q (0≤p≤1; 0≤q≤1) as long as the efficacies in resistant and susceptible strains are known.11 If the eradication rates of a regimen (containing these antibiotics) in strains susceptible to clarithromycin and metronidazole, susceptible to clarithromycin but resistant to metronidazole, resistant to clarithromycin but susceptible to metronidazole and dual resistant to both were A, B, C and D, respectively, the predicted eradication rate of that regimen would be A*(1−p)*(1−q)+B*(1−p)*Y+C*p*(1−q)+D*p*q. Then, we obtained the difference (δ) in the efficacy of sequential therapy and triple therapy, which was a function containing p and q. The function of δ was plotted using the Desmos Graph Calculator (https://www.desmos.com/calculator).
Results
Baseline characteristics, H pylori eradication rates and adverse effects
From February 2012 to March 2014, a total of 1300 subjects were randomised to receive one of two treatments, as detailed in the Consort flowchart shown in figure 1. Baseline characteristics of the two treatment groups (n=650) were similar (table 1). The eradication rates of S10 and T14 were 87.2% (567/650, 95% CI 84.4% to 89.6%) and 85.7% (557/650, 95% CI 82.8% to 88.2%) in the ITT analysis, respectively (p=0.418), and the results were 91.6% (556/607, 95% CI 89.1% to 93.4%) and 91.0% (548/602, 95% CI 88.5% to 93.1%) in the PP analysis, respectively (p=0.726); no significant difference was noted between groups (table 2). The frequencies of adverse effects were not significantly different between the two groups, except for a slightly higher proportion of nausea in S10 than T14 (5.3% vs 2.8%, p=0.04). Less than 3% of patients discontinued the drugs due to adverse effects. The compliance to treatment was not significantly different between two groups (96.3% vs 94.6%, p=0.143).
Demographic characteristics and prevalence of antibiotic resistance
Eradication rates and adverse effects

The Consort diagram. H pylori, Helicobacter pylori; S10, sequential therapy for 10 days; T14, triple therapy for 14 days; PP, per-protocol analysis.
Subgroup analysis
The subgroup analysis results are shown in table 3. In the community population, the prevalence of peptic ulcer, clarithromycin resistance, levofloxacin resistance and adverse effects were lower while their compliance to treatment (eg, took at least 80% of drugs, took the drugs correctly and were lost to follow-up) was similar to that of the hospital population. The treatment efficacies (ITTs) in the eradication of H pylori infection were 85.3% (220/258, 95% CI 81.0% to 89.6%) and 82.2% (213/259, 95% CI 77.5% to 86.9%) for S10 and T14, respectively, in the community population, and the difference was not significant. Tests for interaction did not show any significant factor, which would modify the relative efficacy between the two treatments.
Characteristics and outcomes according to settings
Factors affecting eradication rates
As shown in table 4, the eradication rates in strains susceptible and resistant to clarithromycin were 90.7% and 62.2%, respectively, for S10, and were 91.5% and 44.4%, respectively, for T14, which indicated that the presence of clarithromycin-resistant strains significantly suppressed the eradication rates for both S10 and T14 (p<0.001). In the presence of dual resistance to clarithromycin and metronidazole, the eradication rates of S10 and T14 were further suppressed to 50% (9/18) and 33.3% (7/21). The eradication rates of both regimens were lower in subjects exhibiting poor compliance (p<0.001). The eradication rate of T14, but not S10, was lower in subjects with intermediate/extensive metabolisers of CYP2C19 (408/481, 84.8%) compared with that of the poor metabolisers (73/77, 94.8%), and was lower in the community population (213/259, 82.2%) compared with the eradication rate of T14 in the hospital population (344/391, 88.0%). Multiple regression analyses showed that poor compliance and clarithromycin resistance were risk factors for S10 treatment failure. Poor compliance, clarithromycin resistance and intermediate/extensive metabolisers of CYP2C19 were risk factors for T14 treatment failure.
Factors affecting eradication rates in the first-line therapy
Prediction of efficacy in areas with different prevalence of antibiotic resistance
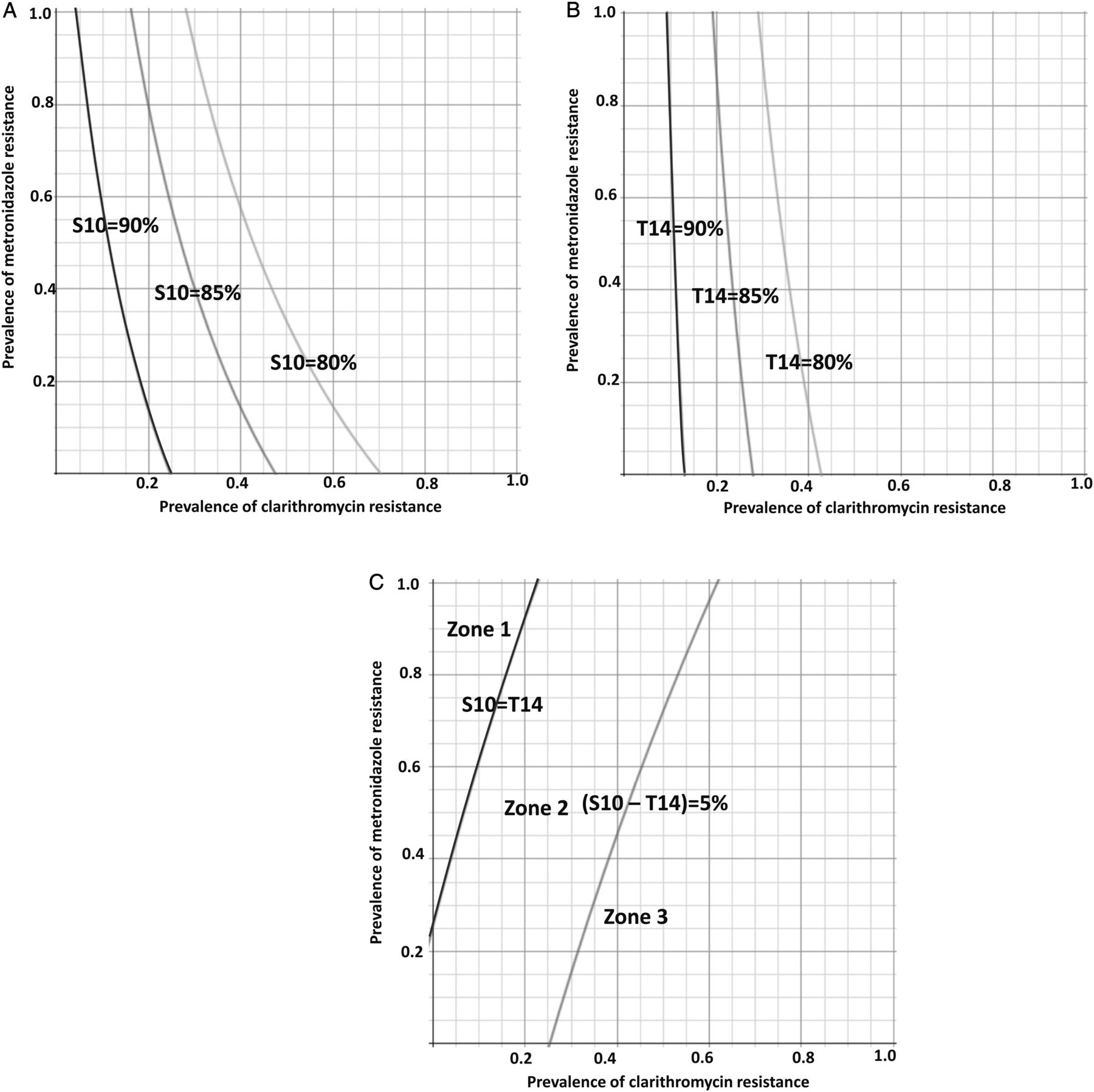
The predicted efficacy of S10 in an area with clarithromycin resistance of p and metronidazole resistance of q would be 0.954*(1−p)*(1−q)+0.918*(1−p)*q+0.735*p*(1−q)+0.5*p*q. The model suggested that the efficacy of S10 would be less than 90% in areas where the clarithromycin resistance rate (p) is 10% and metronidazole resistance rate (q) is greater than 50% (figure 2A). Similarly, the efficacy of T14 would be 0.944*(1−p)*(1−q)+0.947*(1−p)*q+0.567*p*(1−q)+0.401*p*q. The model suggested that the efficacy of T14 would be less than 90%, 85% and 80% in areas where the clarithromycin resistance rate is higher than 10%, 20% and 30%, respectively (figure 2B). The difference (δ) of the efficacy between S10 and T14 would be 0.158*p−0.039*q−0.03*p*q+0.01. The prediction model shows a trend that S10 appears to be more effective than T14 in areas with higher clarithromycin resistance and lower metronidazole resistance, and vice versa (figure 2C).
{kind=link}
{kind=link}
The predicted efficacies of anti-Helicobacter pylori treatments according to the prevalence of antibiotic resistance to clarithromycin and metronidazole. In (A), the predicted efficacies for sequential therapy for 10 days (S10) are shown with the lines labelled with S10=90%, 85% and 80%. In (B), the predictive efficacies of triple therapy for 14 days (T14) are shown with the lines of T14=90%, 85% and 80%. In (C), the predicted differences between S10 and T14 are shown, where the line S10=T14 represents the region where the efficacy of S10 would be equal to that of T14 and the line (S10–T14)=5% represents the region where the efficacy of S10 would be higher than that of T14 by 5%. There are three zones between these two lines: zone 1 represents the regions where the efficacy of T14 would be better than that of S10, zone 2 represents the regions where the efficacy of S10 would be better than that of T14 by less than 5% and zone 3 represents the regions where the efficacy of S10 would be greater than that of T14 by more than 5%.
Discussion
In this large randomised trial, we provided direct evidence with adequate power to demonstrate that S10 was not superior to T14 in either the community-based or the hospital-based population in Taiwan where the prevalence of clarithromycin resistance remains low. The efficacies of both regimens were reduced by clarithromycin resistance and poor compliance. The efficacy of T14 was further affected by CYP2C19 polymorphism and the enrolment setting (ie, community or hospital based). Given the abundant data of antibiotic susceptibility testing, we are able to formulate a prediction model showing that whether S10 is superior to T14 depends on the prevalence of antibiotic resistance in that country.
The differences in the prevalence of antibiotic resistance might be the most important factor leading to the contradictory results of clinical trials comparing the efficacy of sequential therapy and triple therapy.11 ,22 Unfortunately, many of the previous trials did not provide information on antibiotic resistance, which limited their implications for other populations.5–7 Besides, the prevalence of clarithromycin and metronidazole resistance is expected to vary in different geographical areas, and is also expected to change over time even in the same geographical area.2 ,3 ,16 It is impractical and costly to repeat a similar clinical trial in different countries or periodically in the same region. Therefore, we proposed that clinical trials in the treatment of H pylori infection should provide information on the antibiotic resistance. With such information, we can predict the efficacies of the regimen in regions with different prevalence of resistance.11 ,22
The main novelty of our study included the extensive collection of antibiotic susceptibility data from both community-based and hospital-based populations. Among the previous studies that compared the efficacy of S10 and T14,8 ,9 ,23–30 only the study from our research group has provided information regarding antibiotic resistance, which was confirmed to be the most influential factor in the determination of treatment efficacy.8 In the present study, based on 1150 isolated H pylori strains, we again emphasised the importance of antibiotic resistance on the optimal choice of anti-H pylori treatment. In our predictive model, we found that S10 would be superior to T14 in areas with higher clarithromycin resistance, but lower metronidazole resistance (ie, zone 2 and zone 3 in figure 2C). T14 would be superior to S10 only in areas with concomitantly very low clarithromycin resistance and very high metronidazole resistance. In most regions (ie, zone 2), the differences between S10 and T14 would be minimal (less than 5%), which was consistent with the results from the literature.
Another important message provided by our study is the optimal treatment length of sequential therapy.1–3 Previous meta-analyses showed that S10 was superior to T7 or T10.5–7 Our previous study showed that S14 was superior to T14.8 Direct evidence is not yet available with adequate statistical power to compare the treatment efficacy between S10 and T14, especially in regions with low clarithromycin resistance. To further solidify the generalisability of our finding, we did an updated systematic review and meta-analysis by including the present trial and another eight published trials8 ,9 ,23–27 ,29 (the details are available on request). We found that the efficacy of S10 appeared to be similar to that of T14 (summarised OR 1.25, 95% CI 0.91 to 1.72, p=0.17). The finding was similarly seen when the studies were stratified according to the reported prevalence rate of clarithromycin and metronidazole resistance in areas where the clinical trials were conducted. While in areas with high clarithromycin resistance, the non-clarithromycin containing regimens, such as the bismuth quadruple therapy, may be considered as the first-line treatment.3 ,15
In the present study, we found that the efficacy of T14 was affected by the CYP2C19 polymorphism, but not S10, which deserves special attention. Recent meta-analyses have showed that the efficacy of triple therapy containing amoxicillin and clarithromycin was higher in those with CYP2C19 loss-of-function variants, especially when omeprazole or lansoprazole were used, which was consistent with our finding.31 ,32 Regarding the impact of CYP2C19 polymorphism on the efficacy of sequential therapy, we speculated that the use of metronidazole, which was less affected by intragastric pH, might be the possible explanation.33 This speculation was also consistent with our previous study showing that the efficacy of modified sequential therapy was not affected by the CYP2C19 polymorphism.34 Therefore, in populations where the proportion of extensive metabolisers is higher, such as Caucasians,32 sequential therapy might be the preferred regimen.
Our study also evaluated the efficacy of both treatments in a community-based population that underwent gastric cancer chemoprevention.13 Theoretically, asymptomatic subjects are more subject to side effects (related to the dose, kind and number of antibiotics), treatment duration (eg, 14-day regimen) and complexity of the regimen (eg, sequential therapy), which may lead to a lower treatment compliance. Although we did not identify any significant differences in treatment efficacy between the two regimens (in either the community-based or the hospital-based populations), the efficacies of both regimens were lower in the community setting compared with the hospital setting, and T14 had reached a statistically significant level; this finding was consistent with our speculation. Given a similar or lower antibiotic resistance rate in the community population, the reason for such a difference in efficacy is likely related to their lower compliance.
The strength of this study included its large sample size, the analysis of eradication rate according to antibiotic susceptibility, the evaluation of host CYP2C19 polymorphism and the consideration of different enrolment settings. The prediction model was based on the direct comparison of S10 and T14 in our two large randomised trials, which could eliminate the confounding factors and provide more accurate prediction. Nevertheless, our study had several limitations. First, even though we had a high yield rate of bacterial culture of 82.4% (826/1003), the results of antibiotic susceptibility tests were not available in approximately 34% of patients in the present study, which was related to the inherent difficulty in performing such tests. However, this did not affect the main purpose of our study (S10 vs T14). The treatment efficacies were indeed similar between the groups with and without antibiotic resistance data; so, we believe that selection bias was unlikely. Second, the eradication of T14 (85.7%) was slightly higher than that (83.3%) reported in our previously trial, probably attributed to the non-significant lower clarithromycin resistance (9% vs 11%) and non-significant better compliance.8 Third, subjects in the community were eligible only based on a positive 13C-UBT such that the risk of misclassification in detection of H pylori infection might occur. However, through a randomised allocation, the main conclusion of our study was unlikely to be altered. Fourth, the present trial was conducted in Taiwan with a lower clarithromycin resistance rate, but a moderate metronidazole resistance rate. The regimens that were studied may not be applicable to areas with high clarithromycin or high metronidazole resistance. Further evaluation of other regimens may be needed (such as the bismuth-containing quadruple therapy) in order to improve the eradication rate for such areas. Nevertheless, the prevalence of clarithromycin remains lower than 15%–20% in many countries, such as South America, North Europe, UK, Germany and Spain.35 ,36 Fifth, the genotyping for antibiotic resistance was missing in some cases for 23S rRNA (0.4%, 3/812) and gyrA (4.1%, 33/812) because of technical failure such that there was small discrepancy between the results of antibiotic resistance by the agar dilution method and the detection of 23S rRNA and gyrA mutations. Also, antibiotic resistance could be found when there was no genetic mutation. However, although the mutations at position 2142 and 2143 of 23S rRNA were the most important causes of clarithromycin resistance, there could be other point mutations or other mechanisms to account for the clarithromycin resistance.19 ,33 The same is true for the relationship between the gyrA mutation and levofloxacin resistance.37 Finally, it is interesting to find a persisting low prevalence rate of clarithromycin in our country. We believe it is due to the fact that, in National Health Insurance in Taiwan (coverage more than 99% over whole residents), there is a strict regulation of the use of antibiotics, including the macrolides, according to their indications. In addition, following the first-line treatment of H pylori, the retesting process is recommended and reimbursed by the National Health Insurance such that the occurrence of antibiotic-resistant strains of H pylori could be minimised.38 ,39
In conclusion, S10 was not superior to T14 in first-line therapy for H pylori infection in Taiwan where the clarithromycin and metronidazole resistance rates were approximately 10% and 25%, respectively. Our prediction model further suggested that the efficacies of S10 and T14 varied according to the prevalence of clarithromycin and metronidazole resistance. Neither S10 nor T14 achieved acceptable eradication rates in regions with high clarithromycin or high metronidazole resistance, and are not recommended in these settings.
Acknowledgments
The authors would like to express their special thanks to the staff of the Eighth Core Lab, Department of Medical Research, National Taiwan University Hospital, the National Genotyping Center and the first-line healthcare workers in Matsu Island.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
J-ML and C-Chang Chen contributed equally.
Y-CL and M-SW contributed equally.
Contributors The study was conceived by J-ML, C-Chang Chen, Y-CL and M-SW with input from all the other listed contributors from the Taiwan Gastrointestinal Disease and Helicobacter Consortium. J-ML and M-SW designed the study and wrote the protocol. J-ML and Y-CL prepared the statistical analyses. J-ML, Y-CL, C-Chang Chen, M-JC, C-Chang Chen, C-YC, Y-JF, J-YL, T-HY, J-CL, J-YW, T-CL, W-HC, Y-CH, C-CChang, M-JB, C-HT, T-YL, C-FH, J-TL and M-SW recruited patients to the study. C-TS contributed to the histological assessment. J-ML drafted the article, which was critically revised by Y-CL and M-SW. M-SW supervised the hospital setting and Y-CL supervised the community setting in Matsu Island. All authors commented on drafts and approved the final version. All authors had full access to the data and participated in the decision to submit for publication.
Funding The study was funded by the National Taiwan University Hospital (103-002516) and the Ministry of Science and Technology, Executive Yuan, ROC, Taiwan (Grant Number: NSC 103-2325-B-002-022, 102-2628-B-002-034-MY3 and NSC 102-2325-B-002-074). The lansoprazole used in the present study was provided for free by the Takeda Company (Taiwan).
Disclaimer The funding source had no role in study design, data collection, analysis or interpretation, report writing or the decision to submit this paper for publication.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The project was approved by the Institutional Review Board of NTUH and collaborative institutions.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Contact with J-ML for data sharing (dtmed046@pchome.com.tw).
J-ML and C-Chang Chen contributed equally.
Y-CL and M-SW contributed equally.