Article Text

Statistics from Altmetric.com
Clinical presentation
A 45-year-old man developed multiple papules on the abdomen (with sizes of about 2–15 mm) for 9 months (figure 1), intermittent black stool and abdominal pain for 5 months. Colonoscopy revealed chronic inflammation of the colorectal mucosa (pathological results indicated active inflammation of the mucosa and Epstein-Barr virus positive) (figure 2). CT enterography examinations revealed segmental ileal stenosis in the right lower abdomen. The abdominal pain worsened 3 days before admission. Laboratory examinations during hospitalisation showed that C reactive protein was 31.53 ng/L; fibrinogen was 5.77 g/L and D-dimer was 1308 ng/mL, respectively. On the day of hospitalisation, the patient had sudden aggravation of abdominal pain without flatus and defecation. Physical examination showed abdominal tenderness, rebound pain and muscle tension. Abdominal X-ray indicated intestinal obstruction. Emergency laparotomy was performed. During the operation, a large number of gas, yellow faecal water and abscesses were seen. Multiple ischaemia and perforations in the small intestine (seven places) were detected.

Papules on the abdomen.
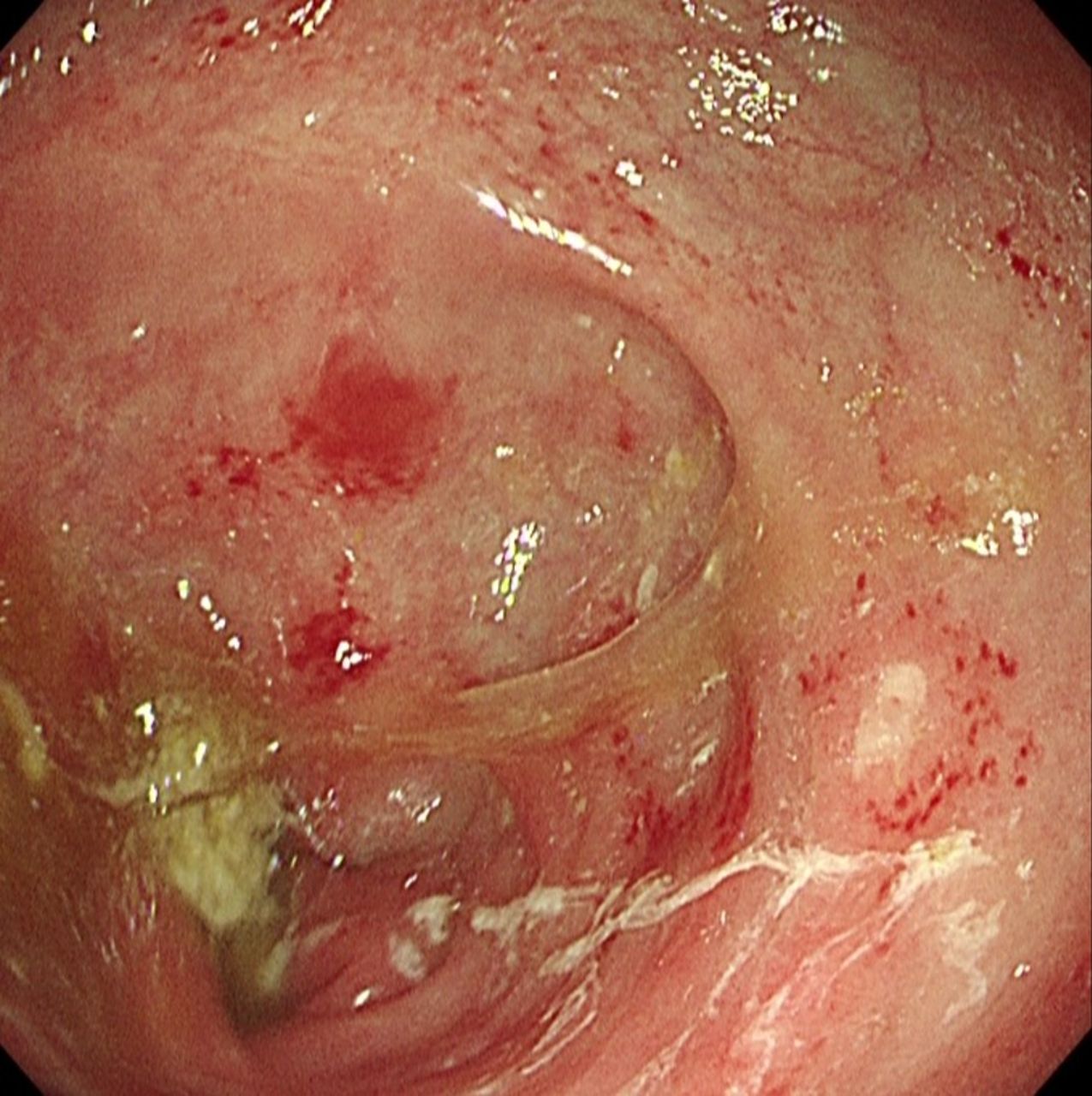
Chronic inflammation of the colorectal mucosa in the ileocecal region and rectosigmoid colon.
Question
What is the diagnosis?
Answer
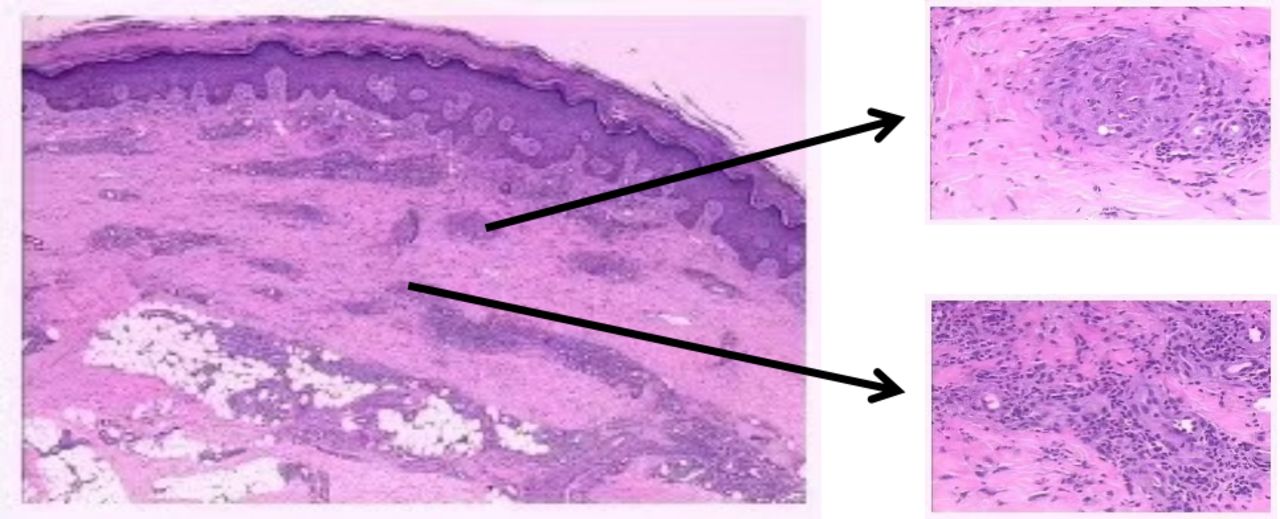
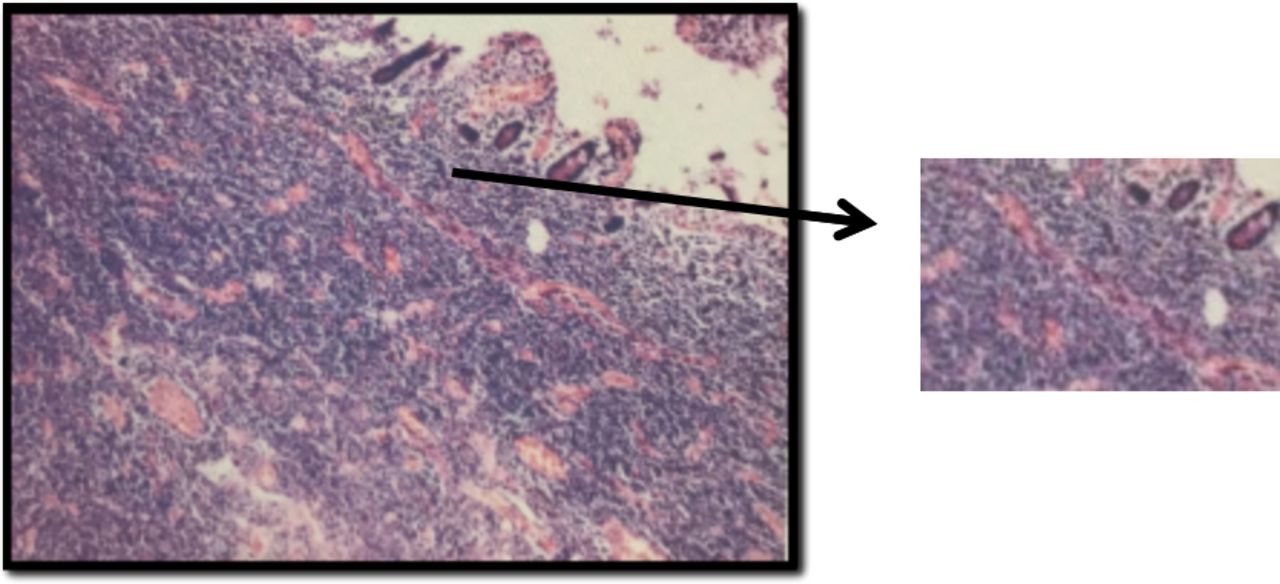
Postoperative pathology from the small intestine showed lymphocyte necrosis, collagen fibre swelling, degeneration and necrosis in the ischaemic area, and infarct ulcer (figure 3). Biopsy from skin lesions showed leucocytoclastic vasculitis, arteriolar obliteration, epidermal atrophy and disarrangement of the collagen fibres in the corium (figure 4). After comprehensive evaluation, the patient was diagnosed as Degos disease.

Postoperative pathology from the small intestine showing lymphocyte necrosis, collagen fibre swelling, degeneration and necrosis in the ischaemic area, and infarct ulcer.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Biopsy from skin lesions showing leucocytoclastic vasculitis, arteriolar obliteration, epidermal atrophy and disarrangement of the collagen fibres in the corium.
Degos disease is a rare vasculopathy that affects the lining of the medium and small veins and arteries, resulting in occlusion (blockage of the vessel) and tissue infarction. The aetiology of Degos disease remains unknown and is assumed to be related to autosomal dominant inheritance, abnormal autoimmunity, decreased fibrinolytic activity and lentivirus infection.1 The incidence is the highest in young and middle-aged men, usually involving the skin and intestines, and skin damage often occurs the first. It can involve the central nervous system, even the eyes, heart, kidney and bladder, but rarely.2 There is no specific treatment for this disease. Typically, the symptomatic treatment is recommended. If there is intestinal obstruction or perforation, an emergent surgery should be performed for its treatment, but the prognosis is poor. This patient developed a postoperative intestinal fistula, but the patient and his families refused a second surgery, and the patient was discharged from the hospital. During the telephone follow-up, we were informed that the patent had unfortunately died. The family did not know the exact reason of death, but we consider it might be related to haemorrhagic shock or septic shock because of the intestinal perforation.
Ethics statements
Patient consent for publication
Acknowledgments
The authors acknowledge the support to this study provided by Airforce Aoxiang Foundation and Young Changjiang Scholars of the Ministry of Education to JL.
Footnotes
Contributors All authors were involved in the conception and design of the study, analysed and interpreted the study data, critically reviewed the content of this article and approved the final version for submission.
Funding This work was supported by the National Scientific Foundation of China (nos. 81772650, 81322037, 81572302 and 81421003 to JL), Airforce Aoxiang Foundation and Young Changjiang Scholars of the Ministry of Education (JL).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.