Article Text

Statistics from Altmetric.com
Clinical presentation
A 53-year-old white European male builder presented emergently with haematemesis and melaena. Four months previously, he underwent an exploratory laparotomy, small bowel resection and anastomosis for a spontaneous jejunal perforation. His immediate postoperative course was uneventful. One month prior to this admission he lost the sight in his right eye because of a central retinal vein occlusion (CRVO): blood cultures, vasculitis and thrombophilia screens were negative and an echocardiogram and carotid Dopplers unremarkable. There was no significant family history. For the treatment of his CRVO, he was taking 15 mg of prednisolone daily and 150 mg of aspirin. He consumed 14 units of alcohol per week but did not smoke cigarettes.
Initial laboratory tests showed haemoglobin 103 g/L (normal range 130–180), mean corpuscular volume 97.6 fL (82–98) and lymphopenia 0.80×109/L (1.1–3.5). Tissue transglutaminase antibodies were 1.2 U/mL (0–10.0) with normal IgA levels and antiendomysial antibodies were negative.
Oesophagogastroduodenoscopy demonstrated a duodenal ulcer with a bleeding vessel that was clipped and injected with epinephrine. Four days later, however, he developed peritonitis that required an emergency laparotomy and small bowel resection (see figures 1–3).
Question
What was the diagnosis?

Macroscopic appearance of the small bowel.

H&E ×10 of small bowel mucosa.

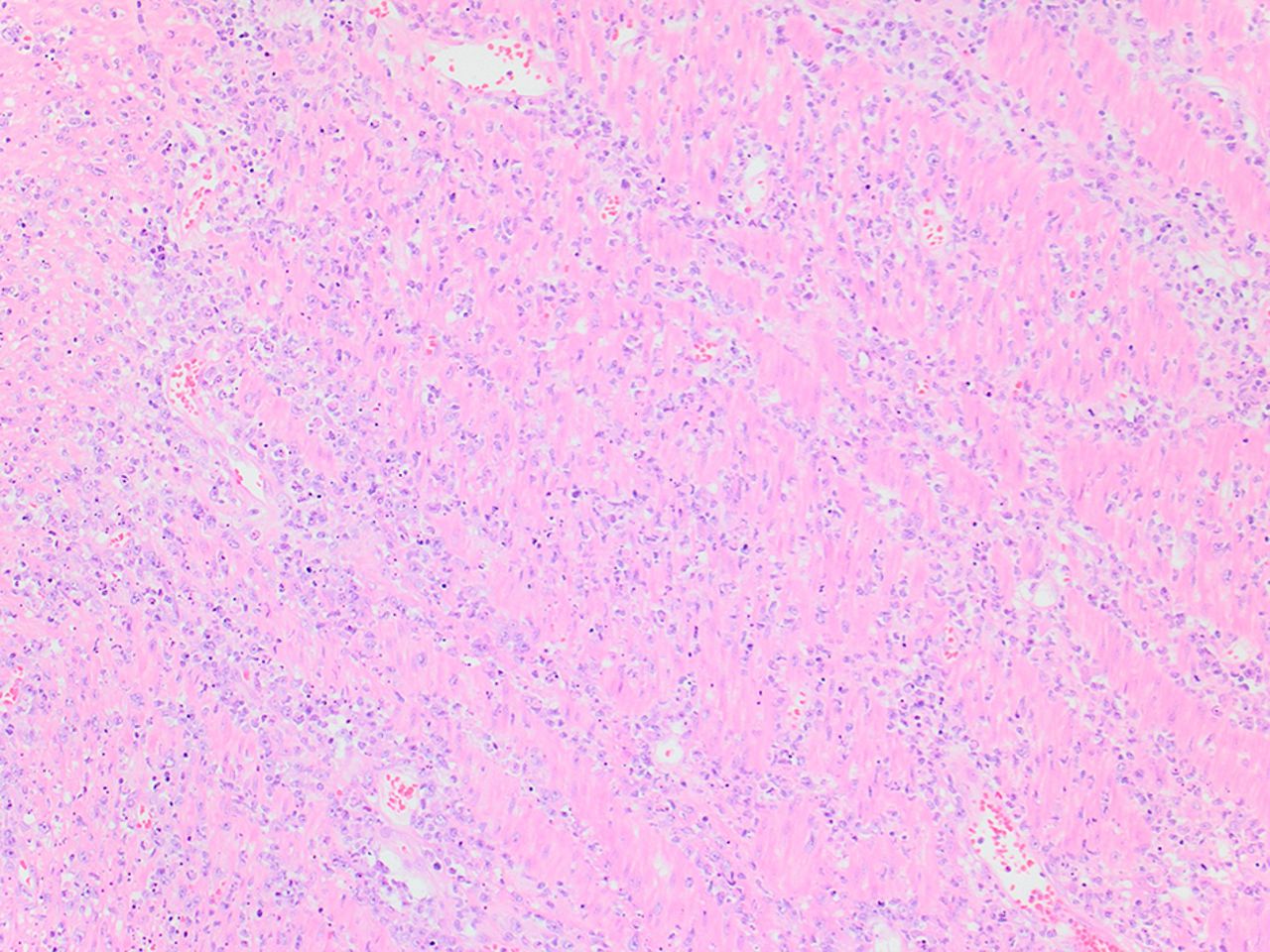
H&E ×40 of small bowel mucosa.
Answer
The small bowel macroscopically was thickened and oedematous with multiple perforations and abundant serosal exudate. The mucosa showed blunting of the intestinal villi with intraepithelial lymphocytosis (see figures 4 and 5): the immunophenotype was characteristic for type 1 refractory coeliac disease. A population of neoplastic T lymphocytes with a clonal cytotoxic immunophenotype were seen to invade the lamina propria indicating enteropathy-associated T cell lymphoma.

H&E ×10 showing areas of mucosa ulceration and wall of the perforation site with florid acute inflammation.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
H&E ×20 showing diffuse infiltration by a population of blasts with abundant apoptotic debris.
About one-third of patients diagnosed with small bowel lymphoma have evidence of proximal villous atrophy.1 Our patient was seronegative but carried the coeliac risk-serotype HLA-DQ2. Seronegative coeliac disease is rare among patients with coeliac disease but is a common cause of seronegative villous atrophy and is associated with high mortality.2 3 Enteropathy-associated T cell lymphoma is a rare form of extranodal T cell lymphoma that is usually, but not always, associated with untreated or undiagnosed coeliac disease.4 Patients are typically diagnosed in the sixth or seventh decade of life and are more often male. The jejunum is the most commonly affected part of the GI tract and the diagnosis is frequently made because of stricturing or perforation.4 The prognosis is poor: the estimated overall and treatment failure-free survival at 5 years is 20% and 4%, respectively.5
Footnotes
Contributors All authors were responsible to writing and reviewing final versions of the article. All were in agreement at submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators N A Kennedy.
Correction notice This article has been corrected since it published Online First. The second author’s name has been corrected.
Patient consent for publication Obtained.