Article Text

Statistics from Altmetric.com
Clinical presentation
A 33-year-old man presented with a 2-month history of dyspepsia and nausea. He had undergone kidney transplantation (KT) 22 years ago due to renal failure of unknown aetiology. He underwent peritoneal dialysis for 14 years due to recurrent renal failure. Fourteen months ago, he underwent a second KT from a living donor. After transplantation, he had been taking prednisolone and tacrolimus. Laboratory studies showed the following results: blood urea nitrogen, 11.0 mg/dL (normal range, 8.0–23.0 mg/dL); creatinine, 0.92 mg/dL (normal range, 0.7–1.2 mg/dL); total calcium, 11.1 mg/dL (normal range, 8.6–10.2 mg/dL); corrected calcium, 11.3 mg/dL; phosphate, 2.6 mg/dL (normal range, 2.5–4.5 mg/dL) and alkaline phosphatase, 156 U/L (normal range, 40–129 U/L).
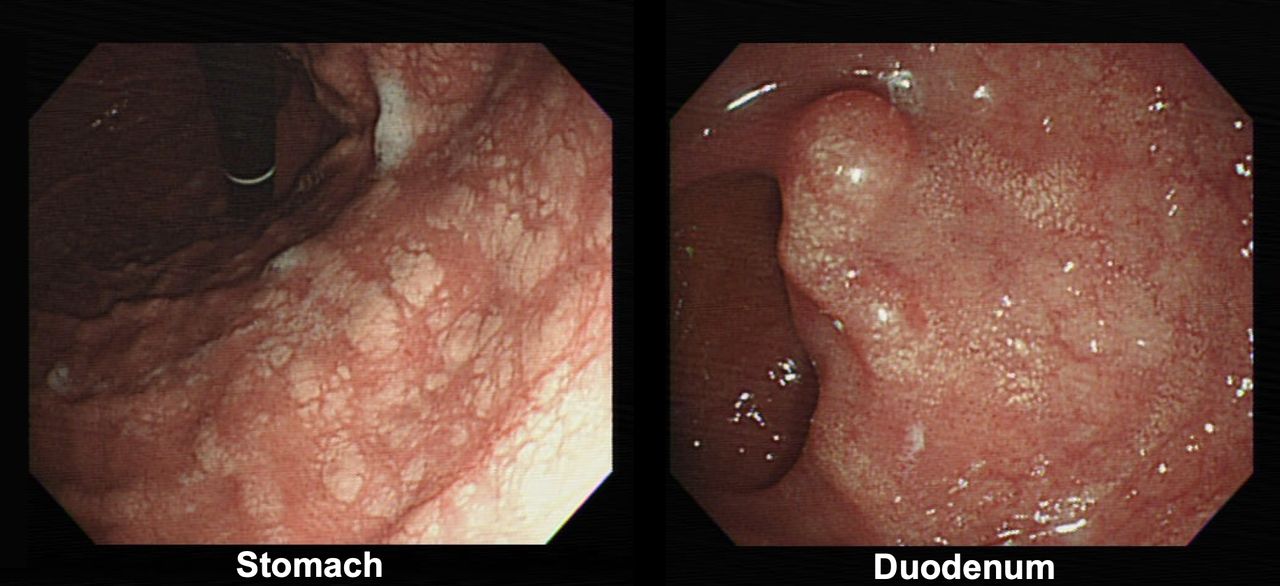
Upper endoscopy was performed to evaluate the patient’s nausea and dyspepsia. Multiple white flat plaques of various sizes and patch-like or nodule-like mucosal changes in a watermelon pattern were observed across the whole stomach. Small, shiny, white plaques were scattered across the bulb of the duodenum (figure 1). Biopsies were performed in the stomach and duodenum.

Gastric and duodenal lesions on oesophagogastroduodenoscopy.
Question
What is the most likely diagnosis?
Answer
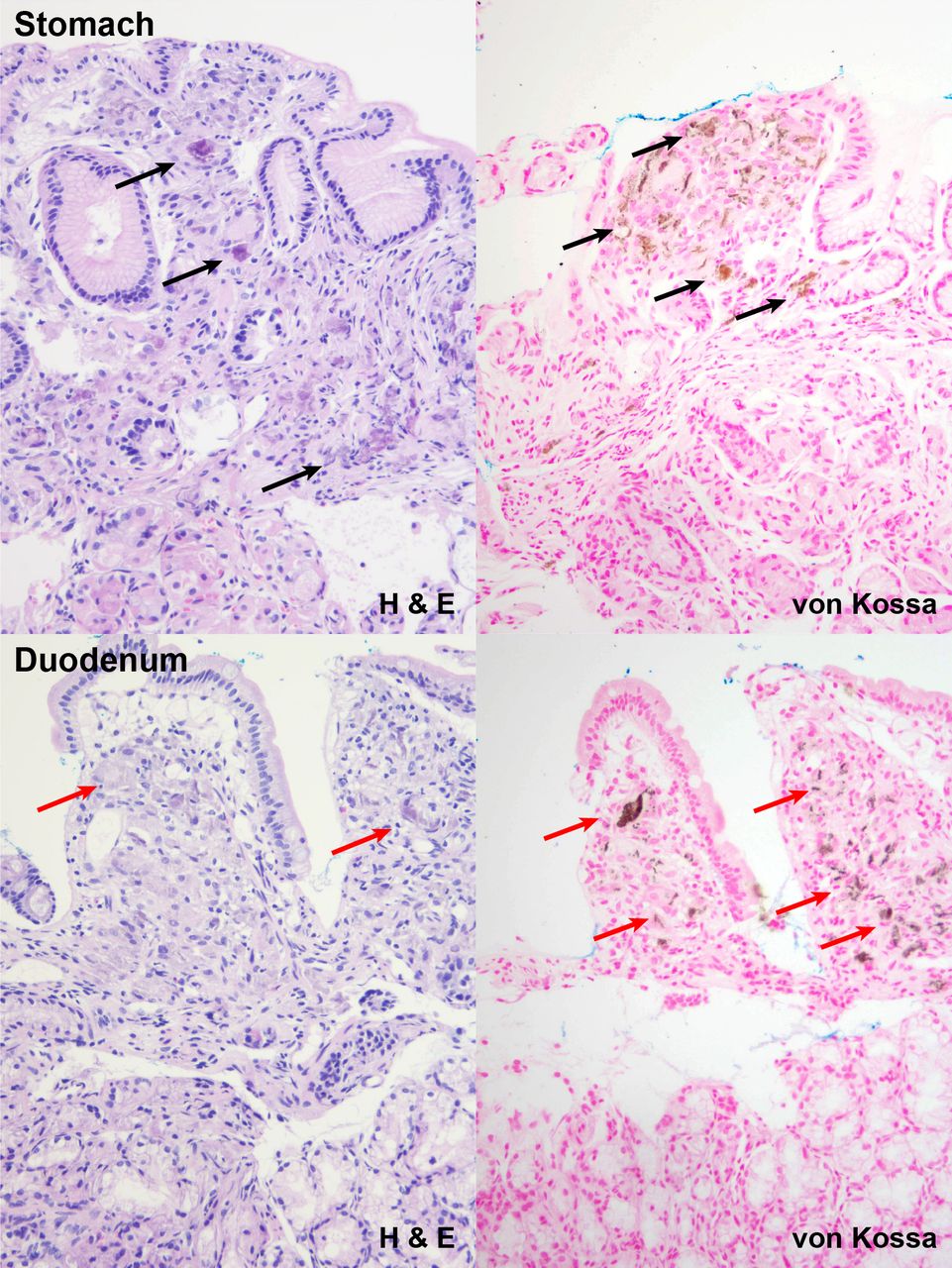
Histological evaluation demonstrated basophilic amorphous deposits predominantly in the superficial lamina propria of the gastric mucosa. Ill-defined, clumpy nodules consisting of homogeneous, fine calcified granules were noted. Positive results on von Kossa staining confirmed that these were calcium deposits (figure 2). The same microscopic findings were identified in the duodenal bulb. Therefore, histopathological findings were consistent with the diagnosis of metastatic gastric and duodenal mucosal calcinosis.

{kind=link}
{kind=link}
H&E and von Kossa stain showing calcium deposit.
Metastatic calcinosis is defined by calcium deposits on the mucosa of the GI tract due to elevated serum calcium levels.1 The most common cause is the alteration in serum calcium and phosphate levels due to renal disease.2 It is unclear how long electrolyte imbalance must be maintained to cause mucosal calcinosis. However, this patient exhibited persistent hypercalcaemia and hypophosphataemia for about a year after KT (before KT: total calcium, 9.3 mg/dL (corrected calcium, 9.6 mg/dL); phosphate, 4.8 mg/dL and parathyroid hormone, 203 pg/mL (normal range, 15–65 pg/mL)). There was no confirmed evidence of tertiary hyperparathyroidism at the pre-transplantation.
This alteration in serum electrolytes caused gastric and duodenal calcinosis, and the clinical prognosis of GI calcinosis was not clear. This is potentially fatal when the heart and lungs are involved.3 Thus, the endoscopists should consider the active evaluation if GI calcinosis is suspected in patients with long-term electrolyte imbalance.
Ethics statements
Patient consent for publication
Footnotes
Contributors JR contributed to editing images, reviewing the case and drafting the manuscript. C-KN contributed to drafting the manuscript and critically revising the manuscript. All the authors approved the final version of the article and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.