Article Text

Statistics from Altmetric.com
Message
The incidence of oesophageal adenocarcinoma (EAC) is steeply rising. Early lesion detection is a critical factor for improving disease prognosis. We developed and investigated wide-field near-infrared fluorescence molecular endoscopy (NIR-FME), using systemic and topical administration of a fluorescence-labelled antibody against vascular endothelial growth factor (VEGFA). Fourteen patients with Barrett’s oesophagus (BE) underwent endoscopic mucosal resection (EMR) combined with NIR-MFE. From a total of 20 confirmed aberrant lesions identified with NIR-FME, 4 lesions were missed by high-definition (HD) narrowband imaging (NBI) and white-light endoscopy (WLE). This overall 25% detection enhancement advocates NIR-FME as a promising ‘red-flag’ technique for improving early oesophageal lesion detection. ClinicalTrials.gov ID NCT02129933.
In more detail
Worldwide, >450 000 people are diagnosed with oesophageal cancer each year. In the western world, at least 80% of these cancers concern EAC.1–4 Late-stage disease detection challenges the efficacy of therapies, resulting in 400 000 deaths each year. Therefore, there is a pressing need for new endoscopic techniques that enable early EAC detection. Endoscopic imaging of targeted fluorescent agents directed against cancer-specific cellular and subcellular moieties, that is, fluorescence molecular endoscopy (FME), has been heralded as a novel method for oesophageal dysplasia and cancer detection.5 FME enables surface and subsurface visualisation of cancer-specific pathophysiology, going beyond the surface-only morphology and tissue discolourations visible with HD-WLE.6–10
In this study, we investigated for the first time real-time NIR-FME of EAC and dysplasia. A pilot study in patients with BE was based on a novel custom-built NIR fluorescence endoscope, paired to a HD-WL clinical scope (online supplementary figure 1) and employed the anti-VEGFA antibody bevacizumab, labelled with the NIR-fluorescent 800CW. The potential of VEGFA as an early discriminating target in BE was first confirmed by immunohistochemistry, demonstrating that all dysplastic tissues expressed VEGFA (online supplementary figure 2).
Supplementary file 1
The study furthermore compared systemic versus topical tracer administration during clinical inspection of the oesophagus in 14 patients with BE, scheduled to undergo an EMR of previously diagnosed lesions (figure 1A). Five patients received an intravenous bolus of bevacizumab 800CW, 2 days prior to the NIR-FME procedure (4.5 mg, bolus injection). The other nine patients received topical administration of the tracer, by spraying bevacizumab 800CW on the luminal surface (100 µg/mL per cm BE) immediately prior to wide-field NIR-FME. The online supplementary table 1 summarises study subjects and lesion characteristics.
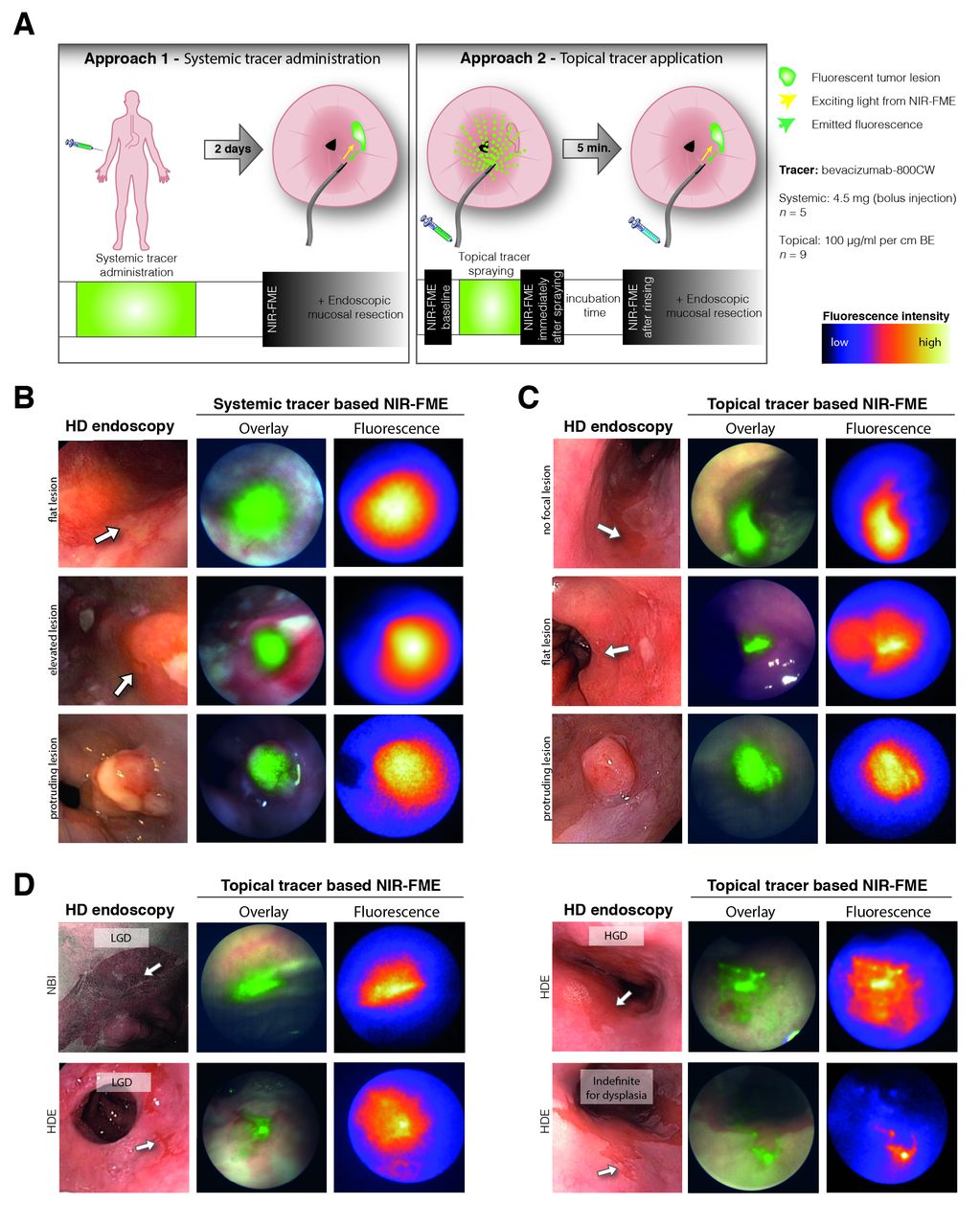
Real-time VEGFA-targeted NIR-FME. (A) Schematic overview and timeline of the two NIR-FME approaches (n=14). (B) Examples of the systemic tracer based, and (C) the topical tracer results, summarising that all lesions could be visualised with NIR-FME, including one EAC area which was not visible during HD inspection (displayed in C—first row). (D) Additionally identified dysplastic areas during NIR-FME, which were missed during HD-NBI inspection. All fluorescence signals presented here are uncorrected; overlay images display the high intensities only. EAC, oesophageal adenocarcinoma; HD, high-definition; HGD, high-grade dysplasia; LGD, low-grade dysplasia; NIR-FME, near-infrared fluorescence molecular endoscopy; NBI, narrow-band imaging; VEGFA, antibody against vascular endothelial growth factor.
In the systemic tracer administration subgroup, four out of five EAC lesions were well identified by wide-field NIR-FME inspection (figure 1B). The fifth lesion had its origin in the gastric cardia and was only visible in endoscopic U-turn. Due to the bending restrictions of the current fibre bundle, this lesion was not accessible for the custom-built NIR-FME endoscope employed in the study. Nevertheless, this fifth lesion demontrated high fluorescent tracer uptake ex vivo (online supplementary figure 3). In the topical tracer group, NIR-FME visualised all (12/12) dysplastic and neoplastic lesions, exactly matching the contour of the lesion during HD-WLE inspection, including a carcinomatous area that was only identified by random biopsies (figure 1C; total of 9 patients: 1/9 no focal lesion on HD-WLE/NBI inspection, 5/9 one focal lesion and 3/9 patients two focal lesions). In addition, topical tracer-based NIR-FME identified four additional dysplastic lesions, which were not identified by HD-WLE and NBI inspection (+33%, figure 1D). Moreover, the topical administration led to a slightly higher in vivo tumour-to-background ratio (TBR) of 4.30±0.41, compared with the systemic administration (online supplementary figure 4).
Comments
The known limitations of clinically available endoscopes initiated a search for novel imaging techniques that allow improved detection of early oesophageal lesions. FME is heralded as a highly promising method for detecting dysplastic and neoplastic lesions. To date, three studies—one ex vivo study and two clinical trials—have been reported on FME in EAC5 11 12; however, none of these studies showed real-time wide-field inspection of the oesophageal lumen. Compared with previous studies, the NIR-FME technique offers three advantages. First, the system design enables concurrent use of HD-WLE and sensitive functional fluorescence detection of lesions. Second, NIR-FME offers a ‘red-flag’ surveillance method that inspects at least four orders of magnitude higher fields of view compared with confocal laser endomicroscopy, an ability that can be further exploited to guide biopsy. Moreover, the switch from visible wavelengths in previous studies5 11 12 to the NIR leads to fluorescence detection with superior sensitivity, allowing for the first time real-time in vivo WLE and concurrent FME imaging. Finally, NIR wavelengths are less subjected to interference by haemoglobin absorption, autofluorescence signals and tissue scattering.13
The endoscopic fluorescence images, concurrently recorded with HD-WLE in vivo, matched the focal areas as defined with HD-WLE. In addition, ex vivo fluorescence imaging precisely matched the histology findings (figure 2A; details online). The areas that exhibited increased fluorescence—including the areas that were not identified as dysplastic by HD-WLE—were identified as aberrant by histopathology (true positives; figure 1B–D). Random biopsies, which contained benign mucosal lining, did not exhibit fluorescence (true negatives). Moreover, we did not observe fluorescence at the submucosal layer or at the resection margin following EMR, which was confirmed by histopathology; all EMR procedures were radical (R0) resections, as evinced by follow-up endoscopy.

{kind=link}
{kind=link}
Ex vivo VEGFA and fluorescent signal analyses of study subjects. (A) Boxplot presenting IHC results (H-score: median, 10–90 percentile); a significant difference in VEGFA staining intensities is observed between the dysplastic and benign tissue sites (**P<0.0001). (B) Tukey boxplot presenting the MFIs observed (mean value in bold) (*P<0.05). (C) Fluorescence scan and 3D surface plot demonstrating that the tracer is located in the EAC area and (D) fluorescence microscopy of this same area showing NIR fluorescence within the stromal tissue, between the tumour ducts. (E) Fluorescence scan demonstrating that the tracer is located in tumour blood vessels and tumour ducts. EAC, oesophageal adenocarcinoma; EMR, endoscopic mucosal resection; HE, haematoxylin and eosin; HGD, high-grade dysplasia; IHC, immunohistochemistry; IM, intestinal metaplasia; MFI, mean fluorescence intensities; NIR, near-infrared; VEGFA, antibody against vascular endothelial growth factor.
In addition, fluorescence signals recorded ex vivo were congruent with high intracellular VEGFA stainings (figure 2A). This finding is consistent with previous observations, linking (labelled)-bevacizumab uptake to areas of elevated VEGFA.14–16 Furthermore, labelled bevacizumab has been shown trapped in the extracellular matrix, when bound to the large VEGFA isoforms that are attached to the cell surface.14 17 This reported high VEGFA expression in dysplastic and neoplastic areas can be explained by the role of VEGFA in neovascularisation and has been reported to be elevated already in BE dysplasia.17-22
Ex vivo assessment of the specimen obtained from the systemic tracer group showed significant differences in mean fluorescence intensity between the aberrant areas (EAC/high-grade dysplasia) and the benign mucosal lining, resulting in a favourable ex vivo TBR of 16.7 (figure 2B, P value <0.001). Furthermore, ex vivo NIR microscopy of the formalin-fixed and paraffin-embedded slices confirmed the presence of NIR fluorescence in EAC areas (figure 2C), tumour stromal tissue and surrounding tumour blood vessels (figure 2D-E), while low fluorescence was seen at the margin containing normal Barrett lining. Likewise, macroscopic ex vivo imaging of the formalin-fixed specimens that received topical tracer administration exhibited NIR fluorescence at dysplastic and EAC sites (online supplementary figure 5), though typically at lower intensity compared with the samples from the group receiving systemic administration due to agent washout during the fixation process.
We observed adverse events in 4/14 patients, all known complications of the EMR procedure: bleeding (n=2), nausea/headache (n=1) and fever (n=1). Most likely these events are not tracer-related as only 1%–1.5% of the therapeutic bevacizumab dose was used (4.5 mg vs 5 mg/kg). Our study has several limitations. First, our NIR-FME system uses a sensitive fibre bundle for fluorescence imaging, but an integrated NIR imaging system in a standard HD endoscope would most likely simplify the procedure. Second, our patient sample is small and powered as phase I study for safety, therefore, a randomised phase II or III trial is required to verify the additive role of NIR-FME in BE surveillance.
In conclusion, this work demonstrates that concurrent use of VEGFA-guided NIR-FME and HD-WLE, following topical or systemic tracer administration, can be used to detect dysplastic and early EAC lesions in patients with BE. Our in vivo results show that even flat and difficult to distinguish lesions were identifiable with NIR-FME. Moreover, the topical tracer approach was able to improve early lesion detection by ~33% compared with HD-WL/NBI endoscopy.
Acknowledgments
The authors would like to thank research analyst W Boersma-van Ek for her assistance in the laboratory, especially for her contribution in the IHC staining and scoring process. Furthermore, they would like to thank Prof JJGHM Bergman for carefully reading the manuscript.
References
Footnotes
WBN and EH contributed equally.
Contributors WBN, EH, FTMP and JHK: involved in the clinical study design. WBN, EH, JJJT, MK and FTMP: enrolled patients, performed endoscopic procedures and/or acquired specimens. PBG-A, WBN and VN: involved in the development of the NIR-MFE system. MDL and AJS: involved in the GMP tracer production. AK: involved in pathological assessment and analyses of the ex vivo data. WBN and EH: drafted the manuscript. FTMP, GMvD and VN: critically revised drafts of the manuscript. WBN, GMvD and VN: designed the research concept and/or supervised all aspects of the research. All authors: had access to the study data and reviewed and approved the final manuscript.
Funding This work was financially supported by the Dutch Cancer Society: KWF Kankerbestrijding (RUG 2012-5416), The DFG Leibnitz Proze Award and via an unrestricted research grant for molecular imaging from SurgVision BV (The Netherlands).
Competing interests WBN and GMvD received an unrestricted research grant for molecular imaging development from SurgVision BV (the Netherlands). GMvD and VN are in the scientific advisory board of Surgvision BV. The other authors have no conflicts to declare.
Patient consent Obtained.
Ethics approval METc Groningen.
Provenance and peer review Not commissioned; internally peer reviewed.