Article Text

Abstract
These guidelines provide a practical and evidence-based resource for the management of patients with Barrett's oesophagus and related early neoplasia. The Appraisal of Guidelines for Research and Evaluation (AGREE II) instrument was followed to provide a methodological strategy for the guideline development. A systematic review of the literature was performed for English language articles published up until December 2012 in order to address controversial issues in Barrett's oesophagus including definition, screening and diagnosis, surveillance, pathological grading for dysplasia, management of dysplasia, and early cancer including training requirements. The rigour and quality of the studies was evaluated using the SIGN checklist system. Recommendations on each topic were scored by each author using a five-tier system (A+, strong agreement, to D+, strongly disagree). Statements that failed to reach substantial agreement among authors, defined as >80% agreement (A or A+), were revisited and modified until substantial agreement (>80%) was reached. In formulating these guidelines, we took into consideration benefits and risks for the population and national health system, as well as patient perspectives. For the first time, we have suggested stratification of patients according to their estimated cancer risk based on clinical and histopathological criteria. In order to improve communication between clinicians, we recommend the use of minimum datasets for reporting endoscopic and pathological findings. We advocate endoscopic therapy for high-grade dysplasia and early cancer, which should be performed in high-volume centres. We hope that these guidelines will standardise and improve management for patients with Barrett's oesophagus and related neoplasia.
- BARRETT'S CARCINOMA
- BARRETT'S METAPLASIA
- BARRETT'S OESOPHAGUS
- OESOPHAGEAL CANCER
- GASTROESOPHAGEAL REFLUX DISEASE
Statistics from Altmetric.com
- BARRETT'S CARCINOMA
- BARRETT'S METAPLASIA
- BARRETT'S OESOPHAGUS
- OESOPHAGEAL CANCER
- GASTROESOPHAGEAL REFLUX DISEASE
Purpose and methods
The purpose of this guideline is to provide a practical and evidence-based resource for the management of patients with Barrett's oesophagus and related early neoplasia. This document is therefore aimed at gastroenterologists, physicians and nurse practitioners, as well as members of multidisciplinary teams (MDTs; surgeons, radiologists, pathologists), who take decisions on the management of such patients. The population covered by these guidelines includes: patients with gastro-oesophageal reflux disease or other risk factors for Barrett's (obesity, family history for Barrett's and oesophageal adenocarcinoma (OAC)); every patient with incident or prevalent Barrett's oesophagus regardless of their age, sex or comorbidities; patients with early OAC and patients with intestinal metaplasia (IM) at the gastro-oesophageal junction (GOJ) with no endoscopic evidence of Barrett's oesophagus. The previous British Society of Gastroenterology (BSG) guidelines were published in 2005 and since then there have been advances in the diagnostic and management tools available. Within these guidelines, we have systematically reviewed the literature in order to address controversial issues in Barrett's oesophagus and to formulate practical recommendations to guide patient management. In particular, we have covered the following key questions.
-
How should Barrett's oesophagus be defined and which patients should undergo regular surveillance?
-
Are there clinical features associated with increased cancer risk in Barrett's oesophagus, which should influence the frequency of endoscopic surveillance?
-
Are there diagnostic tools that should be utilised to screen the population at risk for Barrett's oesophagus?
-
Which imaging modality should be used for the endoscopic diagnosis and surveillance of Barrett's oesophagus?
-
How should we best manage dysplasia in Barrett's oesophagus?
-
Which staging modality is preferred for Barrett's-related early OAC?
-
What are the indications for endoscopic and/or surgical therapy in Barrett's-related adenocarcinoma?
-
Are there minimum standards for training and maintenance of skills in the field of endoscopic therapy?
-
How should patients be followed-up after endoscopic therapy?
-
Are there chemopreventive interventions recommended to reduce the likelihood of the progression of Barrett's oesophagus?
-
What are the priorities for research and development in the field of Barrett's carcinogenesis?
The Appraisal of Guidelines for Research and Evaluation (AGREE II) instrument1 was used to provide a methodological strategy for the development of the guidelines and to aid assessment of the quality of the guidelines. Three appraisers in the author list assessed the compliance of the guidelines to the AGREE II domains. As part of the AGREE II criteria, external review of this manuscript was also performed by two internationally renowned experts in the field (Dr L Lovat and Professor J Bergman). The authors comprised gastroenterologists, endoscopists, surgeons, pathologists, economists, public health physicians and patient representatives. Individuals were selected on the basis of their current membership of the relevant BSG committees or their expertise in the field in order to ensure representation across all the relevant disciplines. A working group was formed for each topic (working groups listed under Contributors) and the authors of that group were then responsible for conducting a comprehensive literature search to identify references relevant to individual topics. Studies were divided according to their methodologies (systematic reviews and meta-analyses, randomised controlled trials (RCTs), cohort studies, diagnostic studies and economic studies), and the rigour and quality of the study was evaluated using the SIGN checklist system (http://www.sign.ac.uk/methodology/checklists.html). The authors included as many studies as possible to support the evidence; however, studies with suboptimal quality were excluded, or included if they represented the only evidence to address particular clinical questions. Cohort studies with very small patient groups, feasibility studies, systematic reviews without meta-analysis and biomarker pilot discovery studies were excluded from evidence-generating literature, as well as studies with methodological flaws that were considered unacceptable after careful review. Evidence was finally scored using the North of England evidence-based guidelines2 as follows.
-
Ia: Evidence obtained from meta-analysis of RCTs.
-
Ib: Evidence obtained from at least one RCT.
-
IIa: Evidence obtained from at least one well-designed controlled study without randomisation.
-
IIb: Evidence obtained from at least one other type of well-designed quasi-experimental study.
-
III: Evidence obtained from well-designed descriptive studies such as comparative studies, correlative studies and case studies.
-
IV: Evidence obtained from expert committee reports, or opinions or clinical experience of respected authorities.
The literature search was performed for Nursing and Allied Health Literature (CINAHL) for English language articles published up until December 2012. We performed additional searches of Medline using the Ovid database, including Ovid Medline 1948 to the present and Ovid Medline (R) in-process and other non-indexed citations. The principal search terms were ‘Barrett's (o)esophagus’, ‘dysplasia’, ‘screening’, ‘surveillance’, ‘high-grade dysplasia’ (‘HGD’), ‘intramucosal carcinoma’, ‘radiofrequency ablation’, ‘endoscopic mucosal resection’, ‘photodynamic therapy’ (‘PDT’), ‘argon plasma coagulation’, ‘(o)esophagectomy’, ‘biomarkers’, ‘p53’, ‘model’, ‘economic’ and ‘Markov’. The panel graded each of the recommendations on the basis of the strength of the evidence, taking into consideration limitations of the studies and weighing the difference between the estimated benefits and risks of the intervention.
Therefore recommendations were graded as follows.
-
Grade A requires at least one RCT of good quality addressing the topic of recommendation.
-
Grade B requires the availability of clinical studies without randomisation on the topic of recommendation.
-
Grade C requires evidence from category IV in the absence of directly applicable clinical studies.
Recommendations were scored by each individual author on the basis of a five-tier system comprising the following agreement categories: A+, strong agreement; A, agree with reservation; U, undecided; D, disagree; D+, strongly disagree. Statements that failed to reach substantial agreement among authors, defined as >80% agreement (A or A+), on the first round of voting were revisited and modified according to authors’ comments. Further rounds of voting were then continued until substantial agreement (>80%) was reached. Online supplementary appendix 1 shows the percentage of authors’ agreement on individual statements and the number voting required to meet the minimum threshold of 80%.
Detailed attention has been paid to other published guidelines, in particular the American Gastroenterology Association (AGA) Medical position Statement,3 a recent systematic review with consensus statements (BADCAT)4 and National Institute of Health and Care Exellence (NICE) guidelines for management of dysplastic Barrett's,5 ,6 in order to try to align international practices and to aid useful comparisons of clinical outcomes for audit and research.
In formulating these guidelines, we took into consideration benefits and risks for the population and national health system as well as side effects. For example, we considered the benefits to the population derived from the reduction of the incidence and mortality for OAC achievable through screening, endoscopic surveillance for Barrett's and endoscopic therapy for dysplasia. We considered risks inherent in invasive interventions, such as endoscopic surveillance and therapy. We also took into account implications for the healthcare system, which can arise from expensive interventions, such as endoscopic screening or surveillance, and economic considerations using existing data in the field. We considered psychological morbidity and reduction of quality of life (QOL) resulting from repeated interventions (surveillance and endotherapy for dysplasia as a preventive measure for cancer development). Patient perspectives were taken into consideration by consulting with two patient representatives. These lay members were consulted from the outset to ensure that patient perspectives were taken into account during the literature review process and in deciding which topics should be addressed before the literature review process. Draft guidelines were then resubmitted to the lay members, and modifications made in accordance with their comments.
After completion, the guidelines underwent appraisal and external review in accordance with the AGREE II instrument, as discussed above. The recommendations were then posted on the BSG website for open consultation and reviewed by BSG and Association of Upper GI Surgeons (AUGIS) Clinical Services Committee reviewers before publication. It is anticipated that a thorough review of these guidelines will be required in about 5 years, and specific sections may need reviewing in the interim as new data emerge when results from the ongoing trials, such as Aspirin Esomeprazole Chemoprevention Trial (AspECT) (UKCRN ID 1339), BEST (UKCRN ID 9461), BOSS (UKCRN ID 4943) and SURF (NTR1198), are available.
Dissemination and implementation of the guidelines
These guidelines have been written to be as practical as possible and it is intended that this will be supplemented by endoscopic and histopathological images for educational purposes. Dissemination will be achieved through publication in the peer-reviewed journal Gut and through presentations at national BSG conferences as well as at relevant training courses. Some of the statements in these guidelines, particularly those concerning endoscopic therapy, are in line with NICE recommendations,6 ,7 which represent an additional source of guidance for the management of this disease. In this article, we have provided tables that should help guide practitioners to acquire the minimum dataset of clinical information in order to optimise patient management (endoscopy and pathology proforma) and ensure consistency among hospitals. There is also a patient information sheet explaining the diagnosis of Barrett's oesophagus (Appendix 4) and the latest surveillance recommendations. These can be easily adapted to individual clinical settings. Audit and monitoring of these guidelines will be carried out through users’ feedback on the BSG website forum (http://www.bsg.org.uk/forum). This is a list of elements in clinical practice that can be subjected to monitoring and auditing activity.
-
Adherence of endoscopists to the Seattle protocol
-
Use of a minimum dataset for endoscopy reporting
-
Use of a minimum dataset for pathology reporting
-
Revision of diagnoses of dysplasia by second GI pathologist
-
Adherence to recommendations for endoscopic surveillance
-
Volume of cases of endoscopic therapy to assess fitness of service provision
-
Safety and efficacy of endoscopic therapy for Barrett's dysplasia and early neoplasia
-
MDT discussion of cases with HGD and Barrett's early cancer
Executive summary of key recommendations
Diagnosis
-
Barrett's oesophagus is defined as an oesophagus in which any portion of the normal distal squamous epithelial lining has been replaced by metaplastic columnar epithelium, which is clearly visible endoscopically (≥1 cm) above the GOJ and confirmed histopathologically from oesophageal biopsies (Recommendation grade C).
-
The proximal limit of the longitudinal gastric folds with minimal air insufflation is the easiest landmark to delineate the GOJ and is the suggested minimum requirement (Recommendation grade B).
-
Endoscopic reporting should be performed using a minimum dataset including a record of the length using the Prague criteria (circumferential extent (C), maximum extent (M) of endoscopically visible columnar-lined oesophagus in centimetres and any separate islands above the main columnar-lined segment noted) (Recommendation grade B).
-
In order to improve the standard of care and to ease discussion between experts, the use of a minimum dataset is recommended to report histopathological findings (Recommendation grade C).
Screening for Barrett's oesophagus
-
Screening with endoscopy is not feasible or justified for an unselected population with gastro-oesophageal reflux symptoms (Recommendation grade B).
-
Endoscopic screening can be considered in patients with chronic GORD symptoms and multiple risk factors (at least three of age 50 years or older, white race, male sex, obesity). However, the threshold of multiple risk factors should be lowered in the presence of family history including at least one first-degree relative with Barrett's or OAC (Recommendation grade C).
Surveillance
-
Although RCT data are lacking, given the evidence from the published studies that surveillance correlates with earlier stage and improved survival from cancer, surveillance is generally recommended (Recommendation grade B).
-
Endoscopic monitoring with histopathological assessment of dysplasia is the only current method of surveillance with sufficient evidence to be recommended (Recommendation grade B).
-
Surveillance regimens should take into account the presence of IM and length of the Barrett's segment (Recommendation grade B).
-
Dysplasia confirmed by two GI pathologists is currently the best tissue biomarker for the assessment of cancer risk (Recommendation grade B).
-
Until randomised controlled evidence is available, biomarker panels cannot yet be recommended as routine of care (Recommendation grade C).
Practicalities of endoscopic surveillance
-
Patients should have early access to an outpatient clinic to be informed about a new diagnosis of Barrett's oesophagus and to have an initial discussion about the pros and cons of surveillance with written information provided (Recommendation grade C).
-
For a given patient, whether or not surveillance is indicated should be determined on the basis of an estimate of the likelihood of cancer progression and patient fitness for repeat endoscopies, as well as patient preference (Recommendation grade C).
-
High-resolution endoscopy should be used in Barrett's oesophagus surveillance (Recommendation grade C).
-
There is insufficient evidence to recommend transnasal endoscopy as a replacement for transoral endoscopy (Recommendation grade C).
-
Advanced imaging modalities, such as chromoendoscopy or ‘virtual chromoendoscopy’, are not superior to standard white light endoscopy in Barrett's oesophagus surveillance and are therefore not recommended for routine use (Recommendation grade A).
-
Adherence to a quadrantic, 2 cm biopsy protocol in addition to sampling any visible lesions is recommended for all patients undergoing surveillance. This should also apply to long segments (Recommendation grade B).
-
Surveillance is generally not recommended in patients with IM at the cardia or in those with an irregular Z-line regardless of the presence of IM (Recommendation grade C).
-
For patients with Barrett's oesophagus shorter than 3 cm, without IM or dysplasia, a repeat endoscopy with quadrantic biopsies is recommended to confirm the diagnosis. If repeat endoscopy confirms the absence of IM, discharge from surveillance is encouraged as the risks for endoscopy probably outweigh the benefits (Recommendation grade C).
-
Patients with Barrett's oesophagus shorter than 3 cm, with IM, should receive endoscopic surveillance every 3–5 years (Recommendation grade C).
-
Patients with segments of 3 cm or longer should receive surveillance every 2–3 years (Recommendation grade C).
Histopathological diagnosis of dysplasia
-
Given the important management implications for a diagnosis of dysplasia, we recommend that all cases of suspected dysplasia are reviewed by a second GI pathologist, with review in a cancer centre if intervention is being considered (Recommendation grade C).
-
Given the difficulties associated with the management of the ‘indefinite for dysplasia’ category, all such cases should also be reviewed by a second GI pathologist, and the reasons for use of the ‘indefinite for dysplasia’ category should be given in the histology report in order to aid patient management (Recommendation grade C).
-
The addition of a p53 immunostain to the histopathological assessment may improve the diagnostic reproducibility of a diagnosis of dysplasia in Barrett's oesophagus and should be considered as an adjunct to routine clinical diagnosis (Recommendation grade B).
Management of dysplasia and early cancer
-
Patients with a diagnosis of indefinite for dysplasia should be managed with optimisation of antireflux medication and repeat endoscopy in 6 months. If no definite dysplasia is found on subsequent biopsies, then the surveillance strategy should follow the recommendation for non-dysplastic Barrett's oesophagus (Recommendation grade C).
-
Management of low-grade dysplasia (LGD) is unclear in view of limited data about the natural history. It is essential that the diagnosis is confirmed by two pathologists, and patients should be surveyed endoscopically at 6 monthly intervals. Currently, ablation therapy cannot be recommended routinely until more data are available (Recommendation grade C).
-
Expert high-resolution endoscopy (HRE) should be carried out in all Barrett's patients with biopsy-detected HGD in order to detect visible abnormalities suitable for endoscopic resection (ER) (Recommendation grade B).
-
Visible lesions should be considered malignant until proven otherwise (Recommendation grade C).
-
Description of lesion morphology using the Paris classification gives an indication of the likelihood of invasive cancer and aids communication between clinicians. This should therefore be used for all visible lesions but cannot at present be used to predict prognosis (Recommendation grade C).
-
All patients with dysplasia or early cancer, for whom therapy is considered, should be discussed at the specialist MDT for oesophago-gastric cancer. This team should include an interventional endoscopist, upper GI cancer surgeon, radiologist and a GI pathologist (minimum standard) (Recommendation grade C).
-
Patients with dysplasia or early cancer should be informed of treatment options and have access to consultation with all specialists as required (Recommendation grade C).
Endoscopic therapy for Barrett's-related neoplasia
-
For HGD and Barrett's-related adenocarcinoma confined to the mucosa, endoscopic therapy is preferred over oesophagectomy or endoscopic surveillance (Recommendation grade B).
-
Endoscopic therapy of Barrett’s neoplasia should be performed at centres where endoscopic and surgical options can be offered to patients (Recommendation grade C).
-
A minimum of 30 supervised cases of ER and 30 cases of endoscopic ablation should be performed to acquire competence in technical skills, management pathways and complications (Recommendation grade C).
-
ER should be performed in high-volume tertiary referral centres. Radiofrequency ablation (RFA) should be performed in centres equipped with ER facilities and expertise (Recommendation grade C).
ER for Barrett's-related neoplasia associated with visible lesions
-
Endoscopic assessment will usually identify the area with the most advanced neoplasia. ER should aim to resect all visible abnormalities (Recommendation grade C).
-
ER is recommended as the most accurate staging intervention for Barrett's early neoplasia (Recommendation grade B).
-
ER should be considered the therapy of choice for dysplasia associated with visible lesions and T1a adenocarcinoma (Recommendation grade B).
-
For patients at high surgical risk, endoscopic therapy can be offered as an alternative to surgery for treatment of good prognosis T1b adenocarcinomas (T1b sm1, well differentiated and without lymph vascular invasion) (Recommendation grade C).
-
For T1b adenocarcinomas with involvement of the second submucosal layer or beyond (T1b sm2-sm3), endoscopic therapy should not be considered curative (Recommendation grade B).
-
The cap and snare technique with submucosal injection and the band ligation technique without submucosal injection are considered to be equally effective (Recommendation grade A).
Pathology reporting of ER
-
Use of a minimum dataset for the reporting of ER specimens is recommended to ensure that all prognostic information is included in reports (Recommendation grade C).
-
The presence of tumour cells at the deep margin indicates incomplete resection and warrants further treatment (Recommendation grade C).
Imaging for HGD and T1 carcinoma: role of CT–positron emission tomography (PET) and endoscopic ultrasound (EUS)
-
Before ER, neither CT nor PET–CT have a clear role in the staging of patients with Barrett's HGD or suspected T1 cancer and neither is routinely required (Recommendation grade B).
-
Since EUS can both overstage and understage T1 lesions, its routine use cannot be recommended for staging before ER for suspected early lesions (Recommendation grade B).
-
In selected cases where the endoscopist cannot exclude advanced stage on the basis of the endoscopic appearance of nodular lesions, EUS with or without fine needle aspiration (FNA) is recommended to inform the therapeutic decision (Recommendation grade C).
-
EUS with or without FNA of visible lymph nodes is recommended in selected cases with T1b (sm1) disease on staging ER for which endoscopic therapy is selected, because of the significant risk of lymph nodal involvement (Recommendation grade C).
Ablative therapy for flat HGD and residual Barrett's after ER
-
In the presence of HGD or intramucosal cancer without visible lesions (flat HGD/intramucosal cancer), these should be managed with an endoscopic ablative technique (Recommendation grade A).
-
There are few comparative data among ablative techniques, but RFA currently has a better safety and side-effect profile and comparable efficacy (Recommendation grade C).
-
Eradication of residual Barrett's oesophagus after focal ER reduces the risk of metachronous neoplasia and is recommended (Recommendation grade B).
-
Endoscopic follow-up is recommended after endoscopic therapy of Barrett's neoplasia, with biopsies taken from the GOJ and within the extent of the previous Barrett's oesophagus (Recommendation grade B).
Surgical management of early Barrett's neoplasia
-
Surgical therapy is considered the treatment of choice for early adenocarcinoma that has extended into submucosa because of the significant risk of lymph node metastasis (Recommendation grade B).
-
Oesophagectomy should be performed in high-volume centres, as these are associated with lower in-hospital mortality than low-volume centres (Recommendation grade B).
-
There is currently no evidence to support one technique of oesophagogastrectomy over another. It is recommended that the procedure is tailored to the particular case and the expertise available in that centre (Recommendation grade C).
-
There are not sufficient data to recommend endoscopic surveillance after oesophagectomy for HGD or T1 adenocarcinoma provided that surgery has removed all the Barrett's mucosa. Until further evidence is available, endoscopy should be performed on a symptomatic basis (Recommendation grade C).
Documentation and audit of treatment for HGD and early cancer
-
Findings and management decisions for HGD and early cancer should be entered into the National Audit (Recommendation grade C).
Economic considerations
-
There are insufficient data to indicate that endoscopic screening and surveillance for Barrett's oesophagus are cost-effective. Further studies on non-endoscopic diagnostic methods are awaited (Recommendation grade C).
-
Endoscopic therapy for dysplastic Barrett's oesophagus and early OAC is cost-effective compared with oesophagectomy (Recommendation grade B).
Strategies for chemoprevention and symptom control
-
There is not yet sufficient evidence to advocate acid-suppression drugs as chemopreventive agents (Recommendation grade C).
-
Use of medication to suppress gastric acid production is recommended for symptom control (Recommendation grade A).
-
Proton pump inhibitors (PPIs) have the best clinical profile for symptomatic management (Recommendation grade A).
-
Antireflux surgery is not superior to pharmacological acid suppression for the prevention of neoplastic progression of Barrett's oesophagus (Recommendation grade C).
-
Antireflux surgery should be considered in patients with poor or partial symptomatic response to PPIs (Recommendation grade A).
-
There is currently insufficient evidence to support the use of aspirin, non-steroidal anti-inflammatory drugs (NSAIDs) or other chemopreventive agents in patients with Barrett's oesophagus (Recommendation grade C).
Patient perspective
-
All patients should be offered an appointment to discuss management decisions. When intervention is considered, therapeutic options should be discussed with an endoscopist as well as a surgeon (Recommendation grade C).
Future developments
The following developments would revolutionise the care of individuals with Barrett's oesophagus and should be priorities for policy makers and funders.
-
A non-endoscopic test(s) for diagnosis and surveillance
-
Studies to determine whether surveillance actually reduces mortality
-
Better understanding of the impact of screening and surveillance on QOL
-
More research into the use of advanced imaging modalities to improve dysplasia detection and cost-effectiveness of surveillance
-
Better risk stratification biomarkers to augment or replace the reliance on a histopathological assessment of dysplasia and better inform the indication for endoscopic ablative therapy
-
More studies on the natural history of Barrett's oesophagus, especially in the context of very short segments of columnar lined epithelium, LGD and cases with particular molecular profiles
-
Research is required to inform the debate surrounding whether patients with LGD or no dysplasia should receive ablation therapy
-
Evidence that endoscopic therapies are durable and do not require long-term endoscopic monitoring or that long-term surveillance can be replaced with a cost-effective non-endoscopic technique
-
Studies to further delineate the role of chemoprevention
-
Health-economic studies should be performed in parallel with trials to evaluate new management algorithms
-
Effects of current and future care pathways on patient QOL should be formally evaluated.
Introduction and historical perspective
Since the original eponymous description in 1950, there have been numerous definitions of the condition, Barrett's oesophagus, which have led to difficulties in diagnosis and management as well as hampering comparison between research studies. Between 1950 and 1970, it was established that Barrett's oesophagus is an acquired condition occurring in response to gastro-oesophageal reflux leading to a columnar lined distal oesophagus.8–10 It then became apparent that this entity embraced a spectrum of at least three different cellular types, which commonly occur as a mosaic. These are principally a gastric fundic-type (oxyntocardiac) epithelium comprising mucus-secreting, parietal and chief cells, a cardiac-type (transitional) mucosa comprising almost entirely mucus-secreting cells, and an intestinal type characterised by goblet cells.11 A multilayered columnar epithelium is also described, possibly specific for an early phase in the development of Barrett's oesophagus.12
The association with adenocarcinoma was established in the 1970s, and, as a result of this endoscopic surveillance, protocols have been introduced. However, there has been significant debate surrounding which features of Barrett's oesophagus predispose to malignant conversion and hence which patients should be classified as having Barrett's oesophagus and the frequency of follow-up advised. For example, the length of the Barrett's segment (ultra-short, short and long) and the different cellular subtypes (gastric or intestinal) have been subclassified over the years with different recommendations emerging over time and between different countries and specialist societies. More recently, there has been interest in whether the relative contribution of individual lifestyle, inherited factors and molecular alterations of the tissue might also alter the potential for malignant conversion.
Diagnosis
Definition summary
In these guidelines, we have taken the view that the basic definition should be descriptive of the acquired metaplastic state and clearly separated from the question of malignant potential. The estimated likelihood of cancer development is an evolving area, which the working group felt should be assessed on the basis of a synthesis of the endoscopic, histopathological and molecular features according to the current evidence in order to inform the precise follow-up or surveillance recommendations.
Barrett's oesophagus is defined as an oesophagus in which any portion of the normal distal squamous epithelial lining has been replaced by metaplastic columnar epithelium, which is clearly visible endoscopically (≥1 cm) above the GOJ and confirmed histopathologically from oesophageal biopsies (Recommendation grade C).
Endoscopic diagnosis of Barrett's oesophagus and irregular Z-line
Defining the GOJ
At the present time, the gold standard diagnostic tool for Barrett's oesophagus is endoscopy. The term endoscopy here refers to standard transoral endoscopy; however, transnasal endoscopy has also been investigated and recently been proven to be an accurate and well-tolerated alternative.13 ,14 Transnasal endoscopy has been shown to have a sensitivity and specificity of 98% and 100%, respectively, for the endoscopic diagnosis of Barrett's oesophagus when compared with standard endoscopy in the study of Shariff and coworkers13 (Evidence grade Ib). The role of transnasal endoscopy in Barrett's oesophagus surveillance is a different question and will be discussed below.
At endoscopy, in order to ascertain whether there is a columnar-lined segment in the lower oesophagus, it is essential to accurately delineate the GOJ. This can be achieved by visualising the distal end of the palisade vessels, which lie in the oesophageal mucosa but penetrate the submucosal layer at the level of the GOJ,15 or by delineating the proximal end of the gastric folds16 ,17 (Evidence grade III). Theoretically, the two landmarks should coincide at the GOJ; however, the presence of oesophagitis, the degree of insufflation, vascular anatomical variants of the oesophageal vessels, as well as respiration and peristalsis can make the correspondence between these two landmarks inconsistent.3 In a study comparing these two diagnostic methods, the palisading criteria resulted in an overall poor diagnostic reproducibility with a κ value of 0.14; endoscopic experience had no impact on the level of agreement.18 After an explanation of the Prague C&M Criteria (see below) using the gastric folds, there was a statistically significant improvement in diagnostic agreement (Evidence grade III).
Barrett's oesophagus should be endoscopically distinguished from an irregular Z-line, whereby the squamocolumnar junction appears with tongues of columnar epithelium shorter than 1 cm and with no confluent columnar-lined segment. In a case–control study, an irregular Z-line has been found with higher frequency in patients with reflux disease19 (Evidence grade IIa). Although one study found that about 40% of cases of irregular Z-line harboured IM on biopsy samples, the significance of this endoscopic finding is still unclear20 (Evidence grade III). Online supplementary appendix 2 shows examples of normal GOJ and irregular Z-lines in contrast with clearly visible Barrett's.
The proximal limit of the longitudinal gastric folds with minimal air insufflation is the easiest landmark to delineate the GOJ and is the suggested minimum requirement (Recommendation grade B).
Documentation of endoscopic findings (proforma of minimum dataset)
It is important to measure the length and shape of the columnar-lined segment using a standardised methodology in order to aid communication between clinicians and to help determine the level of diagnostic confidence and the perceived risk of adenocarcinoma development, which can alter with segment length as discussed below (table 1). It is appreciated that distinguishing between an irregular Z-line within physiologically normal limits and a short tongue of columnar-lined mucosa can be very difficult. Endoscopists need to ensure that they have carefully delineated the GOJ as discussed above and, if uncertain about whether the appearance of an irregular Z-line is sufficient to support a confident endoscopic diagnosis of Barrett's oesophagus, then an endoscopic diagnosis of Barrett's oesophagus should not be made. As stated in the definition ‘columnar epithelium should be clearly visible endoscopically above the gastro-oesophageal junction’. Since the diagnosis of an irregular Z-line is subjective and there is no accepted length cut-off to distinguish between an irregular Z-line and Barrett's oesophagus, we would suggest that 1 cm (M of Prague criteria) should be the minimum length for an endoscopic diagnosis of Barrett's (Evidence grade IV). Biopsies are generally not recommended if there is an irregular Z-line. However, according to the degree of suspicion, biopsies may be performed to aid the diagnosis. If the biopsy specimens are taken within an irregular Z-line, with no clear endoscopic evidence of Barrett's, they should be then labelled as GOJ and not oesophageal biopsy samples. Since the presence of pure fundic/oxyntic mucosa is a very rare finding in Barrett's oesophagus, this pathological finding would suggest sampling of the GOJ (see section on ‘Minimum dataset for histopathology diagnosis and clinicopathological correlation’).
Minimum endoscopic dataset required when reporting the finding of Barrett's oesophagus
The Prague C&M classification for Barrett's length is based on validated, explicit, consensus-driven criteria.21 The International Working Group for Classification of Oesophagitis (IWGCO) developed criteria including assessment of the circumferential (C) and maximal (M) extent of the endoscopically visualised Barrett's segment, as well as endoscopic landmarks such as the diaphragmatic hiatal pinch and the proximal extent of the gastric folds. Video recordings were scored by an international panel of 29 endoscopists, and the overall reliability coefficients for endoscopic recognition of Barrett's ≥1 cm was 0.72, whereas for Barrett's <1 cm, it was 0.22. The reliability coefficients for recognising the location of the GOJ and the diaphragmatic pinch were 0.88 and 0.85, respectively (Evidence grade III). These findings have been reproduced in different patient populations22 ,23 and have recently been validated in a multicentre study24 (Evidence grade III). The Prague classification includes recording as subtext the presence of Barrett's islands, which are increasingly prevalent after endoscopic therapy. In future, a modification of the Prague classification may provide an easier system for recording columnar-lined epithelium that is not continuous with the squamocolumnar junction. The presence and location of visible lesions should also be recorded according to the Paris classification25 in order to improve lesion recognition at the time of endoscopic therapy. Information on the number of biopsy samples taken is necessary to assess the quality of a surveillance endoscopy.
Endoscopic reporting should be performed using a minimum dataset including a record of the length using the Prague criteria (circumferential extent (C), maximum extent (M) of endoscopically visible columnar-lined oesophagus in centimetres and any separate islands above the main columnar-lined segment noted) (Recommendation grade B).
Biopsy protocol and site mapping
The Seattle biopsy protocol, which entails four-quadrant random biopsies every 2 cm in addition to targeted biopsies on macroscopically visible lesions, is recommended at the time of diagnosis and at subsequent surveillance 26 (Evidence grade III). If a patient is unable to tolerate this procedure at the initial diagnostic evaluation, often performed under local anaesthetic spray, then it is recommended that the patient is brought back at the earliest opportunity for further evaluation including the full biopsy protocol in order to inform further management.
Targeted biopsy samples from visible lesions should be taken before random biopsies. Distal areas should be biopsied first starting 1–2 cm above the GOJ and advancing proximally to minimise obscured view from bleeding.
Histopathological diagnosis
Histological features indicative of an oesophageal origin of the biopsy specimens
From a histopathological perspective, it has been proposed that: ‘the true GOJ is distal to the end of the tubular oesophagus and proximal to rugal folds as shown by the presence of submucosal oesophageal glands in this region’. Hence, the distinction between columnar-lined oesophagus and IM at the gastric cardia (CIM) can only be made definitively histologically when columnar mucosa with or without IM is seen juxtaposed with native anatomical oesophageal structures such as submucosal glands and/or gland ducts.27–29 Reports also suggest that multilayered epithelium or squamous islands are helpful, as the former is reported as pathognomonic of Barrett's, and the latter are almost always seen in continuity with the superficial portion of gland ducts.12 ,28 ,30 In large studies, however, native structures are seen in only 10–15% of biopsy samples and therefore are present in less than one in six diagnostic procedures; a definitive oesophageal or gastric origin can only therefore be determined in the minority of biopsy samples.27 ,31 ,32 The great majority of samples may include columnar mucosa of cardiac, oxyntic or intestinal type, often juxtaposed with squamous mucosa, but lacking native structures. The presence of IM in these is highly corroborative but not specific for a diagnosis of Barrett's oesophagus, as CIM cannot be confidently ruled out (see below). Owing to the relative paucity of native structures, it is no longer considered helpful to classify these patients separately as in the previous guidelines. However, this information should be recorded, and the diagnosis of Barrett's oesophagus should take into account the degree of confidence based on a combined analysis of endoscopic and histopathological criteria.
The relevance of IM
IM in Barrett's is most commonly of an incomplete (type II or III) subtype comprising mucous cells and goblet cells, although a complete type (type I with absorptive cells) may also be seen.33 ,34
There is a body of evidence to suggest that, of the types of metaplastic columnar epithelium in the oesophagus, intestinal is the most biologically unstable with the greatest risk of neoplastic progression through dysplasia to adenocarcinoma. This comes from early pathological studies35 ,36 and more recent population-based studies37 (Evidence grade III). It is this evidence that has led the AGA to conclude in their most recent guidelines that: ‘for the purposes of this statement the definition of Barrett's esophagus is the condition in which any extent of metaplastic columnar epithelium that predisposes to cancer development replaces the stratified squamous epithelium that normally lines the distal esophagus. Presently intestinal metaplasia is required for the diagnosis of Barrett's metaplasia because intestinal metaplasia is the only one of the three types of oesophageal columnar epithelium that clearly predisposes to malignancy.’… ‘therefore we suggest that the term ‘Barrett's oesophagus’ presently should be used only for patients who have intestinal metaplasia in the esophagus’.
This AGA definition of Barrett's oesophagus is at odds with the definition in previous BSG guidelines38 (BSG 2005) because of concern that confirmation of the presence of IM can be limited by sampling error in mucosal biopsy samples. In a study by Harrison et al39 of 1646 biopsy samples from 125 patients with long-segment Barrett's oesophagus, the optimum number of samples needed to demonstrate goblet cells in 67.9% of endoscopies was eight, but, in contrast, if only four were obtained, only 34.7% of endoscopies yielded a positive result for identification of goblet cells. Thus there are some data to show that the chance of detecting goblet cells is maximised by taking a minimum of eight samples throughout the Barrett's segment (Evidence grade III). In addition, Gatenby et al40 found that, although the rate of development of dysplasia and cancer in patients without IM at index biopsies (n=322) was equal to that of patients with IM (n=612), they also found that >50% of the patients without IM had evidence of IM at the 5-year follow-up and >90% were diagnosed with IM at 10 years (Evidence grade III). These two studies indicate that a single endoscopy with a low number of biopsy samples is not sufficient to exclude IM, particularly in a short segment of Barrett's oesophagus.
Two additional studies challenged the notion that IM is the most biologically unstable type of columnar metaplasia in the oesophagus. Takubo et al41 carefully analysed the columnar mucosa adjacent to 141 early OACs resected endoscopically and found that fewer than half of them showed evidence of IM, concluding that cancer may also arise in a non-intestinalised columnar epithelium (Evidence grade III). This study, however, does not indicate whether these patients had evidence of IM in the remainder of their Barrett's segment and therefore one cannot exclude the possibility that cancer may be associated with loss of intestinal differentiation. In a retrospective study, Kelty and colleagues found that the cancer risk in a historical cohort of 379 patients with oesophageal IM was similar to a group of 319 patients with columnar-lined oesophagus without IM (Evidence grade III).42 This study, however, lacks information about endoscopic findings and whether patients without IM did go on to develop IM during later surveillance. In keeping with data from these studies, there is also evidence that the non-goblet columnar epithelium may harbour similar molecular abnormalities to goblet cell epithelium.43–46
On the other hand, the recent population-based study from the Northern Ireland register found that the annual incidence of HGD and cancer in patients with IM is significantly higher than in those without IM (0.38% vs 0.07%).37 Even though this study has some of the same limitations as the study of Kelty et al, it is a population study with over 8000 patients, of which 40% had documented endoscopic evidence of Barrett's oesophagus, and 20% had information on the length of Barrett's (Evidence grade III). In addition, there was no significant difference in the cancer incidence between patients with and without endoscopic correlation, suggesting that the absence of endoscopy data in 60% of the cohort is unlikely to affect the overall results.
For these reasons, even though the insistence of the identification of IM to define or confirm a diagnosis of Barrett's oesophagus is problematic, it is recognised that the inclusion of gastric-type mucosa in short tongues of columnar-lined oesophagus is of less clinical importance in terms of the likelihood of malignant transformation and has the potential to greatly influence the frequency of diagnosis of Barrett's oesophagus at index endoscopy and the number of patients entering into follow-up and surveillance programmes. This may in turn profoundly influence our understanding of the natural history and biology of the condition. However, whether or not IM is present can be taken into consideration when determining the frequency and necessity of follow-up of patients. Hence, we suggest that the presence of IM is not a prerequisite for the definition of Barrett's oesophagus, but should be taken into account when deciding on the clinical management, as discussed in the surveillance section.
Distinguishing between true Barrett's oesophagus and IM of the cardia
It is not recommended that biopsy specimens from the cardia are taken routinely. However, if there is concern about the appearance at that site or if specimens are taken in patients having ablation therapy, then the following considerations need to be taken into account. Differentiation of oesophageal IM from IM of the proximal stomach (‘cardia’) in a mucosal biopsy sample from the GOJ region on morphological grounds is difficult in most circumstances, apart from when oesophageal native structures are seen. The different forms of IM may occur at both sites, and, similarly, studies suggesting a distinctive type of cytokeratin 7 and 20 immunocytochemical staining in Barrett's have not been sufficiently reproducible to apply in routine settings.27 ,47–50 In view of the lack of reliable markers to distinguish between IM of the cardia and oesophagus, this distinction needs to be made endoscopically, and the endoscopist is therefore required to carefully label the site from which biopsy samples were taken in reference to the endoscopic landmarks, in order to inform the clinico–pathological correlation.
Minimum dataset for histopathology diagnosis and clinicopathological correlation
The histopathological information needs to be integrated with the endoscopic findings in order to reach an accurate clinical diagnosis and determine the ramifications for follow-up. The pathologist should record the following elements in the histopathological report:
-
number of biopsy samples analysed at each level;
-
the type of mucosa present (squamous or columnar);
-
the presence of any native oesophageal structures;
-
the presence of gastric- (cardiac/fundic) or intestinal-type metaplasia;
-
the presence and grade of dysplasia.
This minimum dataset is recommended to standardise the histopathological reporting for Barrett's oesophagus and to ensure that all the information required for the assessment of disease is included. This dataset can be incorporated into a proforma to facilitate the interpretation of the report, which is particularly encouraged in the presence of dysplasia. Examples of a short proforma (figure 1) and a more comprehensive proforma (figure 2) are given, which may be adapted to suit particular clinical settings and practice.

Example of a short proforma for reporting histopathology diagnosis and surveillance biopsy findings. This could be adapted to suit your locality.

Example of a comprehensive proforma for reporting histopathology diagnosis and surveillance biopsy findings.
We have taken the decision to abandon the previous nomenclature from the 2005 guidelines, since, although academically appealing, it was cumbersome and the distinction between ‘diagnostic’, ‘corroborative of’ and ‘in keeping with’ are difficult to remember. In particular, as discussed above, although native oesophageal structures do identify the oesophageal origin of the biopsy samples, these only occur in a minority and hence cannot be relied upon to help reach a diagnosis.
In the context of biopsy specimens confidently labelled by the endoscopist as being taken within the tubular oesophagus and in the presence of endoscopically visible Barrett's oesophagus, the following diagnostic terms are advocated:
-
‘Barrett's oesophagus with gastric metaplasia only’ (glandular epithelium with cardiac/fundic metaplasia)
-
‘Barrett's oesophagus with IM’ (glandular epithelium with IM)
-
‘No evidence of Barrett's oesophagus’ (squamous mucosa without glandular tissue).
Online supplementary appendix 3 shows histological examples of Barrett's with gastric metaplasia and IM.
Particular attention to exclude sampling from the hiatus hernia or cardia should be given when fundic/oxyntic mucosa only is found, since pure fundic metaplasia is a rare finding in Barrett's oesophagus51 (Evidence grade III). This can be useful when trying to distinguish between an irregular Z-line and true Barrett's oesophagus.
The endoscopist should record whether the biopsy samples are taken at the GOJ (irregular Z-line, without convincing endoscopic evidence of Barrett's oesophagus), as this will lead to the distinct histopathological diagnosis of ‘Junctional mucosa with cardiac or oxyntic epithelium with/without intestinal metaplasia’.
In order to improve the standard of care and to ease discussion between experts, the use of a minimum dataset is recommended to report histopathological findings (Recommendation grade C).
Screening for Barrett's oesophagus
In order to determine the usefulness and potential feasibility of screening, it is necessary to consider: the population prevalence; the identifiable risk factors that might help focus screening on subgroups at higher risk; and the diagnostic tests available.52
Prevalence of Barrett's oesophagus
The prevalence of Barrett's oesophagus in the population at large remains uncertain, which is due to the need for endoscopy to define this condition. Two studies have attempted to assess the prevalence via endoscopy screening of the unselected adult population. An Italian study conducted endoscopies in 1033 individuals, showing a prevalence of Barrett's oesophagus of 1.3%.53 A Swedish population study of 1000 people revealed a prevalence of 1.6%.54 However, the limited participation rate remained a concern in both these studies, since it introduced a risk of selection bias resulting in a possible overestimate of the prevalence.
Risk factors for Barrett's oesophagus
Male gender,55–57 older age56 ,58 and history of reflux symptoms56–61 are the main established predictors of increased risk of Barrett's oesophagus (Evidence grade IIa). There is also an association with obesity, at least when assessed as waist to hip ratio56 ,62 and abdominal circumference63 (Evidence grade IIa), while studies of body mass index only have shown more contradictory results.62–65 A history of cigarette smoking is associated with Barrett's oesophagus in some studies,56 ,59 ,60 but not all.65 Familial clustering for Barrett's oesophagus is reported in about 7% of individuals with Barrett's oesophagus or OAC.66 A positive family history of Barrett's oesophagus or OAC is associated with an increased risk of Barrett's oesophagus,66 ,67 and up to 28% of first-degree relatives of patients with OAC or Barrett's HGD also have Barrett's oesophagus.68 (Evidence grade IIa). Studies on familial aggregation have implicated genetic factors in the development of Barrett's,67 and a recent genome-wide association study has identified the first two loci associated with the disease.69 Studies on this topic are summarised in table 2.
Summary of risk factors for development of Barrett's oesophagus
Diagnostic technologies
The diagnostic technologies used for screening also affect the feasibility and cost-effectiveness of such a programme. For example, ultrathin transnasal endoscopy may have advantages over standard endoscopy, and non-endoscopic cytology devices may also be much more suitable for population-based screening. The data on the sensitivity of these devices and associated assays are summarised in table 3. The use of an immuno-based assay significantly enhances the sensitivity and specificity of a cytology collection device (Cytosponge), and this is promising, but results of further trials, such as the ongoing BEST2 trial, are required before such technologies can be recommended for screening outside of research.
Technologies investigated for screening in Barrett's oesophagus and OAC
Since the literature search was conducted, a study has been published demonstrating that patients belonging to practices with the lowest rates of gastroscopy are at greater risk of poor outcome when oesophagogastric cancer is diagnosed.68 This highlights the importance of referring patients appropriately for endoscopy when risk factors are present.
Screening with endoscopy is not feasible or justified for an unselected population with gastro-oesophageal reflux symptoms (Recommendation grade B).
Endoscopic screening can be considered in patients with chronic GORD symptoms and multiple risk factors (at least three of age 50 years or older, white race, male sex, obesity). However, the threshold of multiple risk factors should be lowered in the presence of a family history including at least one first-degree relative with Barrett's or OAC (Recommendation grade C).
Surveillance
Rationale for endoscopic surveillance
Survival rate for invasive OAC is very poor with <13% overall survival at 5 years71 (also available at http://info.cancerresearchuk.org/cancerstats/). The aim of endoscopic surveillance is to detect cancer or precancer at a stage when intervention may be curative. Specifically, surveillance should detect cancer before invasion of the submucosa when the risk of lymph node metastases significantly increases and varies between 9% and 50% depending on the depth of invasion within the submucosa.72 The practice of surveillance is widespread among European and North American gastroenterologists despite the lack of RCT evidence to demonstrate its efficacy. The BOSS Trial, which is a RCT for systematic Barrett's surveillance compared with endoscopy ‘at the time of need’, is now in the follow-up phase, and it is hoped that this will provide clear evidence one way or the other. In the meantime, the current evidence base is from comparative studies and epidemiological retrospective cohort studies73–80 (Evidence grade III). A study has been published since the literature review that is worthy of mention. Corley et al81 conducted a retrospective case–control study during the years 1995–2009, which compared surveillance histories in 38 cases of OAC in patients with a prior diagnosis of Barrett's oesophagus with 101 living patients under surveillance for Barrett's oesophagus, matched for age, sex and duration of follow-up who had not died from OAC. The data demonstrated that surveillance within 3 years was not associated with a decrease in mortality from OAC. However, it can also be seen that patients were more likely to have had dysplasia during surveillance and ∼50% had advanced disease at diagnosis, suggesting that there is a problem with the quality of surveillance. Hence, we have paid particular attention to providing guidance for how surveillance should be conducted, including the management algorithms when dysplasia is identified (see following sections).
The first consideration with regard to the justification for Barrett's surveillance is the annual cancer conversion rate. Historically, this has been quoted as 0.5% per annum based on a number of case series.82–88 These have tended to be small and subject to publication bias.89 However, two new population-based studies have suggested that the true rate may be lower than this. In a Northern Ireland population-based study, the incidence of cancer and HGD was determined in 8522 patients with an endoscopic diagnosis of Barrett's with or without IM with a mean follow-up of 7.0 years (59 784 patient years). The overall risk of HGD and OAC was 0.22% per year (or 0.16% per year for OAC only), which increased to 0.38% per year when the analysis was restricted to those with IM.37 In a Danish study, the ascertainment was through histopathology records only on the basis of a diagnosis of IM. A total of 11 028 patients were identified with a median follow-up of 5.2 years (58 547 patient years).90 Here the annual risk for HGD and OAC was 0.26% per year (or 0.12% for OAC only). The risk in this Danish cohort is similar to that in individuals with short segments (0.11% per annum for <3 cm in Northern Ireland cohort and 0.19% in a recent meta-analysis91), which is a group likely to be over-represented when ascertainment is based on histopathological criteria.92 Geographical differences in incidence between different countries should also be borne in mind, as there is evidence of a higher incidence of OAC in the UK compared with other areas, including the USA and Northern Europe.93 ,94 Meta-analyses are a useful calibrator, and, in the most recent published meta-analysis,91 57 studies comprising 11 434 patients and 58 547 years of follow-up were selected as meeting the required criteria. Here the incidence of OAC in non-dysplastic Barrett's was 0.33% (95% CI 0.28% to 0.38%) with no evidence of publication bias.
When comparing the cancer risk in patients with Barrett's oesophagus with other conditions, even taking the most conservative study, the standardised incidence ratio of OAC was 11.3,90 which is 4.7-fold and 3.9-fold higher than the colon cancer risk in ulcerative colitis95 and primary sclerosing cholangitis96, respectively, 4.5-fold higher than the risk of any lymphoproliferative disorder/malignancy in coeliac disease,97 and roughly equal to the risk of breast cancer in first degree relatives of BRCA1/2 mutation carriers with breast cancer.98 Therefore, methods to detect individuals at increased risk merit careful consideration.
If surveillance is worthwhile, then it should detect earlier-stage cancers and hence should be a reasonable predictor of longer survival. The published literature suggests that cancers detected during surveillance are generally earlier stage and associated with improved survival (table 4) (Evidence grade III). However, although improved survival rates are the most desirable indicators of the effectiveness of any surveillance programme, these data are often not available and, when they are, are confounded by inherent lead-time bias and length bias.
Summary of studies examining impact of surveillance on OAC outcomes
Although RCT data are lacking, given the evidence from the published studies that surveillance correlates with earlier staging and improved survival from cancer, surveillance is generally recommended (Recommendation grade B).
Endoscopic monitoring with histopathological assessment of dysplasia is the only current method of surveillance with sufficient evidence to be recommended (Recommendation grade B).
Clinical and demographic risk factors associated with malignant progression
As discussed above, there is evidence that the presence of IM correlates with greater biological instability. This has been confirmed in the population study on the Northern Irish cohort, where the cancer risk in patients with IM was almost three times as high as that in patients without IM.37
There have been multiple studies published over the last 20 years demonstrating that men are at increased risk of developing OAC compared with women, and the median age peaks in the 6th decade. In the largest population dataset available, the overall risk (with and without IM for all segment lengths) was 0.28% per year in men and 0.13% per year in women.37 However, there is a paucity of data and inconsistency across the studies concerning the association of male sex and the progression to cancer (table 5) and hence different management for men is not currently indicated.
Studies reporting association with Barrett's oesophagus length and sex with cancer progression
The same group has examined the effect of lifestyle factors and has shown that current tobacco smoking was significantly associated with an increased risk of progression (HR=2.03; 95% CI 1.29 to 3.17) compared with never smokers, and across all strata of smoking intensity99 (Evidence grade III). Alcohol consumption was not related to risk of progression. Measures of body size were rarely reported in studies, and body size was not associated with risk of progression.
The majority of the recent studies (three meta-analyses, 11 cohort studies and two case–control studies) reported a positive correlation between the length of Barrett's segment and the risk for adenocarcinoma, although this did not reach statistical significance in all of them37 ,57 ,84 ,100–113 (Evidence grade III) (table 5). Traditionally, 3 cm has been used as a cut-off to distinguish between long and short segments, and this has been reflected in the majority of the studies. While this is arbitrary, data suggest that interobserver agreement is reduced for very short segments, especially once they are <1 cm21. These studies are summarised in table 5 (see recommendation below). Besides segment length, the presence of ulcers, strictures and nodules are indicative of prevalent malignancy and should be reassessed without delay, including multiple targeted biopsies or diagnostic ER if appropriate.86 ,114
In the future, surveillance intervals should take into account all the socio-demographic risk factors and characteristics of the Barrett's segment; however, such risk algorithms have not yet been developed and validated sufficiently. In the meantime, the segment length seems the most striking discriminator, and the low rate of progression in segments <3 cm is sufficient to warrant differences in surveillance frequency (figure 3).
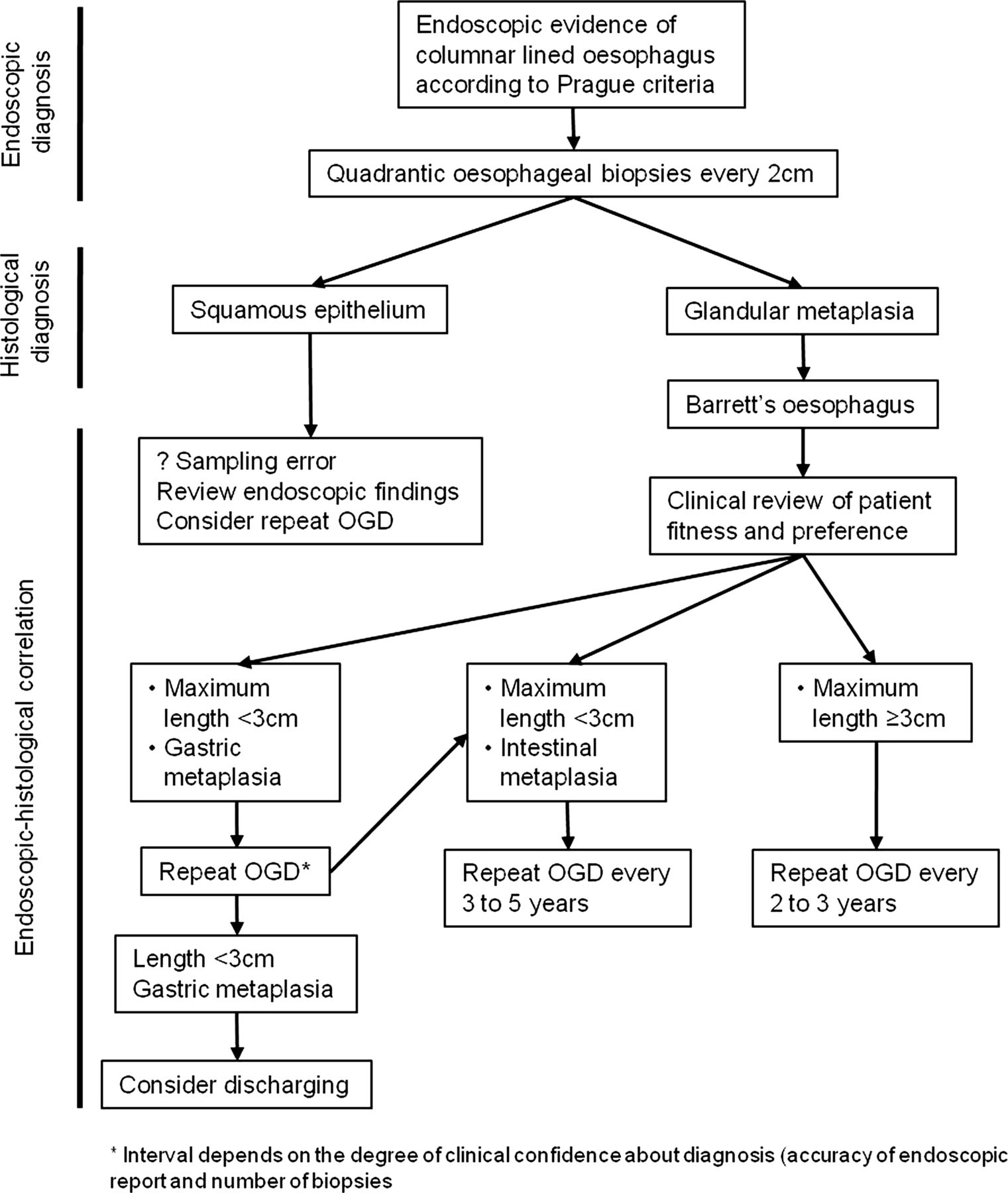
Surveillance flow chart for non-dysplastic Barrett's oesophagus. The endoscopic–pathological correlation is required for the appropriate clinical management of patients with Barrett's oesophagus. The presence of intestinal metaplasia and the length of the Barrett's segment influence the timing of the endoscopic surveillance. OGD, oesophagogastroduodenoscopy.
Surveillance regimens should take into account the presence of IM and length of the Barrett's segment (Recommendation grade B).
IM at the cardia and GOJ
The presence of IM in the gastric cardia or at the GOJ is a common pathological finding at endoscopy and can occur in 5–18% of the normal population.110 ,115 ,116 This appears to have a distinct epidemiological and clinical profile compared with Barrett's oesophagus. IM at the cardia or GOJ has a higher prevalence in female subjects and non-white races, and, according to some, but not all, of the studies can be more often associated with Helicobacter pylori infection110 ,117 ,118 (Evidence grade III). More importantly, there is evidence that individuals with IM at the cardia or GOJ have a significantly lower cancer risk than patients with Barrett's.110 ,119 ,120 In particular, one recent population study that followed-up 86 patients with IM at the GOJ for a median interval of 8 years has found no incident cases of cancer118 (Evidence grade III).
Surveillance is generally not recommended in patients with IM at the cardia or in those with an irregular Z-line regardless of the presence of IM (Recommendation grade C).
Correlation of histopathological grade of dysplasia and tissue molecular markers with risk of malignant progression
The risk of cancer in Barrett's has been shown repeatedly to be higher in glandular mucosa harbouring IM, as discussed above. The current biomarker is dysplasia, which is based on morphological criteria and reflects the underlying complex array of molecular alterations leading to abnormal cell kinetics, differentiation status and epithelial polarity. There is robust evidence that dysplasia is a risk factor for cancer progression, but there are important drawbacks related to the pathological diagnosis of dysplasia.
During surveillance, patients with non-dysplastic Barrett's may be at least 10 times more likely to die from an unrelated cause than to develop OAC.91 ,121–123 Furthermore, the risk appears to decrease over time since the initial diagnosis in non-dysplastic Barrett's.124
In the Danish population study, the risk of LGD was five times higher than that of non-dysplastic Barrett's,90 and, in the Northern Ireland population, the HR for development of HGD and OAC combined was 5.67 for LGD, with no dysplasia as 1.00 as the referent37 (Evidence grade III). In a Dutch study in which all cases of Barrett's oesophagus with LGD were reviewed by expert histopathologists, the progression rate was 13.4% per annum for those that were confirmed compared with 0.49% per annum for the 85% of cases that were down-staged to non-dysplastic Barrett's125 (Evidence grade III). The impact of the consensus diagnosis on the progression rate was confirmed in a UK study.126 On the other hand, in a US study with a similar design, the review by expert pathologists did not make any difference; however, the κ value for agreement for LGD was 0.18,103 highlighting the extreme practical limitations of this diagnosis. The extent of LGD—that is, the number of biopsy samples with LGD, has also been suggested to correlate with risk of progression.127 However, a more recent study has not confirmed this finding.103
Overall, the natural history of LGD is still unclear and is likely to be heavily influenced by the histopathological stringency of the diagnosis.
Dysplasia confirmed by two GI pathologists is currently the best tissue biomarker for the assessment of cancer risk (Recommendation grade B).
A number of molecular abnormalities have been characterised during the progression to adenocarcinoma, and several of these have been suggested as suitable biomarkers to supplement or replace the current problematic assessment of dysplasia128 (summarised in online supplementary table S1). Most of these have not been validated sufficiently to justify clinical use, and technological considerations have also hampered application in routine histopathology laboratories. However, molecular methodologies are being increasingly introduced into routine clinical laboratories, and more robust validation studies suggest that progress is being made.129 There is evidence that immunohistochemistry for p53 can improve interobserver agreement for dysplasia and improve patient stratification126 ,130 ,131 (Evidence grade III) (table 6). This is discussed in more detail in the section on the histopathological diagnosis of dysplasia.
Studies investigating correlation of abnormal p53 expression by immunohistochemistry and cancer risk in Barrett's oesophagus
Until randomised controlled evidence is available, biomarker panels cannot yet be recommended as routine of care (Recommendation grade C).
Practicalities of endosopic surveillance
Patient selection and informed consent
When Barrett's oesophagus is detected at endoscopy and confirmed by histopathological findings, this diagnosis should be discussed with the patient in the clinic, so that patient preference can be taken into account. Patients should receive an early outpatient appointment (ideally within 4–6 weeks) to discuss the implications of this diagnosis with a physician with a clinical interest in Barrett's. Discussion should include the low but significant cancer risk, possible lifestyle changes, whether or not there is an indication for endoscopic surveillance, and the therapeutic options if dysplasia is detected (endoscopic and surgical). Family history for Barrett's oesophagus and OAC should also be recorded. If there is still uncertainty about a diagnosis of Barrett's that requires further work up, this should be clearly explained to the patient to avoid confusion. Written information should be provided for the patient to take away using BSG (see online supplementary appendix 4) or other approved materials such as from MacMillan CancerBACUP (http://www.macmillan.org.uk/Cancerinformation/Cancertypes/Oesophagusgullet/Pre-cancerousconditions/Barrettsoesophagus.aspx) or H-CAS (http://www.h-cas.org/barretts.asp).
Before seeking informed consent for surveillance, the diagnosis of Barrett's oesophagus should have been confirmed on endoscopic and histopathological grounds based on the criteria above. Because of the recent advancement in the endoscopic treatment of HGD and mucosal adenocarcinoma,114 ,132 it is no longer appropriate to restrict surveillance to patients who are fit, and willing, to undergo oesophagectomy. In addition, radiotherapy and/or chemo-radiotherapy may be treatment options in patients with more advanced disease who are deemed not fit for surgery.133 However, the patient should be fit for repeated endoscopy procedures and endoscopic therapy if HGD or early cancer is detected. Very few studies have used the performance status (PS) to correlate patient fitness with the outcome of endoscopic therapy for GI early cancers.134 ,135 Endoscopic therapy can be safely performed in patients with Eastern Cooperative Oncology Group PS 0–2.136 Therefore it is reasonable to consider endoscopic surveillance in patients with PS 0–2, provided that the estimated patient life expectancy is sufficiently long for the individual to benefit from surveillance if dysplasia or early cancer were detected.
If surveillance is thought to be clinically indicated, then the clinician should discuss with the patient the possible benefits of surveillance in detecting early-stage tumours and improving cancer survival. However, this discussion should also mention the lack of randomised controlled data to prove the benefits of surveillance, and clinicians must also emphasise to the patient that the actual risk of death from oesophageal cancer is small. Furthermore, the disadvantages of endoscopy surveillance should also be discussed, including the small risks of the procedure26 and the associated psychological morbidity.137 For example, in an American study conducted in a population of Veterans with a diagnosis of Barrett's, more than half of the patients missed their follow-up endoscopy, suggesting that not all patients are willing to adhere to surveillance programmes.138 Clinicians should also emphasise that, as with any monitoring programme, there is a failure rate, in that surveillance cannot guarantee to detect every tumour that may develop. There are no clear data to support how best to impart this complex information, and more work in this area is warranted.
Patients should have early access to an outpatient clinic to be informed about a new diagnosis of Barrett's oesophagus and to have an initial discussion about the pros and cons of surveillance with written information provided (Recommendation grade C).
For a given patient, whether or not surveillance is indicated should be determined on the basis of an estimate of the likelihood of cancer progression and patient fitness for repeat endoscopies, as well as patient preference (Recommendation grade C).
Endoscopic assessment
Technological advancement with new-generation charge coupled devices has allowed the routine use of high-resolution endoscopy (HRE), which produces images with resolutions ranging from 850 000 to more than one million pixels. HRE allows fine definition of the mucosal layer for the recognition of subtle superficial abnormalities, with theoretical advantage in the recognition of dysplasia and Barrett's oesophagus-related early neoplasia. It is the opinion of the experts that HRE, in conjunction with careful cleaning of the mucosal surface of mucus, saliva and food debris, is the minimum standard for the evaluation of patients with known Barrett's oesophagus4; however, to date, there is no randomised trial comparing conventional endoscopy with HRE in Barrett's oesophagus dysplasia detection (Evidence grade IV). In an RCT, HRE performed equally compared with chromoendoscopy and narrow band imaging (NBI) in the overall diagnosis of dysplasia139 (Evidence grade Ib). Mucolytic agents (eg, 4–10% N-acetylcysteine) or antifoaming agents (eg, simethicone) can be used to disperse excess mucus and bubbles. There is also evidence that longer inspection times during assessment with white light endoscopy is associated with an increased detection rate for HGD and early cancer140 (Evidence grade III). This should be taken into account when planning how much time to allocate for endoscopic surveillance of very long segments of Barrett's, particularly those longer than 10 cm.
Although transnasal endoscopy has been shown to be accurate in the diagnosis of Barrett's oesophagus (Evidence grade Ib), the randomised studies performed so far either included a small number of patients,14 or were performed in a low-risk population.13 Furthermore, it should be noted that the biopsy specimens taken with these endoscopes are significantly smaller,13 and this may increase sampling bias and hamper the interpretation of dysplasia. Therefore there is currently a lack of robust data to recommend transnasal endoscopy in routine Barrett's oesophagus surveillance.
HRE should be used in Barrett's oesophagus surveillance (Recommendation grade C).
There is insufficient evidence to recommend transnasal endoscopy as a replacement for transoral endoscopy (Recommendation grade C).
Use of chromoendoscopy and advanced endoscopic imaging
Advanced endoscopic imaging has been investigated to increase the detection of both IM and dysplasia in Barrett's oesophagus with the aim to help target biopsies (table 7).
Comparative studies between standard and advanced imaging techniques for the diagnosis of IM and dysplasia in Barrett's oesophagus
Chromoendoscopy uses dyes to enhance endoscopic detection. Methylene blue (MB) is a vital dye actively absorbed by columnar intestinal-type cells141 and has been used to improve the yield of IM in Barrett's oesophagus142–144 (Evidence grade III). In a historical cohort, Sharma and coworkers found significant enrichment of IM in MB-targeted biopsy samples compared with random samples145 (Evidence grade III). The detection rate of IM and dysplasia during MB chromoendoscopy has been investigated in a number of randomised and cohort studies with conflicting data14–151 (table 7). A recent meta-analysis has found no incremental yield of both IM and dysplasia with MB chromoendoscopy compared with standard endoscopy with random samples152 (Evidence grade Ia). It should also be noted that MB may damage DNA, which, coupled with the lack of evidence for efficacy, suggests that its use cannot be recommended153 (Evidence grade III).
Indigo carmine (IC) is a contrast agent that allows detailed inspection of the mucosal pattern in combination with magnification endoscopy.154 A prospective multicentre study found that the ridged/villous pattern had a 71% sensitivity for IM, while the irregular/distorted pattern had an 83% sensitivity and an 88% specificity for HGD/early cancer155 (Evidence grade III). The limitation of IC chromoendoscopy is the need for high magnification with consequent narrow field of view. Only one randomised trial has evaluated IC chromoendoscopy for detection of dysplasia in Barrett's, but failed to find an increased rate of dysplasia compared with high-resolution white light endoscopy139 (Evidence grade Ib).
The value of acetic acid (AA) to improve the diagnostic yield of surveillance endoscopy has also been studied. AA induces intracellular protein denaturation, with swelling of the mucosal surface and enhancement of the architecture. Randomised cross-over studies have produced contradictory results on the diagnostic yield of AA-enhanced magnification endoscopy for IM156 ,157 (Evidence grade Ib). AA-enhanced magnification endoscopy has been shown to have a higher dysplasia yield in Barrett's oesophagus surveillance, with 24% of patients having histological upgrade compared with a previous standard endoscopy with random biopsies performed in a non-specialist centre158 (Evidence grade III). In a large single-centre prospective study, Pohl et al159 found that AA-targeted biopsies had a sensitivity of 96.7% and a specificity of 66.5% for a diagnosis of HGD/early cancer. A single-centre retrospective cohort study has showed significantly increased dysplasia yield (p=0.001) compared with standard endoscopy with random biopsies160 (Evidence grade III). The same group showed that histology on AA-targeted biopsies was more cost-effective than the Seattle protocol in a high-risk population.161 More data are needed to decide on the usefulness of this technique.
With recent technological advancements, ‘virtual chromoendoscopy’ has become available, which allows chromoendoscopy without the use of dyes. This is based on light filters (NBI, Olympus) or post-image acquisition processing (i-scan, Pentax and FICE, Fujinon). The most extensively studied ‘virtual chromoendoscopy’ technique in Barrett's oesophagus is NBI, which highlights the mucosal pattern and the superficial vasculature. A number of different classifications have been proposed to describe mucosal pits in non-dysplastic and dysplastic Barrett's, which yielded high diagnostic accuracy162–164 (Evidence grade III). When NBI was compared with standard imaging techniques, one prospective tandem study showed an incremental diagnostic yield for dysplasia in the per-patient analysis165 (Evidence grade IIa), and two additional studies reported an increased dysplasia detection only in the per-biopsy analysis139 ,166 (Evidence grade Ib). A meta-analysis of eight studies has found that NBI has a sensitivity and specificity of 96% and 94%, respectively, for the diagnosis of HGD, and 95% and 65%, respectively, for the diagnosis of IM.167 However, the interobserver agreement for the interpretation of the NBI images is only moderate.168 Overall, despite the finding that NBI performed by an expert endoscopist may increase the targeted yield of dysplasia, it also transpires that high-resolution endoscopy alone is sufficient to maximise dysplasia detection on a per-patient basis.
Autofluorescence imaging (AFI), which exploits endogenous fluorophores excited by short wavelengths, has been studied in the context of Barrett's oesophagus.169 ,170 Initial single-centre cohort studies showed that AFI can improve the diagnostic yield of dysplasia compared with standard endoscopy, but with a false-positive rate as high as 80%171 ,172 (Evidence grade III). To overcome this, AFI has been incorporated into an HRE-NBI scope with magnification, also known as endoscopic trimodal imaging (ETMI). Although an initial multicentre non-randomised feasibility study showed that ETMI increased the diagnostic yield for dysplasia from 63% to 90% compared with standard endoscopy with random biopsies173 (Evidence grade III), this was not confirmed in two subsequent multicentre randomised studies, where ETMI only improved the diagnostic yield of dysplasia in the per-biopsy analysis174 ,175 (Evidence grade Ib). Overall, these studies showed that, in selected high-risk cohorts of patients, ETMI does not allow the requirement for random biopsies to be abandoned. Further studies in low-risk patients will inform whether AFI can have a role in reducing the number of biopsies without loss of diagnostic accuracy.
Other imaging techniques that have showed some value in Barrett's oesophagus include confocal laser endomicroscopy, spectroscopy and optical coherence tomography170 ,176–178; however, further studies are needed to clarify whether they can improve diagnostic accuracy during Barrett's oesophagus surveillance.
In the future, molecular imaging may improve our imaging armamentarium to increase dysplasia detection. Molecular imaging exploits fluorescently labelled molecules that bind with different affinity to dysplastic compared with non-dysplastic cells. Two types of compound have been studied so far. In a proof-of-principle study, Li and colleagues identified a 7-amino acid peptide that binds an OAC cell line more avidly than a non-dysplastic Barrett's oesophagus cell line, and they confirmed the differential binding in surgical specimens of OAC ex vivo.179 Similarly, Bird-Lieberman and coworkers identified a natural lectin (wheat germ agglutinin) that differentially binds surface glycoproteins of dysplastic and non-dysplastic cells and used an autofluorescence endoscope in surgically resected oesophagi to validate the ex vivo findings.180 In vivo studies are needed to validate these techniques.
Advanced imaging modalities, such as chromoendoscopy or ‘virtual chromoendoscopy’, are not superior to standard white light endoscopy in Barrett's oesophagus surveillance and are therefore not recommended for routine use (Recommendation grade A).
Biopsy protocol
To find dysplasia, endoscopists have generally relied on the directed sampling of any visible lesions, which may be aided by enhanced endoscopic visualisation tools as discussed above, together with systematic, four-quadrant biopsies every 2 cm according to the so-called ‘Seattle protocol’.26 A prospective study has demonstrated a significant increase in the detection of early lesions through the introduction of such a protocol181 (Evidence grade III). However, adherence to this protocol is limited and ranges from 10% to 79%, with poorer adherence for longer segments,182–184 and failure to adhere to the protocol has been shown to result in a significantly lower rate of dysplasia detection.185 Overall, although intense and time-consuming, the multiple biopsies involved in the Seattle protocol have been demonstrated to be safe when performed by experienced endoscopists.26 Another limitation of this technique is the high cost generated by processing multiple biopsies, but this still seems justified at the current time in the absence of an alternative. Future RCTs will need to compare cost-effectiveness of the standard practice with alternative techniques such as histology on targeted biopsy samples guided by conventional or virtual chromoendoscopy.
Adherence to a quadrantic, 2 cm biopsy protocol in addition to sampling any visible lesions is recommended for all patients undergoing surveillance. This should also apply to long segments (Recommendation grade B).
Frequency of surveillance for non-dysplastic Barrett's oesophagus
In the previous BSG guidelines published in 2005, the recommended surveillance interval for non-dysplastic Barrett's was every 2 years. However, given the recent data suggesting that the overall risk of malignant conversion is lower than previously thought, we recommend that the interval should be lengthened in line with other guidelines.3 We therefore advocate a new surveillance strategy whereby the managing clinician synthesises the endoscopic and histopathological findings to tailor the surveillance interval on a more individual basis (figure 3). A degree of variation in this interval is permitted, which may be influenced by the presence of risk factors for the development of cancer.
To summarise, in practical terms, short segments of columnar epithelium with no IM have an extremely low risk of malignant conversion37 ,91 (∼0.05% per annum) (Evidence grade III). For these patients, it is recommended to repeat the endoscopy once in 3–5 years time to confirm the findings and account for sampling and measurement error. If there is doubt, the endoscopy could be repeated sooner. If two good-quality endoscopies, each with a minimum number of four oesophageal biopsies where possible, confirm a short segment (<3 cm) with gastric metaplasia only, then discharge is encouraged, as the risks of endoscopy probably outweigh the benefits. In selected cases with a strong personal risk profile for OAC (see recommendation on screening), continued endoscopic surveillance can be considered.
For patients with Barrett's oesophagus shorter than 3 cm, without IM or dysplasia, a repeat endoscopy with quadrantic biopsies is recommended to confirm the diagnosis. If repeat endoscopy confirms the absence of IM, discharge from surveillance is encouraged, as the risks of endoscopy probably outweigh the benefits (Recommendation grade C).
There is evidence that the risk of cancer progression correlates significantly with the length of the Barrett's segment, such that segments shorter than 3 cm have a lower cancer incidence (table 5). Therefore, in view of the recent evidence supporting a lower cancer risk in non-dysplastic Barrett's oesophagus than previously thought, it is reasonable for patients with short segments containing IM to have a longer endoscopic surveillance interval than patients with long segments. We propose a range of 3–5 years to allow the clinician to tailor surveillance on the perceived individual cancer risk.
Patients with Barrett's oesophagus shorter than 3 cm, with IM, should receive endoscopic surveillance every 3–5 years (Recommendation grade C).
For longer segments (>3 cm), a shorter surveillance interval is more appropriate. This is regardless of the presence of IM, since it is noted, that in long segments, IM is almost always present, but can be missed due to sampling error. We propose a range (between 2 and 3 years), which may be informed by the individual risk factors and patient and physician preference. Because of the poor adherence to the surveillance biopsy protocol for long segments of Barrett's oesophagus, consideration should be given to refer patients with a very long segment (>10 cm) to tertiary referral centres for endoscopic surveillance, as suggested also in the new Dutch guidelines (personal communication).
Patients with segments of 3 cm or longer should receive surveillance every 2–3 years (Recommendation grade C).
Histopathological diagnosis of dysplasia
Pathological features and reporting of dysplasia
Online supplementary appendix 3 shows histological examples of Barrett's with different degrees of dysplasia.
There are very few studies that investigated reporting of dysplasia in Barrett's oesophagus. Two studies examined the Vienna classification and found a degree of agreement among pathologists that was at best moderate for HGD, fair for LGD, and poor for indefinite for dysplasia.126 ,186 The approach to reporting upper GI tract neoplasia differs significantly in certain parts of the world and this has led to inconsistency in the terminology used and hence inconsistent data on incidence and clinical progression outcomes. The most recent recommendations by the WHO state that dysplasia should be graded as either low or high grade.187 The revised Vienna classification for GI mucosal neoplasia attempts to standardise diagnostic terminology into biologically similar groupings with scores of 1–5188 depending on the presence or absence of dysplasia or malignancy.
Revised Vienna classification and dysplasia subtypes
1. Negative for dysplasia
This includes normal epithelium, metaplastic epithelium showing reactive or regenerative changes, and mucosa showing reactive/regenerative changes including nuclear enlargement, nuclear hyperchromasia and prominent nucleoli.
2. Indefinite for dysplasia
This category is used for cases where the morphological features between true dysplasia and regenerative/inflammatory atypia are blurred.189 It is important to appreciate that this diagnosis may in fact mean that the patient has features suspicious of HGD, but not enough certainty is present to warrant this call. This may be due to technical factors, such as poor staining, poor orientation, cross cutting or denuded surface epithelium, or to severe active inflammation or ulceration leading to marked atypia, precluding a confident diagnosis of dysplasia. In other cases, the epithelium appears abnormal, but the features are not sufficiently well developed to justify a definite diagnosis of dysplasia. Features favouring dysplasia are the presence of an abrupt transition from normal to atypical epithelium, together with nuclear pleomorphism, atypical mitoses and loss of nuclear polarity.190 Evidence of ‘surface maturation’—that is, loss of the cytological atypia seen in the deeper glands as the mucosa matures into the surface epithelium—is often taken as the best marker to favour regeneration rather than dysplasia, although this is also not invariably true (eg, crypt dysplasia described below). Explicit mention in the pathology report of the reason justifying this diagnosis can be useful to aid patient management.
3. Low-grade dysplasia
In LGD, glandular architecture is relatively preserved and the diagnosis is made on the basis of cytological atypia.
Morphological patterns of LGD
-
LGD generally shows an ‘adenomatous’ cytological appearance (resembling the dysplastic changes associated with adenomatous polyps of the colon) in which nuclei are elongated (pencil shaped), slightly enlarged and hyperchromatic with inconspicuous nucleoli. There may be mild pleomorphism, mucin depletion, mild loss of polarity, nuclear crowding, and stratification of nuclei up to three-quarters of the height of the cell, but not touching the luminal surface. Mitoses and apoptotic debris may be seen on the surface or in the upper portions of the glands. Evidence of loss of ‘surface maturation’—that is, presence of cytological atypia seen in the deeper glands—into the surface epithelium is often taken as the best marker to distinguish true dysplasia from regenerative atypia; however, in the presence of ulceration, regenerative surface epithelium may also closely mimic LGD.
-
A ‘non-adenomatous’ (foveolar) type composed of small round cells with abundant cytoplasm may occasionally be seen.191 Although this is less well characterised, cells with nuclear/cytoplasmic ratios <50% are probably best put into this low-grade category.
4a. HGD (incorporating carcinoma in situ)
The distinction between HGD and LGD is largely based on the presence of architectural changes in conjunction with more marked nuclear atypia. These changes may be accompanied by complex architectural changes including a papillary or villous surface (although villiform change may also be seen in reactive epithelium), in conjunction with branching, complex budding or back-to-back ‘crowding’ arrangements. Intraluminal papillae, bridges or cribriform patterns are also seen. There are increased numbers of atypical mitoses on upper levels of crypts, together with mucin depletion and a loss of nuclear polarity. Of note, HGD can be accompanied by acute inflammation and should not be downgraded in its presence.190
Morphological patterns of HGD
-
‘Adenomatous’ cytological appearance: nuclei are elongated, pencil shaped, enlarged, hyperchromatic and show crowding and stratification up to the luminal surface of the cells. The distinction between the upper end of ‘low grade’ and ‘high grade’ dysplasia can be subjective.
-
‘Non adenomatous’, which includes the term foveolar dysplasia: cells have a cytological appearance characterised by rounded nuclei showing marked nuclear enlargement and marked atypia with increased nuclear/cytoplasmic ratios, irregular nuclear membranes (including angular edges), coarse chromatin, and prominent or irregular nucleoli. The foveolar type may have a more bland appearance, comprising small round nuclei with conspicuous nucleoli. The grading of this variant is less well characterised; however, the nuclear/cytoplasmic ratio appears to be more important for grading, with high ratios (nuclei involving >50% of cell) being put into a high-grade category.
Crypt dysplasia
Significant cytological atypia in the crypt bases with surface maturation has been reported in up to 7.3% of cases of Barrett's.192 Previously, this would have been regarded as either ‘negative for dysplasia’ or ‘indefinite for dysplasia’, as the atypia does not reach the surface epithelium. It seems likely, however, that crypt dysplasia represents an early stage in the development of dysplasia, and the atypia is highly likely to progress up to the surface over time and so warrants recognition.193 Crypt dysplasia stands out as a focus that is distinctly different from the surrounding crypts and can appear as low-grade or high-grade cytological atypia. Although the dysplasia can be of the ‘adenomatous’ or ‘non-adenomatous’ round cell type, the most common features are nuclear enlargement, loss of polarity, marked pleomorphism with irregular shapes and sizes, nuclear crowding, increased mitotic activity and goblet cell dystrophy. Crypt dysplasia should not be diagnosed purely on the basis of stratification and hyperchromasia in the absence of significant nuclear pleomorphism, as these changes may often be seen in regenerative cryptal epithelium. p53 immunohistochemistry may be a helpful adjunct for the assessment of crypt dysplasia. Crypt dysplasia should be reported according to the degree of dysplasia present. If there is uncertainty, then the ‘indefinite’ category may be appropriate. Some pathologists favour putting cases with high-grade features into an ‘at least low grade’ category in view of the likely early nature of the lesion and the implications of a high-grade diagnosis; however, cases of isolated crypt dysplasia are probably best managed as low grade until further data become available.193
4b. Intramucosal carcinoma (including suspicious for invasive carcinoma)
Intramucosal carcinoma is a lesion in which neoplastic cells have penetrated the basement membrane and invaded the lamina propria or muscularis mucosae, but without invasion into the submucosa. However, histological recognition of lamina propria invasion may be difficult because of the absence of objective criteria. Patterns of lamina propria invasion that are used by gastrointestinal pathologists include sheets of neoplastic cells, abortive angulated glands, a never-ending/anastomosing gland pattern, a highly complex cribriform arrangement of glands, tightly packed small tubular glandular arrays, and single-cell infiltration. Recognition of each of these patterns is somewhat subjective, with κ statistics varying between 0.21 and 0.47, suggesting poor or, at best, moderate agreement.126 ,186 If definitive submucosal invasion is in question, the term ‘suspicious of invasive carcinoma’ can be used.
5. Submucosal invasion by adenocarcinoma
Unequivocal invasion of submucosa or deeper structures often accompanied and characterised by a desmoplastic response in the tissue stroma to invasive tumour cords/acini.
Given the important management implications for a diagnosis of dysplasia, we recommend that all cases of suspected dysplasia are reviewed by a second GI pathologist, with review in a cancer centre if intervention is being considered (Recommendation grade C).
Given the difficulties associated with the management of the ‘indefinite for dysplasia’ category, all such cases should also be reviewed by a second GI pathologist, and the reasons for use of the ‘indefinite for dysplasia’ category should be given in the histology report in order to aid patient management (Recommendation grade C).
Dysplasia reporting and reproducibility
It has long been recognised that there is inter- and intra-observer variability in the diagnosis of GI tract dysplasia. This relates to differentiating between HGD and intramucosal adenocarcinoma, HGD and LGD and also distinguishing between regenerative changes and LGD. In the case of definite dysplasia, this is because these divisions involve unnatural cut-offs along a biological/histological continuum.126 Studies have shown that the prediction of progression of oesophageal dysplasia is improved if at least two expert pathologists agree on the diagnosis and increases further when a greater number of pathologists concur with the diagnosis.125 ,130 For practical reasons, and in day-to-day diagnostic practice, a diagnosis of dysplasia in the setting of Barrett's should be corroborated by a second pathologist with a specialist GI interest. The Royal College of Pathology recommends that ‘double’ reporting of a diagnosis of HGD in the upper GI tract should be mandatory and this has been confirmed by consensus statements agreed by Barrett's international experts.4 We have extended this consensus reporting to all grades of dysplasia.
Aids to histological diagnosis of dysplasia and p53 immunostaining
Of all the putative experimental molecular markers, the one with the greatest body of evidence and which can also be applied in the routine clinical setting is immunohistochemistry for nuclear p53. Although the p53 positivity rate in Barrett's oesophagus dysplasia is variably reported in the literature, ranging from 50% to 89%,194 ,195 when positive it can improve interobserver agreement for reporting dysplasia126 and can be a powerful predictor of progression, with an OR between three and eight in different studies129 ,131 ,196–198 (table 6). In a study from Skacel et al130, who analysed factors predictive of progression in patient with LGD, p53 immunostaining positivity and 100% agreement among three GI pathologists on LGD diagnosis correlated with the risk of progression, suggesting that p53 might improve interobserver agreement. This was replicated in a later study.126 Interpretation of p53 immunostaining can be problematic and poorly reproducible subject to variation in methodology and interobserver variation. Notwithstanding this, some pathologists find staining for p53 of use, especially in distinguishing between atypical reactive proliferation (indefinite for dysplasia) and true LGD. Low background wild-type p53 expression is often seen in nuclei of normal columnar and basal layers of squamous mucosa, which is a useful baseline to identify the overexpression pattern typical of dysplasia. Overexpression is generally a consequence of mutations that stabilise the inactivated protein.199 However, not all p53 mutations lead to stabilisation of a mutated inactive p53 protein. A study performed in non-small cell lung cancer showed that, as opposed to missense mutations, the majority of null mutations did not lead to p53 overexpression.200 In such cases, mutation is expected to lead to failed translation of the protein. In fact, an absent pattern of p53 immunostaining, when compared with normal wild-type background, is now recognised as an abnormal pattern which also occurs in dysplasia as a result of silencing mutations of the p53 gene.194 Online supplementary appendix 3 shows immunohistochemical examples of Barrett's with overexpression and loss of p53.
The addition of p53 immunostaining to the histopathological assessment may improve the diagnostic reproducibility of a diagnosis of dysplasia in Barrett's oesophagus and should be considered as an adjunct to routine clinical diagnosis (Recommendation grade C).
Management of dysplasia and early cancer
Indefinite for dysplasia, a controversial entity
There is very little published literature on the management of patients with this histopathological condition. A study looking at interobserver variability showed that the degree of agreement among pathologists for a diagnosis of indefinite for dysplasia is lower than that for LGD, with κ values of 0.18 and 0.35, respectively186 (Evidence grade III). Younes and coworkers showed that the rate of cancer progression in patients with indefinite for dysplasia was similar to non-dysplastic patients; however, if the indefinite for dysplasia was multifocal, the rate of progression was as high as in patients with LGD201 (Evidence grade III). An excess of inflammation is linked to cellular atypia, and this could be resolved by improved medical control of the gastro-oesophageal reflux, although scientific evidence for this is lacking (figure 4).

Surveillance flow chart for dysplastic Barrett's oesophagus (BO). A pathological finding of indefinite for dysplasia does not exclude the presence of dysplasia, therefore a 6-month follow-up is warranted. Six-monthly surveillance and endoscopic treatment are generally recommended for low-grade and high-grade dysplasia, respectively. MDT, multidisciplinary team; OGD, oesophagogastroduodenoscopy.
Patients with a diagnosis of indefinite for dysplasia should be managed with an optimisation of the antireflux medical therapy and re-endoscoped in 6 months. If no definite dysplasia is found on subsequent biopsies, then the surveillance strategy should follow the recommendation for non-dysplastic Barrett's oesophagus (Recommendation grade C).
LGD: surveillance or ablation?
As discussed in the surveillance section, management of LGD is confounded by uncertainty about the natural history and difficulties in making a definitive diagnosis. A diagnosis of LGD correlates with a higher risk of progression to cancer, but it is unclear yet whether this warrants therapeutic intervention. Published literature showed that endoscopic therapy can successfully eradicate LGD. PDT with both 5-aminolaevulinic acid (ALA) and porfimer sodium was shown to be effective in the treatment of LGD150 ,202 (Evidence grade Ib). RFA has also been shown to eradicate dysplasia in over 90% of patients with LGD203 (Evidence grade III). However, this evidence alone does not justify a clinical indication of endoscopic therapy in patients with LGD. The RCT published by Shaheen and coworkers investigated the effectiveness of RFA in preventing disease progression in patients with both LGD and HGD.134 In this study, although the overall outcome showed a lower risk of disease progression in all patients treated with RFA, the subgroup analysis in patients with LGD failed to show a significant advantage from treatment, since none of the patients with LGD progressed to cancer within the follow-up period (Evidence Ib). The results of a multicentre RCT for RFA compared with endoscopic surveillance in a large cohort of patients with LGD are awaited (SURF Trial). It is possible that endotherapy may be recommended if the outcome of this trial is positive, and a recommendation from NICE should be used as guidance, but in the meantime it cannot be recommended on a routine basis. At the present time, in view of the higher progression rate reported for LGD, these patients should be followed-up more intensively than non-dysplastic patients (figure 4). If ablative treatment is considered in selected cases, then this decision should be reviewed by the MDT.
Management of LGD is unclear in view of limited data about the natural history. It is essential that the diagnosis is confirmed by two pathologists, and patients should be surveyed endoscopically at 6-monthly intervals. Currently, ablation therapy cannot be recommended routinely until data from RCTs are available (Recommendation grade C).
HGD and intramucosal cancer: getting the diagnosis right
Most HGD and early cancer (T1) in Barrett's will be discovered at the time of endoscopy, either performed for the first time (in a patient presenting with dyspepsia, for example) or as part of a surveillance programme. Although there may be visible abnormalities, these can often be subtle and overlooked at initial endoscopy. The first indication of a problem may be flagged up by the pathologist finding dysplasia or suspecting invasive cancer on a biopsy, either targeted from a visible abnormality or from among systematic four-quadrant biopsy specimens. The first step should be to confirm the diagnosis with at least one other pathologist with experience in GI histopathology.125 ,126
Whether or not the diagnosis is confirmed, if the possibility of significant dysplasia has been raised, it is essential that there has been a high-quality baseline endoscopy conducted to map out any visible lesions and the extent of any dysplastic changes prior to any management decisions being made. HRE has a high sensitivity for the detection of Barrett's-related neoplasia, and more than 80% of patients referred for work up of HGD or early Barrett’s cancer, apparently without visible abnormalities, will have at least one visible lesion detected in their Barrett’s oesophagus upon expert endoscopic assessment.139 ,173 ,174 Although early Barrett’s oesophagus neoplasia generally presents as subtle flat lesions that may be difficult to detect, most procedures performed with HRE endoscopes do reveal these abnormalities to the experienced eye.204 ,205 However, up to 20% of patients do not have a visible abnormality after HRE and advanced imaging, and, in such cases, four-quadrant biopsies are required to detect HGD.173 ,174 There is some evidence that magnification and electronic/optical manipulation of the image can increase detection of dysplasia in Barrett's oesophagus when compared with HRE, as discussed in the endoscopic surveillance section; however, advanced imaging modalities rarely change the overall diagnostic outcome.166 ,175 These imaging techniques can, however, aid definition and detailed mapping of the edges of visible lesions in order to guide complete ER.206 ,207
Expert HRE should be carried out in all Barrett's patients with biopsy-detected HGD in order to detect visible abnormalities suitable for ER (Recommendation grade B).
Visible lesions should be considered malignant until proven otherwise (Recommendation grade C).
Any endoscopic abnormalities should be documented using the Paris classification, which is based on the Japanese system used to classify early gastric cancer. It has been used used to classify mucosal irregularities in patients with Barrett’s oesophagus,25 although, unlike the Japanese classification for early gastric cancer, it has not been validated as a prognostic tool in this context. Superficial Paris 0-IIa and 0-IIb lesions are unlikely to contain invasive cancer, while type 0-Is sessile lesions and type 0-IIc ‘depressed’ lesions are more likely to contain invasive cancer, with up to 25% of cases subsequently being shown to have submucosal (sm) invasion.204 ,205 ,207
Description of lesion morphology using the Paris classification gives an indication of the likelihood of invasive cancer and aids communication between clinicians. This should therefore be used for all visible lesions but cannot at present be used to predict prognosis (Recommendation grade C).
Role of specialist teams and decision making
Treatment for HGD and early cancer involves endoscopic or surgical management. The success of both modalities should be measured in terms of morbidity and mortality related to the procedure (or series of procedures), long-term survival and QOL. These recommendations are entirely consistent with the guidelines for the management of oesophageal and gastric cancer recently published by Allum et al,133 which, however, focus specifically on HGD and early cancer.
Recommendations for treatment of patients with Barrett's-related neoplasia should be taken in the context of an upper GI specialist MDT taking into account patient comorbidities, nutritional status, patient preferences and staging (figure 5).6 Before treatment decisions are made, the patient should have the opportunity to discuss the options in an outpatient clinic setting (not in endoscopy after sedation), and this may comprise a joint discussion with an endoscopist and a surgeon. The patient should have access to all the supporting evidence being used to make the recommendation according to their wishes. Patients should be copied into any clinical correspondence, as recommended by NICE guidelines for the management of colorectal cancer.209

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Recommended flow chart for the management of high-grade dysplasia (HGD) and early oesophageal adenocarcinoma (OAC). A diagnosis of HGD and early OAC should be discussed in a multidisciplinary team (MDT) setting, and treatment options should be explained in the clinic to the patient. Endoscopic treatment and surgery are generally recommended for mucosal disease and submucosal cancer, respectively. Good prognosis cancer with involvement of superficial submucosal layers (sm1) can be treated endoscopically in patients at high surgical risk. EC, early cancer; HRE, high-resolution endoscopy; OGD, oesophagogastroduodenoscopy; RFA, radiofrequency ablation.
All patients with dysplasia or early cancer, for which therapy is considered, should be discussed at the specialist MDT for oesophagogastric cancer. This team should include an interventional endoscopist, upper GI cancer surgeon, radiologist and a GI pathologist (minimum standard) (Recommendation grade C).
Patients with dysplasia or early cancer should be informed of treatment options and have access to all specialists if required (Recommendation grade C).
Endoscopic therapy for Barrett's-related neoplasia
Although, surgery remains an effective treatment for Barrett's neoplasia, it is associated with significant morbidity and mortality compared with endoscopic therapy. Cohort studies suggest that endoscopic therapy for mucosal OAC has similar long-term disease-specific survival to surgery, but lower death rates.210–212 A number of retrospective case series comparing endoscopic and surgical therapy have demonstrated high survival outcomes in both groups, but higher short-term mortality in the surgical group than in the endoscopic group, but patients were not well matched.212–215 A systematic review showed a mortality of 1.2% in the surgical group compared with 0.04% in the endoscopic group.216 A more recent study showed lower morbidity in the endoscopic group214 (Evidence grade III). A cost-effectiveness study demonstrated that RFA was likely to be more cost-effective than surgery.217 Recent consensus statements issued by a large group of international experts have indicated that endoscopic therapy should be preferred over surgery for the management of early Barrett's neoplasia.4
For HGD and Barrett's-related adenocarcinoma confined to the mucosa, endoscopic therapy is preferred over oesophagectomy or endoscopic surveillance (Recommendation grade B).
Endoscopic therapy in the oesophagus carries a low but significant risk of complication.218 ,219 It is important that therapy is carried out in centres that have the specialist expertise to offer and the necessary back-up if required. For example, endoscopic therapy should be carried out in centres that can also offer surgery if a complication occurs.
Endoscopic therapy of Barrett’s neoplasia should be performed at centres where endoscopic and surgical options can be offered to patients (Recommendation grade C).
There are now good observational data to support the performance of oesophageal surgery in specialist centres for treatment of adenocarcinoma.220 Results for individual surgeons improve with experience, and patient outcomes have consistently been shown to be better in high-volume centres220 ,221 (Evidence grade III). ER series reported from expert high-volume centres have shown a low rate of significant complications (<3%),114 ,212 ,218 but the complication rate is significantly higher in the hands of less experienced endoscopists during their first 20 ER procedures performed.222 Therefore it seems logical that, similar to the recommendations for oesophagectomy, endoscopic therapy should also be performed in centres with the experience, facilities and high throughput of cases to optimise outcomes. Endoscopic training should start with knowledge acquisition, followed by resection and ablation in tissue animal models, before training in human subjects. The GI pathologist should also be trained in the report of ER specimens. In order to achieve a good level of training, it is crucial that professional societies guarantee wide availability of training courses and fellowships for Barrett's endoscopic therapy.
A minimum of 30 supervised cases of ER and 30 cases of endoscopic ablation should be performed to acquire competence in technical skills, management pathways and complications (Recommendation grade C).
ER should be performed in tertiary referral cancer centres for oesophageal cancer disease, which must be equipped with high-resolution endoscopes and all relevant ER facilities. These specialist cancer centres should have an adequate volume of cases, which in the absence of published evidence we have set as 15 ERs per annum for HGD or early cancer in a given centre based on the opinion of experts. Centres should preferably have two endoscopists performing endoscopic therapy, and low-volume centres should consider developing joint services. The endoscopist performing endoscopic therapy must be fully trained in lesion recognition and ER techniques, with expertise in at least one enhanced endoscopy imaging modality (electronic imaging or AA chromoendoscopy). Progression of disease is described during treatment with RFA,132 ,223 therefore an ER may be required during the ablation pathway.
ER should be performed in high-volume tertiary referral centres. RFA should be performed in centres equipped with ER facilities and expertise (Recommendation grade C).
Endoscopic resection
ER should always be performed with therapeutic intent; however, histopathological assessment of the ER specimen is also the most accurate staging technique for Barrett's oesophagus-related early neoplasia.224 ,225 ER is preferred over surveillance biopsies because of the difficulty in differentiating HGD from mucosal cancer and deep invasive cancer on biopsy material.4 ,226 Visible lesions contain the most advanced histological staging in surgical resection specimens, and this is confirmed by experience with step-wise radical ER of the entire Barrett's segment.227 ,228 This supports a policy of removal of all visible abnormalities by ER.
Endoscopic assessment will usually identify the area with the most advanced neoplasia. ER should aim to resect all visible abnormalities (Recommendation grade C).
ER is recommended as the most accurate staging intervention for Barrett's early neoplasia (Recommendation grade B).
Tumours confined to the mucosa (T1a) have been shown to have significantly better 5-year recurrence-free and overall survival rates (100% and 91%, respectively) than those showing involvement of the submucosa (60% and 58%).229 Endoscopic therapy for Barrett's neoplasia has been developed on the evidence that HGD and T1a OAC is associated with a low rate of lymph node metastasis: endoscopic and surgical series indicate a 0–10% risk in T1a cancer, while submucosal invasion carries a higher risk (up to 46%).215 ,229–236 A recent systematic review reported no evidence of nodal metastasis in patients with a final stage of HGD.72 Further stratification of these superficial lesions as in table 8 yields additional prognostic information in that the risk of nodal metastasis correlates with the depth of penetration into the layers,229 ,234 but not all the studies have confirmed this.230 ,236
It is still unclear whether T1sm1 cancer (invading the superficial submucosa within 500 µm) can be confidently treated by ER, and although series from Amsterdam and Wiesbaden suggest this carries a low risk of lymph node metastases,230 ,234 ,237 not all the literature supports this.72 ,236 This debate is further complicated by the technical challenges faced by the pathologist to accurately identify the submucosal invasion depth on the ER specimen. The importance of experienced pathology in deciding whether endotherapy is likely to be curative or not is critical, since not only the depth of invasion but features of the tumour (lymphatic or vascular invasion, degree of differentiation) are thought to be important in the decision-making process.238 Free deep resection margins on the ER specimen (R0), together with an absence of lymphovascular invasion (LVI−) and good differentiation (G1) are all indicative of a good prognosis for early cancer.230 Lymphovascular space invasion and lymph node metastases have been reported in 17% and 10% of patients, respectively, with invasion into the duplicated muscularis mucosae, although these are technically intramucosal.235
ER should be considered the therapy of choice for dysplasia associated with visible lesions and T1a adenocarcinoma (Recommendation grade B).
For patients at high surgical risk, endoscopic therapy can be offered as an alternative to surgery for treatment of good prognosis T1b adenocarcinomas (T1b sm1, well differentiated and without lymph vascular invasion) (Recommendation grade C).
For T1b adenocarcinomas with involvement of the second submucosal layer or beyond (T1b sm2–sm3), endoscopic therapy should not be considered curative (Recommendation grade B)
ER techniques
The basic principle of ER involves identification of the lesion margins by marking with a diathermy device followed by a systematic resection of the marked area. Common resection techniques are cap and snare and band ligation.
The band ligation technique involves suction of the marked area into a distal attachment (preloaded with multiple rubber bands) and deployment of the band on to the tissue to create a pseudo-polyp, which is then resected with a snare. The cap and snare technique also involves a dedicated transparent cap at the distal end of the scope, which is preloaded with a crescent snare. Differently from the band ligation, the area of interest is always injected (submucosal space) and lifted before its suction into the cap. Once the mucosa is placed into the cap, then the snare can be closed around and the tissue resected.
Both cap and snare and band ligation techniques appear to have similar success rates of the order of 85–98%.224 ,239–242 There are two RCTs that compared the two techniques.219 ,243 These studies did not show significant differences either in terms of the depth of resection or complication rates, leading to the conclusion that both techniques were similarly safe and effective. Some endoscopists believe that submucosal injection improves safety of the ER when an attempt is made to resect nodular lesions, which carry a high risk of invasive cancers. In such cases, the presence of the ‘non-lifting sign’ will inform the endoscopist about the possibility of deep invasive cancer and its associated risks.
The cap and snare technique with submucosal injection and the band ligation technique without submucosal injection are considered to be equally effective (Recommendation grade A).
Pathology reporting of ER specimens
ER specimens should be pinned out on a rigid support (eg, cork) and formalin fixed for at least 12 h. Photographs of the fixed specimens can act as a useful record. They should be serially sectioned at 2 mm intervals along the axis of the closest margin and completely embedded. Both of the end pieces should be embedded en face.
The status of the tissue margins is the most significant prognostic factor; however, if the sample has been received in multiple pieces, it will not be possible to identify the true lateral margins, and only deep margins will be relevant.244 Tumours should be graded and T staged. T1a and T1b intramucosal carcinomas can be subclassified as shown in table 8.245 A comment should be made regarding the presence or absence of lymphovascular space invasion, background IM and dysplasia. See minimum reporting dataset (table 9).
Subclassification of T1a and T1b oesophageal adenocarcinoma
Minimum dataset for reporting endoscopic resection specimens
Artefacts such as haemorrhage, heat/cutting artefact, surface loss, fixation contraction with rolling and folding of edges leading to poor orientation of tissue at embedding may all hinder the histological assessment244 (Evidence grade III). The suction technique can cause artefactual lifting and/or disruption of the surface epithelium, with intramucosal haemorrhage, oedema and fibrin deposition on the surface. This should not be confused with true ulceration. Biopsy samples taken 1–16 days after gastric ER can show signet ring cell change and clear cell degeneration in areas of ischaemia.246 Although there are no relevant studies that looked at mucosal changes after ER, tissue regeneration in the immediate post-ER period can hamper proper histological assessment, and therefore it is recommended to delay post-ER biopsies to 6–8 weeks (Evidence grade IV).
It can be difficult to accurately stage these tumours on ER specimens, when there is duplication of the muscularis mucosae, a characteristic finding in Barrett's. This may lead to overstaging by misinterpreting the space between duplicated muscularis as submucosa, and in some instances it may not even be possible to determine if true submucosa is present (see online supplementary appendix 4). The largest and most recent studies suggest that invasion into the space between the duplicated muscularis mucosae has a similar low risk of lymph node metastases to lamina propria invasion if other features (lymphovascular invasion and poor differentiation) are absent230 ,247 (Evidence grade III). In addition, it is important to be aware of entrapped glands and submucosal glands that may mimic submucosal adenocarcinoma.
Further, the use of the muscularis propria as a reference point for determining depth of submucosal invasion is problematic in ERs, as it is generally not represented. In the latter instance, it may be more appropriate to state that submucosal invasion is present and then measure the depth of invasion beyond the muscularis mucosae. In the colon, depth of invasion beyond the submucosa is widely used as a marker of likely lymph node metastases, but studies in OAC have been conflicting, with differences between surgical and ER series.229 ,230 Measurement of the distance from the tumour to the nearest deep margin is recommended to document the adequacy of resection. The presence of tumour cells at the deep margin indicates incomplete resection requiring further treatment.
Use of a minimum dataset for the reporting of ER specimens is recommended to ensure that all prognostic information is included in reports (Recommendation grade C).
The presence of tumour cells at the deep margin indicates incomplete resection and warrants further treatment (Recommendation grade C).
Imaging for HGD and T1 carcinoma: role of CT–PET and EUS
There is little published evidence to support a role for CT (or CT–PET) with regard to early cancer (HGD, mucosal lesions), with most of the evidence being for advanced cancer (see section on surgical treatment). Where biopsy specimens show invasive cancer, CT scanning is often advocated in order to detect distant metastases. However, it has poor accuracy in local T staging and it is less accurate than EUS in detecting local lymph node metastases.248 ,249 PET–CT has a higher accuracy than CT for distant and locoregional metastases, but is inferior to EUS.250–252
Before ER, neither CT nor PET–CT have a clear role in the staging of patients with Barrett's HGD or suspected T1 cancer and neither is routinely required (Recommendation grade B).
Initial evidence that endoscopic resectability (differentiation of T 1/2) could be predicted by EUS has been tempered by most of the recent series, which indicated that 15–25% of cases are understaged compared with ER, while about 4–12% are overstaged.253–256 One study compared endoscopic assessment with EUS and found that accuracy of both techniques in predicting depth of invasion was similar.257 High-frequency EUS miniprobes are more accurate than conventional EUS, but still fail to correctly stage T1 cancers in one-third of cases (Evidence grade Ib).258 Overall, these studies show that EUS misclassifies the T stage in approximately one-quarter of patients with early oesophageal cancer, and this has limited clinical impact over expert high-resolution imaging plus ER. However, in routine clinical practice, the endoscopist may not always be able to confidently exclude an advanced stage (T>1a) on the basis of the endoscopic appearance of nodular lesions, and, in this circumstance, EUS should be performed to guide the therapeutic choice.
EUS is the most accurate tool available for detecting regional lymph node involvement and can add staging information in patients with T1b disease after ER.231 ,249 ,259 Endosonographic criteria that are suggestive of malignant involvement of visible lymph nodes include a width greater than 10 mm, round shape, smooth border, and echo-poor pattern.260 When all four suspicious features are present, there is an 80–100% chance of metastatic involvement; however, only 25% of malignant nodes will have all of these features. Therefore, with the use of echo criteria alone, sensitivity and specificity for regional lymph node metastases were 80% (95% CI 75% to 84%) and 70% (95% CI 65% to 75%), respectively, in this study. FNA can determine more precisely whether or not suspicious lymph nodes are infiltrated, and it has high sensitivity in coeliac, mediastinal and perigastric lymph nodes.261 Sensitivity, specificity and accuracy of EUS FNA for locoregional lymph nodes are currently all around 85%262 (Evidence grade III). One cohort study on 25 patients with baseline HGD or intramucosal adenocarcinoma on biopsies has showed that EUS FNA of suspicious lymph nodes changed management decision in 20% of patients referred for endoscopic therapy of cases263 (Evidence grade III).
Since EUS can both overstage and understage T1 lesions, its routine use cannot be recommended for staging before ER for suspected early lesions (Recommendation grade B).
In selected cases where the endoscopist cannot exclude advanced stage on the basis of endoscopic appearance of nodular lesions, EUS with or without FNA is recommended to inform the therapeutic decision (Recommendation grade C).
EUS with or without FNA of visible lymph nodes is recommended in selected cases with T1b (sm1) disease on staging ER for which endoscopic therapy is selected, because of the significant risk of lymph nodal involvement (Recommendation grade C).
Ablative therapy for flat HGD/intramucosal cancer and residual Barrett's after ER
If HGD or intramucosal cancer are confirmed and there are no visible lesions after expert HRE review, then ablative therapy is the treatment of choice. After ER of any visible lesions, the stage and extent of disease will have been clarified. If disease is confined to the mucosa, then endoscopic therapy is preferred for eliminating the remaining Barrett's segment. Numerous case series on different endoscopic ablative techniques (PDT, argon plasma coagulation (APC), cryotherapy, RFA and step-wise radical ER) reported eradication rates of HGD ranging from 36% to 100%.228 ,264–270 Some were combined with ER for visible lesions. Randomised controlled trial data in patients with HGD are available for some of these techniques: PDT vs PPI,271 RFA vs Sham,132 APC vs PDT,272 RFA vs step-wise radical ER,273 PDT with ALA vs PDT with photofrin (porfimer sodium).274 All ablation modalities improve eradication compared with surveillance for HGD (Evidence grade Ib), but they should only be used as a primary treatment modality in the case of flat dysplasia.275 The studies with the best outcomes relate to PDT and RFA. ALA PDT has been showed to have a better safety and efficacy profile than photofrin PDT, but only in Barrett's shorter than 6 cm.274 Three-year follow-up data of RFA for HGD showed a reduced risk of progression to cancer compared with surveillance.132 ,276 RFA was associated with improvement in disease-specific health-related QOL,277 and this improvement appears secondary to a perceived decrease in the risk of cancer. Endoscopic treatment is associated with a higher rate of recurrence during follow-up; however, recurrent lesions can be effectively treated by further endoscopic therapy.114 ,212 RFA has been compared with step-wise ER for eradication of residual Barrett's epithelium after ER for HGD or mucosal OAC with equivalent efficacy, but with a higher stricture rate in the ER arm273 (Evidence grade Ib). Safety and tolerability were superior, with a decreased number of therapeutic sessions in the RFA group (Evidence grade Ib). RFA has not been compared with PDT, but patients with failed PDT have been successfully treated with RFA.278 PDT has a significant photosensitivity and stricture rate, therefore RFA appears to have a better safety profile and is easier to administer. In addition, RFA also has been associated with a lower incidence of buried glands than PDT and APC.279 ,280 Effectiveness in dysplasia eradication, safety profile and general aspects of all the techniques in patients with HGD are summarised in table 10. It transpires that the overall efficacy and safety profile support RFA as the best ablation modality currently available, as long as it is used for treatment of flat dysplasia only.
Summary of clinical profiles of different ablative techniques for HGD
In the presence of HGD or intramucosal cancer without visible lesions (flat HGD/intramucosal cancer), these should be managed with an endoscopic ablative technique. There is little comparative data among ablative techniques, but RFA currently has a better safety and side-effect profile and comparable efficacy (Recommendation grade C).
More than 20% of patients treated with ER of visible lesions develop metachronous lesions in the Barrett's segment within 2 years.114 Recurrence of neoplasia after ER can be significantly reduced if the residual Barrett's is completely ablated114 ,132 ,273 (Evidence grade III). After ER for early focal neoplasia, >80% of patients will have HGD or LGD detected in the remaining Barrett's epithelium.281 Eradication of the remaining Barrett's epithelium by RFA is a safe and effective treatment for any remaining flat dysplasia281 ,282 (Evidence grade III). Ablation may also be useful to avoid strictures, which are associated with step-wise radical ER of circumferential lesions, particularly with longer Barrett's segments.228 Combining ER with RFA reduces this risk and is effective in eradicating the remaining Barrett's epithelium273 (Evidence grade Ib).
Eradication of residual Barrett's oesophagus after focal ER reduces the risk of metachronous neoplasia and is recommended (Recommendation grade B).
Follow-up after endoscopic therapy
The goal of endoscopic mucosal resection and ablation is to eliminate the subsequent risk of cancer. This requires long-term follow-up data, which are not currently available for ablative techniques. From the limited studies available after ablation, new squamous (neosquamous) epithelium reveals no molecular abnormalities, and seems biologically stable.283 Five-year and 3-year follow-up data from the RCTs of PDT and RFA, respectively, in dysplastic Barrett's oesophagus showed a durable response to treatment.271 ,276 However, buried metaplasia has been reported within neosquamous epithelium biopsy specimens and this can predispose to the development of so-called ‘buried’ cancer.284 Current data suggest that the occurrence of buried glands is higher in patients treated with PDT (14.2%) compared with RFA (0.9%).279 Recurrence of Barrett's at the GOJ has been reported and seems important.285 Currently, follow-up is mandatory not only to detect recurrence but also to allow further therapy to be applied as required.4 Empirically, in patients treated for HGD, endoscopic follow-up is recommended 3-monthly for 1 year and yearly thereafter. This should include biopsies at the GOJ and within the previous extent of the Barrett's epithelium.
Pathological reporting of biopsies after ablation therapy
Ablation therapy is associated with an early acute and chronic inflammatory response, together with reactive epithelial changes followed by lamina propria fibrosis and duplication and splitting of the muscularis mucosae after a few months.244 Neosquamous epithelium is associated with ablation therapy, and interestingly can also be seen with PPI treatment without ablation therapy, especially after extensive biopsies.286 ,287 This neosquamous epithelium can replace the Barrett's segment, forming islands or sheets of ‘normal’ squamous epithelium. However, this may overlie buried glands or buried carcinoma.279 A systematic review has shown an overall incidence of buried glands in 14.2% of patients who received PDT and 0.9% of patients who received RFA.279 However one post-RFA study on the neosquamous epithelium found that only 37% of biopsy specimens contained lamina propria and deeper tissue suitable for assessment of buried metaplasia,283 whereas the other studies do not mention the presence of lamina propria in neosquamous biopsy samples.290 Buried dysplasia can be difficult to evaluate, particularly as the atypia does not reach the surface.244 Again p53 immunohistochemistry may be a helpful adjunct, as dysplastic glands may demonstrate a significant staining pattern.126 ,194 ,289 If there is uncertainty about the significance of the atypia present, then it is best to use the ‘indefinite for dysplasia’ reporting category. In summary, the importance of buried metaplasia after ablation remains unclear, as well as the adequacy of biopsies to detect it, leaving some uncertainties about the usefulness of biopsy specimens taken from the neosquamous epithelium. However, until further evidence becomes available, neosquamous epithelium biopsies are warranted.
Endoscopic follow-up is recommended after endoscopic therapy of Barrett's neoplasia with biopsy samples taken from the GOJ and within the extent of the previous Barrett's oesophagus (Recommendation grade B).
Surgical management of early Barrett's neoplasia
Efficacy and safety
For HGD and T1 OAC, case series suggest that the 5-year survival rates range between 80% and 90%, and the 3-year survival exceeds 90%.211 ,214 ,290 Tumour recurrence after resection of early cancer is rare (1%). There are no reports of long-term tumour recurrence in patients who have had complete surgical resection of HGD alone, and all-cause mortality is equivalent to non-surgical treatments211 ,290 ,291 (Evidence grade III).
Mortality for patients undergoing oesophagectomy for HGD or early adenocarcinoma is difficult to estimate because data are from retrospective studies conducted in self-selected high-volume centres, thus the quality of data was assessed as low. A number of case series21 ,292–301 evaluating over 500 patients with HGD or early adenocarcinoma show an operative mortality for oesophagectomy for HGD and early adenocarcinoma of less than 5%, with an overall operative 30-day mortality of approximately 2%. These results are comparable to the recent UK national audit results, where the mortality for 2200 patients undergoing oesophagectomy for any operable cancer (HGD excluded) was 3.8% for 30-day mortality and 4.5% for in-hospital mortality301 (Evidence grade III).
Surgical resection is associated with significant short-term morbidity (6–37%).290 ,303 A recent retrospective comparison of oesophagectomy (61 patients) versus endotherapy (40 patients) for HGD or T1 cancer in one centre revealed much lower morbidity in the endotherapy group with a similar survival, although follow-up was relatively short in the endotherapy group.214
Surgical therapy is considered the treatment of choice for early adenocarcinoma that has extended into submucosa because of the significant risk of lymph node metastasis (Recommendation grade B).
Volume effect in specialist surgical centres
Good observational data indicate that oesophageal surgery for treatment of adenocarcinoma should be performed in specialist centres, since patient outcomes have been shown to be better in high-volume centres and individual surgeons’ results improve with experience220 ,221 (Evidence grade III). The recent AUGIS guidelines on minimum surgeon volumes for oesophagogastric units recommend that each unit should consist of at least four surgeons carrying out a minimum of 15–20 resections per year.221
Oesophagectomy should be performed in high-volume centres, as these are associated with lower in-hospital mortality than low-volume centres (Recommendation grade B).
Type of surgery
Surgical resection for Barrett’s dysplasia and early cancer must include complete resection of the Barrett’s segment (longitudinal margins). Lymphadenectomy should be performed for T1 sm tumours because of the significant risk of lymph node involvement304–306 (Evidence grade III). There is insufficient evidence to support the use of one technique above the others. Attempts have been made to tailor a less radical, less morbid surgical procedure for these patients with early lesions who do not require extensive lymphadenectomy. These are not associated with a detrimental effect on long-term survival. However, the majority of surgical data come from retrospective observational studies, often comparing outcomes with outdated historical controls.
Data directly comparing the various techniques, or from series restricted to HGD and intramucosal cancer, are extremely limited. A series of 36 patients including left thoracoabdominal oesophagectomy (60%), transhiatal oesophagectomy (20%) and Ivor Lewis oesophagectomy (20%) reported no operative mortality and major complications in only 11% of patients.296 At a mean follow-up of 5 years, QOL outcomes were comparable to age- and sex-matched controls. A study of a further series of patients with HGD and T1 oesophageal cancer undergoing open surgery by either the transhiatal or transthoracic routes reports operative mortality of 2.5% and 5-year survival of 77%. This series included patients with tumour-involved lymph nodes, for whom survival is significantly impaired compared with patients with HGD307 (Evidence grade III).
Transhiatal oesophagectomy
Transhiatal oesophagectomy avoids the need for thoracotomy, with low in-hospital mortality (3%) and length of stay (50% discharges in 1 week) in one high-volume centre.308 Concerns about the adequacy of lymphadenectomy with this procedure may not apply in the context of HGD and intramucosal cancer. In an RCT, the transhiatal procedure was associated with less perioperative morbidity than a transthoracic procedure, and there was no significant difference in perioperative mortality (2% vs 4%, p=0.45).309 Long-term follow-up showed no difference in overall survival when all patients were considered, although a subgroup of patients with between one and eight lymph nodes involved had a better survival in the transthoracic procedure.310 This trial included patients with operable disease of all stages, but does suggest transthoracic oesophagectomy is a preferable procedure where there is a significant risk of lymphadenopathy such as in T1 sm disease (Evidence grade Ib).
Vagal-sparing oesophagectomy for HGD
The vagal-sparing technique aims to reduce the postoperative dumping and diarrhoea associated with oesophagectomy. A study of patients with HGD or intramucosal cancer found that the 49 patients who underwent vagal sparing oesophagectomy had shorter hospital stays and fewer major complications than 39 patients who underwent transhiatal procedures and 21 who underwent en bloc resections.297 Postoperative dumping syndrome and diarrhoea were decreased in the vagal-sparing group, and there was no detrimental effect on long-term outcomes. The vagal-sparing procedure does not involve a lymphadenectomy, and meticulous preoperative staging is required to exclude the presence of submucosal invasive disease, where the risk of lymph node involvement would make this procedure inadequate (Evidence grade III).
Merendino segmental oesophagectomy
A further option for HGD arising within a short (<3 cm) segment of Barrett's is a Merendino limited resection with jejunal interposition. In a series of 24 patients, this was associated with no operative mortality, significantly less perioperative morbidity than standard oesophagectomy, and a normal QOL at 1 year311 (Evidence grade III).
Minimally invasive laparoscopic or thoracoscopic oesophagectomy
The term ‘minimally invasive oesophagectomy (MIO)’ incorporates a very heterogeneous group of procedures. There are no RCTs reported comparing MIO with open surgery, although such a trial is currently underway in France312. A series of 222 patients undergoing MIO, including 47 with HGD, has shown that this procedure is safe, with a 30-day mortality of 1.4%. The median hospital stay was shorter than that usually seen in open surgery, at only 7 days, but the procedure remains associated with major complications including a leak rate of 11.7%313 (Evidence grade III).
A UK series has attempted to compare consecutive series of open Ivor Lewis and minimally invasive procedures. This group found that overall morbidity and mortality were similar for the two groups, but there were fewer pulmonary complications in the minimally invasive group (8% vs 23%)314 (Evidence grade III). A similar reduction in pulmonary complications was found in a recent study of early oesophageal cancer,315 with improved early QOL data in the first few months after surgery. In the recent UK national audit, there were 1541 open oesophagectomies performed for oesophageal cancer compared with 659 minimally invasive procedures. The postoperative morbidity and mortality were comparable in the two groups except that there were statistically significantly more anastomotic leaks in the minimally invasive group (10.8%)302 (Evidence grade III). Long-term outcome data are scarce in the patients having minimally invasive procedures.
Overall, there is insufficient evidence to support the use of one technique above the others. In summary, MIO is evolving and becoming more commonly used. As it develops, it is likely to offer some advantages over open oesophagectomy, although further data are required.
There is currently no evidence to support one technique of oesophagectomy over another. It is recommended that the procedure is tailored to the particular case and the expertise available in that centre (Recommendation grade C).
Quality of life
Patients having oesphagectomy report worse functional, symptom and global health-related QOL scores than before surgery. Oesophagectomy has a negative impact on QOL; the adverse effects lessen in patients who survive for 2 or more years.316 There is some evidence that QOL is improved with MIO compared with open surgery, at least in the short term.315 The evidence of QOL levels after MIO depend more on the curative effect than the mode of resection294 ,296 ,317–321 (Evidence grade III).
Follow-up after treatment of HGD or early carcinoma by surgery
There are three322–324 surgical follow-up series after oesophagectomy involving 102 patients with Barrett's oesophagus. These studies report that new Barrett's oesophagus can occur after curative subtotal oesophagectomy, with gastric conduit reconstruction for adenocarcinoma, squamous cell carcinoma or HGD. The development of Barrett's oesophagus occurs in half of patients studied and may recur from 6 months or less after surgery to 10 years after surgery. Even though a BADCAT consensus statement suggested an endoscopy at 2, 5 and 10 years after surgery,4 it is still unclear whether surveillance strategies after oesophagectomy are justified.
There is not sufficient data to recommend endoscopic surveillance after oesophagectomy for HGD or T1 adenocarcinoma provided that surgery has removed all Barrett's mucosa. Until further evidence is available, endoscopy should be performed on a symptomatic basis (Recommendation grade C).
Documentation and audit of treatment for HGD and early cancer
From 1 April 2012, the National Oesophago-Gastric Cancer audit has included patients with oesophageal HGD in Barrett's oesophagus as well as an ongoing audit of the management of invasive carcinoma.325 The initial estimate of the incidence of HGD in England and Wales is 1350 per year, which corresponds to around 45 patients per Cancer Network per year. In comparison, there are around 17 000 patients diagnosed with oesophagogastric cancer annually.
The National Audit collects data on staging, treatment and outcomes. The questions about the management of HGD patients have been kept simple, partly because their management is a complex and varied process within hospitals in England and Wales. The audit questions related to patients with oesophageal HGD are:
-
Has oesophageal HGD been confirmed by two GI pathologists?
-
What are the characteristics of the HGD at diagnosis (endoscopic appearance, length of Barrett's segment, characteristics of the lesion, focal or multifocal)?
-
Has the patient been discussed in a specialist MDT meeting?
-
What treatments were planned for the patient? (EMR, ablation or surgery)
-
What were the post-treatment pathology results?
-
What are the short-term outcomes of oesophagectomy in patients diagnosed with HGD?
Alongside the national oesophago-gastric audit, individual cancer centres are required, in accordance with the NICE guidance,5 to audit efficacy and safety of endoscopic therapy for Barrett's oesophagus. Other topics that should be considered for audit include the adherence to the Seattle protocol for Barrett's surveillance, the complication rate in patients undergoing Barrett's surveillance, and the compliance with the endoscopic minimum dataset for reporting Barrett's oesophagus. Auditing results will need to be used to implement changes in practice.
Findings and management decisions for HGD and early cancer should be entered into the National Audit (Recommendation grade C).
Economic considerations
Cost-effectiveness of endoscopic screening of patients with GORD with the aim to offer endoscopic surveillance to those with Barrett's oesophagus is highly controversial (see online supplementary table S2). There was wide divergence in cost-effectiveness estimates from US$12 336/quality-adjusted life years (QALY) gained to US$95 559/QALY gained, leaving huge uncertainty about the cost-effectiveness of this approach.326–329 Non-endoscopic devices could prove to be more cost-effective. A cost utility study using microsimulation modelling compared the Cytosponge and endoscopy as screening intervention in patients with GORD and found that they led to a similar QALY gained, but the Cytosponge was more cost-effective330 (Evidence grade III). Future studies in larger cohorts, such as the ongoing BEST2 study, are required to confirm whether the Cytosponge has sufficient diagnostic accuracy to be used as a screening intervention.
When comparing cost-effectiveness of surveillance of Barrett's oesophagus versus no surveillance, only one study found that endoscopic surveillance is cost-effective, while others found that surveillance was dominated by ‘do nothing’ or had an incremental cost-effectiveness ratio of about US$90 000/QALY gained, which is above conventional thresholds of what is considered to be cost-effective.331–334 When surveillance was analysed in the context of offering ablative therapy for dysplastic Barrett's oesophagus, endoscopic ablation proved to dominate and be cost-effective in patients with HGD in comparison with surgery, especially when RFA was modelled.217 ,335–337 However, none of these studies considered the cost of identifying patients with dysplasia in the first place—that is, surveillance of patients with non-dysplastic Barrett's oesophagus. In addition, most studies assumed ∼0.5% annual conversion rate to malignancy, whereas recent data suggests 0.3% may be more appropriate. This would make Barrett's surveillance more expensive per cancer identified and therefore less cost-effective. On the other hand, some models, reported before the advent of ablative therapies, provided more conservative estimates of cost-effectiveness than in the present era, due to the fact that ablative therapies are more cost-effective than surgery in patients with HGD. Some studies evaluated uncertainty in the assumptions made in the models using one-way sensitivity analyses. These do not capture all the uncertainty in the model, and probabilistic sensitivity analyses (PSA) should be conducted. Those that used extensive PSA approaches commented on substantial uncertainty in model estimates.333 Most papers evaluated cost-effectiveness from a third-party payer perspective (eg, healthcare system), and not from a societal perspective.
Overall, it is very unclear whether surveillance is cost-effective for non-dysplastic Barrett's oesophagus. More evidence is needed on natural disease progression, such as the ongoing BOSS trial. Furthermore, future models should: use more conservative estimates for conversion to malignancy; encompass non-endoscopic testing methods; evaluate the impact of ablative therapy in the context of surveillance; assess model uncertainty using PSA; and evaluate the cost-effectiveness from a societal perspective.
Endoscopic therapy, and in particular RFA and the combination of ER and RFA, has been proven to be more cost-effective then surgery. Despite the finding from the NICE cost analysis that surgery was the most cost-effective intervention,339 this has not taken into account the most recent data on more updated models, which showed that endoscopic therapy should be preferred to surgery from an economic perspective.217 ,330 ,340 However, some techniques such as RFA still carry significant costs, and other techniques such as ER require appropriate training to optimise the competence of the operator and ensure the best long-term outcome for the patient. Therefore, the recommendations regarding the minimum number of procedures required for training and for the maintenance of skills (section on Endoscopic therapy for Barrett's-related neoplasia) also have economic implications. In other words, the cost-effectiveness of endoscopic therapy is related to the proportion of patients that is successfully shifted from a surgical to an endoscopic pathway. In order to accomplish this, centralisation of endoscopic services in cancer centres is indicated to reduce costs as well as to improve patient management.
Despite the uncertainties of the cost-effectiveness of screening and surveillance, in these guidelines we have given a weak recommendation (grade C) for screening in selected cases and a moderate recommendation for surveillance (grade B). There are important clinical justifications for these choices. The recommendation of screening in selected cases is one of the very few measures currently available to modify the worrying epidemiological increase in OAC incidence over the last 30 years. The increasing incidence and poor outcomes for this disease have led to ‘a great pathological concern’, as highlighted in the 2008 Annual Report from the Chief Medical Officer.341 The future advent of cheaper and less invasive techniques for diagnosis will make screening more feasible and cost-effective. The recommendation for surveillance in Barrett's patients also emanates from a similar standpoint. However, we think we have made a step forward compared with the previous guidelines, in that we have identified subcategories of patients who could be discharged, because of very low cancer risk, and other subcategories of patients with intermediate risk where surveillance at less frequent intervals is justified, with potential positive impact on the cost-effectiveness of surveillance. Focus will therefore be shifted towards the higher-risk groups. Overall, until definite data will resolve the uncertainties about cost-effectiveness of surveillance, a conservative position on surveillance is justified.
There are insufficient data to indicate that endoscopic screening and surveillance for Barrett's oesophagus are cost-effective. Further studies on non-endoscopic diagnostic methods are awaited (Recommendation grade C).
Endoscopic therapy for dysplastic Barrett's oesophagus and early OAC is cost-effective compared with oesophagectomy (Recommendation grade B).
Strategies for chemoprevention and symptom control
Chemoprevention is defined as the use of pharmacological agents or surgical strategies to prevent the development of cancer. Most of the currently available evidence revolves around studies of PPIs and NSAIDs.
Acid suppression drugs
One prospective longitudinal cohort study found a significantly lower OR for developing dysplasia in patients treated with PPIs (0.25 (95% CI 0.13 to 0.47)) compared with patients receiving no therapy or histamine-2 receptor antagonists (H2RA)342 (Evidence grade III). A retrospective observational study found an OR of 0.43 (95% CI 0.21 to 0.83) in patients receiving PPIs compared with no medical therapy87 (Evidence grade III). When considering the balance of risks and benefits, these drugs are very safe, although long-term side effects including osteoporosis, GI infections and pneumonia need to be taken into account. On the other hand, the benefits, while not well understood, are potentially significant, and, while no placebo-controlled trial data are likely to be forthcoming, the data from the AspECT trial comparing low- versus high-dose PPIs are awaited. However, the vast majority of patients with Barrett's oesophagus have reflux symptoms and are recommended to take medical therapy for symptomatic control.7 An RCT comparing omeprazole 40 mg twice daily with ranitidine 150 mg twice daily found that the better acid suppression in the omeprazole arm correlated with a small but significant reduction in the length of the Barrett's oesophagus.343 These data must be interpreted carefully because of the subjectivity of endoscopic measurement of Barrett's oesophagus length, and a Cochrane review that pooled together data from two other RCTs did not confirm this finding.344 Another Cochrane review found that PPIs are more effective than H2RA for symptom control in patients with reflux disease345 (Evidence grade Ia).
There is not yet sufficient evidence to advocate acid suppression drugs as chemopreventive agents (Recommendation grade C).
Use of medications to suppress gastric acid production is recommended for symptom control (Recommendation grade A).
PPIs have the best clinical profile for symptomatic management (Recommendation grade A).
Antireflux surgery
Some surgical series have suggested that Nissen fundoplication can promote regression of Barrett's oesophagus and prevent progression to dysplasia;346–348 these results must be interpreted carefully, since these are small retrospective studies, which made little reference to pathological sampling error in very short segments of Barrett's oesophagus or to the subjectivity of a diagnosis of LGD (Evidence grade III). One series did find a significant progression rate to HGD of 0.8%/year in patients who underwent antireflux surgery.349 One RCT compared surgery with medical therapy and found no difference in progression rates between the two groups82 (Evidence grade Ib). There are no RCTs that compared surgery versus no therapy. Two RCTs comparing surgery versus PPIs found that they are both effective for symptom control, with a slightly better outcome in the surgical group350 ,351 (Evidence grade Ib).
Antireflux surgery is not superior to pharmacological acid suppression for the prevention of neoplastic progression of Barrett's oesophagus (Recommendation grade C).
Antireflux surgery should be considered in patients with poor or partial symptomatic response to PPIs (Recommendation grade A).
Non-steroidal anti-inflammatory drugs
In a recent meta-analysis of RCTs, low-dose aspirin at a dose of at least 75 mg reduced cancer mortality particularly after 5 years, with an OR of 0.63 (95% CI 0.49 to 0.83)352 (Evidence grade Ia). Both aspirin and NSAIDs have been associated in another recent meta-analysis with a 40% reduction in the risk of OAC.353 The crux of the debate lies in the risk/benefit ratio of aspirin, and this is currently unclear.354
While some have argued that the risk/benefit ratio is favourable, the true risks of GI bleeding and haemorrhagic stroke are, however, unclear. In this regard, it has been argued that the patients who suffer from aspirin-related GI bleeds tend to present early.355 ,356 However, recent evidence has indicated that the risk of bleeding in aspirin users seems more strongly associated with the dose than with the duration of aspirin.357 The AspECT is a randomised trial using a 2×2 factorial design in which patients are assigned to low- or high-dose PPI therapy with or without 300 mg aspirin. A total of 2513 patients have been enrolled, and this trial is specifically powered to answer questions about the role of aspirin in cancer prevention for Barrett's oesophagus. The results of this trial are awaited. Other agents such as statins, curcumin, multivitamin and antioxidants have been suggested to potentially prevent cancer progression in Barrett's oesophagus; however, evidence is not yet sufficient to draw conclusions on this subject.358–360
There is currently insufficient evidence to support the use of aspirin, NSAIDs or other chemopreventive agents in patients with Barrett's oesophagus (Recommendation grade C).
Patient perspective
Patients should be fully informed about their diagnosis and have an initial discussion about the pros and cons of surveillance. In the case of dysplasia (including indefinite, low grade and high grade), the diagnosis should be confirmed by an independent, expert histopathological review, and the patient should be informed of the diagnosis and the implications therein. When intervention is considered, the case should be reviewed by a specialist MDT for upper GI cancer, and the patient should have the opportunity to discuss the options in detail with experts from endoscopic and surgical disciplines.
All patients should be offered an appointment to discuss management decisions. When intervention is considered, therapeutic options should be discussed with an endoscopist as well as a surgeon (Recommendation grade C).
Future developments
The following developments would revolutionise the care of individuals with Barrett's oesophagus and should be priorities for policy makers and funders.
-
A non-endoscopic test(s) for diagnosis and surveillance
-
Studies to determine whether surveillance actually reduces mortality
-
Better understanding of the impact of screening and surveillance on QOL
-
More research into the use of advanced imaging modalities to improve dysplasia detection and cost-effectiveness of surveillance
-
Better risk stratification biomarkers to augment or replace the reliance on a histopathological assessment of dysplasia and better inform the indication for endoscopic ablative therapy
-
More studies on the natural history of Barrett's oesophagus, especially in the context of very short segments of columnar-lined epithelium, LGD and cases with particular molecular profiles
-
Research is required to inform the debate surrounding whether patients with LGD or no dysplasia should receive ablation therapy
-
Evidence that endoscopic therapies are durable and do not require long-term endoscopic monitoring or replacement of long-term surveillance with a cost-effective non-endoscopic technique
-
Studies to further delineate the role of chemoprevention
-
Health economic studies should be performed in parallel with trials to evaluate new management algorithms
-
Effects of current and future care pathways on patient QOL should be formally evaluated
It is difficult to forecast how long it will take to address these important questions, although it is likely that a time period of 5–7 years will be required before the majority of these questions will be answered. Nevertheless, we suggest that these guidelines should be reviewed in 4–6 years’ time or earlier to take into account emerging evidence. In addition, NICE guidelines produced in the interim will be complementary and essential to help implement these recommendations.
Acknowledgments
We are grateful to the BADCAT team for generating an evidence-based consensus review on management of Barrett's neoplasia, which has been used as an aid to the evidence base and recommendations for the sections on the management of dysplasia. We are grateful to Dr Nick Carroll (Department of Radiology, Cambridge University Hospitals) for his critical review of the section on radiological staging of Barrett's-related neoplasia. We would like to thank Dr Laurence Lovat and Professor Jacques Bergman, who are experts in the field, who provided an independent critical review of the guidelines. We are also grateful to Mimi McCord and Peter Benest, who provided valuable input from the patient perspective.
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors All the authors contributed to the literature search and manuscript writing of individual sections. All the authors approved the final version of the manuscript. Authors were divided in working groups as follows: definition of Barrett's, RCF, SS, KR; pathology section, PVK, SS, MO'D; risk factors and screening, PW, JL, J-YK, JAJ, RCF; endoscopic surveillance, KR, SS, YA, DL, MDP and NT; risk stratification and biomarkers, RCF, SS and EB-L; management of dysplasia and early cancer, KR, JAJ, PB, SA, SP, PP, JDC; economic considerations, PM, GL; chemoprevention, JAJ, MDP and RCF; manuscript editing, RCF, MDP and KR.
-
Competing interests RCF developed the Cytosponge technology which has been licensed by MRC-Technology to Covidien. RCF has no direct financial arrangement with Covidien. KR received educational and research grants, speaker and consultancy honoraria from Olympus/Keymed, and research support and speaker honoraria from Barrx/Covidien. MDP received educational grants form Olympus/Keymed, Pentax and Barrx/Covidien. JDC discloses occasional remunerated statements on OTC Zantac utility. PP receives financial support from Synmed Limited for the Wessex Barrett's charity. PB received educational grants from Olympus/Keymed. PM received speaker honoraria from AstraZeneca. JAJ has consultancies with AstraZeneca and Dr Falk.
-
Provenance and peer review Not commissioned; externally peer reviewed.