Article Text

Abstract
Background: Combined pegylated interferon and ribavirin has improved chronic hepatitis C (CH-C) therapy; however, sustained virological response is achieved in only about half of the patients with a 1b genotype infection. We assessed oral ursodeoxycholic acid (UDCA) on serum biomarkers as a possible treatment for interferon non-responders.
Methods: CH-C patients with elevated alanine aminotransferase (ALT) were assigned randomly to 150 (n = 199), 600 (n = 200) or 900 mg/day (n = 197) UDCA intake for 24 weeks. Changes in ALT, aspartate aminotransferase (AST) and gamma-glutamyl transpeptidase (GGT) were assessed. This study is registered at ClinicalTrial.gov, identifier NCT00200343.
Results: ALT, AST and GGT decreased at week 4 and then remained constant during drug administration. The median changes (150, 600 and 900 mg/day, respectively) were: ALT, −15.3, −29.2 and −36.2%; AST, −13.6, −25.0 and −29.8%; GGT, −22.4, −41.0 and −50.0%. These biomarkers decreased significantly less in the 150 mg/day than in the other two groups. Although changes in ALT and AST did not differ between the 600 and 900 mg/day groups, GGT was significantly lower in the 900 mg/day group. In subgroup analysis, ALT decreased significantly in the 900 mg/day group when the baseline GGT exceeded 80 IU/l. Serum HCV-RNA did not change in any group. Adverse effects were reported by 19.1% of the patients, with no differences between groups.
Conclusions: A 600 mg/day UDCA dose was optimal to decrease ALT and AST levels in CH-C patients. The 900 mg/day dose decreased GGT levels further, and may be preferable in patients with prevailing biliary injuries.
Statistics from Altmetric.com
Chronic hepatitis C (CH-C) is a common liver disease worldwide. The prevalence of hepatitis C virus (HCV) infection increased recently in several countries1 and has now resulted in a growing incidence of HCV-related hepatocellular carcinomas.2 3 Following the discovery of HCV, interferon therapy was established as the only treatment to eliminate the viral infection. The introduction of combination therapy with pegylated interferon and ribavirin has substantially enhanced the efficacy of antiviral therapy.4 5 However, the HCV genotype 1b, the major genotype in Japan, is refractory even to this combination therapy and only shows sustained virological response rates of about 50%. Moreover, interferon therapy is sometimes contraindicated or stopped early due to haematological, psychological and other complications.
Ursodeoxycholic acid (UDCA) is a hydrophilic stereoisomer of chenodeoxycholic acid which was used first to dissolve cholesterol gallstones and recently to treat primary biliary cirrhosis.6 7 In 1985, Leuschner et al reported a decrease in serum aminotransferase levels in patients with HBV-negative chronic hepatitis who were given UDCA for concomitant gallstones.8 Traditional Chinese medicine uses ursine bile for liver diseases; it contains plentiful UDCA and inspired the chemical name. Semi-synthetic UDCA became commercially available in Japan in 1957 and has been used since then for chronic liver disease. In 1994, Takano et al reported a randomised, controlled-dose study of UDCA for CH-C: 57 patients were assigned randomly to take 150, 600 or 900 mg/day of UDCA and compared with 17 control patients.9 The authors showed that serum levels of alanine aminotransferase (ALT), aspartate aminotransferase (AST) and gamma-glutamyl transpeptidase (GGT) decreased less with 150 mg/day, the dose recommended by the Japanese national health insurance policy at that time, than with 600 or 900 mg/day, while the results with the latter two doses were similar. Although the effects of UDCA on fibrosis progression rates have not been established, the strong association between serum ALT levels and fibrosis progression rates has been well documented.10 11 and it can be speculated that a decreased ALT level is associated with delayed fibrosis progression. Thus, the present study was conducted primarily as a dose-finding trial, using the changes in ALT levels as the primary endpoint.
PATIENTS AND METHODS
Patients
Patients with CH-C who were 20 years of age or older and tested positive for HCV-RNA or HCV core proteins were recruited as candidates for this study. They were observed for 8 weeks prior to administration of the drug, and those who showed ALT of 61 IU/l or higher in week −4 were enrolled. Patients were excluded from the study if they had received antiviral treatment (interferon with or without ribavirin) within 20 weeks before the observation period or were treated with corticosteroids, immunosuppressive drugs, glycyrrhizic acid, cholestyramine or other drugs that may affect liver function or interfere with UDCA metabolism. Patients were also excluded if they: i) had decompensated cirrhosis, viral hepatitis other than hepatitis C, autoimmune liver disease, alcoholic or drug-induced liver injury, malignant tumour, biliary disorder, fulminant hepatitis or peptic ulcer; ii) required hospitalisation for cardiac, renal or pancreatic disease; iii) were pregnant or lactating; iv) alcohol dependent or drinking more than approximately 22 g/day alcohol; v) were participants in another clinical study within 4 weeks before the observation period; or vi) were sensitive to UDCA or other bile acid preparations.
The protocol was approved by the ethics committee of each institution participating in the study. Patients were informed of the details of the clinical study and agreed to participate. We conducted this clinical study in accordance with the Declaration of Helsinki and good clinical practice.
Study design
After the 8-week observation period patients were treated with oral (prandial) UDCA (Urso, Mitsubishi Pharma, Osaka, Japan) for 24 weeks at 150, 600 or 900 mg/day, divided into three doses, under double-blind conditions. Double blinding used placebo, 50 and 100 mg tablets identical in appearance to the test drug. The UDCA doses were established from a previous clinical study of UDCA in patients with CH-C.9 Concomitant use of drugs and therapies included in the exclusion criteria were prohibited throughout the observation and treatment periods.
Changes in serum ALT levels were previously reported to be −26% and −25.5% with 600 and 900 mg/day of UDCA, respectively, compared to untreated controls and no significant changes were observed with 150 mg/day.9 Based on these data, we assumed a standard deviation of 30% for per cent changes in ALT, and the necessary sample size was calculated to be 200 in each group to detect any superiority of the 600 and 900 mg/day doses over 150 mg/day at a significance level of 0.05 and a power of 0.9.
We enrolled patients who met all criteria and gave written informed consent between July 2002 and May 2004 in 62 institutions with liver clinics throughout Japan. Each patient was assigned randomly to one of the three dose groups by using numbered containers provided based on a permuted block method (block size: 6).
When treatment or evaluation was discontinued because of patient request, aggravation of symptoms, adverse events or other reasons, prior data were included in the evaluation as final observation data.
To investigate the long-term effects of UDCA, the protocol included an option for additional UDCA administration for a minimum of 28 weeks and a maximum of 80 weeks (total 52–104 weeks including the initial 24 weeks) if the ALT level had decreased by at least 15% at week 20 compared to the baseline. In the additional period, the double-blind setting was discontinued and the dose of 600 mg/day was adopted, which could be increased to 900 mg/day by the decision of each patient and the physician responsible. Patients who entered the additional phase could discontinue UDCA administration anytime after week 52.
Laboratory tests
Blood was collected every 4 weeks from the start of the observation period to the end of drug administration. Serum ALT was measured as a primary endpoint of liver function, and AST and GGT as secondary endpoints, using conventional methods. Blood samples taken at the start of observation, at 0, 4 and 12 weeks of treatment, and at the final observation were analysed to determine leukocyte and erythrocyte counts, haemoglobin, haematocrit, thrombocyte count, and the levels of ALT, AST, GGT, alkaline phosphatase, lactate dehydrogenase, total protein, albumin, cholinesterase, total bilirubin, direct bilirubin, total cholesterol, urea nitrogen, creatinine, Na, K and Cl.
For bile acid composition analysis, blood was collected at the start of treatment and at the final observation in a fasted condition. Serum total bile acid was measured by the 3α-hydroxysteroid dehydrogenase method. Bile acid fractions were determined by a specific liquid chromatography-electrospray mass spectrometry, using an HPLC system (Agilent 1100 series, Agilent Technologies, CA, USA) equipped with a C18 cartridge (CAPCELL PAK C18 UG120A, Shiseido, Tokyo, Japan) and a mass spectrometer (Quattro Ultima, Micromass Technologies, Manchester, UK).
Serum HCV-RNA level was measured prior to treatment and at the final observation by a reverse transcriptional polymerase-chain-reaction method.
All analyses and measurements were performed in a single contract laboratory (SRL, Tokyo, Japan).
Statistical analysis
Patients’ backgrounds were compared among the three dose groups by χ2 test and ANOVA. Changes in serum ALT, AST and GGT levels due to UDCA administration were compared among the groups by repeated-measure ANOVA. Differences between groups were tested by using linear contrasts. Subgroup analyses of median changes in serum ALT at the final observation, relative to the pre-treatment levels, were performed according to gender, body weight and pre-treatment serum GGT level with Wilcoxon signed-ranks tests. Changes in bile acid and serum HCV-RNA levels were analysed by paired Student’s t test. Fischer’s exact probability test was applied to the incidences of adverse reactions. A p value <0.05 in a two-tailed test was considered significant. Analyses were done on the full analysis set. This study is registered at ClinicalTrial.gov, number NCT00200343, and is compliant with the published CONSORT guidelines for performance and publication of clinical trials.12
RESULTS
Patients
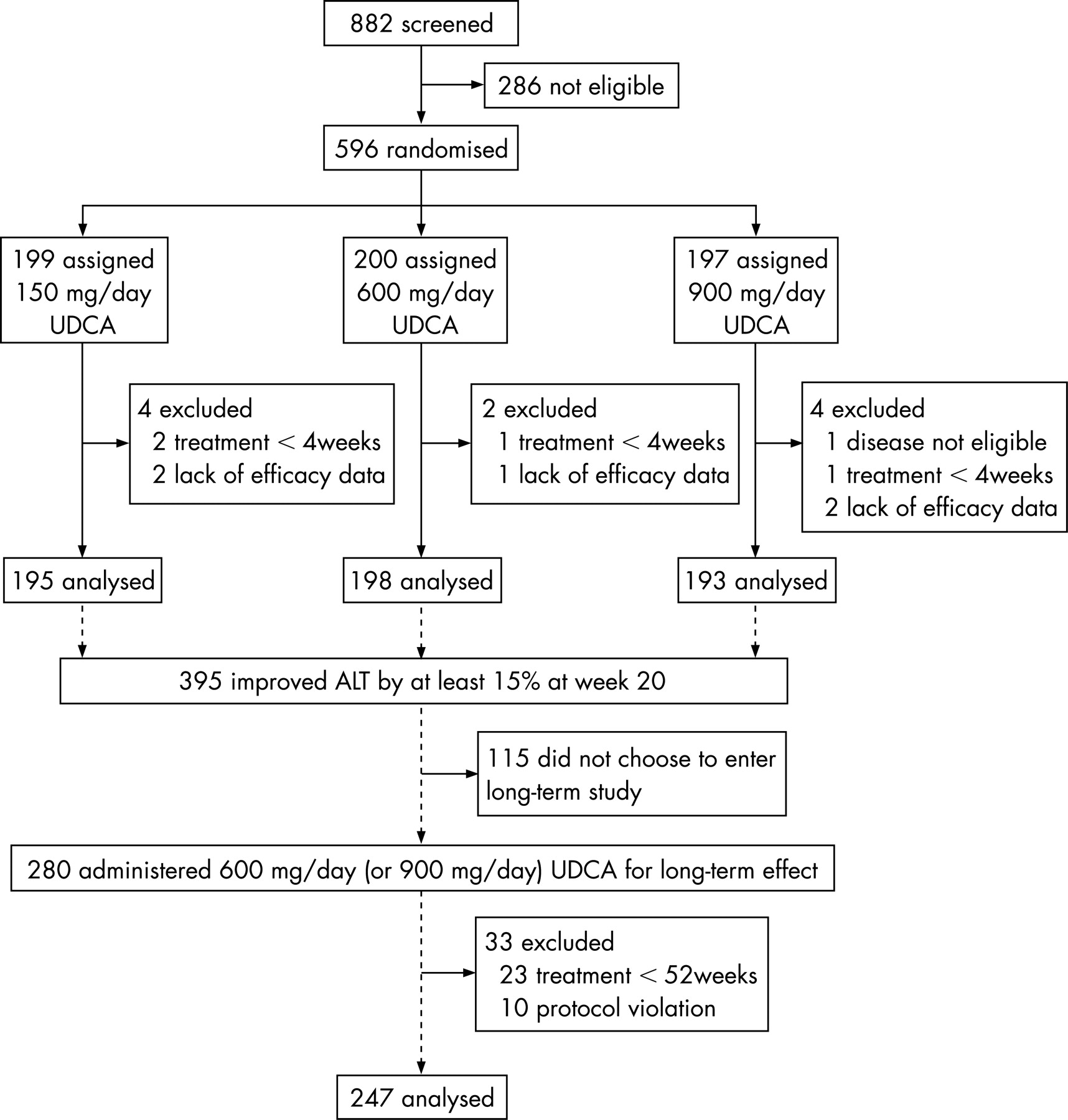
We enrolled 596 patients; 199 received UDCA at 150 mg/day, 200 at 600 mg/day, and 197 at 900 mg/day. Safety was evaluated in all patients as adverse events based on signs and symptoms and abnormal laboratory test results. Efficacy was evaluated in 586 patients (195, 150 mg/day; 198, 600 mg/day; and 193 at 900 mg/day), excluding 10 who lacked sufficient data. At the end of 24 weeks’ administration, 392 patients were eligible for additional long-term administration. Of these patients, 280 chose to participate in the study and others refused mainly because of lack of time. Twenty three patients discontinued before week 52, one of them for biochemical relapse, and other 10 patients violated protocol. The effects of long-term administration were evaluated among the remaining 247 patients (fig 1).
Patients’ backgrounds are summarised in table 1. Differences observed in gender, body weight and history of treatment with interferon between the three groups are indicated (p<0.15).
Changes in ALT, AST and GGT
Serum ALT, AST and GGT levels before and during treatment are shown in figs 2–4. The responses of ALT, AST and GGT over time were greater for 600 and 900 mg/day administration compared to 150 mg/day (ALT, p<0.001 and p = 0.021; AST, p<0.001 and p<0.001; GGT, p<0.001 and p<0.001, respectively). No difference was observed between the 600 and 900 mg/day groups in ALT (p = 0.926) or AST (p = 0.429), but GGT differed significantly (p<0.001). Serum ALT, AST and GGT levels decreased by 4 weeks into treatment and remained constant. Serum ALT, AST and GGT levels at the final observation, together with median changes relative to 0 week (baseline), are shown in table 2. The mean decreases in serum ALT levels from the baseline value were 13.4, 30.6 and 29.3 IU/l in the 150, 600 and 900 mg/day groups, respectively. The median changes in ALT at the final observation were −15.3%, −29.2% and −36.2% in the corresponding groups (table 2).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
The mean decreases in serum AST levels from the baseline value were 8.5, 19.3 and 19.7 IU/l in the 150, 600 and 900 mg/day groups, respectively. The mean decreases in serum GGT levels from the baseline value were 17.1, 32.7 and 42.1 IU/l in the 150, 600 and 900 mg/day groups, respectively.
Long-term effects
The decreases in ALT, AST, GGT levels from the baseline value were maintained during long-term administration of UDCA, as shown in table 3.
Subgroup analyses
The decrease in serum ALT was significantly greater in the 600 and 900 mg/day groups than in the 150 mg/day group for most subgroups by gender, body weight or baseline serum GGT levels (table 4). Although the difference between the 600 and 900 mg/day groups as a whole was not significant, the subgroup of baseline GGT⩾80 IU/l showed a significantly lower level of GGT with 900 mg/day administration (p = 0.004).
Bile acid in serum
Total bile acid concentration in serum increased in a dose-dependent manner from the start of drug administration to the final observation, as shown in table 5. The ratio of UDCA to total bile acid was increased significantly in all groups at the final observation compared to baseline. The ratio of UDCA at the final observation was similar in the 600 and 900 mg/day groups. The proportion of less hydrophilic bile acids was decreased accordingly. The proportion of chenodeoxycholic acid at the final observation was decreased significantly in all groups, and was similar in the 600 and 900 mg/day groups. The proportions of cholic acid and deoxycholic acid were also decreased significantly compared to baseline.
Virus load
HCV-RNA levels (mean±SD) changed from the baseline of 1477±1280 to 1366±1224 kIU/ml in the 150 mg/day group, from 1463±1299 to 1358±1233 kIU/ml in the 600 mg/day group, and from 1553±1318 to 1552±1398 kIU/ml in the 900 mg/day group. None of these changes was significant.
Safety
The observed adverse reactions possibly associated with UDCA administration are shown in table 6. The overall incidences of adverse reactions were 18.1%, 21.5% and 17.8% in the 150, 600 and 900 mg/day groups, respectively, with no significant difference between the groups. Diarrhoea was reported most often. No severe adverse reactions were seen.
DISCUSSION
UDCA is frequently used for cholestatic liver diseases, primary biliary cirrhosis in particular. UDCA improves biochemical indices such as serum GGT, ALT and bilirubin. Histopathological improvements have been shown13 and prolonged survival reported.14 15 Although its effect on survival remains controversial,16 17 UDCA is the only approved medication for primary biliary cirrhosis. Suggested mechanisms for UDCA include reducing the cytotoxicity of hydrophobic bile acids, stimulating hepatobiliary secretion and anti-apoptosis.18
UDCA was used to decrease serum aminotransferase levels for so-called non-A non-B chronic hepatitis before the discovery of HCV.8 19 20 Takano et al restricted their study to patients with CH-C and found the optimal dose of UDCA to be 600 mg/day.9 There was a greater reduction in GGT (40.5%) than in ALT (26.0%), as also observed in the current study. The reported effect of UDCA was stronger among CH-C patients with morphological bile duct injury,21 and UDCA administration was accompanied by histological improvement of biliary lesions but not of hepatitis.22 These data suggest that UDCA may act on the biliary system in CH-C through enhanced bile formation and/or modification of bile acid composition. In fact, bile duct injury is characteristic of CH-C, although not specific.23 In this study, the changes in bile acid composition were similar in the 600 and 900 mg/day groups but smaller in the 150 mg/day group, and this may have been associated with the changes in serum biomarkers.
Nakamura et al reported that UDCA had a greater effect in CH-C patients with autoimmune characteristics, that is high immunoglobulin G concentration or positive anti-nuclear or anti-smooth muscle antibodies,24 which suggests involvement of immunomodulatory mechanisms. Indeed, studies in vitro have shown that UDCA suppresses NF-κB-dependent transcription by binding to the glucocorticoid receptor25 and decreases proinflammatory cytokine-induced transcription of phospholipase A2.26 These mechanisms may act cytoprotectively in vivo. The choleretic and cytoprotective mechanisms are not necessarily mutually exclusive.
We examined the effect of UDCA on CH-C in terms of serum biochemical markers in a large-scale, double-blind investigation. We confirmed that a dose of 600 mg/day, that is 10 mg/kg body weight on average, was more effective than 150 mg/day, while adverse effects remained similar and minimal. The doses of 600 and 900 mg/day induced similar decreases in serum ALT and AST. Consequently, it appears that 600 mg/day is the preferred dose of UDCA, assuming that serum transaminase levels reflect the degree of hepatocellular damage.
The decrease in serum GGT differed significantly between the 600 and 900 mg/day groups. In contrast to the decrease in ALT or AST, that of serum GGT may represent improved cholestasis from biliary injury in CH-C. Although the importance of biliary injury in CH-C is unclear, it is possible that a 900 mg/day dose has additional benefits compared to 600 mg/day, as the incidence of adverse effects did not differ between the two doses. It is of interest that the decrease in ALT was significantly different between the two doses in patients with high baseline GGT levels (table 4).
The long-term effects of UDCA therapy in CH-C patients are yet to be elucidated. Changes in liver histology following UDCA administration are not evident from short-term observation. However, it is possible that delayed progression of fibrosis by UDCA can be revealed only by much longer-term observation, because the natural progression of fibrosis in CH-C is usually slow, taking decades to establish cirrhosis.27 28 The effect of UDCA lasted for at least 104 weeks without attenuation (table 3).
In the natural course of CH-C, those patients with normal serum aminotransferase levels show slow fibrosis progression29 and a low incidence of hepatocellular carcinoma.30 31 By multivariate analysis, the risk of hepatocellular carcinoma after interferon treatment without virological response was shown to be 0.26, 0.36 and 0.91 in patients whose ALT levels were normal, moderately elevated (less than twice the upper normal limit) and highly elevated, respectively, compared to untreated patients. It may be that when UDCA lowers serum ALT levels the risk of hepatocellular carcinoma is decreased. A retrospective study showed that hepatocellular carcinoma developed within 5 years from the onset of HCV-related early cirrhosis in 10 of 56 patients (18%) who took UDCA and 18 of 46 patients (39%) who did not.32 Interestingly, ALT levels were similar in the two groups, possibly because UDCA was likely to be prescribed to those patients with high baseline ALT levels. Although these data were obtained from a non-randomised, retrospective study, they suggest that UDCA may provide cancer protective effects independent of decreasing ALT.
In summary, we confirmed, in a large-scale, double-blind study, that a UDCA dose of 600 mg/day was optimal to decrease serum ALT and AST levels in CH-C patients without serious adverse effects. A dose of 900 mg/day resulted in additional decreases in serum GGT levels, and may be preferred in patients with prevailing biliary injuries. The long-term effects of UDCA administration on prognosis, hepatocarcinogenesis in particular, remain to be investigated in future studies.
Competing interests: Declared (the declaration can be viewed on the Gut website at http://www. gutjnl.com/supplemental).
Acknowledgments
Investigators who participated in this study are as follows (listed in alphabetical order): Y Aizawa (Jikei University, Aoto Hospital), K Chayama (Hiroshima University), M Daikoku (National Hospital Organization Nagasaki Medical Center), K Dohmen (Okabe Hospital), K Egashira (Sakura Hospital), K Fujimura (Nara Social Insurance Hospital), K Fujise (Jikei University, Kashiwa Hospital), E Harada (National Hospital Organization Tokyo National Hospital), K Hayashi (University of Miyazaki), N Hayashi (Osaka University), K Hino (Delta Clinic), M Hirano (Tokyo Metropolitan Police Hospital), M Honda (Kanazawa University), N Horiike (Ehime University), H Ikematsu (Haradoi Hospital), Y Imai (Ikeda Municipal Hospital), F Imazeki (Chiba University), D Ito (Osaka Saiseikai Nakatsu Hospital), S Kakumu (Aichi Medical University), Y Katano (Nagoya University), M Kato (National Hospital Organization Osaka National Hospital), M Kawaguchi (Okayama Saiseikai General Hospital), T Kawanishi (Inazumi Park Hospital), S Kawata (Yamagata University), Y Kishimoto (San-in Rosai Hospital), M Kudo (Kinki University), H Kumada (Toranomon Hospital), T Kumada (Oogaki Municipal Hospital), M Matsumura (The Institute for Adult Diseases, Asahi Life Foundation), Y Matsuzaki (University of Tsukuba), H Moriwaki (Gifu University), Y Murawaki (Tottori University), I Nakamura (Jichi Medical University, Omiya Medical Center), K Nakamura (Asahikawa Medical College), R Nakata (Japanese Red Cross Medical Center), S Nishiguchi (Osaka City University), S Onishi (Kochi University), Y Osaki (Osaka Red Cross Hospital), H Saito (Keio University), I Sakaida (Yamaguchi University), S Sakisaka (Fukuoka University), Y Sasaki (Kumamoto University), M Sata (Kurume University), A Sato (St. Marianna University, Yokohama City-Seibu Hospital), M Suzuki (St. Marianna University), K Tachi (Kamiiida Hospital), K Tagawa (Mitsui Memorial Hospital), I Takagi (Jikei University, Third Hospital), A Takaki (Okayama University), Y Takei (Juntendo University), E Tanaka (Shinshu University), J Tazawa (Tsuchiura Kyodo General Hospital), K Togawa (Kawasaki Medical University), E Tomita (Gifu Municipal Hospital), J Toyota (Sapporo Kosei General Hospital), A Ueda (Miyazaki Prefectural Miyazaki Hospital), S Watanabe (Akita University), K Yasuda (Kiyokawa Hospital), T Yamanaka (Itabashi Central Hospital), J Yamao (Nara Medical University), H Yoshida (Yame General Hospital), K Yoshioka (Nagoya University), M Zeniya (Jikei University).
REFERENCES
Footnotes
- Abbreviations:
- ALT
- alanine aminotransferase
- AST
- aspartate aminotransferase
- CH-C
- chronic hepatitis C
- GGT
- gamma-glutamyl transpeptidase
- HCV
- hepatitis C virus
- UDCA
- ursodeoxycholic acid