Article Text

Statistics from Altmetric.com
- BASL, British Association for the Study of the Liver
- BSG, British Society of Gastroenterology
- PSC, primary sclerosing cholangitis
- CEA, carcinoembryonic antigen
- US, ultrasonography
- CT, computed tomography
- MRI, magnetic resonance imaging
- MRCP, MR cholangiopancreatography
- ERCP, endoscopic retrograde cholangiopancreatography
- PTC, percutaneous transhepatic cholangiography
- TNM, tumour-node-metastasis
- LDH, lactate dehydrogenase
- 5-FU, 5-fluorouracil
1.0 GUIDELINES
1.1 Development of guidelines
There is currently no clear national consensus for the optimal diagnosis and treatment of cholangiocarcinoma. The need for these guidelines was highlighted following the annual meeting of the British Association for the Study of the Liver (BASL) in September 2000. During their development these guidelines were presented at a BASL Liver Cancer Workshop in January 2001. They were also circulated to BASL members and the Liver Section of the British Society of Gastroenterology (BSG) Committee members, including gastroenterologists, hepatologists, gastroenterological surgeons, pathologists, radiologists, and epidemiologists for comments before the final consensus document was drawn up.
1.2 Strategy
The guidelines are based on comprehensive literature surveys including results from randomised controlled trials, systematic reviews and meta-analyses, and cohort, prospective, and retrospective studies. On issues where no significant study data were available, evidence was obtained from expert committee reports or opinions. Where possible, specific recommendations have been graded, based on the quality of evidence available (section 2.4).
1.3 Context and intent
These guidelines are intended to bring consistency and improvement in the patient’s management from first suspicion of cholangiocarcinoma through to confirmation of the diagnosis and subsequent management. As stated in previous BSG guidelines, patient preferences must be sought and decisions made jointly by the patient and health carer, based on the risks and benefits of any intervention.
Furthermore, the guidelines should not necessarily be regarded as the standard of care for all patients. Individual cases must be managed on the basis of all clinical data available for that case. The guidelines are subject to change in light of future advances in scientific knowledge.
2.0 BACKGROUND
Mortality rates from intrahepatic cholangiocarcinoma have risen steeply and steadily over the past 30 years and since the mid 1990s more deaths have been coded annually in England and Wales as being due to this tumour than to hepatocellular carcinoma.1 In 1997 and 1998 cholangiocarcinoma caused almost 1000 deaths/year in England and Wales (approximately equal numbers of men and women). The cause of this rise is unknown and does not appear to be explained simply by improvements in diagnosis or changes in coding practice.1 The incidence of biliary cancers corresponds to mortality rates as the prognosis from these tumours is very poor.
2.1 Risk factors1,2
-
Age (65% of patients are over 65 years old).
-
Primary sclerosing cholangitis (PSC), with or without ulcerative colitis, is the commonest known predisposing factor for cholangiocarcinoma in the UK (lifetime risk 5–15%).
-
Chronic intraductal gall stones.
-
Bile duct adenoma and biliary papillomatosis.
-
Caroli’s disease (cystic dilatation of ducts, lifetime risk 7%).
-
Choledochal cysts (about 5% will transform, risk increases with age).
-
Thorotrast (a radiological agent no longer licensed for use, although the risk of cholangiocarcinoma lasts several decades).
-
Smoking (increased risk in association with PSC).
-
In SE Asia, where the tumour is quite common, the associated risk factors are:
– liver flukes—Opisthorchis viverrini and Clonorchis sinensis,
– chronic typhoid carriers—sixfold increased risk of all hepatobiliary malignancy.
2.2 Anatomical classification3–5
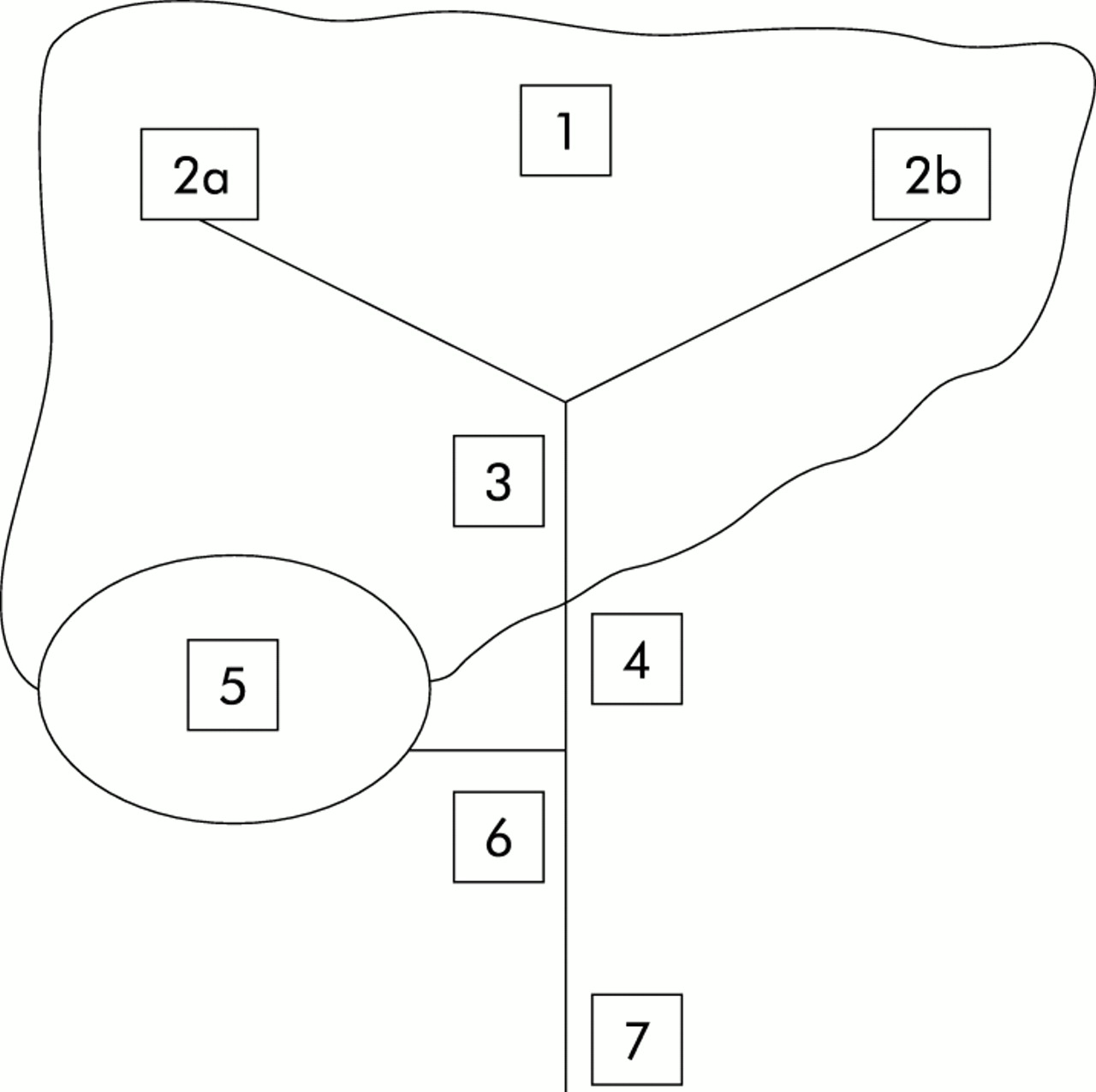
“Cholangiocarcinoma” originally referred only to primary tumours of the intrahepatic bile ducts and was not used for extrahepatic bile duct tumours but the term is now regarded as inclusive of intrahepatic, perihilar, and distal extrahepatic tumours of the bile ducts (fig 1).
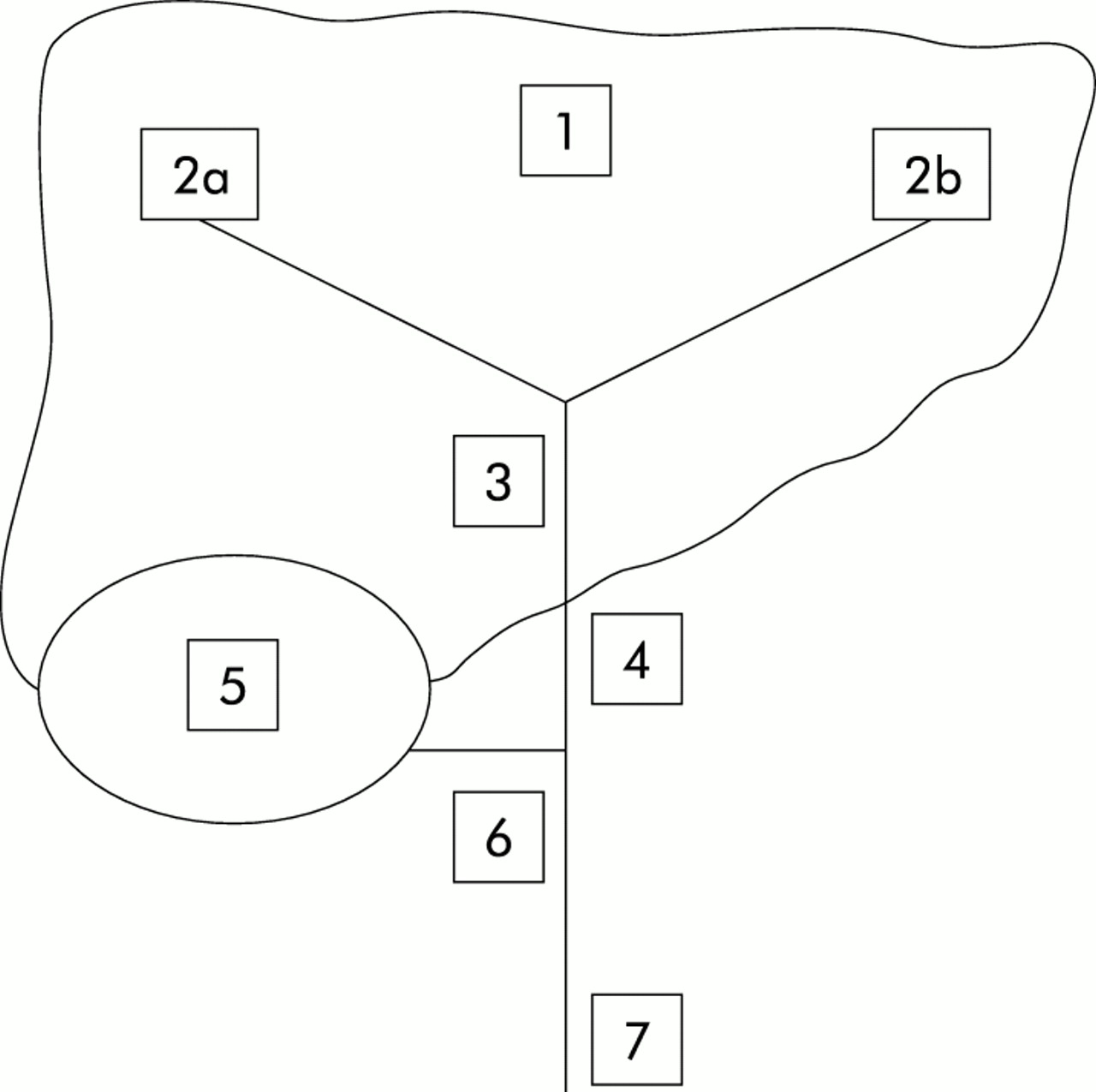
Schematic diagram for sites of cholangiocarcinoma. Intrahepatic cholangiocarcinoma (International Classification of Disease-9 codes (ICD-9) 155.1): 1=peripheral cholangiocarcinoma; 2a, b=right and left hepatic ducts; and 3=confluence of right and left hepatic ducts (perihilar, Klatskin tumours). Extrahepatic (ICD-9 156): 4=common hepatic duct; 5=gall bladder (ICD-9 156.0); 6=cystic duct; and 7=common bile duct.
-
20–25% are intrahepatic.
-
50–60% of all cases of cholangiocarcinoma are perihilar tumours (those involving the bifurcation of the ducts are “Klatskin” tumours).
-
Most Klatskin tumours may have been coded as intrahepatic tumours for purposes of death certification.
-
20–25% are distal extrahepatic tumours.
-
About 5% of tumours may be multifocal.
The extent of duct involvement by perihilar tumours may be classified as suggested by Bismuth:3
type I: tumours below the confluence of the left and right hepatic ducts;
type II: tumours reaching the confluence but not involving the left or right hepatic ducts;
type III: tumours occluding the common hepatic duct and either the right (IIIa) or left (IIIb) hepatic duct;
type IV: tumours that are multicentric or that involve the confluence and both the right and left hepatic ducts.
2.3 Pathology6–14
There are separate histological classifications of intrahepatic and extrahepatic cholangiocarcinomas. The WHO classifications are given below.
2.3.1 WHO classification of carcinomas of the liver
-
Hepatocellular carcinoma
-
Combined hepatocellular cholangiocarcinoma
-
Cholangiocarcinoma, intrahepatic
-
Bile duct cystadenocarcinoma
-
Undifferentiated carcinoma
2.3.2 WHO classification of carcinomas of the extrahepatic bile ducts
-
Carcinoma in situ
-
Adenocarcinoma
-
Papillary adenocarcinoma
-
Adenocarcinoma, intestinal-type
-
Mucinous adenocarcinoma
-
Clear cell adenocarcinoma
-
Signet ring cell carcinoma
-
Adenosquamous carcinoma
-
Squamous cell carcinoma
-
Small cell carcinoma (oat cell carcinoma)
-
Undifferentiated carcinoma
2.3.3 Histological grade
Most cholangiocarcinomas (95%) are adenocarcinomas. Adenocarcinomas are classified (1–4) according to the percentage of tumour that is composed of glandular tissue. Some types of adenocarcinoma are however not graded: carcinoma in situ, clear cell adenocarcinoma, and papillary adenocarcinoma. Signet ring cell carcinoma is given a grade of 3 and small cell carcinoma a grade of 4. Squamous cell carcinomas are graded according to the least differentiated areas. Most studies have demonstrated a relation between histological grade and postoperative outcome although stage is more important.
Levels of evidence lead to subsequent grading of recommendations as:
-
A=consistent level 1 studies;
-
B=consistent level 2 or 3 studies or extrapolations from level 1 studies;
-
C=level 4 studies or extrapolations from level 2 or 3 studies;
-
D=level 5 evidence or inconsistent or inconclusive studies of any level.
2.3.4 Molecular diagnosis15
-
Cholangiocarcinoma is often associated with inactivation of tumour suppressor genes—for example, p53, APC, Smad-4, bcl-2, and p16.
-
Mutations in oncogenes have also been described—for example, K-ras, c-myc, c-erbB-2, and c-neu.
-
Chromosomal aneuploidy has been reported in up to 25% of periampullary tumours.
-
Although these mutations can lead to detectable phenotypic changes, the diagnostic or prognostic usefulness of these developments is unclear and molecular profiling does not, as yet, have an established clinical role in patients with cholangiocarcinoma.
2.4 Levels of evidence16
Studies used as a basis for these guidelines are graded in relation to the quality of evidence according to the Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001).16 These are summarised in the appendix with explanatory notes, and have been reproduced with the permission of the Centre for Evidence-based Medicine.
3.0 DIAGNOSIS
3.1 Clinical features5,17
-
Most common presenting clinical features of perihilar or extrahepatic tumours are those of biliary obstruction: jaundice, pale stool, dark urine, and pruritus.
-
Right upper quadrant pain, fever, and rigors suggest cholangitis (this is unusual without drainage attempts).
-
Cholangiocarcinoma usually presents after the disease is advanced. This is particularly true with more proximal intrahepatic and perihilar tumours obstructing one duct, which often present with systemic manifestations of malignancy, such as malaise, fatigue, and weight loss.
-
Some cases are detected incidentally as a result of deranged liver function tests, or ultrasound scans performed for other indications.
3.2 Blood tests5,17
There are no blood tests diagnostic for cholangiocarcinoma. Liver function tests often show an obstructive picture with raised:
alkaline phosphatase
bilirubin
gamma glutamyl transpeptidase.
However, aminotransferases are frequently relatively normal but may be markedly raised in acute obstruction or cholangitis.
-
Prolonged obstruction of the common bile or hepatic duct can cause a reduction in fat soluble vitamins (A, D, E, and K) and increase prothrombin time.
-
With advanced disease, systemic non-specific markers of malignancy may be altered—for example, reduced albumin, haemoglobin, and lactate dehydrogenase (LDH).
Recommendations
-
As the sensitivity and specificity of individual tumour markers is low, patients should have a combination of serum tumour markers measured where diagnostic doubt exists. However, diagnosis should not rest solely on serum tumour marker measurements (recommendation grade C).
3.2.1 Serum tumour markers5,18–20 (evidence level 2b)
There are no tumour markers specific for cholangiocarcinoma. Overall, the sensitivity and specificity of tumour marker measurements are low but may be useful in conjunction with other diagnostic modalities where diagnostic doubt exists. There is no evidence that measurement of tumour markers is useful for monitoring tumour progression. CA 19-9, carcinoembryonic antigen (CEA), and CA-125 are currently the most widely used serum tumour markers.
CA 19-9
The value of CA 19-9 in patients with suspected cholangiocarcinoma is unclear. However:
CA 19-9 is elevated in up to 85% of patients with cholangiocarcinoma;
it has been reported that a CA 19-9 value greater than 100 U/ml has a sensitivity of 75% and specificity of 80% in patients with PSC;
CA 19-9 elevation can occur in obstructive jaundice without malignancy but persistently raised levels of CA 19-9 after biliary decompression suggest malignancy;
CA 19-9 does not discriminate between cholangiocarcinoma, pancreatic, or gastric malignancy and may also be elevated in severe hepatic injury from any cause;
the value of CA 19-9 for detecting cholangiocarcinoma in patients without PSC is unknown;
CA 19-9 may be useful for the differential diagnosis of cholangiocarcinoma but further studies are needed.
CEA
-
Carcinoembryonic antigen (CEA) is raised in approximately 30% of patients with cholangiocarcinoma.
-
CEA can also be elevated in inflammatory bowel disease, biliary obstruction, other tumours, and severe liver injury.
CA-125
-
This is elevated in 40–50% of cholangiocarcinoma patients.
-
It may signify the presence of peritoneal involvement but further studies are needed
Other serum tumour markers
Several other potential serum tumour markers have been linked to cholangiocarcinoma including CA-195, CA-242, DU-PAN-2, IL-6, and trypsinogen-2. Their clinical role is currently unclear.
3.3 Imaging5,17,21–31
3.3.1 Ultrasonography (US)5,17,21 (evidence level 4)
-
Remains the firstline investigation for suspected biliary obstruction.
-
Diagnosis should be suspected when intrahepatic, but not extrahepatic, ducts are dilated.
-
Intrahepatic cholangiocarcinoma may be seen as a mass lesion but this is unusual.
-
Gall stones excluded.
-
Often misses small perihilar, extrahepatic, and periampullary tumours and not good at defining the extent of the tumour.
-
Colour Doppler can detect tumour induced compression/thrombosis of the portal vein or hepatic artery.
3.3.2 Computed tomography (CT)5,17,21 (evidence level 4)
CT may provide good views of intrahepatic mass lesion, dilated intrahepatic ducts, and localised lymphadenopathy, however:
CT does not usually define the extent of cholangiocarcinoma,
abdominal lymphadenopathy is common in PSC and does not necessarily indicate malignant change,
suspected perihilar tumours or those involving the portal venous/arterial system should be studied by contrast enhanced spiral/helical CT.
3.3.3 Magnetic resonance imaging (MRI)5,22–28 (evidence levels 2b and 3a)
At present good quality MR is the optimal initial investigation for suspected cholangiocarcinoma, providing information on:
liver and biliary anatomy and local extent of the tumour,
extent of duct involvement by tumour with MR cholangiopancreatography (MRCP),
hepatic parenchymal abnormalities and presence of liver metastases,
hilar vascular involvement by MR angiography.
3.3.4 Cholangiography (MRCP, ERCP, and PTC)5,17,22–28 (evidence levels 2b and 3b)
-
Essential for early diagnosis of cholangiocarcinoma and assessing resectability.
-
MRCP is non-invasive and determines the extent of duct involvement by tumour without the risks of endoscopic retrograde cholangiopancreatography (ERCP) or percutaneous transhepatic cholangiography (PTC).
-
ERCP, when available, is usually favoured above PTC. However, ideally, facilities for PTC should always be available to deal with cases where attempts at ERCP have failed.
-
There is no clear evidence that PTC should generally be favoured over ERCP on the basis of the level of obstruction. However, PTC may be the modality of choice depending on local expertise and anatomical considerations.
-
ERCP or PTC allows bile sampling for cytology, which is positive in about 30% of cholangiocarcinoma cases. The yield may be improved by the use of thin preparations and cytospin.
-
Combined brush cytology and biopsy specimens increase yield to 40–70%.
-
Negative cytology from brushings does not exclude malignancy.
-
ERCP and PTC also allow stent insertion for palliative purposes in irresectable tumours (section 4.2).
-
Angiography in combination with cholangiography predicts resectability.
3.3.5 New techniques5,17,29,30
There are several new promising techniques that are under evaluation.
Endoscopic ultrasound
-
Allows good view of distal extrahepatic biliary tree, gall bladder, regional lymph nodes, and vasculature.
-
Facilitates guided fine needle aspiration/biopsy of lesions and lymph nodes.
Recommendations
Patients should have:
an initial US screening (recommendation grade C),
combined MRI and MRCP (recommendation grade B) (where MRI/MRCP is not available, patients should have contrast enhanced spiral/helical CT; recommendation grade C).
Invasive cholangiography should be reserved for tissue diagnosis or therapeutic decompression where there is cholangitis, or stent insertion in irresectable cases.
The above techniques may be complementary and sometimes all are necessary as part of a surgical assessment depending on the clinical situation
Recommendations
-
The role of these new imaging techniques in the diagnosis and staging of cholangiocarcinoma remains poorly defined, and they should best be performed within the context of clinical trials.
Positron emission tomography with [18F]-2-deoxy-d-glucose
-
Cholangiocarcinoma cells have high glucose uptake, like most malignancies.
-
Biliary epithelial cell metabolism is assessed in vivo via the glucose analogue [18F]-2-deoxy-d-glucose.
-
Glucose and [18F]-2-deoxy-d-glucose are both phosphorylated but the latter is not further metabolised and accumulates in cholangiocarcinoma cells giving rise to “hot” spots.
Other new techniques
-
Intraductal US, endoscopic/percutaneous flexible cholangioscopy, and radiolabelled ligand imaging.
3.3.6 Staging5,31 (evidence levels 4, 5)
Cholangiocarcinoma staging is based on the tumour-node-metastasis (TNM) system or alternatively:
stage I: tumour invasion limited to the mucosa or muscle layer;
stage II: local invasion;
stage III: as stages I and II but involving regional and hepatoduodenal lymph nodes or invasion of adjacent tissues;
stage IV: extensive invasion of the liver, adjacent structures, or lymph nodes, and/or distant metastases.
Once cholangiocarcinoma is suspected, comprehensive staging must be carried out to screen for metastatic disease. Up to 50% of patients are lymph node positive, and 10–20% have peritoneal involvement, at presentation. Clearly, previous imaging of US, CT, and MR are also part of staging. Spread to distant parts of the body is late and uncommon. Nevertheless, the following should be carried out:
chest radiography,
CT abdomen (unless abdominal MRI/MRCP already performed),
laparoscopy (most centres perform laparoscopy to determine the presence of peritoneal or superficial liver metastases in those considered resectable on imaging).
3.4 Confirmatory histology6–13,31,32 (evidence level 5)
Although positive histology and cytology are often difficult to obtain at ERCP, they are recommended for confirmation of a diagnosis of cholangiocarcinoma. Histology is also important for planning clinical trials. An adenocarcinoma is the usual histological subtype seen (see section 2.3.3 above). The only histological feature that allows a definite diagnosis of cholangiocarcinoma to be made is the presence of coexisting carcinoma in situ and this is uncommon. However, for patients with potentially curable (resectable) disease, open or percutaneous biopsy is not recommended due to the risk of tumour seeding.
Recommendations
-
The above investigations are advised as a grade C recommendation.
Recommendations
-
Confirmatory histology and/or cytology at ERCP, laparoscopy, or laparotomy should be obtained if at all possible. However, due to the risk of tumour seeding, surgical assessment of resectability should be established prior to the biopsy being performed (recommendation grade B).
3.5 Excluding metastatic disease33,34
Cholangiocarcinoma is sometimes very difficult to differentiate from metastatic adenocarcinoma, particularly if the pathological diagnosis is obtained from outside the biliary tree—for example, porta hepatis lymph node/mass or from liver metastases. Thorough clinical examination and other investigations are necessary to exclude a primary from elsewhere. The extent to which another possible primary is pursued and investigations done (some suggested below) will depend on the clinical situation in each individual case. Metastatic adenocarcinoma mimicking cholangiocarcinoma may arise from several organs, particularly:
pancreas—axial imaging (for example, MR, CT, EUS) (evidence levels 2b, 3a; recommendation grade B);
stomach— axial imaging, endoscopy (evidence levels 2b, 3a; recommendation grade B);
breast—clinical examination, mammography only if breast mass (evidence level 1b; recommendation grade A);
lung—chest radiography (evidence levels 2b, 3a; recommendation grade B);
colon—colonoscopy or spiral CT (evidence level 3a; recommendation grade B).
Serum tumour markers may also be useful—for example, LDH, α-fetoprotein (evidence level 3b; recommendation grade B).
4.0 TREATMENT
4.1 Surgery4,17,35–40 (evidence levels 2a–c, 3a, b)
Surgery is the only curative treatment for patients with cholangiocarcinoma. Surgery cures the minority of patients with cholangiocarcinoma, with a 9–18% five year survival for proximal bile duct lesions and 20–30% for distal lesions.
-
Bile duct cancers may be multifocal (5%).
-
Lymph node involvement is present in 50% of all patients at presentation and is associated with poor surgical outcome.
-
Peritoneal and distant metastases are present in 10–20% of all patients at presentation.
4.1.1 Resectable tumours
-
Patients’ suitability for major surgery should be guided by medical risk factors rather than age.
-
Resection involves a major operative procedure and requires appropriate surgical and anaesthetic experience.
-
Inadequate biliary drainage may increase the risk of sepsis and therefore surgery.
-
Surgical treatment principally depends on the site and extent of bile duct involvement by the tumour.
Recommendations (recommendation grade B)
-
For Klatskin tumours the Bismuth classification is a guide to the extent of surgery required (aim is tumour free margin of >5 mm):
– types I and II: en bloc resection of the extrahepatic bile ducts and gall bladder, regional lymphadenectomy, and Roux-en-Y hepaticojejunostomy;
– type III: as above plus right or left hepatectomy;
– type IV: as above plus extended right or left hepatectomy.
-
Segment 1 of the liver may preferentially harbour metastatic disease from hilar cholangiocarcinoma and removal should be considered with stages II–IV.
-
Distal cholangiocarcinomas are managed by pancreatoduodenectomy as with ampullary or pancreatic head cancers.
-
The intrahepatic variant of cholangiocarcinoma is treated by resection of the involved segments or lobe of the liver.
Survival depends on stage with tumour free margins with the absence of lymphadenopathy being the most important positive prognostic indicator.
-
Median survival for patients with intrahepatic cholangiocarcinoma:
– without hilar involvement is 18–30 months;
– with perihilar tumour is 12–24 months;
– five year survival rates of up to 40% have been reported for intrahepatic cholangiocarcinoma (best results in Japan), and 20% for hilar cholangiocarcinoma.
-
Reported five year survival for distal extrahepatic cholangiocarcinoma is currently 20–30%.
4.1.2 Liver transplantation for unresectable tumours39,40 (evidence level 3a, b)
-
Liver transplantation is currently contraindicated (recommendation grade B)
– It is usually associated with rapid recurrence of disease and death within three years.
– In pilot studies, liver transplantation following preoperative chemoirradiation for unresectable cholangiocarcinoma has resulted in long term survival of carefully selected patients and may be appropriate within clinical trials.
4.1.3 Palliative procedures
-
Surgical resection with palliative, rather than curative, intent is unproved.
-
Symptoms related to biliary obstruction in unresectable disease may be palliated by insertion of a biliary endoprosthesis (see below) rather than a surgical bypass. Stenting procedures resulting in adequate biliary drainage improves survival. Surgical bypass has not been demonstrated to be superior to stenting.
-
Irradiation (for example, brachytherapy or external beam radiation therapy, unproved in cholangiocarcinoma).
-
Intraoperative coeliac plexus block for pain control (unproved in cholangiocarcinoma).
-
Close liaison between oncological and surgical teams is important.
Recommendations
-
Routine biliary drainage before assessing resectability, or preoperatively, should be avoided except for certain clinical situations such as acute cholangitis (recommendation grade A).
4.1.4 Reporting surgical specimens7,8,10,12 (evidence level 5)
All surgical resection specimens from both intrahepatic and extrahepatic cholangiocarcinomas need to be reported in a systematic manner. The following information should be included in the final report (recommendation grade D):
(i) Tumour
-
histological type (see section 1.3),
-
histological grade (see section 1.3),
-
extent of invasion (according to the TNM system),
-
blood/lymphatic vessel invasion,
-
perineural invasion: this is very common and has been show to be associated with a worse outcome. It is also very useful in making the diagnosis of invasive cancer.
(ii) Margins
These must be adequately sampled because it has been shown that local recurrence is related to involvement of the margins. This is particularly important because extrahepatic cholangiocarcinomas may be multifocal (5%).
(iii) Regional lymph nodes
To stage the lymph nodes accurately, the lymph node groups must be specifically identified. It should be noted that peripancreatic nodes located along the body and tail of the pancreas are considered sites of distant metastasis.
(iv) Additional pathological findings
These must be noted if present—for example, carcinoma in situ, sclerosing cholangitis.
(v) Metastases
To other organs or structures.
4.2 Biliary decompression and stents41–47
4.2.1 Stenting prior to surgery (evidence level 1a)
-
Stents ideally should not be inserted prior to assessing resectability.
-
Although the routine use of preoperative biliary drainage is not recommended, in certain patients who are severely malnourished, or who are suffering from acute suppurative cholangitis, preoperative drainage may be beneficial.
-
Preoperative placement of biliary catheters may be a useful technical aid in patients requiring a difficult hilar dissection for proximal biliary diseases.
4.2.2 Stents alone for palliation of jaundice (evidence levels 2a-c, 4)
-
Stents are used to maintain adequate biliary drainage and relieve symptoms.
-
Most stents are inserted endoscopically and are initially plastic.
-
The use of MRCP to plan endoscopic stent placement in complex hilar tumours may reduce the risk of postprocedure cholangitis.
-
In patients with complex hilar lesions, retrospective case control studies suggest that bilateral versus unilateral endoscopic/percutaneous biliary drainage may result in improved jaundice, postprocedure cholangitis, and survival, although this was not confirmed in a recent randomised trial
Recommendations
-
If the initial plastic stent becomes blocked, replacement with a metal stent is favoured if the estimated survival is expected to be greater than six months (recommendation grade B).
-
Surgical bypass should be re-considered in patients with a good estimated life expectancy where stenting has failed (recommendation grade C).
Plastic versus metal stents
-
Cost analysis has demonstrated that metallic stents are advantageous in patients surviving more than six months whereas a plastic stent is satisfactory for patients surviving six months or less.
-
Placement of metal stents may be associated with shorter hospital stay and lower hospital costs overall.
-
Tumour growth through the mesh of metal stents may lead to further problems with biliary obstruction. This may be overcome by inserting plastic (Cotton-Leung) stents through the lumen of the metal stent or placement of a further mesh metal stent where technically possible.
-
Mesh metal stent occlusion may give rise to complex biliary obstruction and sepsis.
-
Alternatively, semicovered stents have been recently developed which reduce tumour ingrowth but are as yet unproved to have superior long term patency.
4.2.3 Complications of stenting
-
Complications of endoscopy.
-
It should be noted that following palliative stenting, patients can die from recurrent sepsis, biliary obstruction, and stent occlusion as well as disease progression.
4.3 Oncological approaches48–55 (evidence levels 2–4)
Surgery is the only curative treatment for patients with cholangiocarcinoma but it is only effective in a minority of cases. At presentation, half of all cholangiocarcinomas have lymph node metastases. Thus successful non-surgical oncological approaches could have a significant beneficial impact on this disease, on the majority of patients if efficacy could be demonstrated. However, to date, the level of evidence for the majority of published studies is 2a or less.
-
To date, a review of over 65 disparate studies using chemotherapy and/or radiation suggests that there was no strong evidence of survival benefit. However, most studies were small, lacked control groups (phase II), and were difficult to interpret, particularly as radiological responses for cholangiocarcinoma are not easy to document.
-
As a general guide from published trials:
– (i) patients who are relatively healthy, stable, and not deteriorating rapidly should be treated early in their course of disease rather than wait for their disease to progress. The performance status is generally the most important prognostic factor (patients with a Karnofsky47 status of 50 or more that are not rapidly deteriorating are usually suitable);
– (ii) good symptom control is paramount throughout and requires multidisciplinary team input;
– (iii) in those patients on treatment in whom quality of life is preserved or improved, a survival benefit is more likely. Thus quality of life should probably be the primary focus and survival a secondary end point in disease management;
– (iv) achieving stable disease (or lack of objective progression) in patients on therapy has value that can be translated into both length and quality of life, and so should not be underestimated as a surrogate end point. This is particularly important because of the frequent difficulty in confirming objective radiological responses, particularly in the perihilar area.
Trial approaches may involve chemotherapy, radiotherapy (external beam, intraoperative, intraluminal brachytherapy), or combinations of the above with or without surgery. Presurgical approaches attempting down staging are classified as “neoadjuvant” and immediately postsurgical as “adjuvant”.
4.3.1 Chemotherapy49,52–54
-
In advanced disease, one randomised study of combination chemotherapy versus best supportive care reported a significantly improved survival (four months of benefit) and quality of life to the chemotherapy arm. (The study also included pancreatic cancers with a positive result although the analysis was separate.)
-
There is currently no evidence to support postsurgical adjuvant therapy outside a trial setting.
-
Conclusions from predominately phase II studies suggest:
– (i) cholangiocarcinomas are relatively chemosensitive, with most studies being 5-fluorouracil (5-FU) based, and 10–20% partial response rates to (older) single agents;
– (ii) partial response rates to newer single agents, such as gemcitabine, vary from 20% to 30%;
– (iii) partial response rates to recent phase II combinations vary from 20 to 40%.
– Gemcitabine in combination with cisplatin shows 30–50% partial response rates. It is encouraging that several patients have been clearly documented as being down staged and converted to operability in some phase II studies, with occasional long term survivors.
-
the chance of responding appears to be correlated with performance status at the outset. Quality of life is significantly improved, particularly in responders.
Currently, a European study of infusional 5-FU with cisplatin compared with infusional 5-FU (EORTC-GITCCG randomised phase II) is recruiting. Oral 5-FU analogues are also now available (UFT-tegafur or capecitabine).
Targeted chemotherapy through the hepatic artery or portal vein has been shown to achieve greater local drug concentrations and improved response rates (44% in one phase II study) but because of the patterns of relapse, it is unlikely to replace systemic chemotherapy entirely.
4.3.2 Radiotherapy 49–51,55
(a) External beam radiotherapy (and chemoradiation)
-
There is currently no evidence to support adjuvant postoperative radiation therapy. Radiotherapy did not improve survival or the quality of life in patients with resected perihilar cholangiocarcinoma when assessed prospectively.
-
There is no evidence for radiotherapy improving survival or the quality of life in advanced disease. There is significant toxicity from current methods of delivery and no evidence of disease sterilising effects without significant morbidity.
-
The role of chemoradiation (chemotherapy combined with local radiation) remains to be established in randomised clinical trials as local and systemic toxicity is also concomitantly increased.
-
Radiation alone still has potential important palliative value for painful localisable metastases, uncontrolled bleeding, etc.
Recommendations
-
All patients who have inoperable tumours, or who are operable but have not been rendered disease free, or those patients with recurrences should be actively encouraged to participate in chemotherapy and/or radiotherapy clinical trials (recommendation grade B).
(b) Local radiation techniques: intraoperative or intraluminal brachytherapy
-
A few uncontrolled studies using intraluminal brachytherapy (iridium implants), combined with external beam irradiation, have suggested a benefit. In one study, median survival rates reached about 10 months compared with seven months in patients managed by stenting alone.
-
Median survival using a combination of external beam irradiation, transcatheter iridium, and chemotherapy (fluorouracil) was 13 months in another uncontrolled study.
-
In advanced disease, liver and abdominal cavity relapse were the major causes of progression in these and other radiotherapy studies.
Thus although intraoperative radiotherapy and intraluminal brachytherapy appear promising, the studies do not support their use in isolation and there are no controlled data confirming their value in comparison with standard chemotherapy, chemoradiation, or stenting alone.
Oncology conclusion
Definitive evidence from large randomised studies for a survival benefit of non-surgical oncological intervention compared with best supportive care is still lacking. Patients with advanced cholangiocarcinoma should therefore be actively offered the opportunity to participate in clinical trials as there are many newer promising agents and combinations with potential improved efficacy and tolerability. In chemotherapy trials, good performance status patients appear to have the most significant benefit in terms of quality of life.
4.4 Recurrent bile duct cancer
The prognosis for any treated patient with progressing, recurring, or relapsing bile duct cancer is poor. Further treatment depends on several factors, including prior treatment and site of recurrence, as well as individual patient considerations. Relief of recurrent jaundice usually improves quality of life. Clinical trials, of chemotherapy in particular, may be appropriate and should be considered when possible.
A management algorithm for cholangiocarcinoma is shown in fig 2.

{kind=link}
{kind=link}
Management algorithm for cholangiocarcinoma. US, ultrasonography; MRCP, MR cholangiopancreatography; MRA, MR angiography; ERCP, endoscopic retrograde cholangiopancreatography; PTC, percutaneous transhepatic cholangiography. *Where magnetic resonance imaging/MRCP is not possible, patients should have contrast enhanced spiral/helical computed tomography. **Fine needle biopsy or biopsy is ideally avoided until resectability has been assessed by a specialist surgeon.
5.0 REVISION OF GUIDELINES
We recommend that these guidelines are regularly audited and we request feedback from all users. These guidelines should be formally revised within three years of publication or sooner in light of new evidence.
6.0 APPENDIX: LEVELS OF EVIDENCE
Levels of evidence are shown in table A1.
Levels of evidence