Article Text

Statistics from Altmetric.com
1. EXECUTIVE SUMMARY
Purpose of report
This document has been commissioned by the British Society of Gastroenterology. It is intended to draw together the evidence needed to fill the void created by the absence of a national framework or guidance for service provision for the management of patients with gastrointestinal and hepatic disorders. It sets out the service, economic and personal burden of such disorders in the UK, describes current service provision, and draws conclusions about the effectiveness of current models, based on available evidence. It does not seek to replicate existing guidance, which has been produced for upper and lower gastrointestinal cancers, hepatobiliary and pancreatic disorders, and many chronic disorders of the gut. It does, however, draw on evidence contained in these documents. It is intended to be of value to patient groups, clinicians, managers, civil servants, and politicians, particularly those responsible for developing or delivering services for patients with gastrointestinal disorders.
Methods used
A systematic review of the literature was undertaken to document the burden of disease and to identify new methods of service delivery in gastroenterology. This systematic review was supplemented by additional papers, identified when the literature on incidence, mortality, morbidity, and costs was assessed.
Routine data sources were interrogated to obtain additional data on burden of disease, the activity of the NHS, and costs, in relation to gastrointestinal disorders.
The views of users of the service were sought, through discussions with the voluntary sector and through a workshop held at the Royal College of Physicians in December 2004.
The views of professionals were obtained by wide dissemination of the document in a draft form, seeking feedback on the content and additional material.
Main findings
The burden of gastrointestinal and liver disease is heavy for patients, the NHS, and the economy, with gastrointestinal disease the third most common cause of death, the leading cause of cancer death, and the most common cause of hospital admission. There have been increases in the incidence of most gastrointestinal diseases which have major implications for future healthcare needs. These diseases include hepatitis C infections, acute and chronic pancreatitis, alcoholic liver disease, gallstone disease, upper gastrointestinal haemorrhage, diverticular disease, Barrett’s oesophagus, and oesophageal and colorectal cancers. Socioeconomic deprivation is linked to a number of gastrointestinal diseases, such as gastric and oesophageal cancers, hepatitis B and C infections, peptic ulcer, upper gastrointestinal haemorrhage, as well as poorer prognosis for colorectal, gastric, and oesophageal cancers.
The burden on patients’ health related quality of life has been found to be substantial for symptoms, activities of daily living, and employment, with conditions with a high level of disruption to sufferers’ lives found to include: gastro-oesophageal reflux disease, dyspepsia, irritable bowel syndrome, anorectal disorders, gastrointestinal cancers, and chronic liver disease. However, impact on patients is neither fully nor accurately reflected in routine mortality and activity statistics and although overall, the burden of gastrointestinal disease on health related quality of life in the general population appears to be high, the burden is neither systematically nor comprehensively described.
An overwhelming finding concerning evidence related to service delivery is the lack of high quality health technology assessment and evaluation. In particular, evidence of cost effectiveness from multicentre studies is lacking, with more research needed to establish a robust evidence base for models of service delivery.
Waiting times form the bulk of patients’ concerns, with great difficulty in meeting government standards for referral and treatment. An extensive and systematic study of the problem of access for the delivery of gastrointestinal services has yet to be carried out and significant publications reporting inequalities in the delivery of gastrointestinal services are lacking. There is also a need to increase awareness and the implementation of initiatives aimed at improving the information flow between patients and practitioners.
Strong evidence exists, however, for a shift in care towards greater patient self management for chronic disease. The development of general practitioners with a special interest in gastroenterology is supported in primary care, but their clinical and cost effectiveness need to be researched. Indeed, emphasis needs to be given to developing interventions to increase preventative activities in primary care, and more research is required to determine their effectiveness and cost effectiveness.
Despite strong support for the development and use of widespread screening programmes for a wide variety of gastrointestinal diseases, there is a lack of evidence about how they are managed, their effectiveness, and their cost effectiveness. In contrast, a strong body of evidence exists on diagnostic services, and the need to develop and implement appropriate training and stringent assessment to ensure patient safety. There is also a substantial amount of work detailing guidelines for care.
In hospital, patients with gastrointestinal disorders should be looked after by those with specialist training, and more diagnostic endoscopies could be undertaken by trained nurses. Importantly, for service reconfiguration, there is currently insufficient evidence to support greater concentration of specialists in tertiary centres. More research is needed especially on the impact on secondary services before further changes are implemented.
Consultant gastroenterologist numbers need to increase to meet a rising burden of gastrointestinal disease. Gastroenterology teams should be led by consultants, but include appropriate non-consultant career grade staff, specialist nurses, and other staff with integrated specialist training, where appropriate.
More research is needed into the delivery and organisation of services for patients with gastrointestinal and liver disorders, in particular to assess the clinical and cost effectiveness of general practitioners with a special interest in gastroenterology and endoscopy; the clinical and cost effectiveness of undertaking endoscopy or minor gastrointestinal surgery in diagnosis and treatment centres; and the reconfiguration of specialist services and the potential impact on secondary and primary care and on patients.
2. INTRODUCTION
2.0 Background including policy drivers
This document has been commissioned by the British Society of Gastroenterology. It is intended to draw together the evidence needed to fill the void created by the absence of a national framework or guidance for service provision for the management of patients with gastrointestinal (GI) and hepatic disorders. It sets out the service, economic and personal burden of such disorders in the UK, describes current service provision, and draws conclusions about the effectiveness of current models, based on the presently available evidence. It does not seek to replicate existing guidance, which has been produced for upper and lower gastrointestinal cancers, hepatobiliary and pancreatic disorders, and many chronic disorders of the gut. It does, however, draw on evidence contained in these documents.
The document takes into account recent strategies for the NHS in the UK, and recommendations for quality and service improvement, new information strategies in England and Wales. In particular, it builds on the recommendations of three reports from Derek Wanless, which have significantly influenced the strategic direction of the NHS.
In July 2000 the Government published the NHS plan which set out the core principles for the NHS and a framework for delivering these principles over the next decade. Following on from this the Chancellor of the Exchequer commissioned the first Wanless Report1 to examine future health trends and resources required over the next two decades. The report welcomed the Government’s intention to extend the National Service Framework (NSF) approach to other disease areas and recommended that the NSFs and their equivalents in the developed administrations are rolled out in a similar way to the diseases already covered. It also recommended that a more effective partnership between health professionals and the public should be facilitated in a number of ways. These include setting standards for the service to help give people a clearer understanding of what the health service will and will not provide for them. Other factors include improving health information, reducing key health risk factors, and reinforcing patient involvement in NHS activities.
These recommendations were repeated and reinforced in a report on the NHS in Wales advised by Sir Derek Wanless.2 The report re-emphasised the need for sustainable change: a shift in delivery from secondary care towards greater care in the community and more self management by patients; and significant investment in improving information and information technology. The report also emphasised the importance of change based on evidence. The third Wanless report3 emphasised the need for improvements in public health and the need for greater investment in prevention and risk reduction.
2.1 Aims and objectives
This review aims at describing how best to provide services for patients with gastrointestinal disorders from a professional and patient perspective, based on available evidence on disease burden and service provision.
Its objectives are to:
-
Review and synthesise published research evidence and routine data concerning the burden of GI diseases on
Patients—their mortality, morbidity, and quality of life
The NHS—its volume and cost
The economy of the UK.
-
Systematically review and synthesise research findings concerning the effectiveness of models of service provision for GI diseases and the cost effectiveness of GI services.
-
Describe the patients perspective on emerging issues of service delivery highlighted through the literature review as undergoing change.
-
Draw conclusions about optimal service provision based on evidence of burden and effectiveness, patients’ view and in the current policy and service context.
The report covers the broad spectrum of GI and liver conditions. It does not examine disorders of nutrition, both malnutrition and obesity, as these have been dealt with in detail elsewhere.4–6
2.2 Overview of methods
Four methods were used in the generation of this document:
-
A systematic review of the literature was undertaken to identify research papers concerning the effectiveness of methods of service delivery in gastroenterology. This systematic review was supplemented by additional papers identified when the publications on incidence, mortality, morbidity, service activity, and costs were assessed. Some further papers were identified and included from consultation feedback.
-
Routine data sources were interrogated to identify additional data on burden of disease and the activity of the NHS in relation to GI disorders.
-
The views of users of the service were sought, through discussions with the voluntary sector and through a workshop held at the Royal College of Physicians in December 2004.
-
The views of professionals were obtained by wide dissemination of the document in a draft form, seeking feedback on the content and additional material. The full draft report was presented at the BSG annual conference in March 2005, alongside a strategy document outlined by the BSG president, based on the review findings. After this meeting, comments were invited, and the online report was made available to the BSG membership through a web link. In addition, patient representative groups and other GI specialist organisations were contacted to gain feedback. Comments were received over a 6 month period after release of the first draft, and these were incorporated where they were supported by evidence from well designed and reported research studies. Table A.13 summarises and appraises these papers.
More detail of the methods used is given in the appropriate sections of the document.
3. BURDEN OF GASTROINTESTINAL AND LIVER DISEASE IN THE UK
3.0 Methods and data limitations
Gastrointestinal and liver disorders affect people of all ages. Some disorders are acute and life threatening, others are more chronic, less dangerous to life, but severely debilitating. Gastrointestinal cancers are common—some are curable, others are almost invariably fatal. Bowel problems cause considerable distress in the elderly. The care and management of such diverse problems requires contributions from a wide variety of professions.
The main methods used in this chapter involved extensive and comprehensive searches of the literature on incidence, prevalence, mortality, and patients’ quality of life for the various gastrointestinal diseases in the UK and, for comparative purposes, for those in other European or Western countries. Part of the literature had been already compiled through reviews undertaken during the course of previous studies of the incidence and mortality of gastrointestinal diseases such as inflammatory bowel disease, liver cirrhosis, and acute pancreatitis.
The literature searches were primarily undertaken on the Medline and Embase databases with “incidence”, “prevalence”, “case fatality”, “mortality”, “quality of life”, “death rate”, “hospital”, “admission”, “gastrointestinal”, “review”, “epidemiology”, “aetiology”, “trend”, “population”, “rate”, “100 000”, “10 000”, “million”, “UK”, “England”, “Scotland”, “Wales”, other countries, and the various gastrointestinal diseases as the main search terms.
The literature reviews were supplemented with extensive searches of routine data sources in the UK to provide additional information on the burden of gastrointestinal disease in the UK. The main routine data sources used in this chapter were: firstly, the cancer surveillance and registry units in England, Wales, Scotland, and northern Ireland for publications and data on the incidence, mortality, survival, and socioeconomic aspects of gastrointestinal cancers. Secondly, data and reports published by the Office of National Statistics (ONS) and its predecessor, the Office of Population Censuses and Surveys (OPCS), were obtained for information on the causes of gastrointestinal and other mortality in England and Wales. Thirdly, information on hepatitis B and C infections was obtained from publications involving communicable disease surveillance units in the UK.
The main categories of gastrointestinal disease with corresponding ICD-9 and ICD-10 codes used are as follows: diseases of the digestive system (ICD-9 = 520–579; ICD-10 = K00-K93), malignant neoplasms of the digestive system (150–159; K15-K26), benign and other neoplasms of the digestive system (210, 211, 230, 235.2–235.5; D00, D01, D12, D13, D37), intestinal infectious diseases (001–009; A00-A09), and viral hepatitis (070; B15-B19).
Some of the main limitations of available data in the UK for investigating the burden of gastrointestinal diseases are: firstly, that incidence and prevalence data are routinely compiled for gastrointestinal cancers and communicable diseases only. Fairly complete incidence data for a few acute gastrointestinal disorders such as acute pancreatitis and acute appendicitis can be traced from hospital admissions, although there have been major concerns about the accuracy of routine hospital data.8,9,10,11 Secondly, different criteria for measuring incidence, case mix variation, and different methods used for age standardising population based incidence and mortality rates can also affect comparability across studies; while case fatality from follow-up studies is affected by factors such as the length of follow-up and the inclusion of deaths after discharge with in-hospital deaths, as well as case mix. Trends in hospital admissions for many gastrointestinal disorders, such as gallstone operations and liver replacements, are also strongly affected by factors such as the availability of hospital facilities, as well as the prevailing clinical practice at the time.
People with other gastrointestinal diseases such as functional disorders are mainly managed in primary care; and so incidence or prevalence data for these diseases can usually only be determined through national primary care surveys, costly databases compiled by pharmaceutical companies, or through intensive local or regional surveys of general practices.
For other gastrointestinal disorders, many people remain undiagnosed. Incidence or prevalence data for some of these diseases, such as gastro-oesophageal reflux disease, irritable bowel syndrome, and dyspepsia, can often be obtained at a regional level only, through diagnostic questionnaires or interviews; while differences in diagnostic criteria often affect comparability across studies.
For some gastrointestinal disorders, it is not possible to distinguish functional disorders from more serious diseases without the use of special investigation or tests. The growing sophistication of gastrointestinal diagnostic methods has probably resulted in increased diagnosis of milder forms of what would have been traditionally regarded as serious digestive diseases, and caution is therefore required when making comparisons longitudinally over time.12 In other words, increases in reported incidence over time may be attributable to improvements in diagnostic methods rather than real increases.
Routine mortality data are usually available for underlying cause of death only, while patterns of certification of the underlying cause of death vary according to the type of disease or condition. People who die soon after a hospital admission for myocardial infarction, stroke or lung cancer are almost always certified with these diseases as their underlying cause of death. In contrast, the certified underlying causes of death for those who die soon after admission for most gastrointestinal disorders are typically much less likely to be these gastrointestinal diseases.13 Therefore, mortality statistics, based on underlying cause of death often underreport true mortality from gastrointestinal diseases.
In summary, for many gastrointestinal diseases, other than cancers, burden of disease data are often patchy, collected at a local or regional level, have variation in case ascertainment and in comparability between studies and longitudinally over time, and can underreport the true burden of disease. Even for cancers that have been allocated specialist surveillance and registration units, despite improvements over time, there are sometimes differences between cancer registries in case ascertainment and completeness of registrations, so that some degree of caution is required when making comparisons longitudinally and between registry regions.
3.1 Spectrum of gastrointestinal disorders
Gastrointestinal disorders cover disease of the alimentary canal (from oesophagus to anus) and its associated organs (liver, gallbladder, and pancreas). They affect a significant proportion of the population. Of the cancers, those of the gastrointestinal tract are among the most common, with colorectal cancer being the second most common cancer in England and Wales as measured by incidence and mortality when both sexes are included.14 It includes very common conditions such as gastro-oesophageal reflux disease, non-ulcer dyspepsia, and functional bowel disease, which although a significant proportion of the population probably self treat at some stage in their life, have a huge impact on primary and secondary care. Other common conditions include inflammatory bowel disease, coeliac and diverticular disease. Alcoholic liver disease remains a significant problem but with increasing obesity and lifestyle trends chronic liver disease due to non-alcoholic fatty liver disease and hepatitis C is being increasingly seen. The wide spectrum of disorders requires a range of treatment involving self care, primary care through to secondary care, and highly specialised tertiary referral centres.
3.2 Incidence of gastrointestinal diseases
Gastrointestinal symptoms and complaints are common among the general population. About one in six admissions to hospital are for a primary diagnosis of gastrointestinal disease, and about one in six of the main surgical procedures in general hospitals are performed on the digestive tract. The following sections outline patterns of incidence and prevalence for some of the main gastrointestinal disorders in anatomical sequence: diseases of the oesophagus, followed by diseases of the stomach and duodenum, the small bowel and colon, the liver, pancreas and gastrointestinal cancers.
Incidence of diseases of the oesophagus
Gastro-oesophageal reflux disease
Gastro-oesophageal reflux disease (GORD or GERD when oesophagus is spelt as esophagus) occurs when reflux of stomach acid into the oesophagus is severe or frequent enough to impact the patient’s life or damage the oesophagus, or both. It is the most common disorder of the gastrointestinal tract, resulting from failure of the gastro-oesophageal sphincter. GORD is a chronic condition that, in most cases, returns shortly after discontinuing treatment.
Risk factors for GORD include hiatus hernia, certain foods, heavy alcohol use, smoking, and pregnancy. There is also a strong genetic component in the incidence of GORD: a first degree relative of a patient is four times more likely to be afflicted, while a recent study estimated that 50% of the risk of GORD is genetic.15 Other possible risk factors include concomitant drugs for treatment of hypertension, angina, and arthritis,16 and obesity.17
The risk of GORD increases with age, rising sharply above the age of 40. More than 50% of those afflicted are between the ages of 45 and 64. Incidence varies geographically, it is slightly higher in women than in men, and it is higher among white people than among Asian and Afro-Caribbean ethnic groups.18,19
In Western countries, 10–40% of the adult population experience heartburn, which is the main symptom of GORD, although estimates vary according to the diagnostic criteria used.18,20,21 In the UK, a recent community based study reported a prevalence of 28.7% for GORD symptoms.22 Subjects with chronic GORD are at risk of developing Barrett’s oesophagus (see below). About 10–15% of subjects who undergo endoscopy for GORD evaluation are found to have Barrett’s oesophagus,16,23 while other complications of GORD include erosive oesophagitis, ulceration, strictures, and gastrointestinal bleeding.24
Barrett’s oesophagus
Severe, longstanding gastro-oesophageal reflux disease can damage the oesophagus and lead to a condition known as Barrett’s oesophagus. This refers to an abnormal change or metaplasia in the cells of the lower end of the oesophagus. Barrett’s oesophagus, or columnar-lined oesophagus (CLO), occurs in about one in 400 of the general population, or about 15% of patients with reflux oesophagitis. It is a rare diagnosis in people aged under 40 years, but its prevalence increases sharply with age and with obesity. It is much more common in white people than in Asian and Afro-Caribbean ethnic groups,18 among men than women, and among people in higher socioeconomic groups.25
Barrett’s oesophagus is a major risk factor,16,23,24 and the only known precursor,26–28 for oesophageal adenocarcinoma, although the degree of risk is not very clearly defined as many people with Barrett’s oesophagus remain undiagnosed. The diagnosed incidence of Barrett’s oesophagus has been increasing sharply over time in the UK,29,30 indicating real increases in its prevalence.
Oesophagitis
Oesophagitis refers to the inflammation of the lower end of the oesophageal lining, arising mainly through the chronic reflux of stomach acid and digestive enzymes into the oesophagus. When the inflammation is severe, oesophageal ulcers may develop. Around 50% of people with GORD also have oesophagitis.31 Other, less common causes of oesophagitis include hiatus hernia, certain fungal infections such as monila and candida, viruses, irradiation, and caustic substances such as lye. The prevalence of oesophagitis increases with age and obesity, and it is also more common in men than in women, and among white people than in Asian and black ethnic groups.32,33
Oesophagitis is present in about 20% of patients at endoscopy,34 although case series from endoscopy units suggest that the diagnosis of oesophagitis is increasing over time. For example, one recent British study reported a diagnostic rate of 32%.35 It is likely that this reflects a true increase in the prevalence of oesophagitis, but the magnitude of the increase may not be entirely accurate owing to effective treatments for the condition, such as the advent of proton pump inhibitors.21
Dyspepsia
Functional gastrointestinal disorders are defined by symptoms in the absence of any structural abnormalities, and affect all areas of the GI tract, ranging from globus (feeling of a lump in the throat), non-cardiac chest pain, functional dyspepsia in the upper GI tract, and irritable bowel syndrome (IBS) in the lower GI tract. Functional gastrointestinal disorders are characterised by poorly understood abnormalities of gut motility and sensory perception. These and rare motility disorders occur owing to dysfunctional interactions between the brain/central nervous system and the gut/enteric nervous system. Biological triggers underlying functional gastrointestinal disorders are being identified, leading to research aimed at providing effective treatments.
Dyspepsia describes pain or discomfort in the upper abdomen, rather than a defined condition, and it is a chronic, relapsing, and remitting symptom. Causes of dyspepsia include peptic ulcers, acid reflux disease, oesophagitis, anti-inflammatory drugs, gastritis and duodenitis, hiatus hernia, gastric motility disorder, oesophageal or gastric cancers, although in many cases there is no underlying disease.
Dyspepsia has been defined in different ways by a number of expert groups. For example, the 1988 Working Party classification states that symptoms need to be referable to the upper GI tract, and need to be present for the past four weeks. The less inclusive Rome II criteria later stated that patients need to have predominant pain or discomfort centred in the upper abdomen for at least 12 weeks of the past year, and excluded patients with heartburn or acid reflux as their only symptoms. More recently, the BSG have defined dyspepsia as any group of symptoms that alert doctors to consider diseases of the upper GI tract.
Dyspepsia symptoms typically affect between 20 and 40% of the UK population, depending on the diagnostic criteria used.21 Most recent British studies have used the BSG definition and have typically reported dyspepsia prevalence rates of about 40% (table 3.2.1),36–39 although lower rates of 26%,40 29%,41 and 12%,42 have also been reported. Prevalence rates in the UK have often been higher than those reported for populations in other Western countries (table 3.2.1).
Table 3.2.1 Prevalence rates (% of population) of dyspepsia, as reported from various regional studies in the UK and in other Western countries
Dyspepsia also accounts for between 1.2 and 4% of all consultations in primary care in the UK.34,43 Half of these consultations are for functional dyspepsia. Non-cardiac chest pain may be of gastrointestinal origin but sufferers often persist in the belief that they have heart disease, resulting in severe morbidity. Fifty per cent of patients consulting their GP for chest pain,44 and a similar proportion seen in rapid access chest pain clinics,45 have no cardiac cause of their symptoms. Although mortality in people with functional gastrointestinal disorders is not raised compared with the general population, these disorders have a significant impact on quality of life. For example, two studies reported that 75% of people with non-cardiac chest pain suffered persistent symptoms and impaired quality of life over periods of 10 years or more; 30–50% never returned to work and were unable to carry out household tasks.44,46
Peptic ulcers have been thought to account for a quarter of all cases of dyspepsia.47 Several British studies from the 1940s to the 1980s reported that 18%,48 26%,41 and 31% 39 of people referred with dyspepsia were found to have peptic ulcers, although more recently this percentage has fallen to around 10–15%.34,39,49,50
Incidence of diseases of the stomach and duodenum
Peptic ulcer
Peptic ulcer is the collective term that includes ulcers of the stomach and the duodenum. About 90–95% of duodenal ulcers and 70–80% of gastric ulcers are caused by the Helicobacter pylori infection. Other risk factors include non-steroidal anti-inflammatory drugs (NSAIDs) and corticosteroids, increased gastric acid secretion, blood group “O”, smoking, and heavy alcohol use.
Duodenal and gastric ulcer differ in their incidence by age and sex. The incidence of duodenal ulcer peaks at age 45–64 years, and is twice as common in men than in women, whereas gastric ulcer is more common in the elderly and more equally found in men and women.
The incidence of peptic ulcer in the UK increased during the first half of the 20th century. Since the 1950s, however, hospital admission rates for peptic ulcer have fallen among most age groups.66–70 Since the early 1980s, this is largely because of a reduction in recurrent ulcer disease consequent upon the identification and eradication of Helicobacter pylori infection in patients presenting with peptic ulcer. For example, admission rates for duodenal ulcer in Scotland fell by 38% from 157 to 98 per 100 000 population between 1975 and 1990,69 and the prevalence of peptic ulcer in primary care in England and Wales fell by 50% from 1994 to 1998.71 Hospital admissions for perforated peptic ulcer have also fallen over time in the UK; for example, by 26% in Oxford between 1976 and 1982,72 and by 44% in Scotland for perforated duodenal ulcer between 1975 and 1990.69
However, in contrast with this downward trend, hospital admissions for perforated peptic ulcer increased among elderly women in the UK during the 1970s and 1980s,69,73,74 and perforated duodenal but not gastric ulcer, and haemorrhagic peptic ulcers, increased among elderly people in England during the 1990s.75 These increases have been linked to the use of NSAIDs, which have been shown to cause both gastric and duodenal ulceration, including ulcer perforation and haemorrhage.76,77 Patients taking NSAIDs have been reported to be at 4.7 times greater risk of haemorrhagic peptic ulcer, with an increasing risk with age up to 13.2 in people aged over 60.21 Recent small reductions in the incidence of peptic ulcer among elderly women since the mid-1980s, indicates increased awareness of the side effects of NSAIDs, and more selective prescribing of these drugs.12,70
Helicobacter pylori infection
Helicobacter pylori is a bacterial infection that was discovered in 1982 and is the causal agent in 90–95% of duodenal ulcers and 70–80% of gastric ulcers. It is also linked to other gastrointestinal diseases such as gastritis and dyspepsia,34,49 and it is estimated to be the cause of 73% of all gastric cancers.78,79Helicobacter pylori has been listed as a grade I carcinogen because gastric cancer can occur after Helicobacter pylori gastritis leads to atrophy and metaplasia.80
Risk of infection is strongly linked to social deprivation in childhood, and it is much higher in unsanitary or overcrowded living conditions with no fixed hot water supply.80 It is thought that the crowded living conditions of the expanding cities at the beginning of the industrial revolution led to a decline in hygiene and the spread of the infection early in life.12,81
The prevalence of the Helicobacter pylori infection in the UK has declined in recent decades, as the infection is progressively eradicated from patients presenting with peptic ulcer and also because of a declining incidence as conditions improved over time. Successive birth cohorts have had a lower risk of childhood infection: the prevalence of Helicobacter pylori in 20–30 year olds is 10–20%, rising with age to 50–60% in 70 year olds.
Up to half of the world’s population is infected with Helicobacter pylori.80 Prevalence varies between about 80% for adults in developing countries, Japan, and South America, around 40% in the UK, and 20% in Scandinavia. Local differences in prevalence exist where there has been substantial immigration from countries with a higher prevalence of infection.
About 15% of people infected with Helicobacter pylori will develop peptic ulcer or gastric cancer as a long term consequence of the infection. Infection in infancy is thought to lead to pangastritis, which predisposes to gastric ulcer and gastric cancer, while infection in later childhood may lead to antral gastritis, which predisposes to duodenal ulcers and duodenitis.82 It has been estimated that one in 35 men and one in 60 women in England and Wales die from a Helicobacter pylori related disease.78 Eradication therapy for Helicobacter pylori infection has been shown to be effective for pylori peptic ulcer disease.49
Gastrointestinal haemorrhage
Gastrointestinal haemorrhage refers to bleeding from the bowel wall or mucosa anywhere along the GI tract. Presentation depends on the location and rate of haemorrhaging and includes melaena from rapid bleeding high in the gastrointestinal tract, iron deficiency anaemia from chronic slow blood loss, or red blood from the colon or ileum.
Acute upper gastrointestinal bleeding is the commonest emergency managed by gastroenterologists. About half of all upper gastrointestinal haemorrhages are caused by peptic ulcers and NSAIDs, while other causes include oesophageal or gastric varices, gastric erosions, Mallory-Weiss tear in the lining of the oesophagus, angiodysplasia, and upper gastrointestinal malignancies. For example, a review of nine European studies from 1973 to 1995 reported that the main causes of haemorrhage were duodenal ulcer (24% of all cases), gastric ulcer (13%), varices (9%), gastritis/erosions (9%), oesophagitis (8%), malignancies (5%), and no diagnosis (14%).83
Lower gastrointestinal haemorrhage accounts for about 20% of all acute gastrointestinal haemorrhages. The most common causes are diverticular disease, inflammatory bowel disease, colonic polyps, ischaemic or infective colitis, gastroenteritis, haemorrhoids, angiodysplasia, and colorectal neoplasms. Most lower gastrointestinal haemorrhages occur in elderly people, and most of these bleeds settle spontaneously and do not require emergency surgery. It is estimated that 20–30% of all gastrointestinal haemorrhages are related to the use of non-steroidal anti-inflammatory drugs.
The incidence of upper gastrointestinal haemorrhage increases very sharply with age, it is higher in men than in women, and it tends to be highest in areas with high incidence of peptic ulcer—for example, in Scotland and the north of England rather than in southern regions. High hospital admissions rates of upper gastrointestinal haemorrhage have been reported in the west of Scotland (172 per 100 000 in 1992–93),92 Aberdeen (117 in 1991–93),90 and the north east of Scotland (116 in 1967–6886; table 3.2.2).
Table 3.2.2 Hospital admission rates (per 100 000 adult population) for upper gastrointestinal haemorrhage as reported from various regional studies in the UK and in other countries
A study of four health regions in the south of England and the Midlands reported an overall hospital admission rate of 103 per 100 000; which varied between 91 for north west Thames and 107 for Trent.91 However, lower hospitalised incidence rates of 45–70 per 100 000 were reported from earlier studies particularly in relatively affluent studies such as Bath and Oxford from the 1950s to the 1980s.84,85,88,89 With an ageing UK population, incidence is likely to continue to rise.91
Incidence rates of upper gastrointestinal haemorrhage in the UK are often higher than those reported in other recent studies in Europe and elsewhere. These include studies in Central Finland,99 the Netherlands,83 Saudi Arabia,98 Estonia,99 and a multicentre study in Spain and Italy. None the less, high incidence rates of 160 per 100 000 have been reported from studies in Crete in the late 1990s,100 and Spain in the 1980s.95
Incidence of diseases of the small bowel and colon
Inflammatory bowel disease
Ulcerative colitis and Crohn’s disease are the two main idiopathic types of inflammatory bowel disease. Ulcerative colitis, otherwise known as idiopathic proctocolitis, causes inflammation and ulcers in the colon. Crohn’s disease differs from ulcerative colitis because it can occur anywhere along the GI tract and causes inflammation deeper within the intestinal wall. Inflammatory bowel disease usually affects younger people and has a chronic relapsing course that impacts on educational, social, professional, and family life. Along with gastrointestinal cancers and liver disease, inflammatory bowel disease is one of the three most important areas for British gastroenterologists.
A total of about 150 000 people have inflammatory bowel disease in the UK, and a total of approximately 2.2 million across Europe.102 Although there is substantial regional variation (table 3.2.3), the prevalence of Crohn’s disease in the UK is currently about 55–140 per 100 000 population, and that of ulcerative colitis is about 160–240 per 100 000, with a combined incidence of about 13 300 new cases diagnosed each year.103
Table 3.2.3 Incidence and prevalence rates (per 100 000 population) for Crohn’s disease and for ulcerative colitis, as reported from various regional studies in the UK
The causes of ulcerative colitis and Crohn’s disease are not fully known. Although they are thought to be autoimmune diseases, it is not certain whether autoimmune abnormalities are a cause or result of the diseases. Suggested risk factors include appendectomy, diet, smoking, perinatal and childhood infections, and oral contraceptives,102 while a possible link with measles vaccination has been disputed.104,105 Inflammatory bowel disease predisposes strongly to cancer of the colon,106–110 to venous thromboembolism,111–113 and osteoporosis,114–116 and it is also associated with coeliac disease,117,118 and primary sclerosing cholangitis.119,120
There is a peak in incidence of inflammatory bowel disease between the ages of 10 and 19 years, and a smaller peak beyond 50 years of age. Women may be at a slightly increased risk of Crohn’s disease than men, whereas the risk for ulcerative colitis is the same for men and women.
Studies of Crohn’s disease in the UK, and in Europe, have typically reported large increases in incidence over the past 50 years, while others have reported incidence rates that have stabilised after earlier increases (table 3.2.3). There was a sharp increase in the incidence of Crohn’s disease in Cardiff from the early 1960s to the early 1980s, before levelling off in the late 1980s,121 and subsequently declining during 1991–95.122 Other sharp increases in incidence of Crohn’s disease up to the 1980s have been reported for the north east of Scotland,123 Derby,124 Blackpool,125 and among Europeans in Leicestershire.126
Incidence rates for ulcerative colitis have been more stable over time than those for Crohn’s disease,127 although a few recent European studies have reported increasing,128,129 or decreasing rates.130 Several regional British studies have reported incidence rates of about six or 7 per 100 000 (table 3.2.3),131–133 although substantially higher rates of 11 to 15 have been reported for northern regions such as north Tees and the north east of Scotland.134–136
Although the incidence of inflammatory bowel disease may have shown a tendency to plateau in recent years, large increases in the incidence of paediatric Crohn’s disease have continued to be reported in the UK. For example, in Scotland there was a threefold increase in paediatric incidence from 1968 to 1983,142 a further 50% increase from 1981–83 to 1990–92,143 and a 100% increase in north east Scotland from 1980–89 to 1990–99.144 In south Glamorgan there was a 140% increase in the incidence of paediatric disease from 1983–88 to 1989–93,145 although it is now thought to have reached a plateau.146 A recent comparison of two national British birth cohorts indicates that the prevalence of Crohn’s disease has increased in younger people, although the prevalence of ulcerative colitis has remained stable.147
A comparison of incidence rates for Crohn’s disease and ulcerative colitis in the UK, with those reported for various other European countries in 1991–93, is shown in figs 3.2.1 and 3.2.2.148 There is substantial international variation in the incidence of both types of inflammatory bowel disease. For Crohn’s disease, incidence tends to be much higher in northern European countries, particularly in Scandinavia and the Netherlands.

The digestive system. Source: Department of Gastroenterology, University of Miami, 2005.7
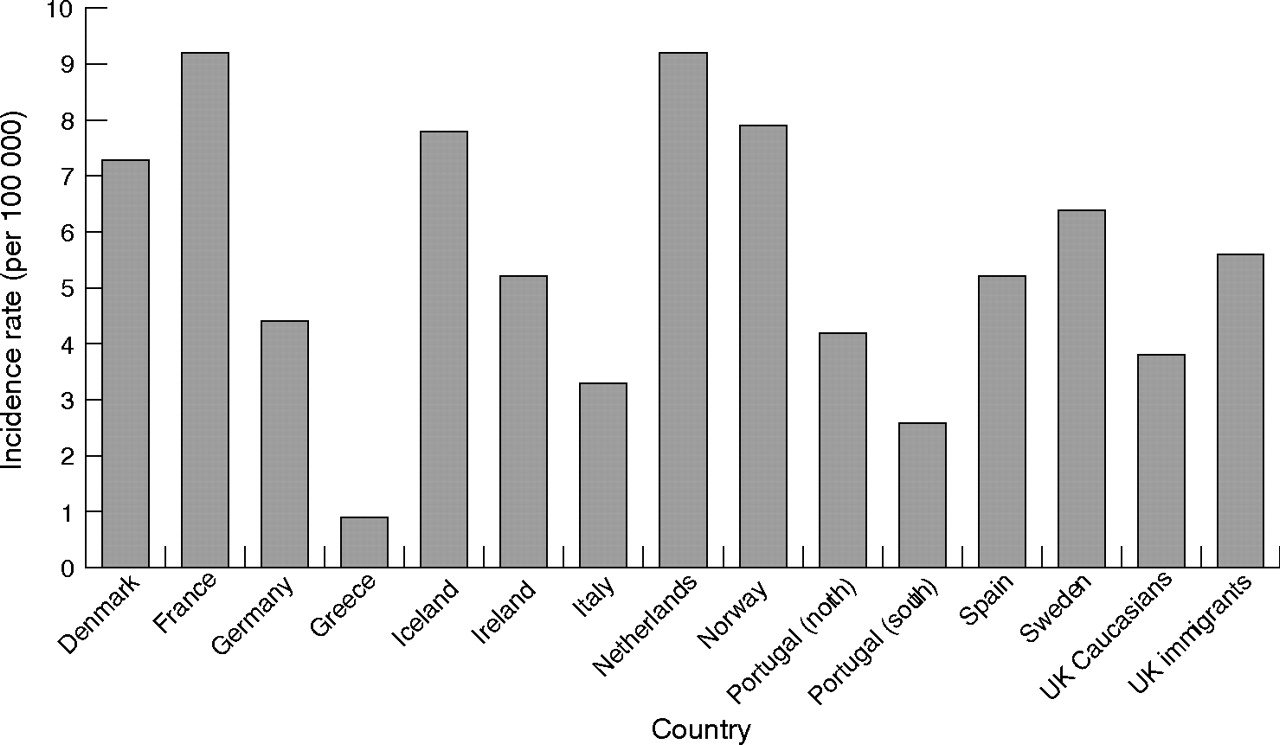
Incidence rate (per 100 000 population) for Crohn’s disease in the UK and in other European countries. Source: Shivananda et al, 1996.148

Incidence rate (per 100 000 population) for ulcerative colitis in the UK and in other European countries. Source: Shivananda et al, 1996.148
The incidence of ulcerative colitis among the UK white population (10.0 per 100 000) is similar to the average of all European countries reported here (9.4), but UK immigrants have a substantially higher rate (figs 3.2.1 and 3.2.2). The incidence of Crohn’s disease in the UK white population (3.8) is lower than the European average (5.5), but UK immigrants have similar incidence (5.6).
Irritable bowel syndrome
Irritable bowel syndrome (IBS) refers to longstanding symptoms of abdominal pain, bloating, flatulence, diarrhoea, and/or constipation. It is the most common functional gastrointestinal disorder seen by GPs, and it is the most common disease diagnosed by gastroenterologists. Although not life threatening, IBS may severely impair quality of life, and it usually persists for several years. Like dyspepsia, IBS has been defined in a number of different ways according to different diagnostic criteria, which affects prevalence estimates.
IBS typically affects 10 to 25% of the general UK population. About half of people with IBS consult their GP, and of these about 20% are referred to a consultant.149 Consultation behaviour is often influenced by life events or psychological factors, as well as severity of symptoms. IBS constitutes about 20 to 50% of the outpatient gastroenterology workload.150–152
IBS can occur at any age, although it most commonly starts in late teenage years or early adulthood, and it is up to three times more common in women than in men. Although there is no consistent effect of age and ethnicity on symptoms,149 they vary according to which parts of the gut are affected.
Recent community based studies in the UK have reported an IBS prevalence of 10.5% in Birmingham,158 16.7% in Teeside,154 9.5% and 2.5% in Bristol,155,156 and 22% in Hampshire.43 In each of these studies, the prevalence in women was two to four times higher than in men. Prevalence also appears to be increasing in the UK. For example, a comparison of two British national birth cohorts revealed a prevalence rate that had risen from 2.9% in 1988 to 8.3% in 2000 among people aged 30 years.147
The prevalence of IBS ranges in all countries of the world from about 3% to 25%. Although differing diagnostic criteria affect comparability across studies, reported prevalence rates in the UK appear to be comparable with, or perhaps slightly higher than those reported in most other Western countries (table 3.2.4).
Table 3.2.4 Prevalence rates (expressed as percentages) of irritable bowel syndrome (IBS) reported from various studies in the UK and in other Western countries
Coeliac disease
Coeliac disease is an inflammatory condition of the small intestine resulting from sensitivity to gluten, a protein in wheat flour, and similar proteins in barley and rye. It develops in genetically predisposed people but can be diagnosed at any age from early childhood to old age. It appears that a “trigger factor” may be required to initiate that response. The trigger might be a viral infection but is usually not known. Removal of wheat gluten (as well as barley and rye) from the diet permits the intestinal mucosa to recover.
Coeliac disease is highly prevalent throughout the world, particularly in countries where wheat forms part of the staple diet, and it is one of the most important conditions managed by gastroenterologists. It is more prevalent in the families of those who are affected: it is estimated that as many as 10% of first degree relatives of patients are also affected.173 Previous underdiagnosis of coeliac disease in primary care reflects an evolving awareness of the diversity in the presentation of coeliac disease.174 Coeliac disease is often associated with other diseases such as ulcerative colitis, biliary cirrhosis, primary sclerosing cholangitis, osteoporosis, malignant lymphomas, and thyroid disorders,175–183 as well as being linked to increased risks of gastrointestinal cancer.182,184,185
The prevalence of coeliac disease is thought to be about 1% in the UK,186 which appears to be comparable with other countries, globally (table 3.2.5). The prevalence of coeliac disease has increased sharply in the UK in the last couple of decades; largely because of improved diagnosis rates as a result of the introduction of screening tools which can be used in primary care. In the diagnosis of coeliac disease, IgA antibodies to tissue transglutaminase and endomysium show good sensitivity and specificity for coeliac disease; however, it is recommended that the diagnosis is confirmed by small bowel biopsy. Cases of coeliac disease have been described in patients with normal biopsy and positive serology and visa versa. In patients with coeliac disease and IgA deficiency the serology will be negative, in such patients IgG transglutaminase and endomysial antibody should be determined.
Table 3.2.5 Prevalence rates of coeliac disease as reported from various international studies
Diverticular disease
Diverticular of the intestine is a major cause of mortality and morbidity in the UK, mainly among elderly people. It refers to diverticula, or small sacs or pouches that form in the wall of the colon. The most common complication is acute diverticulitis, which occurs when the diverticular become infected, and is sometimes associated with perforation, intestinal obstruction, fistula or abscess formation. Diverticular disease is very common in elderly people, but it is rare in younger age groups and in developing countries. It is thought to be caused mainly by longstanding constipation.198
Risk factors for diverticular disease include low fibre diets and low levels of physical activity, while vegetarians have a lower incidence of diverticular disease.199,200 Increased risks of perforated diverticula have been identified for NSAIDs,201–204 corticosteroids,205 and opiate analgesics,206 whereas calcium antagonists are thought to have a protective effect.203
Diverticular disease is much more common in the west than in less developed countries.203 For example, a study from the 1960s reported a hospital admission rate of 12.9 per 100 000 in Scotland that was over 60 times higher than those in Fiji, Nigeria, and Singapore.207 Westerners residing in those countries were also substantially more affected than the native populations. In Singapore, for instance, the admission rate among Europeans (5.4 per 100 000) was over 40 times that in the indigenous population.207
In the UK, diverticular disease is much more common among white people than among Asian ethnic groups,208 while incidence increases sharply with age. About 5% of people are affected when in their 40s, and about 50% of people when aged over 80.209 Diverticular disease is more common in men than in women among younger age groups, but it is more common in women among older age groups.203
Because uncomplicated disease is not associated with any particular symptoms, it is often not discovered until postmortem examination, while few studies have examined the progression from uncomplicated to complicated diverticular disease. Lower gastrointestinal haemorrhaging, which occurs in about 15–20% of cases, and infection resulting in peritonitis or abscesses are the most common complications, and are the causes of most admissions to hospital.210 For details of mortality associated with complicated and uncomplicated diverticular disease, see section 3.3.
With an ageing UK population, the incidence of diverticular disease is increasing.211,212 For example, hospital admissions for diverticular disease increased by 16% in men from 20 to 23 per 100 000, and by 12% in women from 29 to 32 per 100 000 in England during the 1990s,212 while emergency surgical admissions for diverticular disease increased significantly in the south west of England from 1974 to 1998.213
Incidence of diseases of the liver
Chronic liver disease and cirrhosis
Chronic liver disease and cirrhosis, traditionally referred to as liver cirrhosis, encompasses a wide range of acute and chronic liver conditions that are caused by a number of different agents. These conditions may lead to cirrhosis, resulting in scarring, injury, and dysfunction of the liver. They include heavy alcohol consumption, hepatitis B or C viral infections, prolonged exposure to certain drugs and toxins, inherited diseases such as haemochromatosis and Wilson’s disease, autoimmune liver disease, and chronic liver diseases such as alcoholic fatty liver disease, primary biliary cirrhosis and other chronic diseases of the bile ducts. Around 25% of liver disease is alcohol related, and a similar amount is caused by hepatitis C.214
Alcoholic liver disease
Alcoholic liver disease refers to a handful of liver diseases that are attributed to the effects of alcohol. These include alcoholic cirrhosis, alcoholic fatty liver disease, alcoholic hepatitis, and alcoholic hepatic failure. Because of diagnostic difficulties, there is negligible reporting of population based incidence rates for the different aetiologies; while in most cases routine hospital data fail to distinguish between them. For example, in Scotland in 1999–2000, 71% of hospital discharges for alcoholic liver disease were diagnosed as “unspecified alcoholic liver disease”.215 Since only 15–30% of heavy consumers of alcohol develop advanced alcoholic liver disease,216 genetic and other environmental factors also have an important role.
Earlier, regional British studies reported incidence rates for alcoholic liver disease of 6.5, 14.6, and 2.8 per 100 000 population in respectively, west Birmingham in 1971–76,217 Tayside in 1975–79, and the Scottish Islands of Lewis and Harris in 1977–82.218 The study of west Birmingham also reported an increase in alcoholic liver disease from 2.3 to 9.5 per 100 000 from 1959–61 to 1974–76.217
More recent figures show a 160% rise in hospital admissions for alcoholic liver disease in Scotland between 1996 and 2000,219 while an earlier Scottish study also reported a 160% increase in admissions for liver cirrhosis from 1983 to 1995.220 The large increase in alcoholic liver disease in the UK in recent years has become a major public health concern and has led to the publication of a national alcohol reduction strategy.221
Incidence rates for alcoholic liver disease in the UK are still relatively low compared with those in many other Western countries. For example, a rate of 32 per 100 000 was recently reported for Los Angeles, which varied between 8 per 100 000 for Asian ethnic groups and 61 for Hispanics,216 while the incidence rate in Stockholm County increased from 8 to 24 per 100 000 during the 1970s before falling to 12 per 100 000 by the late 1980s.222
Non-alcoholic fatty liver disease
Non-alcoholic fatty liver disease (NAFLD), largely unheard of before the 1980s, is another liver disease on the increase, coinciding with the epidemic of obesity in the UK and in other Western countries. NAFLD is the term used to describe a number of liver conditions, including simple steatosis (fat accumulation in liver cells), steatosis with non-specific inflammation, steatohepatitis (fat accumulation and liver cell injury), and hepatocellular cancer.223 It has also been suggested that cryptogenic cirrhosis may often actually be “burned out” non-alcoholic steatohepatitis.224
NAFLD is commonly seen in conjunction with type 2 diabetes, obesity, hypertension, and dyslipidaemia, and is regarded as the liver’s response to the metabolic syndrome. Although not the only risk factor, obesity is the most prevalent risk factor for NAFLD and is present in 65–90% of cases. Additional risk factors include advanced age and type 2 diabetes, while men and women are equally affected. Although many people with NAFLD remain undiagnosed, it is thought to affect about 20% of the general population in the UK,225 while the obesity epidemic is expected to result in increases in the prevalence of NAFLD in the future.
Non-alcoholic steatohepatitis
Non-alcoholic steatohepatitis (NASH) is a major cause of non-alcoholic liver disease which closely resembles alcoholic liver disease, but occurs in people who consume little or no alcohol. As with alcoholic liver disease, an excess of fat is deposited in the liver, which leads to NASH, inflammation, and scarring, and can progress to cirrhosis. NASH is thought to progress to advanced liver disease in about 15–20% of cases. Most cases are asymptomatic and are diagnosed when abnormal liver blood results are discovered during routine investigations.226
Until relatively recently NASH was thought to be confined largely to middle aged obese women with diabetes. However, it has become increasingly recognised that NASH also occurs in people who are neither obese nor diabetic, and that it may be one of the most common liver diseases in the Western world.226 Unfortunately, figures on the incidence or prevalence of NASH in the UK are conspicuous by their absence.
Hepatitis C
The hepatitis C infection is caused by a virus, which is mainly passed through blood and blood products. Most new cases in western Europe are related to intravenous drug abuse, through using infected needles, and to the increased prevalence of hepatitis C infection in Eastern European immigrants.227 Other less common routes of infection in the UK include unprotected sex, through contaminated skin piercing and tattooing equipment, or from mother to baby.228 As symptoms from acute hepatitis C infection are uncommon, infection is often discovered by chance on routine screening or on testing after the patient’s liver function tests have been found to be abnormal.
An estimated 0.5% of the general UK population, or about 300 000 people, are infected with hepatitis C. Since about one fifth of those infected appear to get rid of the virus naturally without treatment,228 the estimated prevalence of hepatitis C infection is about 0.4% or 240 000 people, which is about four times higher than the total number of 60 294 reported hepatitis C diagnoses in the UK up to the end of 2003.229
Prevalence rates, based on the total number of reported laboratory diagnoses in the UK, at the end of 2003 were 0.08% for the general population in England, 0.36% in Scotland, 0.11% in Wales, and 0.04% in Northern Ireland.229 These are typically lower than prevalence rates reported for other European countries (fig 3.2.3). There are an estimated five million hepatitis C carriers in western Europe,227 and 170 million in the world.230 Prevalence rates in the UK, and in Europe (1.0% of the population) are lower than in other parts of the world, such as Africa (5.3%), the Eastern Mediterranean (4.6%), and South East Asia (2.2%).230
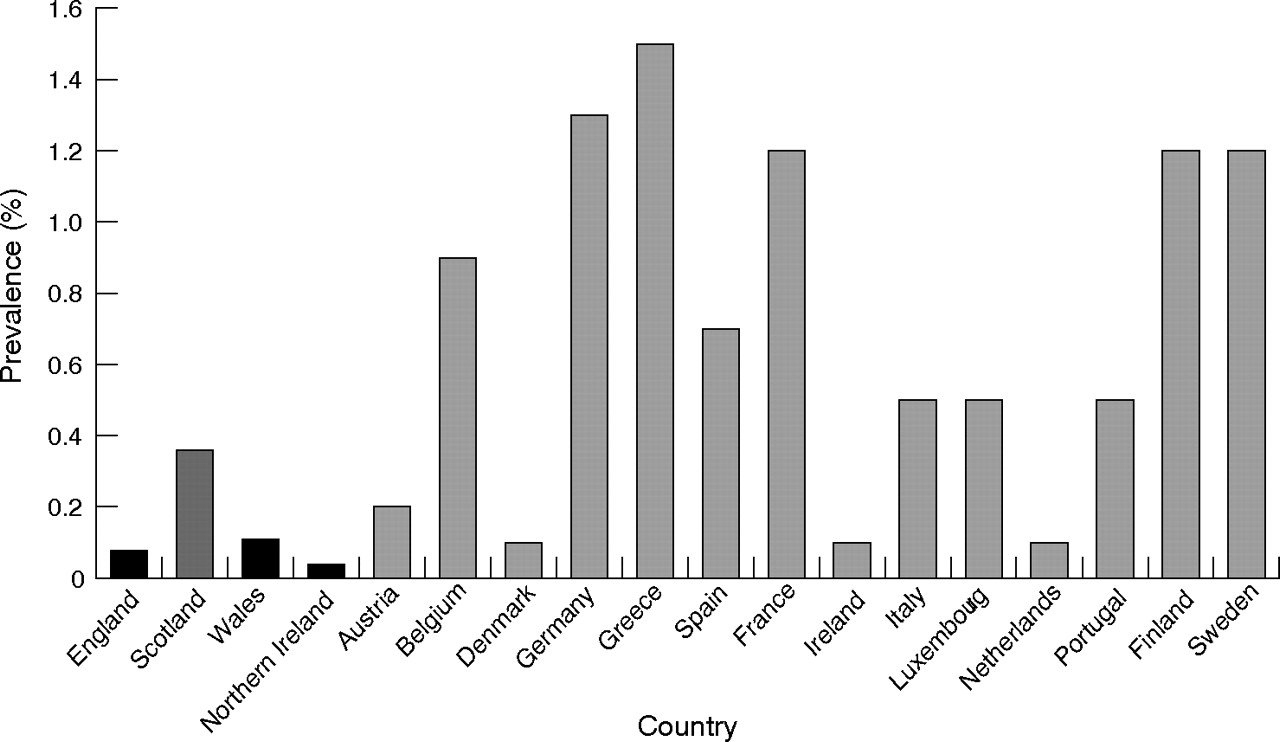
Prevalence rates (% of population) for reported hepatitis C infections in England, Scotland, Wales, Northern Ireland, and other European countries. Notes: Rates in England, Scotland, Wales, and Northern Ireland are based on reported laboratory diagnoses.229 The data source for reported rates in the other European countries is Burroughs and McNamara.227
Greatly increased risks of hepatitis C infection are found among high risk subgroups of the UK population, such as injecting drug users. In Scotland, for example, reported prevalence rates for hepatitis C antibodies among injecting drug users varied between 23% in the Forth Valley and 62% in Greater Glasgow in 1999–2000,229 while a prevalence rate of 44% was reported for injecting drug users in London in 2001.231 Another document reported the highest prevalence in 2001–02 of about 45–50% in London and the north west of England, the lowest prevalence of about 15% in the north east, and a prevalence of 20–35% in other English regions.232
Reported incidence rates for hepatitis C increased alarmingly in the UK during the 1990s, particularly in Scotland (fig 3.2.4A). Based on reported diagnoses, the incidence is currently about 40 per 100 000 in Scotland, 10–15 per 100 000 in England, Wales, and in the UK overall, and around 5 per 100 000 in Northern Ireland.229 In Tayside, prevalence increased from 0.01% to 1.03% of the population from 1988 to 1998.233 The rise of hepatitis C infections has led to the recent publication of national English strategy and action plan documents.228,232

Trends in incidence rates (per 100 000 population) for reported hepatitis C and B infections in the UK, England, Scotland, Wales, and Northern Ireland, 1990–2003. (A) Hepatitis C infection; (B) hepatitis B infection. Notes: These incidence rates are based on reported laboratory diagnoses.229
About 40% of people with an acute hepatitis C infection have lifelong chronic infection, which often causes liver cirrhosis or cancer many years after the initial infection. Infected people who consume alcohol have accelerated liver damage, and increased incidence of liver cirrhosis and hepatocellular cancer.234,235 Hepatitis C infection invariably causes chronic illness, resulting in a major financial burden on healthcare resources. In western Europe, hepatitis C accounts for 70% of all cases of chronic hepatitis, 40% of all liver cirrhosis, and 60% of all hepatocellular cancer.227 Because of the increasing incidence of hepatitis C, it is estimated that the future burden of hepatitis C health care related to new incidence of cirrhosis will increase by 60% by 2008, and that there will be a fivefold increased need for liver transplantation.214
Hepatitis B
Hepatitis B is also caused by a virus; which, in Europe and North America, is mainly passed from person to person by unprotected sex. In the rest of the world it is mainly passed from infected mothers to their children or from child to child.226 Both hepatitis B and chronic hepatitis C are premalignant diseases leading to hepatocellular cancer. However, unlike hepatitis C, vaccination for hepatitis B has proved to be successful in reducing infection rates.227
The prevalence of hepatitis B in the UK is thought to be 0.1% of the general population or approximately 60 000 people,226 which compares with a total of about 13 000 reported diagnoses up to the end of 2003.229 In districts of the UK where there are high levels of immigration, prevalence can be much higher; as high as 2% of the population. In Europe, an estimated one million people are infected each year, although the infection is more common in South East Asia, the Middle and Far East, Africa, and southern Europe.
Compared with hepatitis C, there is a less discernible trend in the incidence of reported hepatitis B diagnoses in the UK in recent years (fig 3.2.4B), although there appears to have been quite sharp increases in Scotland during the late 1990s and in Northern Ireland during the past few years. Reported incidence rates for hepatitis B are about one fifth of those for hepatitis C. Recent World Health Organisation figures also indicate that the incidence and prevalence of hepatitis B in the UK is relatively low compared with many European countries; particularly south European countries such as Turkey and Greece (figs 3.2.5A and 3.2.5B).

Incidence rates (per 100 000 population) and prevalence rates (% of population) for hepatitis B infection in the UK and in other European countries. (A) Incidence rate; (B) prevalence rate. Source: World Health Organisation.230
Primary biliary cirrhosis
Primary biliary cirrhosis is a disease characterised by inflammatory destruction of the small bile ducts within the liver that eventually leads to cirrhosis of the liver. The cause of primary biliary cirrhosis is unknown, but because of the presence of autoantibodies, it is generally thought to be an autoimmune disease. However, other aetiologies such as infectious agents have not been completely excluded.
About 90% of primary biliary cirrhosis occurs in women, and most commonly between the ages of 40 and 60 years. Incidence appears to be increasing sharply in the UK (table 3.2.6).236 For example, the prevalence of primary biliary cirrhosis in northern England rose sevenfold between 1976 and 1987,237 and by 70% from 1987 to 1994.238
Table 3.2.6 Incidence and prevalence rates (per 100 000 population) for primary biliary cirrhosis as reported from various studies in the UK, and in other countries
There are large geographical and secular variations in the prevalence of primary biliary cirrhosis world wide (table 3.2.6). The disease appears to be most common in north west Europe, particularly in northern Britain and Scandinavia: some of the highest reported prevalence rates are for northern England (34.5 per 100 000 population)243 and for northern Sweden (15.2).245 These compare with much lower prevalence rates of 1.9 in Victoria, Australia,251 2.2 in Ontario, Canada,249 and 2.7 in Estonia,253 while primary biliary cirrhosis is rarely found in Africa or Asia.
Primary sclerosing cholangitis
Primary sclerosing cholangitis is a chronic inflammatory condition that occurs when the bile ducts inside and outside the liver become inflamed and scarred. As the scarring increases, blockage of the ducts leads to damage to the liver. Although the exact cause of primary sclerosing cholangitis is unknown, it is thought that the tissue damage is mediated by the immune system.257
Primary sclerosing cholangitis usually begins between the ages of 30 and 60 and is about twice as common in men as in women.120 Primary sclerosing cholangitis is closely associated with inflammatory bowel disease, particularly ulcerative colitis,257,258 and coeliac disease.177 Around 75–80% of northern European people with primary sclerosing cholangitis have underlying inflammatory bowel disease.120
Primary sclerosing cholangitis usually progresses to biliary cirrhosis, persistent jaundice, and liver failure. For patients with end stage primary sclerosing cholangitis, liver transplantation remains the only effective treatment. Primary sclerosing cholangitis also predisposes to cholangiocarcinoma in up to 30% of cases,120,259 and has been associated with increased risks of cancer of the colon, pancreas, gallbladder, and liver.260 It has also been shown to potentiate the risks of cancer of the colon in people with ulcerative colitis.261–263
Although the disease is becoming increasingly common, there is relatively little reported information on incidence or prevalence. Prevalence rates of 12.7 per 100 000 have been reported in south Wales in 2003,264 8.5,252 and 5.6265 per 100 000 population have been reported from Norwegian studies in the mid-1990s, and 20.9 per 100 000 for Minnesota, USA in 2000.254
Gallstone disease
Gallstones or cholelithiasis occur when bile stored in the gallbladder hardens into pieces of stone-like material. The two types of gallstones are cholesterol stones that are made primarily of hardened cholesterol, and account for about 80% of gallstones, and pigment stones that are darker and made of bilirubin. It is thought that cholesterol stones form when bile contains too much cholesterol, too much bilirubin, or not enough bile salts, or when the gallbladder does not empty for some other reason. However, the cause of pigment stones is uncertain, although they tend to occur in people who have cirrhosis, biliary tract infections, and hereditary blood disorders, such as sickle cell anaemia, in which too much bilirubin is formed.
Gallstone disease is the most common abdominal condition for which patients are admitted to hospital in developed countries.266 The incidence of gallstones increases with age and obesity, and it is higher in women than in men. Other risk factors include diabetes, Crohn’s disease, cholesterol lowering drugs, gastric bypass surgery, hormone replacement therapy, fasting, and rapid weight loss. Gallstones are very common in the UK among older age groups, with reported prevalence rates of 12% among men, and 22% among women, who were aged over 60 years in an ultrasound survey in Bristol.267
Gallstones can block the normal flow of bile if they lodge in any of the ducts that carry bile from the liver to the small intestine. Complications of gallstones include chronic inflammation or infection of the gallbladder (cholecystitis), abscess formation, acute pancreatitis, and biliary obstruction.266 Gallstones have been shown to be the dominant aetiological agent in 30–60% of cases of acute pancreatitis in the UK, and in 25–75% of cases in other European or Western countries (table 3.2.7).
Table 3.2.7 Aetiology (expressed as percentages) of acute pancreatitis, as reported from various regional studies in the UK, and in other European or Western countries
Hospital admission rates and operations for gallstones have mainly increased in the UK in recent decades,213,268–271 although admissions reflect the availability of hospital facilities and the prevalent medical practice, as well as the level of incidence.271 In England, for example, admissions increased by 30% in men, and by 64% in women, in England from 1989–90 to 1999–2000.271
Figure 3.2.6 shows prevalence rates for gallstones, as measured through cross-sectional ultrasound surveys, in regional studies in England and in other European countries. The rates varied between 5 and 24%, they were typically 1.5 to two times higher in women than in men, and the highest rates were reported for Norway and for the former East Germany. The rates reported from the English study of Bristol are lower than those in most of the other European countries.

Prevalence rates (expressed as percentages) of gallstones among men and women in regional ultrasound surveys in the UK and in other European countries. Source: Aerts and Penninckx, 2003.266 Notes: The year before publication is stated where the study period was not specified. Study regions, overall study sizes and references for the different studies from left to right are: Norway—Schwedt, n = 1371272; East Germany—Neuruppin, 3226273; Sweden—Stockholm, 556274; France—Viduaban, 831275; Italy—multicentre study, 29 379276; Poland—national study, 10 133277; Italy—Sirmione, 1911278; Romania—Timisoara, 1323277; Spain—Guadalajara, 536279; Italy—Rome, 2320280; Denmark— Copenhagen, 3608281; England—Bristol, 1896267; Germany—Romerstein, 2498.282
Haemochromatosis
Haemochromatosis is an inherited condition that is characterised by the deposition of excessive iron in tissue and organs throughout the body, resulting in progressive damage and organ failure. Apart from liver disease, other conditions associated with iron overload include diabetes, joint damage, heart disease, and impotence. Excessive iron overload is associated with increased risks of mortality; mainly from liver cirrhosis, liver failure, liver cancer, and diabetes. Many patients with haemochromatosis remain undiagnosed for several years during the early stages of this condition.227 Although reliable prevalence data for haemochromatosis are not available for the UK, the disease is common in northern Europe. Prevalence rates of 1% and 0.93% have been reported for Germany and Ireland, with lower rates reported for France (0.5%), Sweden (0.5%), Denmark (0.38%), Iceland (0.37%), and Norway (0.34%).227
Incidence of diseases of the pancreas
Acute pancreatitis
Like liver disease, acute pancreatitis is also becoming increasingly common in the general population of the UK. It refers to a sudden inflammation of the pancreas that is activated by destructive pancreatic enzymes. Acute pancreatitis often lasts for a short period of time and, in many cases, it resolves. Severe cases of pancreatitis, however, particularly when necrotising pancreatitis occurs, usually lead to prolonged stays in hospital of three to six months, often with many weeks spent in intensive care and with a high mortality rate.
As there is no specific treatment for acute pancreatitis, surgery and manipulative endoscopy may be required for common duct stones or pancreatic necrosis, and especially for infected necrosis, which occurs in about 5–10% of cases of acute pancreatitis. However, surgery can carry a high mortality, particularly in the short term. Traditional open surgery for infected pancreatic necrosis carries a mortality rate of up to 50%, although a number of less invasive techniques, such as radiological drainage and a minimal access retroperitoneal approach, have been developed.283
The two main causes of acute pancreatitis are blockage of the pancreatic duct by gallstones and heavy alcohol consumption, although other causes can include abdominal trauma, surgery, hyperlipidaemia (types IV, V or VI), hyperparathyroidism, infections such as mumps, and some drugs such as corticosteroids, oral contraceptives, and thiazide diuretics. Because almost all people with an attack of acute pancreatitis are admitted to hospital, acute pancreatitis is one of few gastrointestinal diseases for which hospitalised incidence provides a good measure of true incidence.
Several British studies have shown sharp increases over time in the incidence of acute pancreatitis in recent decades (tables 3.2.7 and 3.2.8), although variation in the definition of incidence to some extent affects comparability across studies. One study of four counties in south east England reported a twofold increase in the incidence of acute pancreatitis from 4.9 to 9.8 per 100 000 population from 1963–74 to 1987–98.303 A recent national English study reported a 43% increase in incidence from 1989–90 to 2000–01,304 and an earlier study of Bristol reported a 35% increase in incidence from 1968 to 1979.285
A study of Scotland reported an even greater, 10-fold increase in incidence of acute pancreatitis among men, and a fourfold increase among women, from 1961 to 1985 (table 3.2.8),305 although a more recent Scottish study reported a more modest (62%) increase from 1985 to 1995.306 Increases in the incidence of acute pancreatitis have been attributed to a rise in alcoholic pancreatitis, linked to the increased use of alcohol in the community in the UK,284,303 and in Finland,291 although elsewhere in western Europe increases in incidence have been linked to gallstones.299 Table 3.2.7 shows trends in aetiology across studies, most notably a rise in alcoholic pancreatitis, and a fall in gallstones pancreatitis, across most British studies since the 1950s.
Table 3.2.8 Incidence rates (per 100 000 population) for acute pancreatitis, as reported from various national and regional studies in the UK
Despite differences in the measurement of incidence across studies, recently reported rates for acute pancreatitis are substantially higher in Scotland (about 25–65 per 100 000),287,305,306 than in England (about 8–25 per 100 000).285,288,303,304 Incidence rates in Scotland are typically comparable with the high rates reported in the Scandinavian countries,293,298,307,308 Iceland,301 and Germany,309 while rates in England are comparable with those in the Netherlands.310,311
Chronic pancreatitis
Chronic pancreatitis occurs when digestive enzymes attack and destroy the pancreas and nearby tissues, causing scarring and pain. It is not usually the result of recurrent attacks of acute pancreatitis but seems to develop separately. The pancreatic gland becomes fibrosed and possibly calcified. Chronic pancreatitis is a disease that is characterised by horrific pain, it severely impairs quality of life and shortens life expectancy, although the exact prognosis is difficult to quantify and it is poorly documented.
The most common cause of chronic pancreatitis is long term, heavy alcohol use. Alcohol has been shown to be the dominant aetiological agent in about 70–80% cases of chronic pancreatitis in recent European studies.312–314 However, chronic pancreatitis may be caused by blockage or narrowing of the pancreatic duct by gallstones. In other cases it is genetically linked, or it may be triggered by only one acute attack, especially if the pancreatic ducts are damaged, or it can be caused by the effects of malnutrition when calcification is present, and in other cases the cause cannot be determined. Some patients with chronic pancreatitis develop pancreatic cancer.
Chronic pancreatitis is more common in men than in women, and it often develops between the ages of 30 and 50. The prevalence of chronic pancreatitis in the UK is currently about 40–75 per 100 000 population,315 with an incidence of about eight new cases per 100 000. The tropical form of pancreatitis is a major health problem in southern Africa and Asia, with, for example, high prevalence rates of 114–200 and 25–50 per 100 000 reported for southern India,316 and Japan,317,318 respectively.
Although less common than acute pancreatitis, the incidence of chronic pancreatitis is also increasing,319 particularly with large increases in alcohol use in the UK population over the past 30 years.320,321 Between 1989–90 and 1999–2000 the hospital admission rate for chronic pancreatitis doubled in England.304
There is a large geographical variation in the reported incidence of chronic pancreatitis in Europe, partly reflecting differences in alcohol consumption. High rates of 26, 23, and 14 per 100 000 have been reported for France,322 Finland,314 and Stockholm County, Sweden,222 moderate rates of 5–8 per 100 000 in Luneberg County, Germany,309 Warsaw, Poland,323 and the Czech Republic,314 and a low rate of 1.3 in Switzerland.314
Incidence of gastrointestinal cancer
Gastrointestinal cancer is the most common type of cancer in Europe. Out of 2.1 million new cancers in Europe in 2000, gastrointestinal cancers accounted for 579 542 or 28.3% of the total.324 In the UK, there are about 60 000 new cases of gastrointestinal cancer each year.
Of all cancers in men in England and Wales in 1997, colorectal cancer was the third most common (incidence of 14 900, 13.7% of all new cases), while cancers of the stomach (5800, 5.3%), oesophagus (3600, 3.3%), and pancreas (2700, 2.5%) were ranked 5th, 7th, and 10th, respectively.14
Among women, colorectal cancer was the second most incident cancer (14 000, 12.4% of all new cancers), and cancers of the stomach (3300, 2.9%), pancreas (3000, 2.7%), and oesophagus (2500, 2.2%) were ranked 8th, 9th, and 12th, respectively. Together, gastrointestinal cancers represent around a quarter of all cancers in men (the most common cancer grouping by some margin), and one fifth of cancers in women, behind only breast cancer.14,103
Colorectal cancer
Colorectal cancer is the most common type of gastrointestinal cancer in the UK, with about 30 000 new cases a year, and an incidence rate of about 50 per 100 000 population. It accounts for just over half of all gastrointestinal cancers in the UK, and mainly affects people aged between 50 and 80.324 Of all cancers, when both sexes are included, colorectal cancer is the second most common cancer in England and Wales.14
Risk factors for colorectal cancers include a family history of bowel cancer, long term inflammatory bowel disease, high fat diets with low consumption of fibre, smoking, and lack of exercise. Table 3.2.9 illustrates the strong familial association with colorectal cancer. The predisposition to colorectal cancer among people with ulcerative colitis is well established,106,107,325 with relative risks as high as 21 cited.108,109 The link between Crohn’s disease and colorectal cancer is less well documented, although in recent studies it has been reported as comparable to that for ulcerative colitis.108,326,327
Table 3.2.9 Familial association in the lifetime risk of developing colorectal cancer
From 1971 to 1997 in England and Wales, age standardised incidence of colorectal cancer increased by about 10% in men from about 45 to 50 per 100 000 population, and also increased slightly in women from about 30 to 35 per 100 000.14
Gastric cancer
Gastric cancer is twice as common in men as in women, and mainly affects older people: 80% of cases are diagnosed in people aged between 60 and 80. There are currently about 10 000 new cases a year in the UK, representing about 15% of all gastrointestinal cancers, with an incidence rate of approximately 17 per 100 000 population. In the past 30 years there has been a change in the distribution of gastric cancers, with an increase in the incidence of proximal tumours near the gastro-oesophageal junction, but a larger decline in the incidence of antral cancers that used to dominate.324
Risk factors include longstanding infection with Helicobacter pylori, family history of gastric cancer, a history of gastric polyps, and other disorders such as atrophic gastritis and pernicious anaemia, poor hygiene and socioeconomic conditions, malnutrition, heavy alcohol consumption, smoking, and certain food products and preservatives, including salt and pickled foods. Diets high in fresh fruit and vegetables seem to protect against gastric cancers as they contain high levels of antioxidant vitamins that are thought to protect the stomach lining.
From 1971 to 1997 in England and Wales, the age standardised incidence of gastric cancer fell by about 50% in men from about 30 to 20 per 100 000, and almost halved in women from about 15 to 8 per 100 000.14
Oesophageal cancer
There are about 7000 new cases of oesophageal cancer a year in the UK, with an incidence rate of about 11 per 100 000 population. This represents about 11% of all gastrointestinal cancers in the UK, which is higher than the 5.9% in Europe as a whole. Oesophageal cancers mainly occur in people between the ages of 60 and 80, and are three times more common in men than in women.324
The most important risk factor is smoking, although others include severe acid reflux from the stomach, heavy alcohol consumption, obesity, a rare muscular disorder known as achalasia, diet, and chewing of betel nuts. Although the incidence of adenocarcinoma of the oesophagus is increasing in several European countries, squamous cell carcinoma remains the predominant histological type. In Europe, it is estimated that 63% of all squamous cell carcinomas in men and 33% in women are attributable to smoking.328
It is unclear why oesophageal adenocarcinoma is on the increase, although it is thought to be linked to the rise of gastro-oesophageal reflux disease.21,329 From 1971 to 1997 in England and Wales, age standardised incidence of oesophageal cancer increased by about 50%, from 8 to 12 per 100 000 population in men, and from 4 to 6 per 100 000 in women.14
Pancreatic cancer
In the UK, there are about 6000 new cases of pancreatic cancer a year (about 8% of all gastrointestinal cancers), with an overall incidence rate of about 11 per 100 000 population. Cancers of the pancreas are more common in men than in women, and are predominantly diagnosed in the 50–70 year age group.324
Risk factors include pre-existing chronic pancreatitis, liver cirrhosis, diabetes and a history of surgery to the upper digestive tract, smoking, family history, and environmental exposure to certain insecticides or chemicals such as gasoline. Chronic pancreatitis is an especially important risk factor for pancreatic cancer, with relative risks as high as 27 having been reported.330
From 1971 to 1997 in England and Wales, age standardised incidence of pancreatic cancer fell by approximately one sixth in men from about 12 to 10 per 100 000 population, but remained stable at about 7 per 100 000 in women.14
Liver cancer
Most liver cancers (about 95%) are metastatic: primary cancer sites in order of frequency are colon and rectum, pancreas, oesophagus, stomach, breast, lung, and kidney.324 There are about 2300 new cases of primary liver cancer a year, with an overall incidence of approximately 4 per 100 000 population. Primary liver cancer accounts for about 3% of all gastrointestinal cancers in the UK, and is more common in men than in women.
Risk factors for primary liver cancer include liver cirrhosis, either of alcoholic aetiology, through hepatitis B or C infection, or through inherited conditions such as haemochromatosis and α1 antitrypsin deficiency, exposure to certain chemicals such as vinyl chloride, smoking, and long term use of anabolic steroids.
Incidence of other gastrointestinal diseases and related conditions
Appendicitis
Appendicitis refers to the inflammation of the appendix when it becomes blocked. The blockage is thought to be caused by a build up of thick mucus within the appendix, or by a stool that enters the appendix from the caecum, or by swollen lymphatic tissue within the appendix. The most common complication of appendicitis is perforation, which is usually caused by a delay in treatment, and which can lead to a periappendiceal abscess or diffuse peritonitis.
Appendicitis can occur at any age, although it is rare in children under 2 years of age. Incidence peaks in late teens and early twenties, it declines with increasing age, and it is higher in men than in women. Appendicitis has also been linked to low fibre and refined carbohydrate diets, amoebiasis, bacterial gastroenteritis, and mumps.
About 10% of the UK population will develop acute appendicitis at some stage, and about 70 000 appendicectomies are performed each year. The incidence of acute appendicitis declined in the UK and in most other Western countries between the 1930s and the early 1990s, and there was a further reduction in hospital admissions for acute appendicitis, of 13% among men and 19% among women in England during the 1990s.331
Obesity
Obesity is not a gastrointestinal disorder but plays a significant part in many diseases of the liver and gut. A recent report by the Royal College of Physicians dealt with the growing epidemic of obesity in the UK and outlined its impact on a number of diseases, including heart disease, diabetes, and gastrointestinal disorders such as gallstones, liver disease, and gastrointestinal cancers.6 Other studies have also documented obesity as a risk factor for a wide range of gastrointestinal diseases, such as colorectal cancer,332–334 oesophageal cancer,334–336 gastric cancer,337,338 hepatocellular cancer,339,340 gallstone disease,328,333 alcoholic liver disease,341–343 non-alcoholic fatty liver disease,333,339,342,344–346 gastro-oesophageal reflux disease,17 Barrett’s oesophagus,347,348 hiatus hernia,349 surgical complications,350,351 and prognosis for acute pancreatitis.352,353
The Royal College of Physicians recommend prevention strategies targeted towards improvements in nutritional labelling of foods, public education, and social marketing and retailing, promotion of leisure-time sports and activities, NHS priorities and planning, promoting healthy schools, “active transport”, further research and development, and promotion of local level programmes.6
Alcohol related morbidity
Several of the gastrointestinal disorders covered in the previous sections of this report, such as alcoholic liver diseases, upper gastrointestinal haemorrhage from oesophageal varices, acute and chronic pancreatitis, gastric, oesophageal and liver cancer, and gastro-oesophageal reflux disease are linked to alcohol consumption in varying proportions of cases. Alcohol has often been associated with a wide range of other non-gastrointestinal diseases and conditions such as injury from traffic accidents, other trauma, violence, suicide, breast cancer, and haemorrhagic stroke, as well as being the direct cause of other disorders such as alcoholic psychoses and alcoholic dependence syndrome.354 In the UK in recent years, there have been reports of increasing numbers of people admitted to general hospitals with alcohol related illnesses, particularly in Scotland.220,355,356 For example, a recent study in Glasgow reported that during one month, 51% of all gastroenterology inpatients had been admitted owing to alcohol related conditions,357 and 65% of these were caused by alcoholic liver disease.
Infectious intestinal diseases and food poisoning
Food poisoning and infectious intestinal disease (IID) are important diseases in the UK. Food poisoning notifications and laboratory reports of pathogens responsible for IID have been falling in the past four years. However, in 2001, there were over 85 000 food poisoning notifications; and 1 in 60 people consulted a GP for IID in England and Wales.358
Defaecation problems
Faecal incontinence, the involuntary loss of rectal contents at a socially inappropriate time or place, is an underappreciated condition, which affects at least 2% of adults in the community. The prevalence in elderly people is up to 15%, and higher still among those living in residential or nursing homes. However, compared with urinary incontinence, the condition is neglected.359 Neurological related bowel problems present a heavy burden on nursing resources,360,361 with diseases or conditions such as multiple sclerosis,362–364 Parkinson’s disease,365 spina bifida,366 stroke,367 and spinal cord injuries,368–370 associated with faecal incontinence or constipation, or both in 50% or more cases.371 The management of constipation alone can account for up to 10% of district nursing time.372
Biliary atresia
Biliary atresia is a disease of unknown cause in which all, or part of, the extrahepatic bile ducts are obliterated, leading to complete biliary obstruction. Biliary atresia is, however, a rare condition with fewer than 50 cases annually in the UK and Ireland.373
Short bowel syndrome (HPN)
Patients with a short small intestine as a result of disease or surgery may need additional feeding. Home parenteral nutrition (HPN) is a complex technology involving the intravenous infusion of all nutrients required for life directly into a central vein. These nutrients include carbohydrates, fat, amino acids, electrolytes, trace elements, and water. The patient, or carer, is taught to manage the complicated routine, enabling transfer of care to the home. Patient referral patterns for HPN treatment are inconsistent, with some regions in the UK having very few patients receiving HPN. However, there are several large centres in the UK where HPN is considered as an essential, life-saving treatment. The point prevalence of patients receiving HPN in the UK in 2003 was 8.8 per million. Prevalence was higher in Scotland (12.9 per million) than in England (8.6), Wales (4.5), and Northern Ireland (9.6). There is considerable regional variation in period prevalence of patients receiving HPN in the UK: across strategic health authorities in the UK, prevalence varied between 1 and 21 per million population, with higher prevalence reflecting that HPN is more common in areas that are close to major referral centres.374
Iron deficiency anaemia
Iron deficiency anaemia (IDA) resulting from gastrointestinal bleeding is a common feature of many gastrointestinal disorders, including colorectal and gastric cancers. Patients investigated for IDA have been found to have gastrointestinal cancers in about 5–20% of cases,375–377 while IDA is also one of the most common presenting symptoms of coeliac disease.378
International comparisons of the incidence of gastrointestinal cancers
Figure 3.2.7 shows estimates of population based incidence rates for the main types of gastrointestinal cancer in the UK and in other regions of Europe in 1995.328 Among men, the UK had the third highest, age standardised incidence of oesophageal cancer in Europe (12.9 per 100 000), after France (17.0) and Hungary (14.9), with an overall rate of 9.9 for the whole of Europe. Among women, the UK had the second highest incidence of oesophageal cancer (5.9 per 100 000) after Ireland (6.6), with an overall rate of 1.9 for Europe.328

Estimates of age standardised population based incidence rates (per 100 000 population) for the main types of gastrointestinal cancer among men and women in the UK, eastern Europe, northern Europe, southern Europe, western Europe, and in Europe in 1995. (A) For colorectal cancer; (B) for oesophageal cancer; (C) for gastric cancer; (D) for pancreatic cancer. Notes: Western Europe includes Austria, Belgium, France, Germany, Luxembourg, Switzerland, and The Netherlands. Eastern Europe includes Belarus, Bulgaria, Czech Republic, Hungary, Poland, Republic of Moldova, Russia, Slovakia, and the Ukraine. Northern Europe includes Denmark, Estonia, Finland, Iceland, Ireland, Latvia, Lithuania, Norway, Sweden, and the UK. Southern Europe includes Albania, Croatia, Greece, Italy, Macedonia, Malta, Portugal, and Spain. Europe refers to all countries listed above for these four regions. Source: Bray et al, 2002.328
Incidence rates for gastric cancer among men and women in the UK were similar to those in western Europe and in northern Europe, but lower than in eastern Europe, southern Europe and Europe overall. Incidence of gastric cancer was highest in eastern Europe, and probably reflects the relatively low levels of affluence in these countries, and the resulting poor diet of their inhabitants. For both colorectal and pancreatic cancers, incidence in the UK among both men and women was very similar to those in Europe overall.328
Figure 3.2.8 shows incidence rates of colorectal cancers in the UK and in 26 other European countries in 2000. Incidence rates vary greatly across countries among men, although the highest rates were in eastern European states such as the Czech Republic (60.3 per 100 000), Hungary (59.8), and Slovakia (50.6). The rate for the UK (35.4) is similar to the average of these 27 countries (35.9). Among women, there is considerably less variation in national rates, with the UK incidence rate (25.3) similar to the European average of 24.2. The UK ranked as 13th of 27 for highest incidence of colorectal cancer in men, and 11th for women.
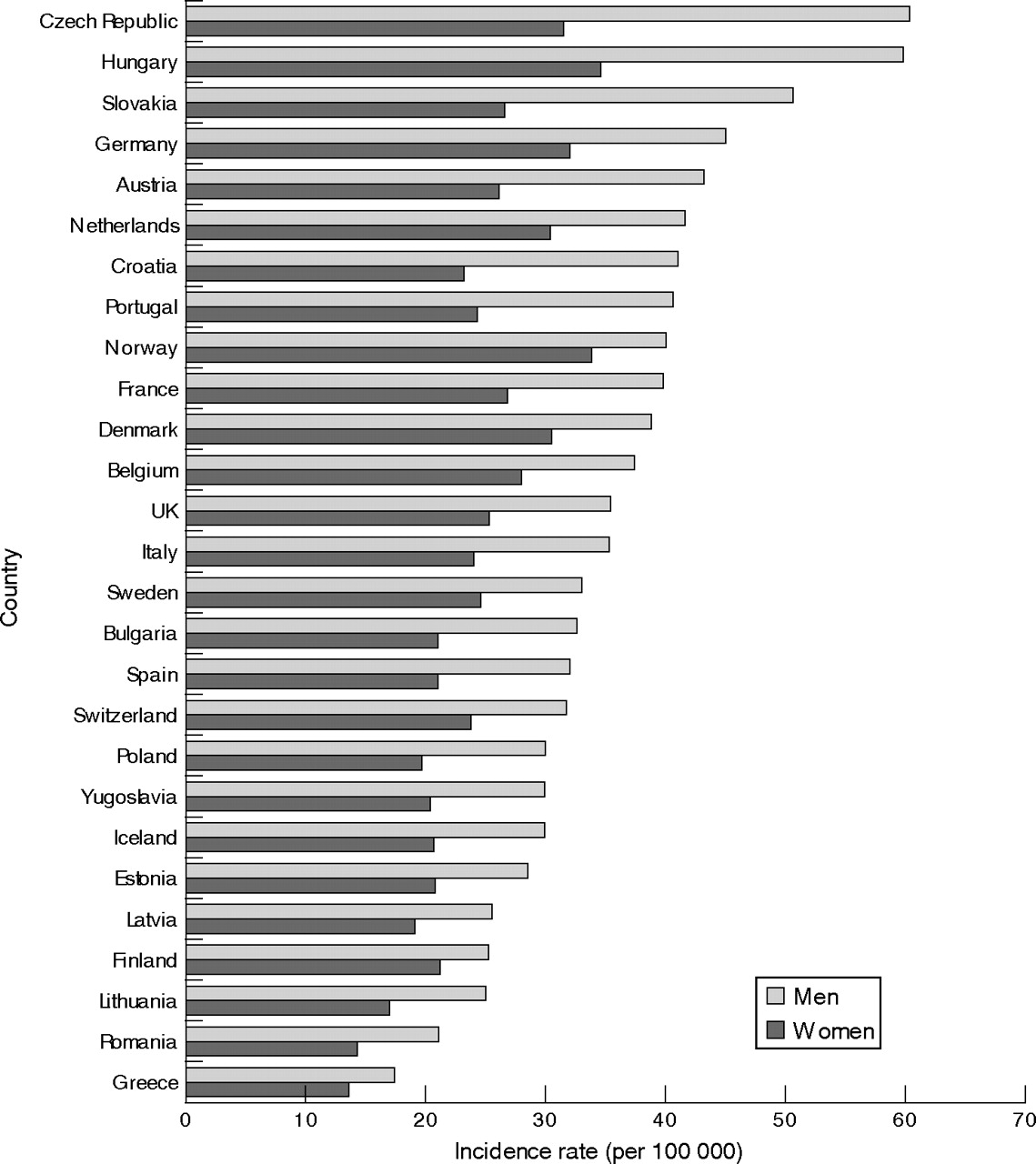
Standardised population based incidence rates (per 100 000 population) for colorectal cancer in 27 different European countries, 2000. Source: Keighley, 2003.324
3.3 Mortality from gastrointestinal diseases
Of 533 329 deaths in England and Wales in 2000, 59 959 (11.2%) had a gastrointestinal disease as the certified underlying cause of death. These include diseases of the digestive system (37% of all deaths from gastrointestinal disease), malignant neoplasms of the digestive system (62%), benign and other neoplasms of the digestive system (0.1%), intestinal infectious diseases (0.9%), and viral hepatitis (0.3%; tables 3.3.1 and 3.3.2).
Table 3.3.1 Population based mortality rates for the different ICD-9 chapters in England and Wales, 1990 and 2000
Table 3.3.2 Population based mortality rates for different gastrointestinal diseases in England and Wales, 1990 and 2000
Diseases of the digestive system, which exclude gastrointestinal neoplasms and infectious diseases, ranked as the fourth ICD chapter that accounted for most deaths in England and Wales in 2000, after diseases of the circulatory system (207 228 deaths), neoplasms (134 793), and diseases of the respiratory system (92 461).
Figure 3.3.1 shows population based mortality rates for each major body system when deaths from cancer were allocated to their respective body systems; for example, when gastrointestinal cancers were included with diseases of the digestive system, when respiratory cancers were included with diseases of the respiratory system, etc. Then, gastrointestinal disease was the third body system that accounted for the most deaths (59 000), after circulatory diseases (207 000) and respiratory diseases (123 000). Among people aged 15–64 years, however, the mortality rate for gastrointestinal diseases was roughly equal to that from respiratory diseases, as the leading major cause of death after circulatory diseases among working aged people (fig 3.3.2).

Population based mortality rates for major disease groupings, in England and Wales, 2000: people of all ages. Source: ONS, 2001.379

Population based mortality rates for major disease groupings, in England and Wales, 2000: people aged 15–64 years. Source: ONS, 2001.379
The number of deaths from diseases of the digestive system in 2000 increased by 20% from 18 429 in 1990. Deaths from malignant neoplasms of the digestive system fell by 10% from 40 965 in 1990, and the small numbers of deaths from intestinal infectious diseases and from viral hepatitis respectively, almost trebled and increased by 80% from 1990 to 2000 (table 3.3.2).
The major causes of death from diseases of the digestive system, excluding gastrointestinal cancers, in 2000 were liver cirrhosis (22%), peptic ulcer (18%), vascular insufficiency of the intestine (9%), diverticular disease of the intestine (8%), and gastrointestinal haemorrhage (6%; fig 3.3.3).

Percentage causes of all deaths from diseases of the digestive system (excluding cancers) in England and Wales, 2000. Source: ONS, 2001.379
Gastrointestinal cancer is the most common cause of cancer death of all major cancer groupings. In England and Wales in 2000, gastrointestinal cancers caused 27% of all cancer deaths, followed by respiratory cancers (23%) and cancers of the genitourinary system (17%; fig 3.3.4). The gastrointestinal tract was also the most common site for all cancer deaths (fig 3.3.5).
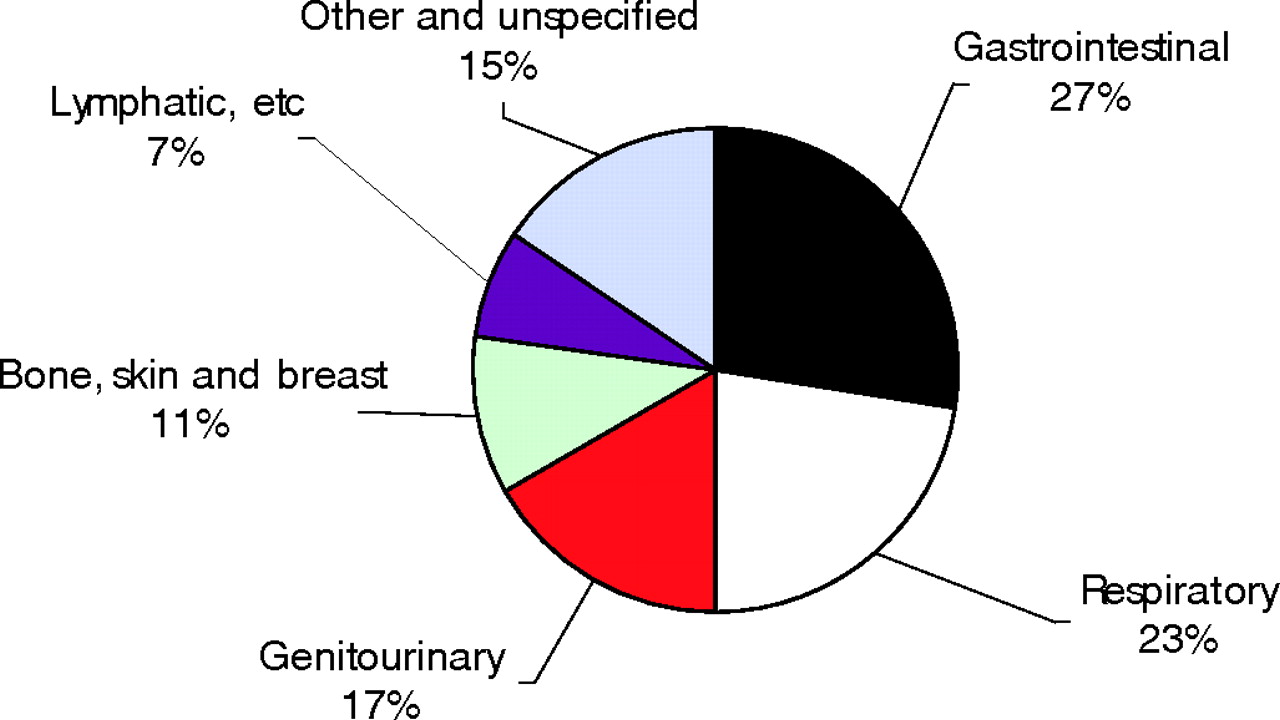
Percentage causes of all deaths from cancer, according to major groupings of cancer, in England and Wales, 2000. Source: ONS, 2001.379

Percentage causes of all cancer deaths, according to the site of the cancer, in England and Wales, 2000. Source: ONS, 2001.379
Figure 3.3.6 shows the most common sites for all gastrointestinal cancer deaths. These were the colon and rectum (39% of all gastrointestinal cancer deaths), the pancreas, the oesophagus, and the stomach (16% each).

Percentage causes of all gastrointestinal cancer deaths, according to the site of the cancer, in England and Wales, 2000. Source: ONS, 2001.379
Table 3.3.3 shows the number of deaths and corresponding population based mortality rates in England and Wales in 2000 among working aged people (aged 15–64 years) for some of the most common diseases and causes of death in the general population. The mortality rate for diseases of the digestive system (16.3 per 100 000 population) was lower than that from all cancers (97.6) and from ischaemic heart disease (43.4), but was about twice as high as for stroke and for pneumonia, six times higher than for diabetes mellitus, and 12 times higher than for asthma. If gastrointestinal cancers are included with diseases of the digestive system as gastrointestinal diseases, the corresponding mortality rate (39.9) was only slightly lower than for ischaemic heart disease, and much higher than for stroke, pneumonia, diabetes mellitus, chronic airways obstruction, and asthma (fig 3.3.7).
Table 3.3.3 Population based mortality rates for selected causes of death among people aged 15–64 years in England and Wales, 2000

Population based mortality rates (per 100 000 population) for selected causes of death among people aged 15–64 years in England and Wales, 2000. *Gastrointestinal diseases include diseases of the digestive system, malignant neoplasms of the digestive system, benign and other neoplasms of the digestive system, intestinal infectious diseases, and viral hepatitis. Source: ONS, 2001.379
Mortality statistics, based on underlying cause of death, to some extent underreport true mortality from gastrointestinal diseases and, importantly, this underreporting is greater for gastrointestinal diseases than for the two other major causes of death, circulatory and respiratory diseases. The following sections describe mortality rates and patterns in the UK for some of the main gastrointestinal disorders in anatomical sequence.
Mortality from diseases of the stomach and duodenum
Peptic ulcer
Although the incidence of peptic ulcer has fallen sharply in the UK in recent years, it was still the second largest cause of gastrointestinal death, after liver cirrhosis, in England and Wales in 2000, with over 4000 deaths and a mortality rate of 7.6 per 100 000 population (table 3.3.2).
Patient deaths after hospital admission for peptic ulcer in the UK between 1991 and 1994 was reported as 4.4%,381 with increased risks of mortality for patients who had no previous history of peptic ulcer (relative risk = 3), or who were undergoing surgery, were elderly or were current users of non-steroidal anti-inflammatory drugs. Much higher case fatality rates of 34% for perforated peptic ulcer,382 and 43% for perforated duodenal ulcer,383 have been reported in regional British studies.
Gastrointestinal haemorrhage
Gastrointestinal haemorrhage was the cause of almost 1500 deaths in England and Wales in the year 2000, with a population based mortality rate that had risen by over 17% since 1990 (table 3.3.2).
Patient deaths for upper gastrointestinal haemorrhage vary in the UK from about 5% to 15% (table 3.3.4), although lower rates of less than 4% have been reported.89,90 Case fatality varies strongly according to case mix, which would explain some of the geographical variation; while, as ever, case fatality is affected by factors such as the length of follow-up and the inclusion of deaths after discharge with in-hospital deaths.
Table 3.3.4 Case fatality rates (% of cases) after hospital admission for upper gastrointestinal haemorrhage, as reported from regional studies in the UK
Case fatality for upper gastrointestinal haemorrhage is increased in surgical cases, and for cases of haemorrhages in inpatients. For example, surgical mortality rates of 13–41% have been reported from studies since the 1980s,84,85,89 while case fatality for haemorrhages in inpatients of 18–45% have also been reported.73,74,86,87,90,91,334,335,387 Other important risk factors include gastrointestinal malignancies or other pre-existing comorbidity, shock, and advanced age.92,391,398 Despite improvements in treatment and management over time, a lack of impact on patient deaths is probably linked to older ages at presentation, increases in comorbidities,399 and less selective reporting over time.400
Mortality from diseases of the small bowel and colon
Inflammatory bowel disease
Inflammatory bowel disease is a major cause of debilitating morbidity, particularly among young adults, rather than a major cause of mortality. In the year 2000 in England and Wales, there were only 166 and 184 deaths, respectively, which were certified with Crohn’s disease and ulcerative colitis as the underlying causes of death.
Most British population based studies have found no increased mortality among people with inflammatory bowel disease. For example, a study in Leicestershire reported standardised mortality ratios (SMRs) of 0.72 (compared to a mortality of 1.00 in the general population) for Crohn’s disease,401 and 0.93 for ulcerative colitis,402 among European subjects; another study of three district hospital general centres reported SMRs of 0.94 for Crohn’s disease and 0.93 for ulcerative colitis.403
However, some population based studies have reported increased mortality. For example, a study of Crohn’s disease in Cardiff from 1934 to 1976 reported a significantly increased SMR of 2.2, that was particularly high in people aged under 20 (SMR of 11.0).404 Another study, a national UK primary care based study during the 1990s, reported significantly increased hazard ratios of 1.7 for Crohn’s disease and 1.4 for ulcerative colitis. The hazard ratios were more highly increased among younger age groups: 3.8 among people aged 20–39 years with Crohn’s disease, and 1.8 among those aged 40–59 with ulcerative colitis.405
Coeliac disease
Although coeliac disease is not usually recorded as an underlying cause of death, people with coeliac disease have been shown to be at moderately increased risks of mortality. For example, cohort studies in Scotland, Italy, and Sweden have reported increased mortality of 1.9- to 3.8-fold respectively,406–409 with excess mortality often caused by malignant lymphomas or malignancies of the gastrointestinal tract.406–410
Diverticular disease
Diverticular of the intestine is quite a common cause of death in the UK, accounting for 1826 deaths in England and Wales in 2000. Population based mortality rates for diverticular disease increased greatly over the course of the 20th century, although this probably reflects an increase in the use of barium enema diagnostic testing and changing fashions of death certification, as well as a true increase in the prevalence of diverticular disease. From 1979 to 1999, age standardised population based mortality rates remained fairly constant in England at about 1.5 per 100 000 population in men and 2.25 per 100 000 in women.212
Mortality rates after hospital admission for diverticular disease are fairly low. From 1989–90 to 1990–2000 in England, age standardised in-hospital case fatality rates were about 2.5% and 3.5% among men and women respectively,212 while a recent study in London reported case fatality of 9.5% at one year after admission.411
Higher mortality is associated with the severe complications such as perforated diverticular.203 For example, a recent study in Exeter reported a case fatality rate of 5.7% for acute complications of diverticular disease, which rose to 18% for those undergoing surgery412; a study in Birmingham reported case fatality of 11% for acute complications of diverticular disease from 1985–88413; and a study in Glasgow reported surgical mortality of 26% for perforated diverticular disease from 1976 to 1983.414
Mortality from diseases of the liver
Chronic liver disease and cirrhosis
Chronic liver disease and cirrhosis is one of the major causes of death from gastrointestinal disease in the UK. Cirrhosis mortality increased by 50% in England and Wales from 6 to 9 per 100 000 population during the 10 year period from 1990 to 2000 (table 3.3.2). From 1957–61 to 1997–2001 it increased by over threefold among men in England and Wales and in Scotland, by 250% among women in England and Wales, and by 160% among women in Scotland.415 Other studies have reported increases of 350% in England from 1970 to 1998,416 and 112% in the West Midlands from 1993 to 2000.417
This contrasts with a fall of almost 30% in the EU average cirrhosis mortality rate of 14 to 10 per 100 000 from 1970 to 1998. Together with a rise in national alcohol consumption,320,321 and in hospital admissions for alcoholic liver disease,220 the increase in cirrhosis mortality in the UK has led to the recent publication of a national alcohol harm reduction strategy.221
In recent years, the large increases in the number of people infected with the hepatitis C virus, who have a rapid progression of liver cirrhosis,234 and a poor outcome,418 have also contributed towards the increase in cirrhosis mortality.234 Hepatitis C infection has also been the subject of national strategy and action plan documents in England.228,232
Mortality after hospital admission with chronic liver disease and cirrhosis is extremely high, and does not appear to have improved in the past 40 years.217,419 Mortality varies greatly according to aetiology: case fatality rates of 40% for alcoholic cirrhosis and 17% chronic hepatitis were reported from an earlier study of west Birmingham in 1959–76.217 Mortality from chronic liver disease and cirrhosis is still relatively low compared with that in many other European countries (fig 3.3.8). However, while cirrhosis mortality rates have been falling in most European countries in recent years, there has been a sharp increase in mortality in the UK (fig 3.3.9).

Standardised mortality rates (per 100 000 population) for chronic liver disease and cirrhosis, in men and women in the UK and in 17 other European countries, 2000. Source: Burroughs and McNamara, 2003.227
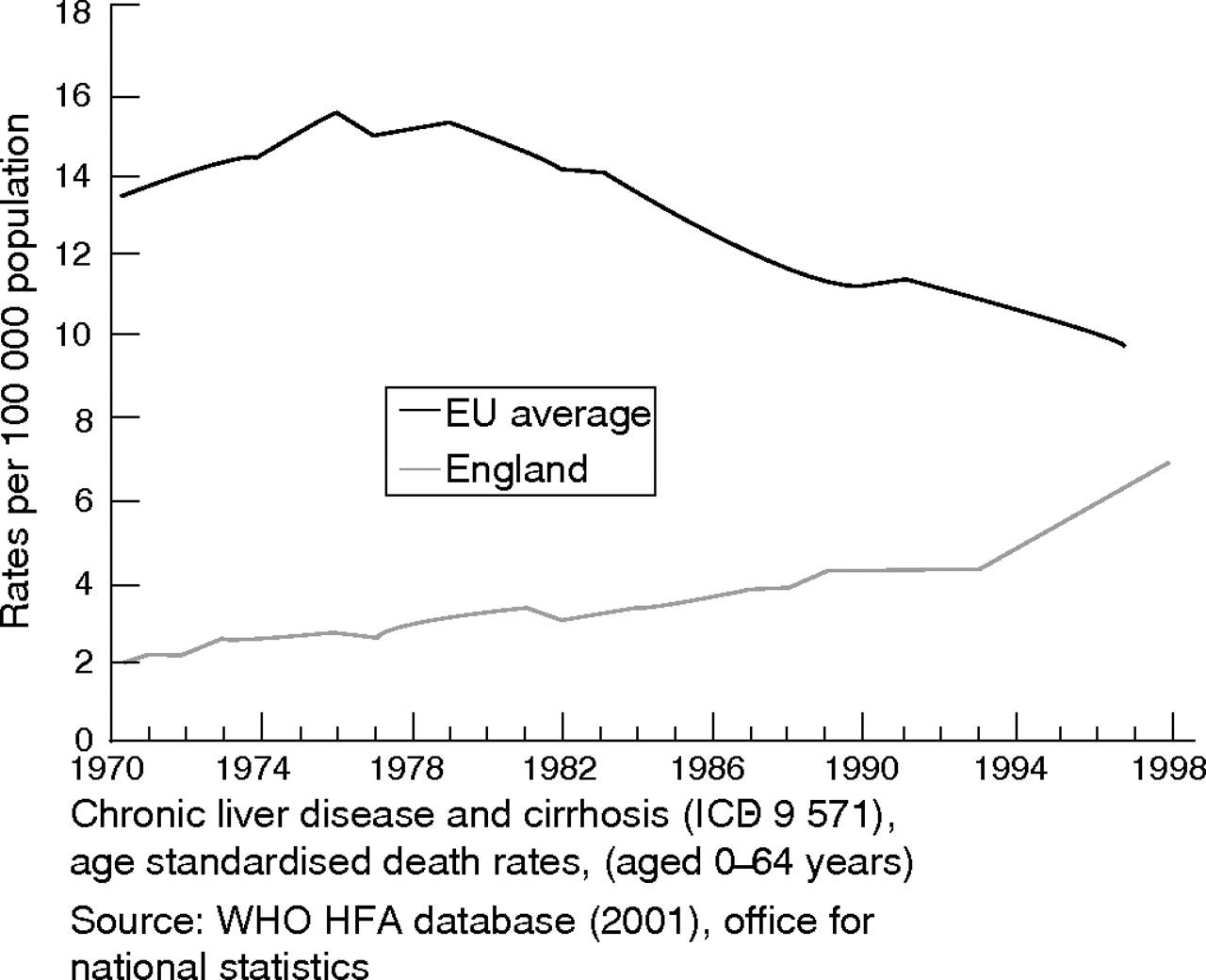
Trends in standardised mortality rates (per 100 000 population) for chronic liver disease in the UK and in Europe, 1970–1998. Source: Department of Health.420
Gallstone disease
Cholelithiasis, cholecystitis, and other diseases of the gallbladder were the cause of almost 800 deaths in England and Wales in 2000. Age standardised mortality for cholelithiasis fell from about 8.5 to 5.5 per 100 000 population in England from 1979 to 1989, but has not fallen since.271
Case fatality after hospital admission for gallstones fell by one third in men (from 0.6% to 0.4%) and by 42% in women (from 0.5% to 0.3%) in England from 1989–90 to 1999–2000.271 Although death rates after admission for gallstones are low, reported risk factors include acute pancreatitis, liver cirrhosis, age, acute cholecystitis, and diabetes.421
Mortality from diseases of the pancreas
Acute pancreatitis
Acute pancreatitis was the underlying cause of about 850 deaths in England and Wales in 2000. Population based mortality for acute pancreatitis in England and Wales increased slightly from 1.56 per 100 000 population in 1990 to 1.60 in 2000 (table 3.3.2), which had increased from 1.37 per 100 000 in 1980. A slightly lower mortality rate of 1.23 per 100 000 population was reported for Northern Ireland in 1974–83,422 while mortality increased from 2.7 to 4.0 per 100 000 in Nottingham from 1969 to 1983.423
Almost all people with acute pancreatitis are admitted to hospital. Case fatality has fallen over time from about 30% to roughly 10%, although as there seems to have been little further improvement in recent years, it remains a lethal disease. Case fatality at one year after admission for acute pancreatitis fell only slightly in four counties of southern England from 13.5% in 1963–74 to 11.8% in 1987–98.303 However, it appears to have fallen more sharply in Scotland; with reported reductions from 17.6% in 1961–65 to 5.6% in 1981–85,305 and from 9.1% to 6.6% from 1984 to 1994.306
Other British studies have reported case fatality of 9.1% in the Wessex region in 1994–95,288 9.0% in the North West Thames region in 1988–92,424 6.3% in Somerset in 1991–95,290 5.4% in Nottingham in the late 1990s,425 and 17% in Cottingham in 1998.426 Reported mortality rates for acute pancreatitis in England have been comparable or slightly higher than those in Europe. For example, case fatality was 6.1% in Luneberg, Germany from 1980 to 1994,427 5% in an Italian multicentre study in 1996–2000,428 7.5% in north Jutland from 1981 to 2000,308 and 10.7% in the Netherlands in 1995.310
Prognosis depends strongly on disease severity, with much higher case fatality in severe cases; which can be as high as 50% for surgery or for infected pancreatic necrosis.283,429 For example, two Scottish studies reported case fatality of 38% and 43% for pancreatic necrosectomy,430,431 and a study in London reported mortality of 39% for severe cases.432 The Italian multicentre study reported case fatality that varied between 1.7% for mild acute pancreatitis and 17% for severe cases,428 a Swedish study reported mortality of 27% in severe cases,433 while a German study reported mortality of 17% for necrotising pancreatitis, compared with 5% overall.434
Chronic pancreatitis
Although chronic pancreatitis is rarely recorded as an underlying cause of death—in only 77 cases in England and Wales in 2000—it often leads to substantially increased risks of mortality. For example, an American study identified an SMR of 3.6 for people who underwent treatment for chronic pancreatitis, with prognosis influenced strongly by age at diagnosis, alcohol consumption, and smoking.435 In particular, chronic pancreatitis often leads to increased risks of pancreatic cancer,330,436–440 which carries a very poor prognosis.
Mortality from gastrointestinal cancers
Colorectal cancer
Colorectal cancer is the most common cause of death from gastrointestinal cancer, causing 39% of all gastrointestinal cancer deaths, and 11% of all cancer deaths, in England and Wales in 2000. There were over 14 000 deaths from colorectal cancers in England and Wales in 2000, with a population based mortality rate of 27 per 100 000, which has fallen in recent decades.14
Prognosis for colorectal cancer is substantially better than for most other gastrointestinal cancers. Five year survival rates after diagnosis with colorectal cancer were 35% for men, and 39% for women in England and Wales between 1996 and 1999.441 These had increased from 31% and 35% respectively, in 1991–95. Over 80% of people with colorectal cancers in Europe undergo surgical treatment, and five year survival after surgical resection ranges from 40% to 60% depending on the stage of the tumour.324
Survival rates for colorectal cancer in the UK have been rising steadily over the past three decades, but substantial international differences suggest that there is considerable scope for further improvement: five year survival in the UK is lower than in Europe as a whole (table 3.3.5). The contrast in survival for the UK and western Europe is particularly marked for colon cancer, which often presents in an advanced state as an emergency, with a relatively poor prognosis. This further indicates that the poor survival in the UK has been mainly due to late diagnosis. Some studies have linked late diagnoses in the UK to patients’ GP consultation behaviour: for example, while rectal bleeding is a common symptom that affects up to 15% of adults,43 and is often an important symptom of colon cancer,442,443 many patients don’t seek medical advice.444
Table 3.3.5 Percentage five year survival after diagnosis for the main types of gastrointestinal cancers in various European countries
Survival rates are also lower in Europe than in the USA.445 This has also been attributed to diagnoses at earlier stages in the USA, as well as a higher proportion of cancers in the USA that are coded as adenocarcinoma in polyp, and which have a better prognosis.445
Oesophageal cancer
Cancers of the oesophagus represented over 6000 deaths in England and Wales in 2000, or 4.5% of all cancer deaths, with a mortality rate that has increased in recent decades.14
Five year survival after diagnosis with oesophageal cancer in the UK (9%) is slightly lower than a European average of 9.6% (table 3.3.5). The poor prognosis is largely due to the spread of tumours from the wall of the gullet, by the time of diagnosis. In Europe, only about one quarter of all oesophageal cancers are operable and, of these, five year survival is only about 20–30%.324
Gastric cancer
Cancers of the stomach are also responsible for 4.5% of all cancer deaths in the UK. In England and Wales in 2000, there were a total of 5779 deaths from gastric cancers, with a corresponding mortality rate of 10.9 per 100 000 population, which has fallen over time.14
The five year survival of about 12% in the UK is much lower than a European average of 21% (table 3.3.5). In Europe, only about 60% of gastric cancers are resectable when first diagnosed and surgical resection for cure is only achieved in about 40% of cases. Five year survival after surgical resection is closely related to the spread of the tumour, and varies from 95% for early cancers to only 20% for extensive lesions.324
Pancreatic cancer
Cancer of the pancreas also caused 4.5% of all cancer deaths in England and Wales in 2000 (6105 deaths), with a population based mortality rate of 11.5 per 100 000 that has remained fairly stable since the 1970s.14
Prognosis after diagnosis remains extremely poor. Survival is about 2% at five years among both men and women in England and Wales (table 3.3.5).441 A small minority (about 7%) of pancreatic cancers occur around the distal end of the bile and pancreatic ducts, present early and have relatively good prognosis. The rest, however, are located in the main body of the pancreas, present late and have dismal prognosis. In Europe, only 10% of pancreatic cancers are resectable, and the overall postoperative five year survival rate is only 10–15%.324 Prognosis in the UK is slightly worse than in the rest of Europe (table 3.3.5).
Liver cancer
Liver cancer caused 2091 deaths in England and Wales in 2000 and mortality has been increasing since the 1960s. Age standardised mortality rates per 100 000 population increased from 1.29 to 1.93 in women, and from 2.56 to 3.70 in men, between 1968 and 1996.446
Prognosis for liver cancer is also extremely poor (table 3.3.5). Five year survival in the UK was recently reported as 4%.324 This is largely because 95% of liver cancers are secondary deposits from tumours located elsewhere. Prognosis is slightly worse than the European average of 4.6% (table 3.3.5).
International comparisons of gastrointestinal cancer
Figure 3.3.10 shows population based mortality rates for each of the four main types of gastrointestinal cancer in the UK and, for comparison, with corresponding age standardised rates in other regions of Europe. Mortality from cancer of the oesophagus is particularly high in the UK (fig 3.3.10B), among both men and women, and it is higher than that in all other European countries presented here, except France (for men) and Ireland (for women).

Estimates of age standardised population based mortality rates (per 100 000 population) for different gastrointestinal cancers among men and women in the UK, eastern Europe, northern Europe, southern Europe, western Europe, and in Europe, 1995. (A) For colorectal cancer; (B) for oesophageal cancer; (C) for gastric cancer; (D) for pancreatic cancer. Notes: Western Europe includes Austria, Belgium, France, Germany, Luxembourg, Switzerland, and the Netherlands. Eastern Europe includes Belarus, Bulgaria, Czech Republic, Hungary, Poland, Republic of Moldova, Russia, Slovakia, and the Ukraine. Northern Europe includes Denmark, Estonia, Finland, Iceland, Ireland, Latvia, Lithuania, Norway, Sweden, and the UK. Southern Europe includes Albania, Croatia, Greece, Italy, Macedonia, Malta, Portugal, and Spain. Europe refers to all countries listed above for these four regions. Source: Bray et al, 1997.328
Mortality from gastric cancer, which is particularly high in eastern Europe (fig 3.3.9C), is substantially lower in the UK than in the rest of Europe. Death rates from colorectal cancer in the UK are similar to the European average, while mortality from pancreatic cancers in the UK is about average in women, but slightly lower in men.
Figure 3.3.11 shows large variation in mortality rates for colorectal cancer among men across 27 different European countries in 2000. Highest colorectal cancer mortality is found in eastern European countries such as the Czech Republic, Hungary, and Slovakia, with the UK mortality rate of 18.7 per 100 000 population similar to the European average of 19.1. Among women, there is much less variation, with the UK again similar to the European average.

Population based mortality rates (per 100 000 population) for colorectal cancer in the UK and in 26 other European countries, 2000. Source: Keighley, 2003.324
Figure 3.3.12 shows incidence to mortality ratios for colorectal cancers in the 27 European countries in 2000. The highest mortality ratios among men were in Lithuania (0.72), Latvia (0.70), and Denmark (0.61), and among women in Latvia (0.70), Iceland, and Lithuania (both 0.63). Mortality ratios in the UK, 0.55 and 0.53 for men and women, respectively, were similar to the corresponding European averages.

Mortality:incidence ratios for colorectal cancer in the UK and in 26 other European countries, 2000. Source: Keighley, 2003.324
3.4 Morbidity, quality of life
Although the data for mortality and activity in hospital and primary care are relatively reliable, they do not describe the burden of chronic GI diseases on the lives of sufferers. Several common chronic conditions—gastro-oesophageal reflux disease (GORD), non-ulcer dyspepsia, irritable bowel syndrome (IBS), and inflammatory bowel disease (IBD)—have mortality rates that are similar to those of the general population.447 Consulting rates vary, with some people more likely to opt for self care or alternative complementary therapies.53 Activity data reflect the burden on the health service, therefore, more than on the population.
Objective evidence or clinical assessment and self reported symptoms do not match well.20 Because of this there has been an increasing focus in health care generally, and in gastroenterology, in particular, on assessing patients’ health related quality of life (HRQoL). Measurements of HRQoL can be used to identify problems of individual patients or populations, to enhance understanding of diseases, and to assess health technologies, treatments, and service delivery.448
Using self reported HRQoL, the prevalence of functional GI disorders in a population in Australia was found to be 34.6%.449 Sufferers were found to be more likely to have impaired mental health and physical functioning, measured by the SF12, an effect which was intensified amongst those who sought treatment. Halder et al emphasised the confounding effect of the psychological state, and suggested that some of the association between IBS/dyspepsia and HRQoL can be explained by psychological factors.450 Gastrointestinal symptoms in the elderly were found to be common in a study in Minnesota, with chronic constipation and chronic diarrhoea having prevalences of 24% and 14%, respectively. Faecal incontinence more than once a week was reported in 3.7%. IBS was estimated from reported symptoms to be a condition for 10.9%. Only 23% had seen a physician during the previous year, and attendance did not correlate well with symptom reporting.53
Borgaonkar and Irvine’s review of HRQoL measures for GI diseases summarised research into the impact of chronic GI disorders on the quality of life of patients.447 HRQoL measures can be global, generic or disease-specific. Disease-specific tools have been developed to measure HRQoL for patients in each of the disease groupings below.
-
Symptoms of GORD occur in about 40% of adults each month, and in 7% daily. Symptoms such as heartburn, regurgitation, and chest pain substantially impair HRQoL and over half of patients require treatment. Patients with GORD were reported to feel as seriously affected as patients with cardiovascular disease, with SF36 physical functioning scores worse than for patients with acute myocardial infarction, and social function scores lower than for patients with congestive heart failure.
-
Dyspepsia occurs in 25% of the general population, with patients reporting considerable anxiety, abdominal pain, interruption of daily activities, and decreased sexual drive.
-
Irritable bowel syndrome is a commonly experienced disorder, with a prevalence of up to 22%. Sufferers report abdominal pain, altered bowel habit, and disturbed sensory and motor function, as well as symptoms elsewhere in the body—back pain, headache, dyspareunia, urinary symptoms, and sleep disturbances. People with IBS have significantly poorer SF36 scores than healthy controls, and patients have difficulty travelling, playing sports, and attending social events. Sufferers take time off work and finish their working lives at a young age.
-
Patients with IBD have been shown to have impaired HRQoL compared with healthy controls in physical, emotional, and social function. Family members and clinicians tend to underestimate the effects on patients compared with self reported health status. The most common problems reported are loose or frequent stools, abdominal pain, worries about disease flares, cancer or the need for surgery, and social restrictions. Eighty per cent of sufferers can maintain employment.
-
Anorectal disorders affect 4% of the population. Patients with anal fissure, constipation, or incontinence have all been reported to record depressed HRQoL life scores.
-
GI cancers account for 20% of all newly diagnosed cancers. Many do not respond to treatment and require palliative care. Patients experience side effects of treatment such as nausea, vomiting, pain, and fatigue, in addition to the symptoms directly caused by the cancer.
-
Patients with hepatitis C were found to record lower SF36 scores than those with hepatitis B across the dimensions of social functioning, physical role limitation, and energy and fatigue, although both groups displayed lower scores than healthy controls.
Overall the burden of GI disease on HRQoL in the general population is not well described, although there are efforts to assess impact in some conditions in studies carried out in various locations. Standardised measures for specific diseases are being developed and validated, which will help to understand and describe the burden and assess treatments and models of care.
3.5 Geographical variation
Peptic ulcer
The incidence of peptic ulcer has been higher in Scotland and in the north of England than further south,66,92 to some extent because of a higher prevalence of the Helicobacter pylori infection in the north.451 In primary care, the prevalence of peptic ulcer has also been reported as two to three times higher in the north of England than in the south.71
Gastrointestinal haemorrhage
The incidence of upper gastrointestinal haemorrhage is higher in Scotland and in the north of England than further south. High incidence rates of upper gastrointestinal haemorrhage have been reported in the west of Scotland (172 per 100 000 in 1992/93),92 and Aberdeen (117 per 100 000),90 compared with the lower rates of 107 for Trent, 102 for the West Midlands, 99 for South West Thames and 91 for North West Thames.91
Inflammatory bowel disease
Regional studies of the incidence of Crohn’s disease in the UK show little systematic geographical variation (table 3.2.2). However, the highest incidence rates for ulcerative colitis have been reported in northern regions such as north east Scotland,134 and north Tees.135,136 The incidence of juvenile onset Crohn’s disease has been reported as 50% higher (p<0.001) in northern Scotland than in southern Scotland during 1981–95, although no significant difference was found for ulcerative colitis.452
Alcoholic liver disease
There seems to be a substantially higher incidence of alcoholic liver disease in Scotland than in England. For example, in 1999–2000 the hospital admission rate for alcoholic liver disease in Scotland, 75.2 per 100 000 population,215 was about 2.5 times higher than the corresponding rate in England during the four year period, 1999–2000 to 2001–02, 31.4 per 100 000.453
Hepatitis B and C infection
Reported diagnoses of hepatitis B and C infections have been shown to vary geographically throughout the UK (fig 3.2.4). In particular, the incidence of both infections since the early 1990s has been highest in Scotland, with rates about four times higher than in the rest of the UK. The lowest rates of reported hepatitis B infections were in Wales, and the lowest rates for hepatitis C were in Northern Ireland.229
Primary biliary cirrhosis
Some of the highest prevalence rates for primary biliary cirrhosis in the world have been reported for northern England: 34.5 per 100 000 population,238 and 24 per 100 000.243 Relatively high rates of 20 and 9 per 100 000 have been reported for south Wales,244 and the west of Scotland.242
Acute pancreatitis
Reported incidence rates for acute pancreatitis, which is sometimes associated with heavy alcohol consumption, are normally substantially higher in Scotland,287,305,306 than in England.285,288,303,304
Gastrointestinal cancers
Figure 3.5.1 shows incidence rates among men and women, respectively, for the main types of gastrointestinal cancer in England, Scotland, Wales, and Northern Ireland during the period 1991–2002. Among both men and women, the incidence of colorectal cancer is lowest in England, oesophageal cancer is most common in Scotland, gastric cancer is most common in Wales among men, and pancreatic cancer shows little cross-national variation in incidence among men, but a substantially reduced incidence rate in Northern Ireland among women.
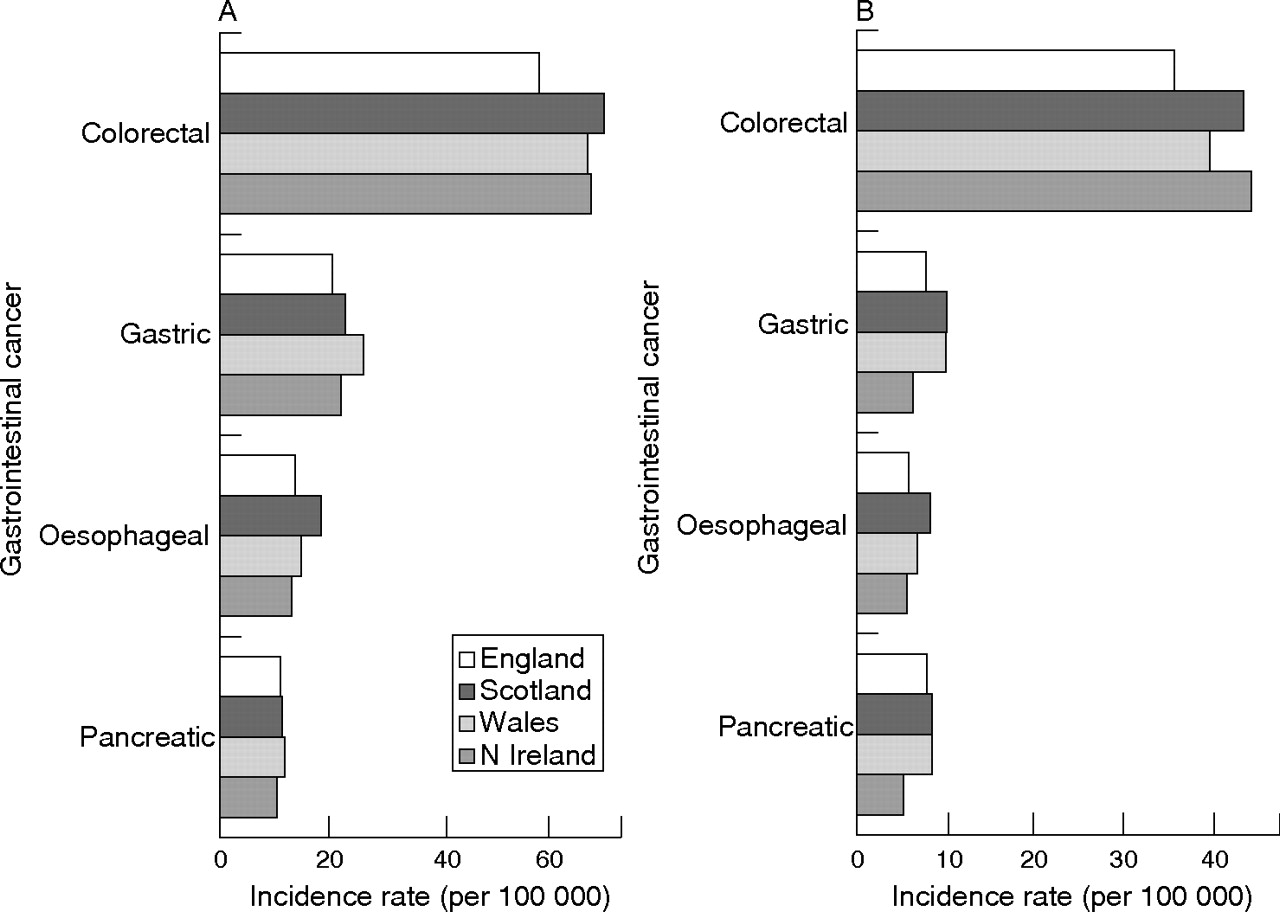
Standardised incidence rates (per 100 000 population) for colorectal, gastric, oesophageal, and pancreatic cancers in England, Scotland, Wales, and Northern Ireland, for the period 1993–2001. (A) For men; (B) for women. Notes: Incidence rates are directly standardised to the standard European population. Sources: England: National Cancer Intelligence Centre, Office for National Statistics; Scotland: Information and Statistics Division, NHS in Scotland; Wales: Welsh Cancer Surveillance and Intelligence unit; Northern Ireland: Northern Ireland Cancer Registry.215,454–456
For colorectal cancer, there is evidence of a north-south gradient in incidence among men in Scotland, with the highest incidence rates in the Shetlands, Highlands, the Grampian region, and the north of Scotland, but less of a geographical trend for women (fig 3.5.2). In Wales there is little geographical pattern in the incidence of colorectal cancer in either men or women (fig 3.5.3). Importantly, the incidence rates in Scotland and Wales are standardised using different standard populations, so no direct comparison of rates can be made across countries.

Incidence rates for colorectal cancer among men and women in different regions of Scotland, 1992–2001. Incidence rates are directly standardised to the standard European population. Source: Information and Statistics Division, NHS in Scotland.215

Incidence rates for colorectal cancer among men and women in different Welsh unitary authorities, 1992–2001. Incidence rates are directly standardised using the Welsh population. Source: Welsh Cancer Surveillance and Intelligence unit.455
Figure 3.5.4 shows incidence rates for the main types of gastrointestinal cancer in different regions of England during the calendar year 2001. For gastric cancer, there is a clear north-south gradient, with incidence highest in the north and lowest in the south. For colorectal cancer, incidence among men is lowest in London and the south east and highest in the north and the south west, while for women there appears to be no clear pattern. Similarly for oesophageal and pancreatic cancers, no clear pattern is evident. Mortality to incidence ratios for each of the main types of gastrointestinal cancer also show little geographical pattern in England (fig 3.5.5).

Incidence rates (per 100 000 population) for colorectal, oesophageal, gastric, and pancreatic cancers in different regions of England, 2001. (A) For men; (B) for women. Source: England: National Cancer Intelligence Centre.454

Mortality: Incidence ratios for colorectal, oesophageal, gastric, and pancreatic cancers in different regions of England, 2001. (A) For men; (B) for women. Source: England: National Cancer Intelligence Centre, Office for National Statistics.
For each of the main types of gastrointestinal cancer, table 3.5.1 shows which Welsh unitary authorities have significantly increased or reduced incidence rates relative to the rest of Wales. Unlike England, there is no systematic geographical pattern in the incidence of any of the main gastrointestinal cancers.
Table 3.5.1 Significantly increased and reduced risks of gastrointestinal cancers among men and women resident in Welsh unitary authorities, 1992–2001
3.6 Socioeconomic factors
Dyspepsia
There is little evidence of an association between dyspepsia and social class.457 A historical study found a similar incidence of dyspepsia in private practice and in a dispensary in London around 1800,458 and a recent study in England and Scotland reported that symptom prevalence was unrelated to social class, but that social class affected consultation behaviour, rising from 17% in social class I to 29% in social class IV.38
Helicobacter pylori infection and peptic ulcer
There is a well recognised association between Helicobacter pylori infection, socioeconomic group,459 and childhood living conditions,460 which has persisted over time. For example, a recent study of [13C]urea breath testing for Helicobacter pylori infection among children in Glasgow, reported a significantly higher prevalence of 34% among children classified with the least affluent Carstairs’ deprivation categories, compared with 16% among the most affluent categories, and 22% among intermediate groups.461
The incidence of peptic ulcer is strongly associated with lower social class or socioeconomic conditions,147,462,463 largely because of the higher prevalence of the Helicobacter pylori infection among people from lower socioeconomic backgrounds. However, gastric ulcers have been associated with manual social classes, and duodenal ulcers with non-manual classes.464
Gastrointestinal haemorrhage
Gastrointestinal haemorrhage is also strongly related to social class, especially as the most common underlying cause of upper gastrointestinal haemorrhage is peptic ulcer. A recent study of the west of Scotland reported that the incidence of upper gastrointestinal haemorrhage was higher in areas of greater social deprivation: it was 2.2 times higher in the least affluent quarter than in the most affluent quarter.92
Inflammatory bowel disease
Inflammatory bowel disease is not thought to be related to social class or poverty. Studies of British national birth cohorts have found no association with social class for either Crohn’s disease or ulcerative colitis.147,465 In Scotland, though, the incidence of juvenile onset Crohn’s disease has been reported as significantly higher in areas of most affluence from 1981 to 1995, although no association was found for ulcerative colitis.452
Irritable bowel syndrome (IBS)
Some studies have reported of an increased prevalence of IBS in higher social classes, which has been considered as consistent with an allergic aetiology for IBS. These include studies in England466 and Australia.467 However, other British studies have reported of no significant association between IBS and social class,147,468 and a Danish study also reported no association for incidence or prevalence of IBS.166 Some studies,166,469,470 although not others,157,471,472 have reported that psychiatric illness or psychological factors may be of greater importance for IBS than socioeconomic and lifestyle factors.
Coeliac disease
There is not thought to be a strong association between coeliac disease and social class or poverty. One British study reported of a non-significant tendency towards a higher prevalence among higher socioeconomic groups.186
Diverticular disease
Socioeconomic factors are thought to influence the incidence of diverticular disease of the intestine. A Scottish study reported that diverticular disease was more common in lower than in higher income groups. It is likely that higher income groups are more aware of the importance of dietary fibre and more able to afford protective foods such as fresh fruit and vegetables.473
Liver cirrhosis
A recent study reported that social class is a risk factor for alcohol related mortality, including liver cirrhosis, with men in manual occupations significantly more likely than professional men to die of alcohol related causes. Alcohol seems to be similar to other psychoactive substances in that problem use is linked to social structural factors such as poverty, disadvantage, and social class.474 Another recent study reported that social class differentials in mortality from liver cirrhosis increased from 1961 to 1981 in England and Wales and in Scotland.475
Hepatitis B and C infections
Both hepatitis B and C are linked to deprivation and poverty. For example, a study of routine neonatal screening in Scotland found the highest prevalence of hepatitis C infections in high deprivation areas, particularly the most deprived areas in Greater Glasgow476; and a USA study reported of a strong association between both hepatitis B and C with deprivation, that was largely related to the impact of poverty on the spread of the two viruses.477
Acute pancreatitis
The incidence of acute pancreatitis is often much higher in areas of higher alcohol consumption and lower affluence—for example, in Scotland compared with the south of England. However, one prominent British study found no association between social class and the incidence of acute pancreatitis in the Nottingham region, but instead found a large excess for people resident in areas with “particularly hard drinking water”.286
Gastrointestinal cancers
The incidence of gastric cancer, in particular, and cancer of the oesophagus is highest in deprived or poor areas. In Scotland from 1991 to 1995, for example, there was a strong social gradient for gastric and oesophageal cancers, with the highest incidence in areas having the highest Carstairs’ deprivation scores, and the lowest incidence found in areas that were the most affluent (fig 3.6.1). Socioeconomic variation in gastric cancer incidence occurs to some extent because of the association between Helicobacter pylori infection and poverty. However, there were no significant associations between deprivation and incidence of colorectal and pancreatic cancers; although colorectal cancer incidence appears to be highest in the most affluent areas.
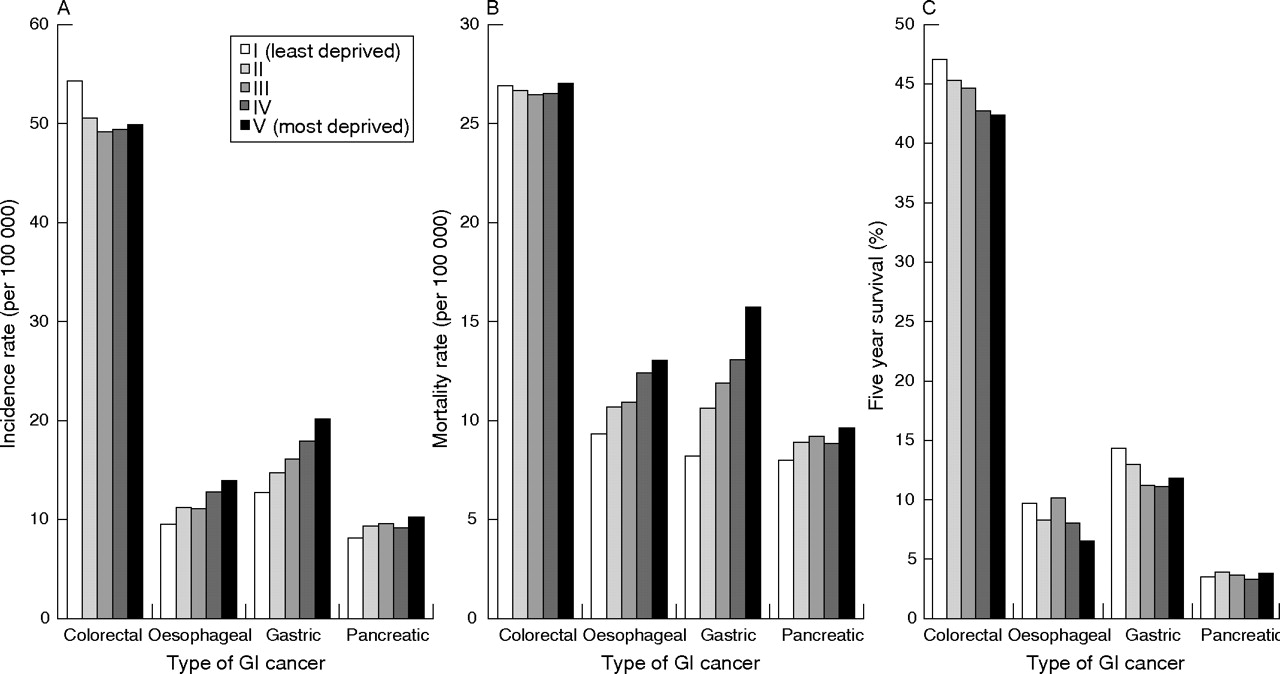
Standardised incidence and mortality rates (per 100 000 population), and five year survival, for colorectal, oesophageal, gastric, and pancreatic cancer shown for Carstairs deprivation categories in Scotland: cases diagnosed between 1991 and 1995. (A) Incidence; (B) mortality; (C) five year survival. Notes: Incidence and mortality rates are standardised using the European population. Incidence and mortality rates for oesophageal and gastric cancers are strongly associated with deprivation (both p<0.001), but those for colorectal or pancreatic cancers are not. Five year survival for colorectal (p<0.01), oesophageal (p = 0.01), and gastric (p = 0.04) cancers are all associated with deprivation, but that for pancreatic cancers is not. Carstairs deprivation categories are measured in quintiles. Source: Information and Statistics Division, NHS in Scotland.215
In England and Wales, use of the ONS longitudinal Study from 1976 to 1990 showed significantly higher incidence of gastric cancers among lower social groups, no social inequalities in incidence of pancreatic cancer, and a significantly higher incidence of colorectal cancer among women but not among men in advantaged social groups.478 Colorectal cancer has similarly been associated with professional or managerial occupations in another British study,464 and colon cancer with sedentary occupations in Sweden.479
Population based mortality in Scotland shows similar patterns to those for incidence, although mortality from colorectal cancer in the most affluent areas is comparable to that in the rest of the population (fig 3.6.1). Five year survival rates in Scotland are positively and significantly correlated with affluence for colorectal cancer, in particular, and also for gastric and oesophageal cancer. However, for pancreatic cancers, which have the poorest prognosis, there is much less scope for socioeconomic variation in survival.
In England, inequalities in survival for colorectal cancer have been attributed to earlier surgical resection among people from more affluent backgrounds, reflecting inequalities in access to treatment,480 while others have reported lower uptake of screening among people from more deprived areas.481,482 For details of the impact of socioeconomic and demographic factors on consultations in primary care for diseases of the digestive system, see section 4.3.2.
3.7 Costs to society
Costs to the NHS of GI disease are reported in section 4.5 below. In addition to health services costs, however, GI disease imposes a considerable burden on the other parts of the UK economy, as well as to patients and their families.
It was not possible to undertake a study of the full burden of illness within the time and financial constraints of this review. However, in 1996 the British Society for Gastroenterology commissioned the Unit for Policy Research in Science and Medicine (PRISM) of the Wellcome Trust to undertake a study to estimate the burden of GI disease in the UK.483 The following estimates are based on that report.
One major element of burden is the years of working life lost by those who die of GI diseases before reaching retirement age. The PRISM study estimated that in 1997 approximately 147 400 person years were lost (from age of death (if 20+) to 65) from GI diseases in both men and women. They reported that “… the burden of gastrointestinal disease in terms of premature death has been approximately constant in recent years”. On the assumption that this burden has remained constant since 1997 and applying their valuation method updated with current average earnings, the estimated cost of early death by GI disease in 2004 is £3230m.
A second major element of the burden of GI disease is the lost productivity due to long term sickness absences from work. The PRISM study estimated that GI disease causes 46 680 person years of lost productivity or roughly 1.7% of long term sickness absence in the UK. Applying their valuation method updated with current average earnings produces an estimated value of lost productivity in 2004 of £1050m.
With respect to short term sickness absence, the PRISM study crudely estimated that one fifth of all short term sickness absences were due to GI diseases. Updating their estimate with current earnings produces a value of lost productivity estimate of £2900m.
On this basis, the total estimated cost to the British economy in 2004 is thus £7180m. Although this figure may be crude, it identifies an order of magnitude which clearly indicates that GI morbidity and mortality impose major costs on the British economy.
In addition to costs for the economy, GI diseases impose considerable burden on individual patients and their families. This includes travel and other costs incurred in receiving treatment and the cost of over the counter drugs, which are not included in the NHS costs reported in section 4.5.
4 CURRENT SERVICE PROVISION IN THE UK
4.0 Methods and data limitations
The main methods used for the activity analysis in this chapter involved using routine data sources in the UK to provide information on hospital activity and costs. The main source used for hospital inpatient activity was hospital episode statistics (HES) in England, produced by the Department of Health. Record linkage allows hospital activity to be determined for the numbers of people receiving inpatient care, as well as the numbers of episodes of care. Linked hospital episode data were provided by the Unit of Health-Care Epidemiology, University of Oxford.484
Hospital activity for surgical procedures was also obtained from hospital episode statistics. However, because outpatient activity data are not yet available for the UK, data were obtained for outpatients from the USA.
For activity in primary care, the most recent comprehensive study of consultation patterns in primary care is the fourth national morbidity study in England and Wales in 1991–92.485 This comprised a representative national sample of 60 general practices, covering just over half a million registered patients or 1% of the population of England and Wales. This study followed the third national morbidity survey in 1981–82.486
Some of the main data limitations for investigating activity include concerns about the accuracy of routine hospital episode statistics,8,9,10,11 as well as increasing doubts that the finished consultant episode is still a valid measure in a health service where changing roles and teamwork are increasingly becoming the norm.11,487,488
A limitation of the investigation of primary care activity is that the latest comprehensive and freely available study of consultation patterns in primary care in England and Wales is the fourth national morbidity study which covers the period 1991–92.
The literature review described in section 5.0.1 has also contributed to some sections in this chapter. Workforce data have been collected by an annual census of consultant gastroenterologists taken on 30 September each year. These data are cross checked with the Royal College of Physicians annual census data (coordinated to 30 September each year). Advertisements in the BMJ and consultant gastroenterology advisory appointment committees are constantly monitored. Specialist registrars also complete an annual census, with data being cross checked against information from the consultant census, Joint Committee for Higher Medical Training, and by monitoring movements of the specialist registrar workforce as they occur. Data on nurses and non-consultant career grade (NCCG) doctors are collected from the consultant census, from the RCN directory, and from an unpublished survey of nurses.
4.1 Organisation
The current provision of services for patients with gastrointestinal disorders has been summarised in a joint report from the British Society of Gastroenterology and Royal College of Physicians in 2003.489 Common problems include indigestion, reflux, irritable bowel syndrome, and constipation. Many of these problems can be diagnosed and treated by the patient’s family practitioner. Those with worrying or persistent symptoms will usually be referred to a consultant gastroenterologist in outpatients, to identify or exclude organic disease and receive advice on treatment. Investigations will often include blood tests, endoscopy, and imaging. If problems arise suddenly or appear very serious, urgent inpatient assessment and treatment may be required. Such problems include bleeding from peptic ulcer, jaundice, acute liver disease, and severe exacerbations of colitis and Crohn’s disease. In hospitals many GI disorders require a team approach involving physicians, surgeons, radiologists, pathologists, specialist and non-specialist nurses, dieticians, nutritionists, physiotherapists, clinical scientists, physiologists, speech and language therapists, hypnotherapists, and psychologists. Some problems will require referral to a tertiary centre where a specific concentration of expertise is required to manage serious or rare disorders, both medically and surgically.
Conventional services for patients with gastrointestinal disorders reflect the traditional division between the primary and secondary care sectors. General practitioners usually have direct access to laboratory, radiological, and endoscopic investigations, but are required to refer patients to consultant colleagues in hospitals when a specialist opinion or care is needed. Not all hospitals provide a full range of diagnostic and treatment facilities and tertiary referral to a subregional or regional hospital is often necessary for complex problems.
The management of many gastroenterological conditions has been reviewed in evidence based guidelines produced by the British Society of Gastroenterology (table 4.1.1), National Institute for Health and Clinical Excellence (NICE; table 4.1.2), and Scottish Intercollegiate Guidelines Network (SIGN; table 4.1.3). This document will not examine the clinical management of individual disorders except in the context of the location and nature of the services required.
Table 4.1.1 BSG published guidelines, including work-in-progress
Table 4.1.2 NICE guidelines relating to GI disorders
Table 4.1.3 SIGN guidelines relating to GI disorders
4.2 Workforce
Most patients with persistent symptoms suggestive of gastrointestinal disease will be managed by a team led by a gastroenterologist. The Royal College of Physicians has set out a description of the specialty490 and defined the workload of a consultant-led gastroenterology team. It is recommended that a consultant-led team should look after no more than 20–25 inpatients at any one time, the majority being admitted on emergency take days. In outpatients a consultant physician in gastroenterology, working alone, in a new patient clinic, should see 6–8 patients; each allotted 20–30 minutes. When reviewed, 12–15 patients should be seen in a single session.
The Royal College of Physicians recommends that 65–74 consultant programmed activity sessions are required to serve a population of 250 000, which indicates a need for about six consultants for such a population. This takes into account the need to allow for education and training, audit, and service management. For diagnostic upper gastrointestinal endoscopy or flexible sigmoidoscopy, a maximum of 10–12 procedures should be carried out in a single session, allowing 15–20 minutes for each procedure. Therapeutic procedures will take at least twice as long, and diagnostic and therapeutic colonoscopy will usually take 30–40 minutes for each procedure.
The workforce in gastroenterology has expanded substantially over the past few years. The robust data on consultant gastroenterologist numbers show a rise from 335 to 725 in England and Wales (fig 4.2.1), with an average expansion of 6.3% a year over the whole of that period (fig 4.2.2). At present growth rates it will take 13 years to reach the recommended six consultants per 250 000 population. The total number of academic gastroenterologists is 118 (England 104, Scotland 10, Wales 3, and Northern Ireland 1). Currently, in excess of 400 stoma care nurses are listed in the RCN directory and, from a recent unpublished survey, there are about 100 IBD nurses in the UK. No data are available on workforce numbers in the allied professions that support the care of patients with GI disorders, but there are concerns that expansion has not matched that in medicine and nursing.

Numbers of consultant gastroenterologists in England and Wales against time.
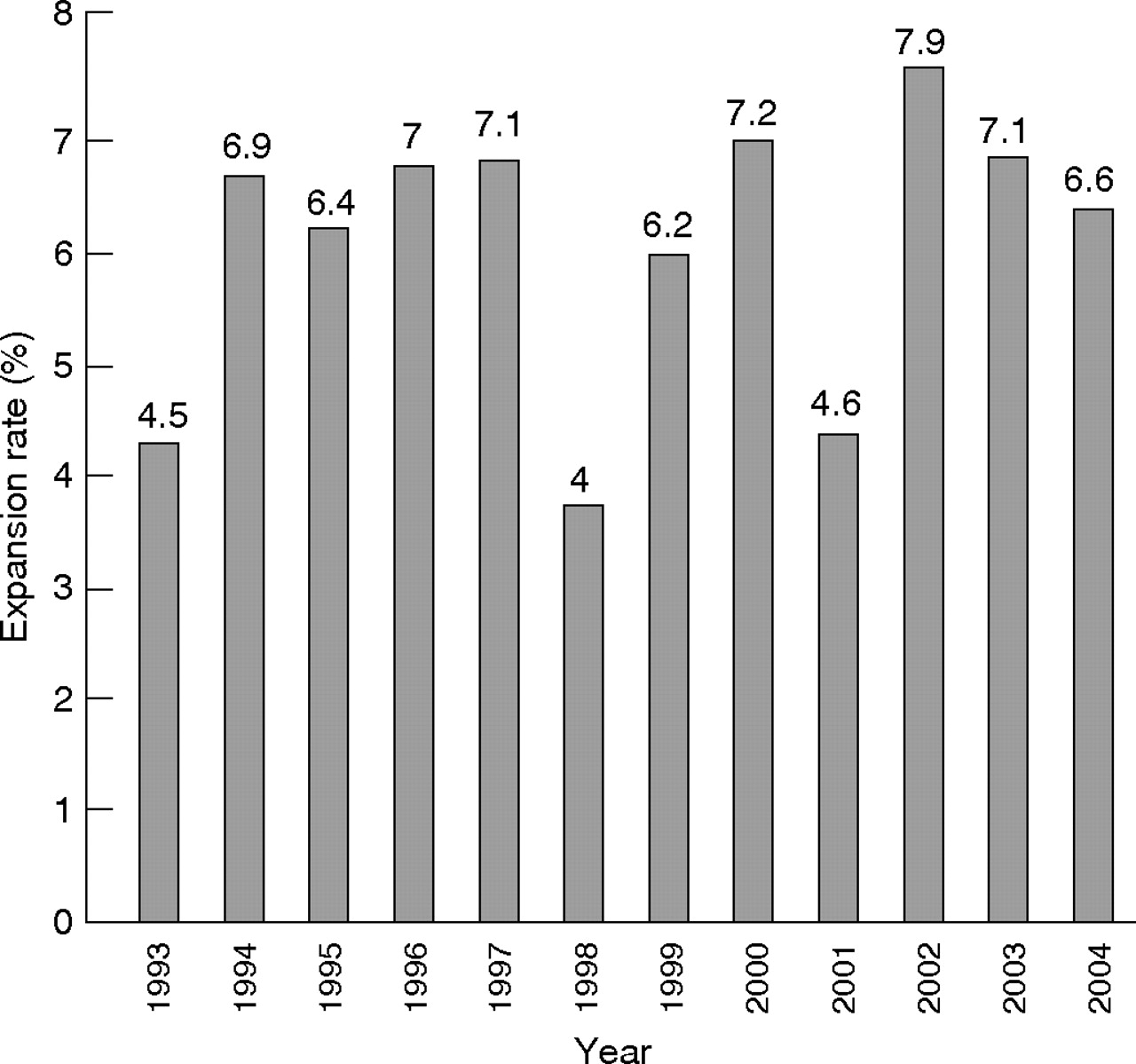
Consultant gastroenterologists expansion rates (England and Wales).
Expansion in consultant numbers has been greater in the past five years, averaging 7% in England with similar expansion in Wales and Northern Ireland and slightly less in Scotland (table 4.2.1). Thus the numbers of gastroenterology consultants in the UK total 826 (as of 30 September 2004) (table 4.2.2).
Table 4.2.1 Annual expansion (%) of consultants in different parts of the UK by year
Table 4.2.2 Numbers of consultants in different parts of the UK by year
This consultant workforce is supported by at least 418 associate specialists (371 England, 18 Wales, 16 Scotland, 13 Northern Ireland) and 312 nurses undertaking duties that a few years ago would have been deemed the province of doctors—for example, endoscopy nurses (268 England, 13 Wales, 28 Scotland, 3 Northern Ireland). Neither of the groups is evenly distributed through regions or principalities, varying from 3 specialist nurses in Northern Ireland, 6 in Oxford to 32 in Trent and 35 in North Thames (East). For NCCG doctors this variation ranges from 14 in South Thames (West) to 39 in South Thames (East). The lack of correlation (direct or inverse) between consultant numbers, specialist nurse, and NCCG doctors suggests the distribution has developed in an ad hoc fashion rather than by formal planning based on population needs (see table 4.2.3).
Table 4.2.3 Numbers of nurses and associate specialists contributing to gastroenterology service provision in the UK
In addition the specialist registrar trainees provide substantial service work and any reduction in training numbers (as seems likely as the number of consultants plateau at a required level) would need to be replaced by consultants or other workers of similar skill. Five hundred and fifty specialist registrars or equivalent currently have posts in the UK (as of 30 September 2004), though 131 are out of programme or undertaking research so contribute only a proportion of their time to service delivery (table 4.2.4).
Table 4.2.4 SpR/NTN posts in the UK (as of 30 September 2004)
In detailed work reported in Consultant physicians working with patients490 the need for approximately 1950 consultant gastroenterology posts in the UK as a whole (assuming a population of 59.6 million), providing 1665 whole time equivalent posts, was demonstrated to deliver acceptable levels of care. This number allows for a proportion of part time consultants as estimates suggest such work is increasingly popular. Larger numbers may be required with the predicted expansion of the population to 65 million. Typically six to seven will serve a population of 250 000, with extra needed where other duties are fulfilled. These will include specialist training (for example, endoscopy courses), undergraduate teaching, academic and research roles over and above those expected in a district hospital. Each team will require additional support staff such as non-consultant career grade doctors, specialist nurses (with roles in nutrition, endoscopy, inflammatory bowel disease and more technical functions—for example, pH and manometry, videocapsule endoscopy, etc) and the service time provided by specialist registrars. No clear information exists on likely need but one could imagine a team consisting of six whole time equivalent consultants, one to two whole time equivalent non-consultant career grade doctors, two endoscopy nurses, and two to three specialist nurses (each providing additional help with IBD, pH, etc) and one to two specialist registrars being trained in gastroenterology and general medicine.
The MINuET study491 has concluded that more diagnostic endoscopies could be undertaken by nurses. The implications of this are that at least one whole time equivalent specialist nurse, trained in endoscopy, would be required in each medium sized district general hospital. In practice, it is unlikely that a nurse endoscopist would wish only to undertake endoscopies and it is more probable that other specialist nurse roles would be included in the job description. On this basis it is predicted that two whole time equivalent specialist nurses would be required for each hospital. A survey of 196 endoscopy units, registered with the Joint Advisory Group for Gastrointestinal Endoscopy in 2004, identified 149 nurse endoscopists in post in 96 units (64% of the 150 units that responded).492 On this basis it can be predicted that approximately 200 nurse endoscopists will need to be found and trained in the UK, if the majority of diagnostic procedures are to be undertaken by nurses.
4.3 Activity
4.3.1 Primary care
Routinely collected clinical data are coded and analysed using the International Classification of Diseases (ICD) for diagnosis and Office for Population Censuses and Surveys Classification (OPCS) for surgical operations and procedures.
During 1991–92, 78% of people consulted a general practice on at least one occasion. Table 4.3.1 shows the prevalence rate or percentage of people who consulted for the major disease groupings (ICD-9 chapters). Of the different gastrointestinal diseases, 8.7% of people consulted for diseases of the digestive system, 4.1% consulted for intestinal infectious diseases, 0.1% consulted for malignant neoplasms of the digestive system, and 0.04% for viral hepatitis (table 4.3.1).
Table 4.3.1 Rates per 10 000 population for patients consulting general practice, and for the total consultation rate, for the different ICD-9 chapters, England and Wales, 1991–1992
Diseases of the digestive system formed one of the leading ICD chapters as the cause of people consulting their GP, following respiratory diseases (30.7% of all people), diseases of the nervous system (17.3%), musculoskeletal diseases (15.2%), diseases of the skin and subcutaneous tissue (14.6%), infectious diseases (14.0%), injury and poisoning (13.9%), genitourinary diseases (11.3%), and diseases of the circulatory system (9.3%).
The percentage of patients consulting general practice for diseases of the digestive system rose by one fifth from 7.2% of people in 1981–82 to 8.7% in 1991–92 (fig 4.3.1), which was closer to the 8.2% and 10.0% of people consulting for diseases for the digestive system in the historical national morbidity surveys in 1955–56 and 1971–72, respectively.12 The proportion of people consulting for most other ICD-9 chapters also increased, although there were reductions for infectious diseases, mental disorders, and ill-defined diseases.

Percentage of patients consulting general practice for the different ICD-9 disease chapters in England and Wales, 1981–82 and 1991–92; a comparison over time between the last two national morbidity surveys. Source: McCormick et al, 1995.485
The total consultation rate for gastrointestinal diseases was 2083 per 10 000 population; or just over one consultation for every five people in the general population (table 4.3.2). These comprised 1495 consultations per 10 000 for diseases of the digestive system, 517 for intestinal infectious diseases, 54 for malignant neoplasms of the digestive system, nine for benign and other neoplasms of the digestive system, and eight per 10 000 for viral hepatitis.
Table 4.3.2 Consultation rates (per 10 000 population) for patients consulting general practice for gastrointestinal diseases in England and Wales, 1991–1992
Consultation rates per 10 000 population for individual gastrointestinal diseases are also shown in table 4.3.2. The most common causes of consultation were ill-defined intestinal infectious diseases (497 consultations per 10 000 population), disorders of the function of the stomach (224 per 10 000), diseases of the oral cavity, salivary glands and jaws (185), diseases of the oesophagus (169), hernia (104), gastritis and duodenitis (101), and peptic ulcer (90; table 4.3.2).
For people consulting GPs with gastrointestinal diseases, the most common causes of consultation were infectious intestinal diseases (4.0% of people), functional disorders not elsewhere classified (2.1%), disorders of function of stomach (1.5%), diseases of the oesophagus (1.0%), and gastritis and duodenitis (0.7%; fig 4.3.2).

Percentage of patients consulting general practice for the most common gastrointestinal diseases in primary care in England and Wales, 1991–1992 (at least 0.10% of the general population consulting). Source: McCormick et al, 1995.485
Socioeconomic and demographic influences on consultations for diseases of the digestive system in primary care
Consultations for diseases of the digestive system in primary care in 1991–92 show a strong social class gradient, with significantly increased rates of consultation for the manual social classes IV, V, and III manual, and reduced consultation levels for social classes I, II, and among men in the III non-manual class (fig 4.3.3A).
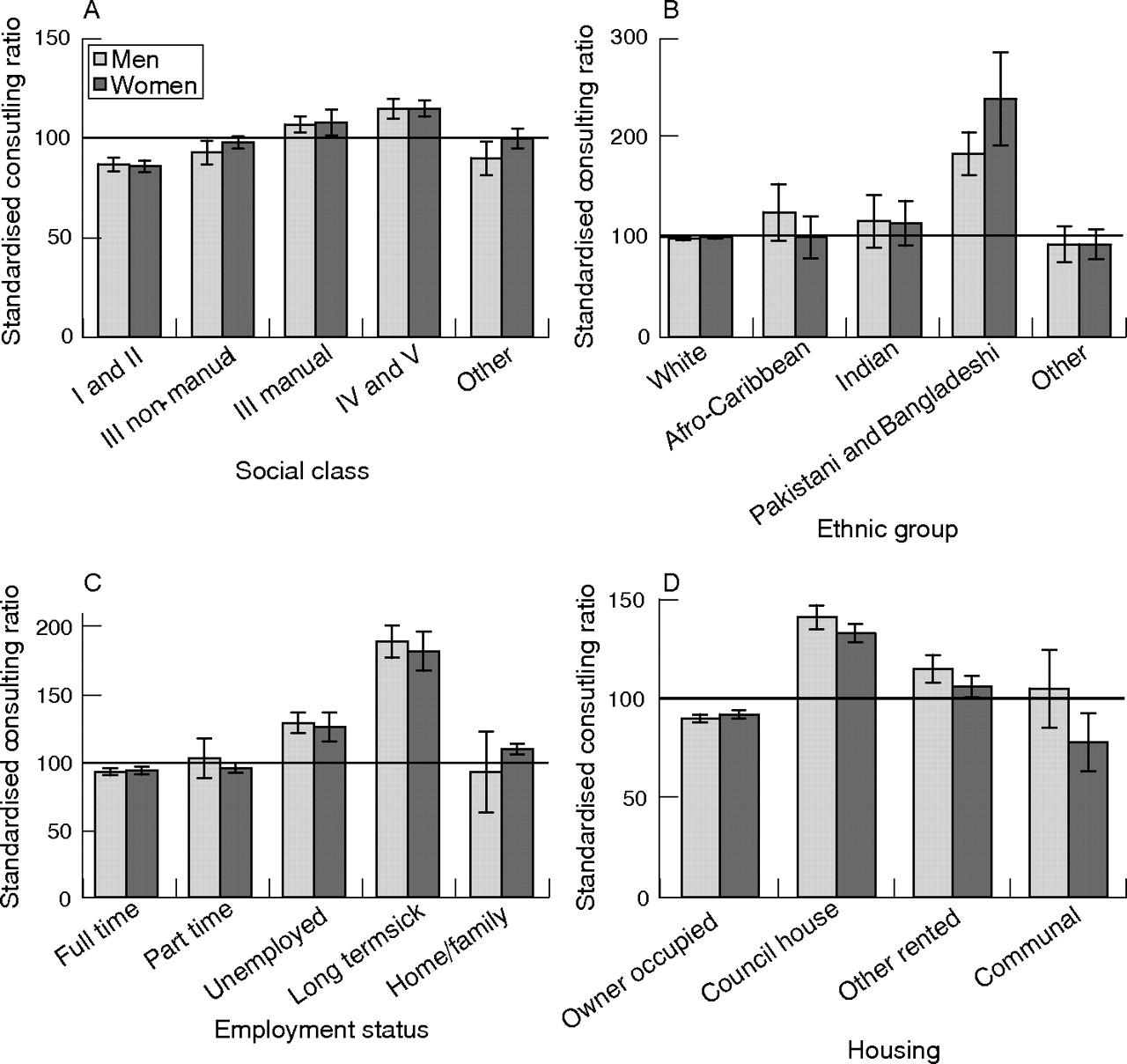
Standardised consulting ratios (general population = 100) for diseases of the digestive system in general practice in England and Wales, 1991–92 according to (A) social class; (B) ethnic group; (C) employment status; (D) housing. Note: Standardised consulting ratio in the general population = 100. Vertical bars represent 95% confidence intervals. Source: McCormick et al, 1995.485
Consultation rates for digestive diseases were greatly increased for Pakistani and Bangladeshi ethnic groups, by 84% among men and 139% among women, but were not significantly increased or reduced for all other classified ethnic groups (fig 4.3.3B).
Consulting was reduced among people in full-time employment, and among women in part-time employment, but was increased among people who were unemployed or who were registered long term sick, and for women who were classified as looking after the home or family (fig 4.3.3C). People living in council housing and other rented accommodation also had increased rates of consultation, while people in owner occupied housing and women in communal accommodation had reduced consultation rates (fig 4.3.3D).
Increased rates of consultation were also reported for men in the Midlands and Wales, widowed or divorced people, and smokers, while people in southern England, people in rural areas of residence, single women, and non-smokers had reduced rates of consultation (fig 4.3.4).

Standardised consulting ratios (general population = 100) for diseases of the digestive system in general practice in England and Wales, 1991–92 according to (A) region of England and Wales; (B) urban or rural residence; (C) marital status; (D) smoking habit in past week. Note: Standardised consulting ratio in the general population = 100. Vertical bars represent 95% confidence intervals. Source: McCormick et al, 1995.485
4.3.2 Inpatients
Out of 39 million finished consultant episodes (FCEs) in England during the four year period 1998–99 to 2001–02, 6.5 million (17%) had a gastrointestinal disease as the principal diagnosis (table 4.3.3); although about 45% of these admissions were day cases and mainly refer to endoscopic assessments. Of these, 5.2 million were for diseases of the digestive system, one million were for malignant neoplasms of the digestive system, 225 820 were for benign and other neoplasms of the digestive system, 160 160 were for intestinal infectious diseases, and 20 232 were for viral hepatitis.
Table 4.3.3 Annual population based hospital admission rates (per 10 000 population) for ICD-10 chapters, based on numbers of finished consultant episodes (FCEs) and on numbers of people admitted in England, 1998–99 to 2001–02
Diseases of the digestive system was the second ICD chapter after neoplasms, and excluding “symptoms, signs, and abnormal findings”, that was the principal diagnosis for most FCEs (table 4.3.3). Using record linkage to identify person based admission rates, as well as episode based rates, diseases of the digestive system was the ICD chapter that was the principal cause for most people being admitted to hospital (4.4 million in England from 1998–99 to 2001–02).484
Figure 4.3.5 shows the percentage of inpatient admissions for each major body system, after deaths from cancer were allocated to their respective body systems—for example, when gastrointestinal cancers were included with diseases of the digestive system, when respiratory cancers were included with diseases of the respiratory system, etc. Then, gastrointestinal diseases were the leading major cause of hospital admission, either as FCEs (6.55 million; 17% of the total) or as people admitted (5.00 million; 17% of the total).

Percentage hospital admissions for major ICD-10 disease groupings in England, 1998–99 to 2001–02 (A) based on the number of finished consultant episodes (FCEs). Source: Department of Health, 2004453; (B) based on the number of people admitted. Sources: Unit of Health-Care Epidemiology, Oxford, 2004.484
In other words, 1 in 39 people were admitted each year with a principal diagnosis of gastrointestinal disease. This compares with 1 in 60 people admitted each year for genitourinary disease, 1 in 63 for circulatory disease, 1 in 76 for accidents and injury, 1 in 81 for respiratory disease, and 1 in 90 for musculoskeletal disorders.
Using the criterion of “any diagnosis” rather than “main diagnosis”, a total of 7.5 million people were admitted with “any diagnosis” of gastrointestinal disease during the four year period (one in 26 people per year), with a corresponding total of 10.0 million FCEs (26% of all FCEs).
Gastrointestinal cancer is the most common cause of hospital admission of all major cancer groupings. It was the principal diagnosis of 23% of all cancer FCEs, followed by lymphatic and haematological cancer (22%) and genitourinary cancer (18%; fig 4.3.6). FCEs for GI cancers mainly comprised colorectal cancer (60%), followed by cancers of the oesophagus (12%), stomach (11%), pancreas (7%), and the liver and intrahepatic ducts (2%).

Percentage hospital admissions, based on number of FCEs, for major groupings of cancer in England, 1998–99 to 2001–02. Sources: Department of Health, 2004.453
The main causes of hospital admission for (non-cancer) diseases of the digestive system include hernia (12% of all FCEs), non-infective gastroenteritis and colitis (9%), cholelithiasis, cholecystitis and other diseases of the gallbladder, and gastritis and duodenitis (7%; fig 4.3.7).

Percentage of hospital admissions, based on number of FCEs, for diseases of the digestive system in England, 1998–99 to 2001–02. Sources: Department of Health, 2004.453
Figure 4.3.8 shows hospital admission rates, based on number of FCEs and on number of people admitted, for some of the most common diseases and conditions in the general population. The number of people admitted for gastrointestinal diseases was more than double that for all types of accident, four times that for ischaemic heart disease, over 10 times that for stroke and pneumonia, and 20–40 times that for diabetes, asthma, and all traffic accidents.

Annual population based hospital admission rates (per 10 000 population) based on numbers of FCEs, and on numbers of people admitted, for gastrointestinal diseases and for other selected diseases and conditions in England, 1998–99 to 2001–02.*Gastrointestinal disease includes diseases of the digestive system, malignant neoplasms of the digestive system, benign and other neoplasms of the digestive system, intestinal infectious diseases, and viral hepatitis. Sources: Department of Health, 2004.453
4.3.3 Outpatients
Currently HES only includes data on admitted patients. In the near future, outpatient data will be available on HES online, but this will not include clinical data.
However, using figures for the USA in 2000, these show that out of an estimated total of 27.4 million outpatient visits for gastrointestinal symptoms, the leading gastrointestinal complaint was abdominal pain, cramps and spasms (12.3 million outpatient visits), followed by diarrhoea (4.06 million), nausea (3.32), vomiting (2.89), dyspepsia (1.82), constipation (1.33), anal or rectal bleeding (1.26), and melaena (1.18).493
The leading physician diagnoses for the same 27.4 million outpatient visits were abdominal pain (5.24 million), gastro-oesophageal reflux disease (4.62 million), gastroenteritis (3.43), gastritis (2.4), haemorrhoids (1.57), irritable bowel syndrome (1.56), non-inguinal hernia (1.54), benign neoplasms of the colon (1.52), malignant colorectal neoplasm (1.49), inguinal hernia (1.24), and diverticulosis of the colon (1.00).
4.3.4 Procedures
Table 4.3.5 shows the total number of surgical procedures undertaken in England in 2000–01 for the different OPCS-4 chapters, as well as the total numbers of “main procedures” during a given episode, and the numbers of day case procedures.
Out of a total of 12.7 million procedures, 1.21 million (9.5%) were performed on the digestive tract and a further 128 886 (1.0%) on other abdominal (principally digestive) organs. Considering main procedures only, 1.03 million out of a total of 6.5 million procedures (16%) were performed on the digestive tract, and a further 97 102 (1.5%) on other abdominal organs (table 4.3.5).
A total of 5.8 million of the 12.7 million procedures (45%) were undertaken as day case admissions, including 59% of the procedures on the digestive tract and 11% of the procedures on the other abdominal organs (table 4.3.5).
Figure 4.3.9 shows the percentage breakdowns of surgical procedures on the digestive tract and other abdominal organs in England in 2000–2001 (A) for all surgical procedures and (B) for the main surgical procedure during the episode. Most procedures were performed as day case admissions for endoscopy examination. The other most common gastrointestinal procedures were excisions of gallbladders (42 013, 3% of all gastrointestinal procedures), emergency excisions of appendices (36 657; 3%), and destruction of haemorrhoids (21 720; 2%; fig 4.3.9).
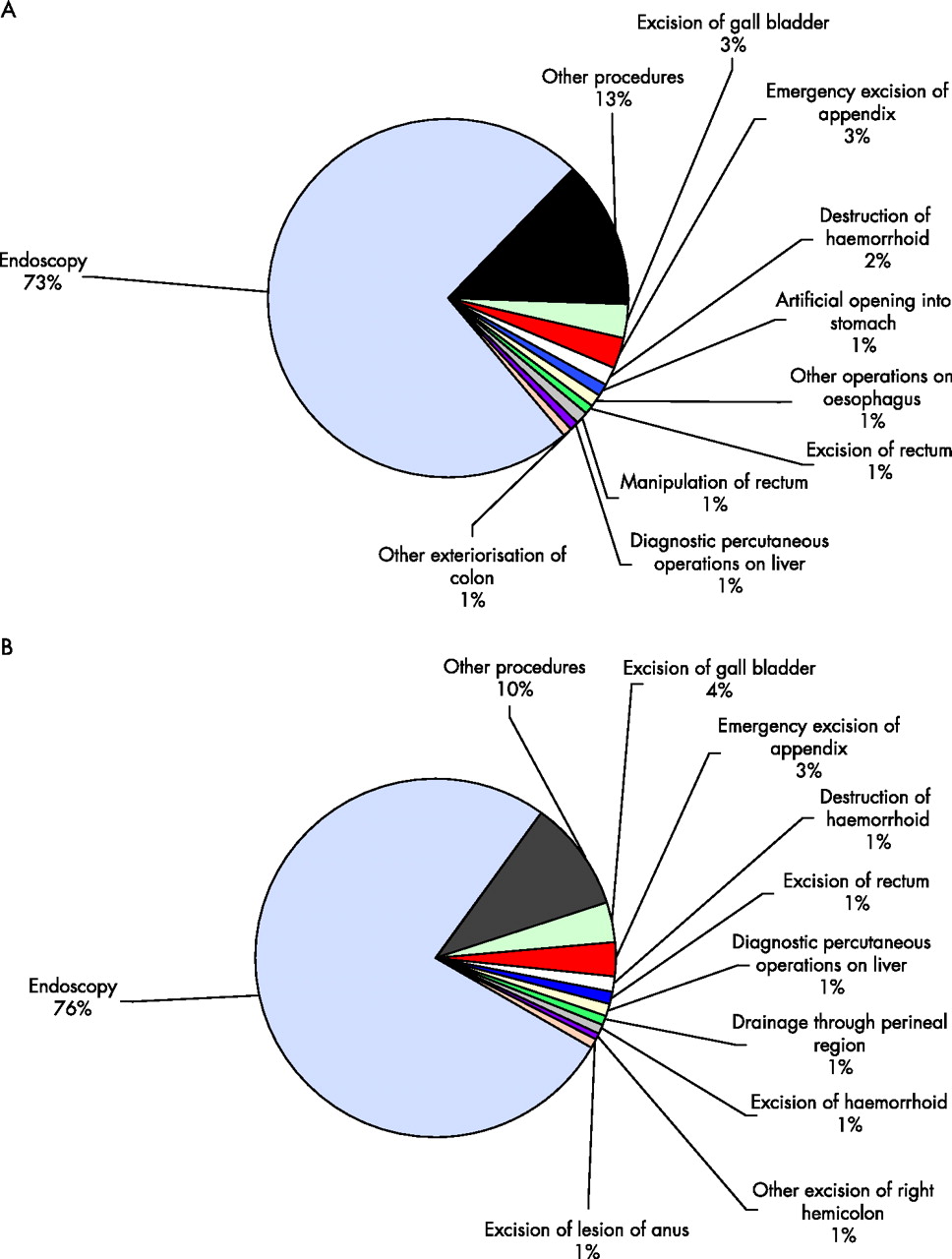
A total of 17.4 million (17 364 212) bed days were associated with the total of 6.51 million main procedures. Of these, 2.6 million (2 629 352; 15.1%) were for procedures on the digestive tract, 1 389 613 on the upper digestive tract, and 1 239 739 on the lower digestive tract. An additional half a million (519 393) bed days were for procedures on the other abdominal organs.
Therefore, a total of 3.15 million bed days (18.1% of the total) were for gastrointestinal procedures, which was second only to procedures on “other bones and joints” (3.17 million) as the heaviest burden on hospital beds (fig 4.3.10).

Total number of bed days for main surgical procedures in England, 2000–2001. Source: Department of Health, 2004.453
Table 4.3.6 shows surgical procedures on the digestive tract with mean waiting times to admission in excess of 90 days in England in 2000–01. Eight of 69 procedures on the upper digestive tract, 10 of 52 procedures on the lower digestive tract, and 7 of 61 procedures on other abdominal organs had waiting times of 90 days or more.
4.4 Voluntary sector patient support groups
Voluntary organisations provide support for patients with coeliac disease, inflammatory bowel disease, irritable bowel syndrome, liver disease, and after bowel surgery. These organisations are listed in Appendix 1. The voluntary sector plays a major part in the care and support of patients with chronic gastrointestinal disorders and has conducted many surveys which document the considerable impact of chronic GI disorders on the physical, mental, social, and financial health of those affected.494–497
4.5 Costs to the NHS
As with non-NHS costs reported in section 3.7, a comprehensive costing of all NHS resources devoted to GI disease was not possible within the time and resource constraints of the present study. Several key cost areas such as GI cancers (recorded under cancer rather than GI disease) are not included. For others, cruder methods were used here than would have been the case in a more detailed costing exercise. Nevertheless the costs below give a general picture of costs in the relevant areas.
Hospital costs
Data on the number of FCEs in England for all HRGs for diseases of the digestive system were obtained from the Royal College of Physicians iLab using Hospital Episode Statistics. Activity data for each HRG were multiplied by the relevant NHS reference cost.498 Table 4.5.1 below shows the total number of emergency, overnight elective and day cases in 2001–02 and the associated costs. Total hospital costs (England only) were £1400m.
Drugs
In 2002, 60 million prescriptions were issued for diseases of the gastrointestinal system (represented by therapeutic group 1 in the British National Formulary). The net ingredient cost of these drugs was £802m, of which £596m was for ulcer healing drugs and £51m for laxatives, which represents 7.9% of the total number of prescriptions issued in the UK and 9.5% of the total UK drug cost.499 These reported costs are solely for the “net ingredient cost” of the drugs and do not include other cost items such as containers or dispensing fees.
Primary care
The Office of Health Economics has estimated the cost of general practitioner consultations in the UK in 2000–01 for diseases of the gastrointestinal system to be £136m. This represents 7.8% of the cost of all GP visits.
These three elements of NHS costs due to GI diseases give a total of under £2400m but it must be emphasised that this understates total NHS costs for the reason given above.
4.6 Problems with existing service provision
4.6.1 Access
Statistical data on actual usage of resources are covered in section 4.3 and 4.5. Many of the underlying problems concerned with rising demand and limited access are examined, providing a more comprehensive reflection than the brief summary given here. Although many studies give a passing mention to problems of access, only three studies were found to cover this topic for GI services in any significant detail. Indeed, as one would expect, there are clear concerns for a range of services including endoscopy,500 outpatient management,501 and open access gastroscopy,502 with specific problems being excessive workload,502 ways to restrict access as a means to control costs,500,502 and the inappropriate use of services.501 It seems that an extensive and systematic study on the problem of access for the delivery of GI services has yet to be carried out.
4.6.2 Inequalities
No significant publications were found on the problems of inequalities in the delivery of GI services. Only one study—a brief, opinion based commentary on the topic of the inverse care law—was found to highlight general issues of inequalities in the health service.503 One likely reason for the lack of reliable evidence is that inequality is a much wider ranging concern, and is generally not confined to specific disciplines of medicine or health care. Readers concerned with this topic are therefore advised to consult other sources for an overview of this problem.
4.6.3 Waiting lists
Five studies were included in this section. Unsurprisingly, a literature review by Dunnill and Pounder504 found that waiting times (whether for an appointment or in the outpatient department) form the bulk of patients’ concerns. Guidelines set out by the Association of Coloproctology of GB and Ireland recommend that surgeons should expect to achieve waiting times of four weeks or less between making a diagnosis of colorectal cancer and the start of treatment.505 But an audit by Duff et al506 carried out in the north west of England found that the median time between referral from the surgeon and the start of radiotherapy was 40 days, while only four patients (6% of the sample) received radiotherapy within 28 days of referral.
For bowel cancer, Flashman et al507 showed that most patients were not referred according to the two week standard set out by the Department of Health (that is, that all patients suspected by their GP of having bowel cancer should be seen by a specialist within two weeks). Clinics did not shorten the overall time to treatment or improve the stage of disease because the time lags before referral and after the outpatient appointment caused major delays. A brief report by Hellier508 outlined the problems with meeting the two week standard in endoscopy clinics, and emphasises that in order to make it a realistic possibility and to avoid distorted referral practices, funding needs to be targeted at GI outpatient and endoscopy facilities.
4.6.4 Patient safety
Several papers have dealt with patient safety for the treatment of GI disease. These can be generally divided into the safety of methods of treatment (such as the use of NSAIDs and complementary medicine) and procedures (for example, endoscopy and surgery). A wide breadth of studies cover various aspects of treatment,509–518 and are generally beyond the scope of this report. However, it is worth noting that the main concerns in this area are focused on ensuring that sufficient evidence and research is carried out to assess the safety of new drugs and treatments for GI disease,509,510,515 which include over-the-counter drugs,513 unlicensed and off-label drugs,511 prescription of NSAIDs,512,514,516 complementary medicines used by children,518 and endoscopic therapy for acute non-variceal upper GI haemorrhage.517
As far as the safety of procedures is concerned, most studies have generally found that upper GI endoscopies are safe regardless of age and where they are performed.519–522 However, some caveats remain in the area of how the service is delivered, including a restriction of upper GI endoscopy in elderly patients (85 years and over) to cases of bleeding (overt and suspected) and anaemia in order to reduce costs.522 There are also suggestions that simple diagnostic endoscopies can be performed safely in the primary care setting, leaving secondary care units to concentrate on those patients requiring sedation, who are acutely ill, and who require therapeutic procedures519—problems on location of care are covered in greater detail in section 5. Despite these positive findings, endoscopy does carry some risk. In a study by Quine et al,521 out of 13 036 patients undergoing endoscopic endoscopy without any therapeutic intervention, there were seven deaths, and this was expected to have been an underestimate owing to the reliance on self reporting by doctors. Another study520 reported significant complication and death from diagnostic oesophageal gastroduodenoscopy as 1 in 1000 and 1 in 10 000 procedures respectively, but that patients’ sex, age, or preference for sedation or endoscopist did not affect the morbidity rate.
A report in 2004 from the National Confidential Enquiry into Patient Outcome and Death523 identified a low mortality from therapeutic endoscopy, with the exception of percutaneous endoscopic gastroscopy (PEG), which had a mortality of 6%. The report made many recommendations to improve the structure and process of therapeutic endoscopy, including the importance of careful selection for PEG insertion and ERCP, and the importance of endoscopy for gastrointestinal haemorrhage being undertaken only by experienced endoscopists.
More complications can be found for GI related surgery, especially for older patients.524,525 For malignant bowel obstruction, it is suggested that patients should only undergo surgery if their life expectancy is at least two months,526 but endoscopic enteral stents for patients with this disease is a safe and cost effective alternative.527
4.6.5 Information to patients and practitioners
There seems to be widespread encouragement for initiatives aimed at improving the information flow between patients and practitioners.511,513,528–534 Key issues include the need for nurses and doctors to give relevant and holistic information to patients undergoing gastroscopy at the right time532; information leaflets on drugs, illnesses, and diet511,513,529–531; and the need for practitioners to be more alert and vigilant in identifying the need to provide information.528,533,534
Studies also highlight specific problems due to poor communication. Sewitch et al found that a poor or ineffectual conversation between patients and practitioners increased the risk of intentional non-adherence to IBD drugs by patients.535 It is also interesting to note that in a survey of around 800 patients undergoing colorectal cancer screening in the USA by Greiner et al,536 61% felt they had inadequate or no time to discuss colorectal cancer with their physician. It was suggested that new and creative methods are needed to satisfy patients’ information needs and encourage discussion. In the UK, a study in 1997537 highlighted that the opportunity to educate and inform patients about IBD in outpatient clinics is often wasted, as practitioners neglect to mention key information sources such as the National Association for Colitis and Crohn’s Disease, especially to patients with long term chronic diseases. There is evidence that patients are more satisfied with the information given before and after endoscopy, when it is given by nurses rather than doctors.523
4.6.6 Speed of diagnosis and complications of care
Not surprisingly, a considerable number of reports have been published on diagnosis for GI disease. Thirty five studies examining the topic in great detail were included in this report. For the most part, these highlight the need for a quick and accurate diagnosis for a spectrum of GI illnesses, including IBD,538,539 IBD in children,540,541 IBS,542,543 abdominal pain in the elderly,544 coeliac disease,174 gastro-oesophageal reflux disease,545 dyspepsia,546–548 disorders of the large bowel,549 ultra-short bowel disease,550 functional bowel disorders,551 Crohn’s disease,552 and acute bowel ischemia.553 Complementing these are studies which deal specifically with the diagnosis for GI related cancers.554–561 Some research was also found on the use of diagnostic procedures (which were largely effective) such as colonoscopy and biopsy,562 oesophago-gastroduodenoscopy,563 imaging techniques (for example, computed tomography, ultrasonography, and MR scan),553,558 push enteroscopy,564 and molecular-pathological diagnosis.565
Table 4.3.4 Annual population based hospital admission rates (per 10 000 population) for different gastrointestinal diseases, based on numbers of finished consultant episodes (FCEs) and on numbers of people admitted in England, 1998–99 to 2001–2002
However, there is also evidence which points to the possible complications which may arise during the treatment of patients or due to the procedures mentioned above, or both. Lang et al suggest that resources and costs double for patients who develop complications after undergoing gastroenterological surgery.566 For upper GI endoscopy, Quine et al warn of the risk of perforation during diagnostic and therapeutic procedures,521 a problem which seems to be occurring at a significant rate owing to inexperienced practitioners. A similar concern is also voiced by a study by Schofield,567 where alleged negligence comes from the activity of GPs, gynaecologists, and colorectal surgeons, and patients receive laparoscopic injuries such as bowel perforation, bleeding, and major vascular damage. In a small study of coeliac disease by Hin et al,378 attention has also been given to problems of underdiagnosis and misdiagnosis.
Clearly, a strong body of evidence exists on providing adequate diagnostic services, which require appropriate training and stringent assessment to ensure patient safety. If this is achieved, the problem that remains is not one of effectiveness, but of ensuring that a sufficient level of service to support the inevitable rise in demand is available.
4.7 Drivers for change
4.7.1 New evidence and guidelines about best care
A plethora of literature can be found on a range of topics concerning guidelines for the care of GI diseases. A total of 45 studies were included for this section of the report, but only a brief summary will be given here owing to the sheer amount of information they cover; readers with a special interest in this area are advised to examine these and other related documents in greater detail. As with previous sections, evidence here can be broadly divided into two areas—treatment and procedures. Some examples include guidelines for the treatment of colorectal cancer,505,556,568,569 bowel cancer,507 other GI related cancers,570–572 Barrett’s oesophagus,573 dyspepsia,546,574–582 IBD,583–585H pylori eradication,586–588, and other GI related diseases.589–598 For procedures: colonoscopy,599,600 endoscopy,600–602 and coloproctology.603 Despite the quantity of such studies, there remains a distinct lack of reference to service provision—in those where such topic was examined, only tentative suggestions are given, or where more substantial studies have been carried out, conclusions lack an evidence base.574,576,578,598,604–606 In light of these findings, and the general lack of an evidence based framework for GI service delivery, there is clearly a pressing need for more research and planning of how services should be delivered and the resources required to meet the demand.
4.7.2 Changing incidence of cancer
Colorectal cancer incidence increased by about 20% among men and by 5% among women from 1971 to 1997. However, reflecting large improvements in prognosis over time, mortality rates fell by 20% among men and by 34% among women (fig 4.7.1A).

Trends in standardised incidence and mortality rates (per 100 000 population) for gastrointestinal cancers, among men and women in England and Wales, 1971–97 (A) for colorectal cancer; (B) for oesophageal cancer; (C) for gastric cancer; (D) for pancreatic cancer. Source: Quinn et al, 2001.14
For cancers of the oesophagus, incidence and mortality both increased by about 60% in men 1971 and 1997, illustrating the poor prognosis associated with oesophageal cancers. Among women, incidence increased by about 40% and mortality increased by about a quarter (fig 4.7.1B).
The incidence of gastric cancer fell sharply by 40–50% in both men and women. Reflecting, improvements in diagnosis and treatment, mortality fell slightly more sharply than incidence; by about 60% in both men and women (fig 4.7.1C).
The incidence of pancreatic cancers fell by about one sixth in men from 1971 to 1997, but remained stable in women. With extremely poor prognosis for pancreatic cancers, annual mortality rates closely tracked incidence rates (fig 4.7.1D).
Figure 4.7.2 shows slightly updated trends up to 2002 for the incidence of each of the four main gastrointestinal cancers separately in England, Wales, Scotland, and Northern Ireland. They show little further trend for colorectal and pancreatic cancers, but further increases in the incidence of oesophageal cancers among men in Scotland and in Wales, and further reductions in gastric cancer among men and women in all four countries.
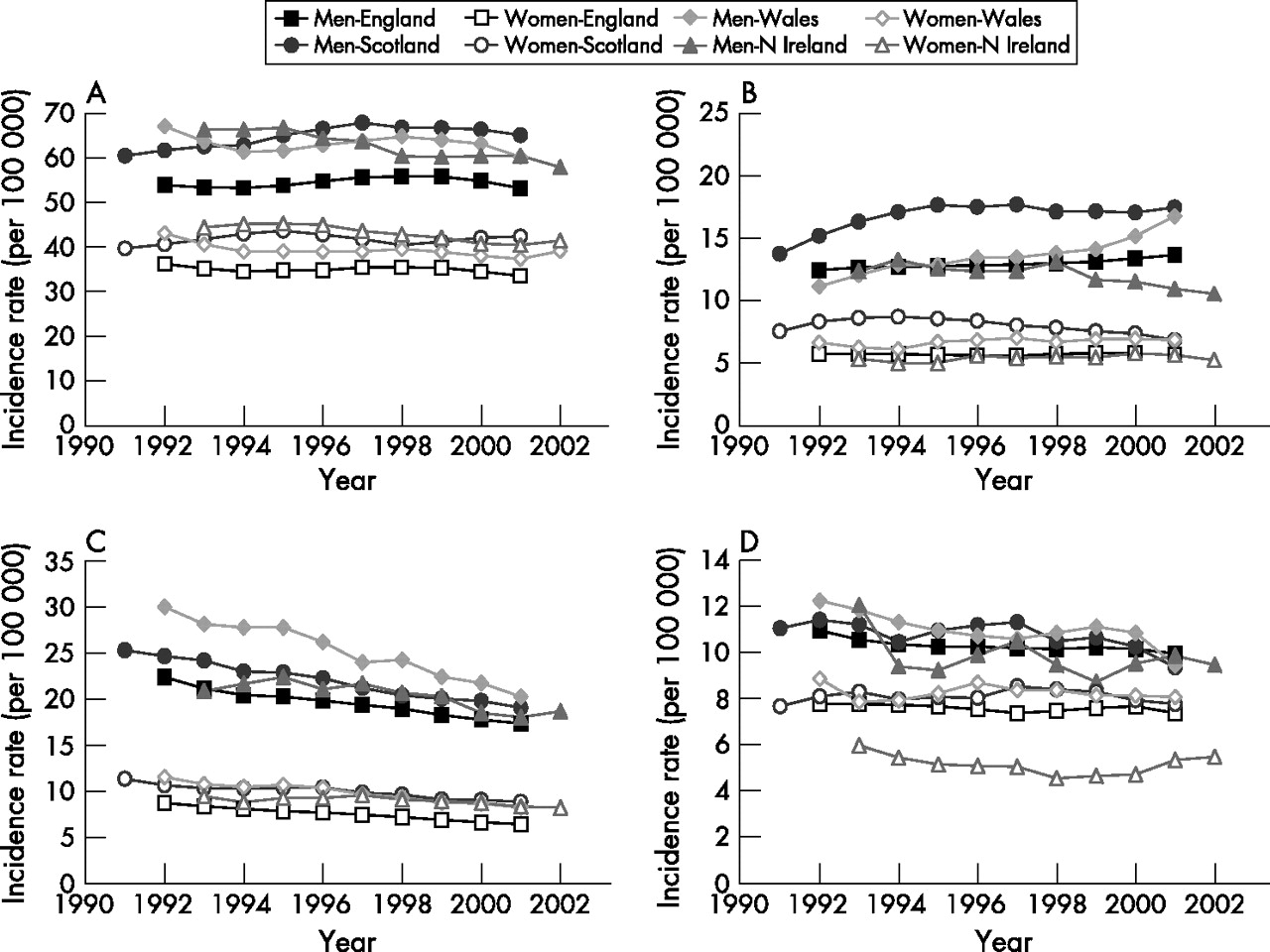
Trends in standardised incidence rates (per 100 000 population) for gastrointestinal cancers, among men and women in England, Wales, Scotland, and Northern Ireland, 1991–2002 for (A) colorectal cancer; (B) oesophageal cancer; (C) gastric cancer; (D) pancreatic cancer. Sources: England: National Cancer Intelligence Centre, Office for National Statistics; Scotland: Information and Statistics Division, NHS in Scotland. Wales: Welsh Cancer Surveillance and Intelligence Unit; Northern Ireland: Northern Ireland: Northern Ireland Cancer Registry.215,454–456
4.7.3 Changing incidence of other gastrointestinal and liver diseases
For a few gastrointestinal diseases, such as acute appendicitis and peptic ulcer in most age groups, there has been a fall in incidence in the UK in recent years. However, for most other gastrointestinal and liver diseases, there have been increases in incidence or prevalence over time (see earlier section 3.2).
These include, in particular, liver diseases such as liver cirrhosis, including alcoholic liver disease, non-alcoholic fatty liver disease, primary biliary cirrhosis and hepatitis C infection, which will have a major impact on health care in this area.
There have also been increases in the incidence of acute and chronic pancreatitis, gallstones disease, upper gastrointestinal haemorrhage, diverticular disease of the intestine, coeliac disease, irritable bowel syndrome, and Barrett’s oesophagus.
For some gastrointestinal diseases, such as inflammatory bowel disease, there is little evidence of a discernible upward or downward trend in incidence in recent years, even sometimes after earlier increases during previous decades. However, because of improvements in treatment, care, and prognosis, the overall prevalence of these diseases continues to rise.
In summary, the overall burden of gastrointestinal and liver diseases has increased greatly in the past few decades, and will continue to rise in the future.
4.7.4 Screening programmes
A significant amount of research has been carried out into screening and surveillance methods for GI diseases. This is reflected by a total of 32 studies included in this report. On the whole, there is strong support for the development and use of widespread screening programmes for a wide variety of GI diseases, where the poor prognosis of GI cancers is mainly attributed to delays in diagnosis.324 Most of the evidence relates to GI cancers607–611 but also covers diseases such as Barrett’s oesophagus,573,612,613Helicobacter pylori,614 GERD,615 and diarrhoea.616 The main problems in this area are the economic costs associated with such programmes–that is, that they need to be adequately managed and feasible608,610,614,615,617–623; need to control and ensure high quality screening practices573,607,612,613,624–628; and need to provide a greater awareness of the effectiveness of existing and new methods for screening.611,629–635
Currently the British Society of Gastroenterology recommends colonoscopic surveillance of patients with inflammatory bowel disease636 and colonic polyps.636
A national screening programme for bowel cancer is to start in England in 2006.637 This will have significant implications for endoscopy services.
4.7.5 Genetics
Medical genetics, in the form of Cancer Genetics Services already impacts on the delivery of GI services, albeit to only a relatively small extent, for those patients, and their relatives, who are at increased risk of GI tumours owing to some form of genetic predisposition and hence require some form of GI surveillance, usually by colonoscopy.638–640 Cancer genetics is a rapidly developing field, becoming increasingly sophisticated, and in the future, clinical genetics input is likely to extend to other common GI conditions—for example, IBD and coeliac disease.641,642 Advances in genetics will improve not only the ability to predict who is, or is not, at risk of certain conditions, but also improve diagnosis, partly through molecular pathology.643,644
Medical genetics will also play a part in other areas of GI services—for example, predicting a person’s responses to drugs, including adverse events (pharmacogenetics), and predicting response of tumours to treatment (somatic genetics, as opposed to germline genetics). It is likely that pharmacogenetics will impact first on avoiding adverse events, with individual tailoring of prescriptions following later.641,642,645,646 Although the science of predicting response to treatment from an analysis of a tumour’s genetics is in its infancy, certainly as far as GI medicine is concerned, it promises to deliver truly individualised treatment. A considerable amount of work needs to be done, however, to translate this into practice.644,646–650 More widespread molecular genetic testing of tumours will also reveal more people who are genetically predisposed and thus warrant the attention of cancer genetics services.
4.7.6 Prevention
Studies on the prevention of GI diseases are not as prolific as might be expected. Only five studies were found to examine the subject in any significant detail,512,651–654 and even in these varied in the topics and diseases covered. Among those included in this review, are the prevention of H pylori,654 traveller’s diarrhoea,653 and NSAID related morbidity and mortality.512 Muller and Sonnenberg emphasise the beneficial effects of endoscopy for reducing mortality due to colorectal cancer and cancers of the large bowel, and outline its crucial role as a preventative procedure.652 Hulscher et al also discuss the role of interventions to increase preventative activities in primary care, and the need for more research to determine their effectiveness.651
4.7.7 Development of managed clinical networks
The complexity of some disorders has been a driver for the development of clinical networks that cover many disciplines across different healthcare organisations. The Calman-Hine report was the catalyst for clinical networks to support the care of patients with cancer and it has been proposed that similar networks be set up for liver disease and hepatopancreatobiliary surgery.214
4.7.8 Quality assessment of endoscopy
At present, there is no agreed national approach to quality assessment of endoscopy, but this is now being remedied, after the appointment of a national clinical lead for endoscopy by the Department of Health. The following activities are in progress:
-
Development of a global rating scale
This is a scale that provides an indication of how a patient will experience having an endoscopy in an endoscopy unit. There are 12 items on the scale that reflect two dimensions: quality and safety of care, and customer care. A recent census in England using this scale was completed by >90% of endoscopy units. Further measurements will be done twice yearly. The scale has been underpinned with objective measures, and a web reporting system for the scale has been completed (http:www.grs.nhs.uk, accessed 18 January 2007). The scale is designed to support quality improvement and help inform patient choice as well as quality assure endoscopy units.
-
Ensuring the appropriateness of endoscopy and referral pathways
This work aims at streamlining the patient pathway. It is likely that the “Map of Medicine” commissioned by the National Electronic Library for Health will provide an electronic framework for referral pathways linked to choose and book systems (http://www.mapofmedicine.com, accessed 21 December 2006).
-
Development of a competency framework
A competency framework for all health professionals working in endoscopy is currently being prepared. This will form the basis of certification of trainee endoscopists and endoscopy assistants.
-
Re-validation of established endoscopists
A re-validation methodology for established colonoscopists is currently being tested. Only those who have successfully completed this process will be allowed to perform colonoscopy on patients referred for colonoscopy through the bowel cancer screening programme which began in 2006.
-
Accreditation of endoscopy units
A process for accreditation of endoscopy units is currently being designed and tested. This peer review type process will replace the self completed questionnaire accreditation process required by the JAG (Joint Advisory Committee on Gastrointestinal Endoscopy). Formal accreditation of units which began in 2006.
-
Development of quality and safety markers
The BSG endoscopy committee is currently preparing quality and safety markers for endoscopy that will underpin the Global Rating Scale and the accreditation process.
5. MODELS OF SERVICE DELIVERY AND THEIR EFFECTIVENESS: OVERVIEW OF THE RESEARCH LITERATURE
5.0 Methods
5.0.1 Systematic review of evidence
To promote a reliable, consistent, and unbiased reflection of existing research is the principal idea behind the use of systematic reviews. The establishment of numerous organisations such as the Cochrane and Campbell Collaborations which provide up-to-date reviews in the area of health, educational, and social research, and of course, a proliferation of such reviews and associated methodology in the traditional academic arena, underlines the sort of attention directed towards them over the past decade or so. In comparison with conventional literature reviews, systematic reviews are designed to answer a specific question based on research evidence rather than to provide a general overview of a topic. Thus, the practical advantages of systematic reviews and the associated analyses are generally transparent—to deliver a holistic summary and synthesis of individual pieces of research evidence which together constitute a stronger body of evidence. However, the immense resources needed for the retrieval, appraisal, and synthesis of the relevant literature are a prominent drawback. Indeed, the inspection of literally thousands of publications is not uncommon in systematic reviews, all of which require careful screening for inclusion or exclusion, from which only a small percentage can be deemed appropriate for the research question.655–657 Moreover, the processes undertaken during a review can be contentious, including claims that the review can be used as a means of exerting political control over new research; criticisms of the outcomes derived from it (with respect to relative importance and methods used); and the way in which users are to be involved throughout (see, for example, Davies658 and Gough and Elbourne659 for a more detailed discussion). Although these concerns are beyond the scope of this report, they represent real and substantial problems, which should be borne in mind throughout. What is clear, is that any critical evaluation of literature should take into account the techniques used in systematic reviews so as to promote consistency and reliability and obtain an accurate reflection of the work that is already out there. For these reasons, particular attention was placed on the design and development of suitable review methods with which to conduct a literature review and synthesis for this report.
At the heart of any systematic review is its review protocol. This consists of explicit criteria for the retrieval of relevant literature, and includes factors such as keywords, sources of information (such as databases, periodicals, and reports), and systematic methods for conducting and managing the search to enable repeatability—that is, a search that can be performed as many times as necessary by any researcher using the same criteria. The final list of factors deemed appropriate for the task is often referred to as the inclusion and exclusion criteria, which clearly specify the types of study to be included in the final analysis, as well as how, where, and with what the search is to be carried out. These factors ultimately determine the shape of the literature search, and hence the final outcomes of the study. The protocol thus represents the methodology which underpins the research, and forms the basis for the evaluation of the data obtained. A crucial element in this report was therefore the design and implementation of a protocol which adheres closely to the established conventions of systematic reviews and one which could be applied with a high degree of repeatability and consistency using the available resources so as to enhance the quality of information for the final analysis.
Design aspects of review protocols660 were taken into account to enable a reliable method of literature and data retrieval to be constructed, particularly for the central aspects of the investigation. It can also be seen later in this section that an extensive quality appraisal and grading of evidence was carried out to enhance the interpretation of the findings. The first subject to be examined was specification of the research question. This was deemed to be of two parts: (a) the current burden of GI disease and services (representing the general areas of the report), and (b) service provision and its effectiveness for GI disease in the UK (section 5). In order to tackle these areas, two sets of criteria for the protocol (such as those mentioned above) needed to be established. The first protocol would be used for sections dealing with general GI topics (the burden of GI disease), while the second would be developed to focus on service provision and its effectiveness for GI treatment. Figure 5.1.1 provides a map of the various stages of the protocol to be incorporated.

As can be seen in fig 5.1.1, the report follows the general structure of a systematic review, with the main difference being that a broad set search strategy is used for related topics of interest, while a separate criteria is used for the main area of study. This approach thus allows key points of interest to be reviewed systematically, and related areas to be incorporated into other sections of the review. The remainder of this chapter outlines the various components of the review protocol used in this study.
General search strategy
The design of this search is to examine the current burden of GI disease and services in the UK. It was expected that a wide a variety of literature would be encountered during the study, which includes paper based and electronic articles, research articles, general reports, and systematic reviews. To determine the basis for inclusion and exclusion, a consideration was made of the following topics:
-
Relevance of content
Searches in electronic databases were carried out using the keywords shown in table 5.1.1; only those which adhered to the aims of the report were included. Manifestly, it was not possible to incorporate every conceivable synonym under each subject heading as this would not only make the search process unmanageable but would probably also make the search too broad for the requirements of this report. Nevertheless, the words shown in table 5.1.1 were defined after thorough consultation with subject experts and librarians, and can be considered accurate for the purpose. Furthermore, terms used as part of medical subject headings (MeSH) produced by the National Library of Medicine were used where permissible (such as Cochrane) as a thesaurus to cover a broad range of keywords and synonyms. Although keywords, synonyms, and MeSH terms allow a considerable amount of literature to be retrieved, the specificity and appropriateness of content might require a more detailed examination because publications may or may not be relevant even with the presence of certain keywords. Consequently, an in-depth assessment of abstracts and, where required, the entire article or report, was carried out by researchers and subject experts where the appropriateness of content was uncertain. A more detailed description of this and actual search techniques can be found below.
Table 4.3.5 Numbers of surgical procedures: all, main, and day case procedures according to OPCS-4 chapter in England 2000–2001
Table 4.3.6 Surgical procedures of the digestive tract and other abdominal organs with waiting times in excess of 90 days in England, 2000–01
Table 4.5.1 Number of finished consultant episodes and costs (£000) digestive system HRGs: England 2001–02
Table 5.1.1 Keywords
-
Setting and population
Although a comparison of results from other countries would have been useful, this was outside what could be realistically achieved in the given time frame. Publications were thus restricted primarily to those relevant to the UK, but no stipulations were made about the population studied (such as men and women).
-
Date of research
Despite the emphasis on current issues pertaining to the burden of GI disease, older articles and reports are also of interest because they allow for interesting comparisons, particularly for the rate of development. As a consequence, no restrictions were placed on date (in the majority of databases used in this study, this would include studies published between 1966 to present), but primary focus was placed on more up-to-date literature.
-
Research methods
No specific requirements were made of certain study types or experimental designs. The expectation was that a wide variety of publications would be obtained for general concerns of GI disease (owing to the breadth of the subject), including survey, evaluative, and experimental studies. All types of study design were thus included in the search criteria, and included those published in peer reviewed academic journals, relevant reports, and systematic reviews. Owing to the wide range of sources, an important concern was that of literature assessment with respect to the overall quality of the articles used (that is, the reliability of the results) and the grading of evidence (see below).
-
Language
An inherent problem for any extensive literature review is that highly relevant articles and reports may be written in a language other than English. Given the report’s primary focus on GI disease in the UK, this particular problem was not expected to be too important. Nevertheless, to guard against possible exceptions, and in particular, the obvious pitfall of excluding potentially relevant studies, the decision was made not to exclude on the basis of language. As far as resources permitted, the aim was to obtain and translate relevant foreign publications for the report where English titles and abstracts indicated potential relevance.
-
Inclusion and exclusion procedure
After a systematic search of the relevant sources (a discussion of the criteria is given below), a detailed screening of the articles retrieved was required to determine final inclusion or exclusion. To maximise the consistency and accuracy of this process, a pilot test was undertaken in which two researchers (one of whom is a gastroenterologist) carried out inclusion and exclusion on the same set of articles. Although perfect agreement is difficult to achieve, discrepancies were examined, from which a standard protocol was developed. The final set of articles were then individually screened and categorised into one of two groups—include (including borderline cases with some degree of relevance) and exclude.
The next stage was thus the development of the actual search strategy to incorporate these various requirements. The crux of this process is defined by the terms set out in table 5.1.1. Although these help to increase the accuracy and specificity of the search, there are literally tens of thousands of combinations (that is, searches) possible by using a word from each of the five columns, making the workload virtually unmanageable. Despite this apparently colossal task, the use of Boolean operators (AND, OR, NOT) allowed the search to be conducted with greater efficiency. The fields in which individual terms were searched are article/report keywords, abstracts, title, and where possible, MeSH categories.
The configuration of Boolean operators and keywords is shown in fig 5.1.2. This procedure sets the specificity of the search, and can easily be broadened or narrowed, if necessary, depending on the quantity of articles retrieved. Should it be found, for instance, that a search combining all five columns in table 5.1.1 yields results which are too specific (exemplified by a low number of studies retrieved), the search can be broadened by combining terms from only four columns, and so on. Although great care must be exercised throughout (it might be the case that the paucity of studies is due to the fact that very little has been written about the subject in question, rather than an inherent problem with the search strategy), this iteration was employed during the search process until the team was satisfied that coverage and specificity were adequate.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
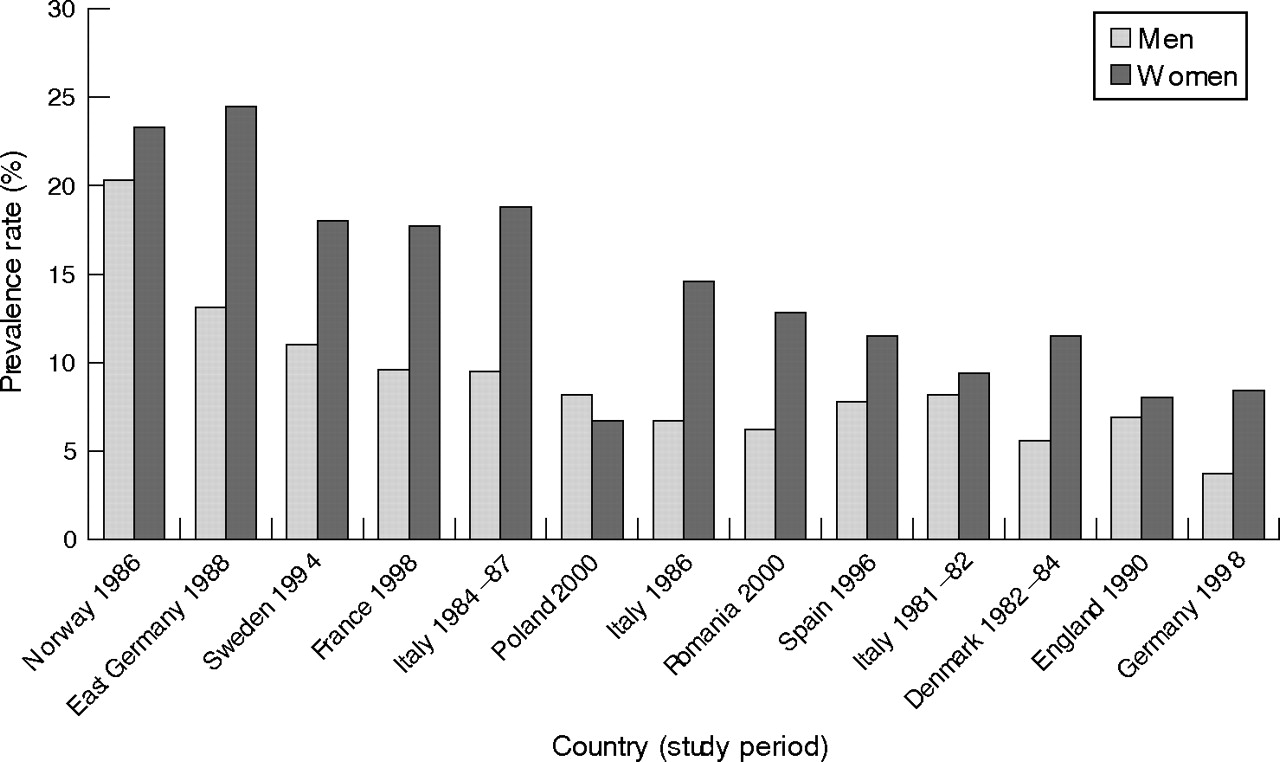{kind=link}
{kind=link}
{kind=link}
{kind=link}
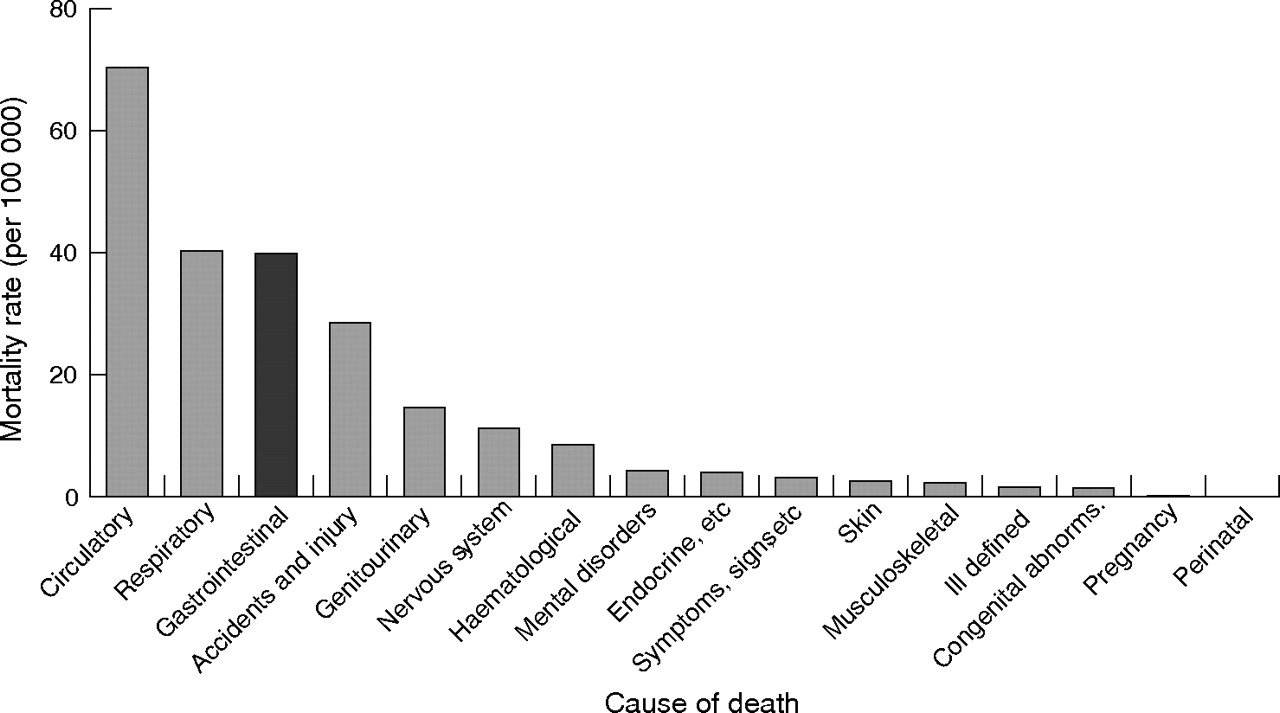{kind=link}
{kind=link}
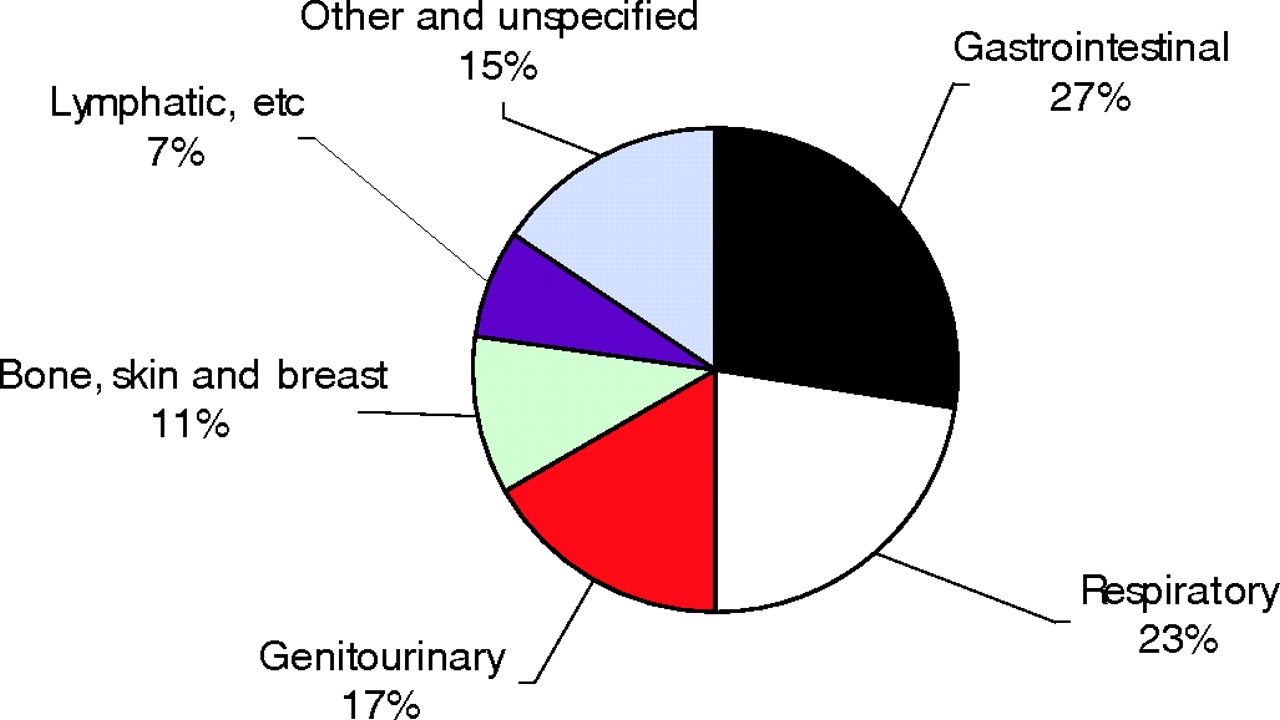{kind=link}
{kind=link}
{kind=link}
{kind=link}
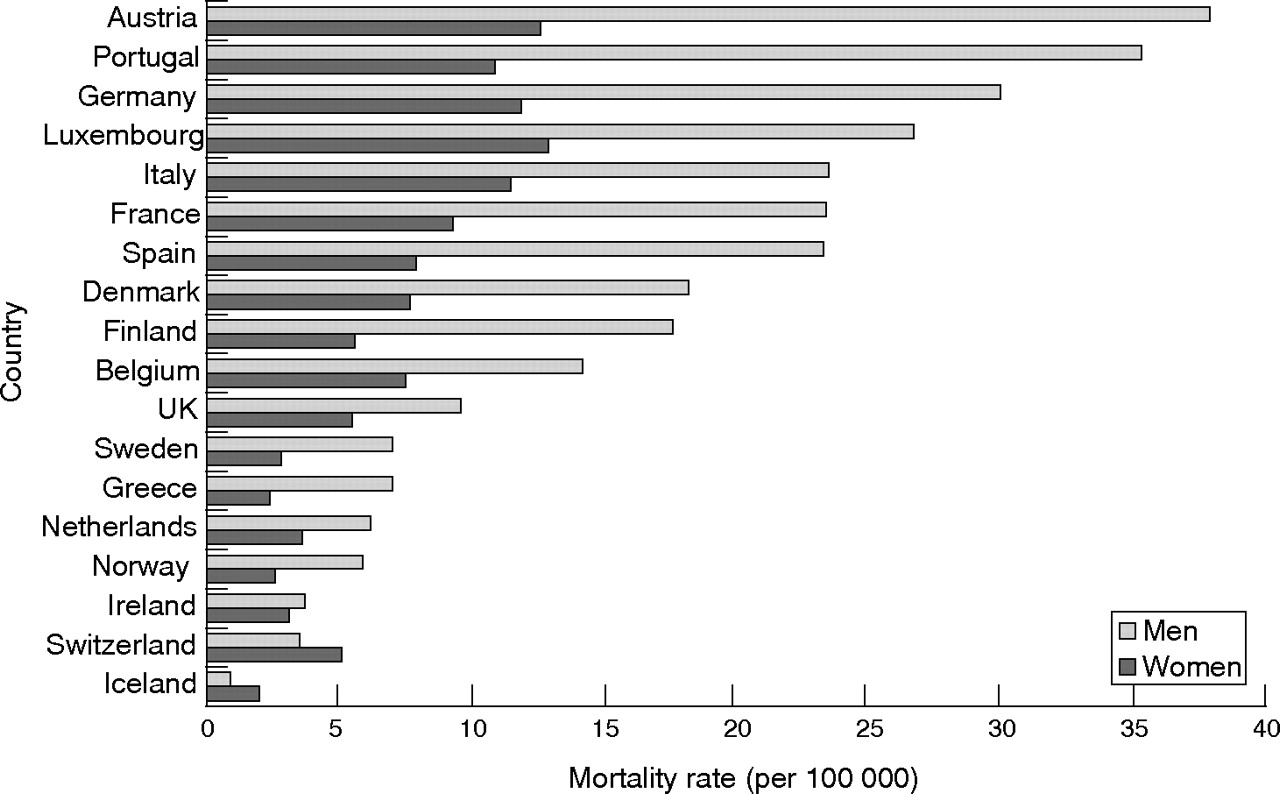{kind=link}
{kind=link}
{kind=link}
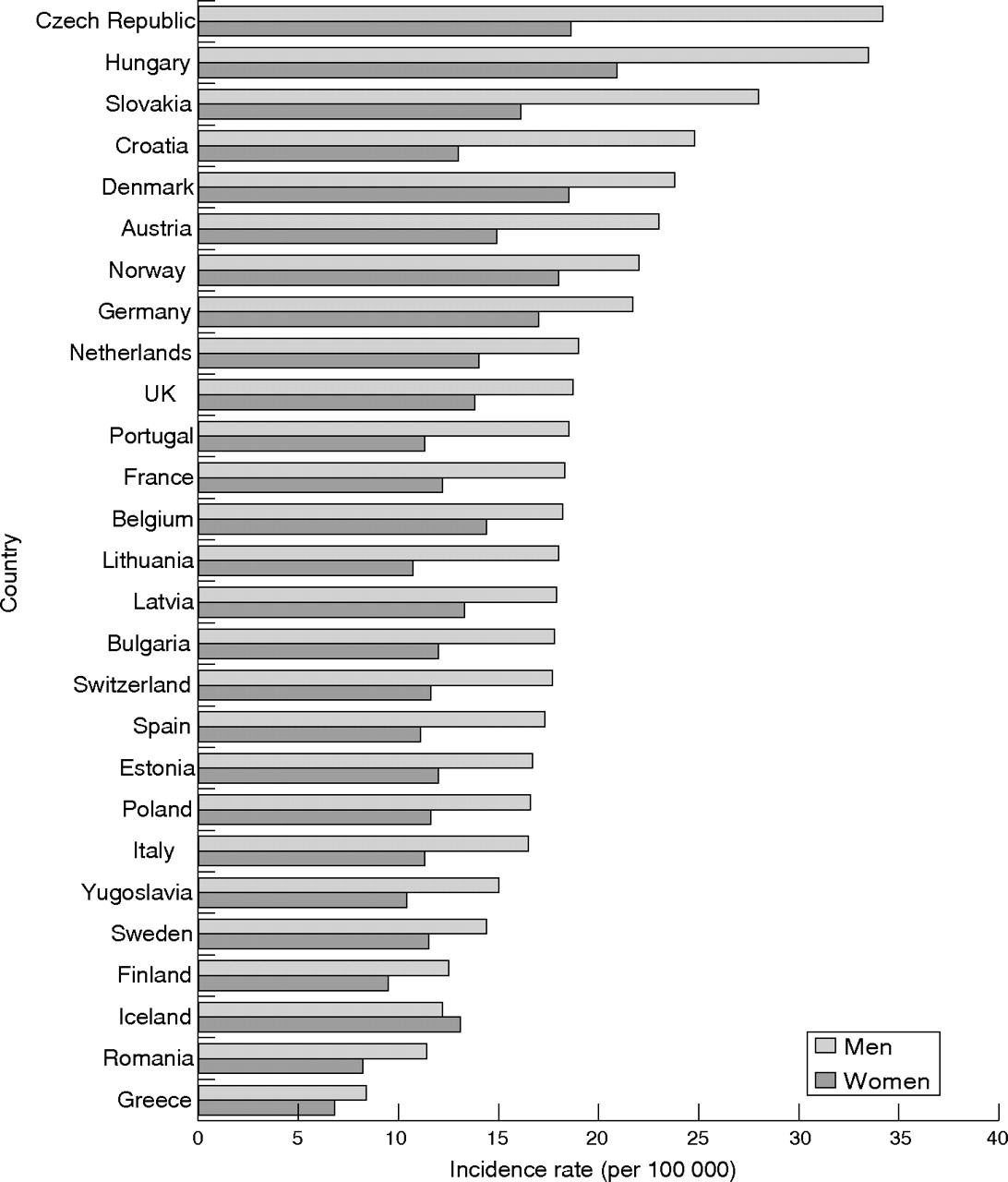{kind=link}
{kind=link}
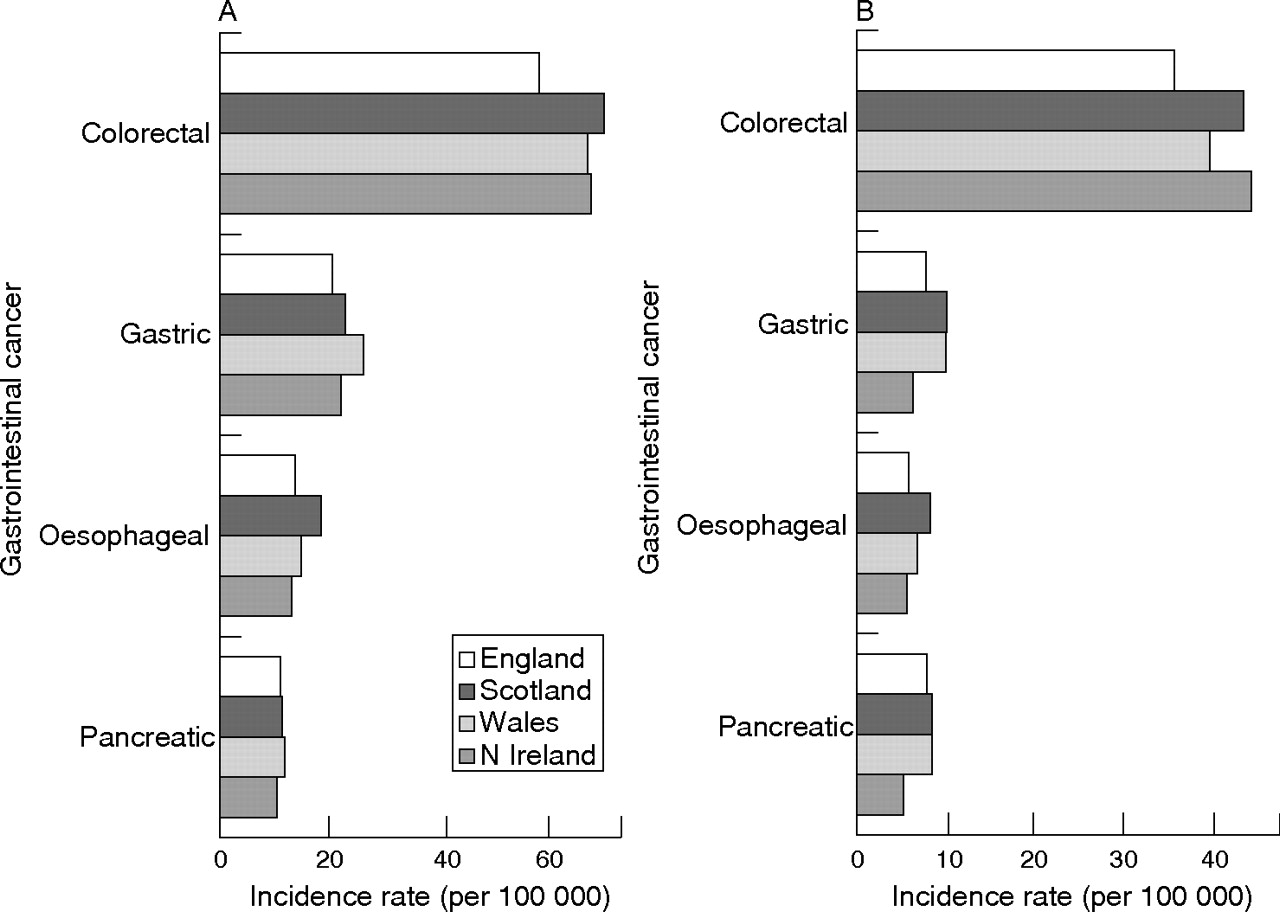{kind=link}
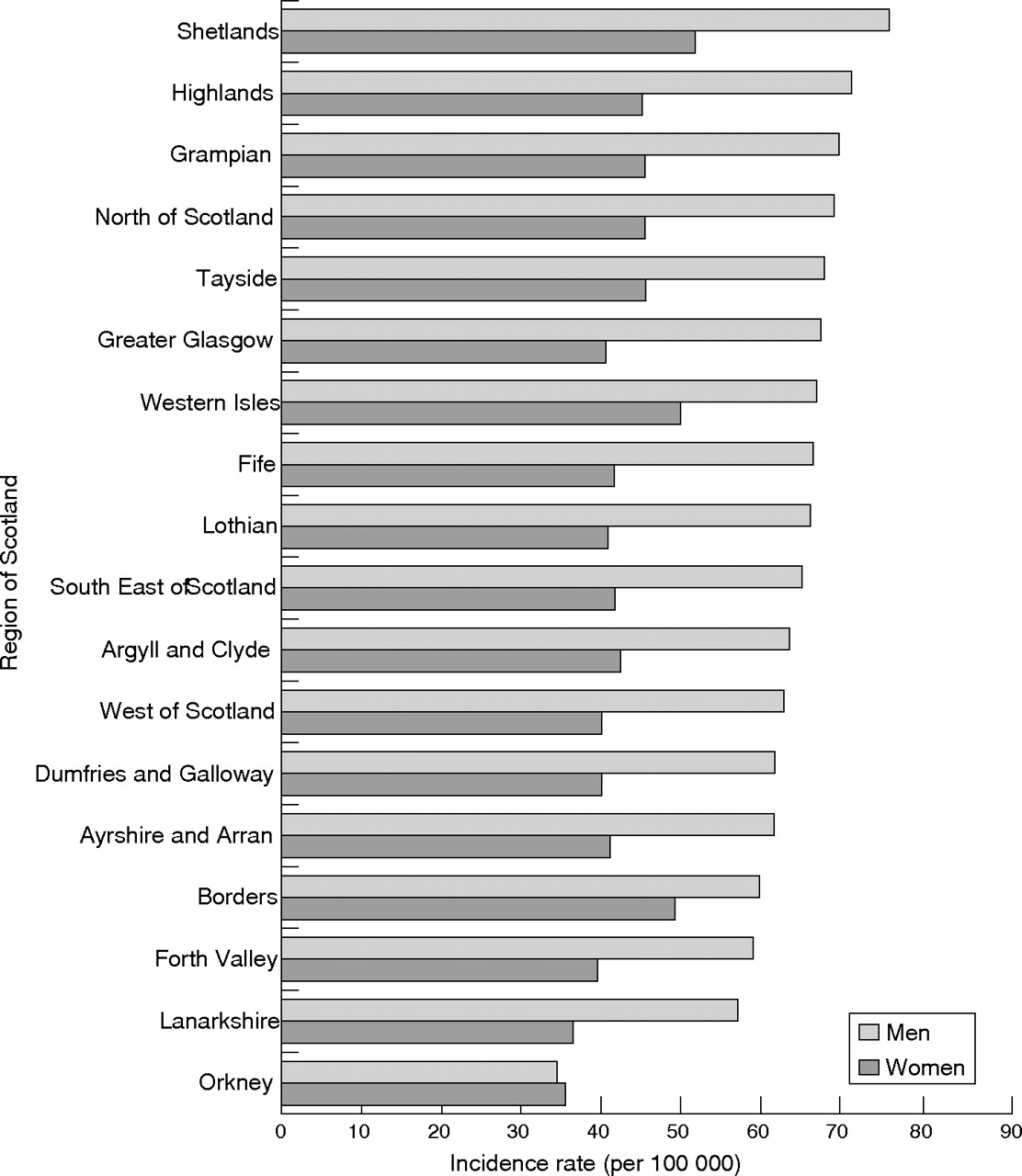{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
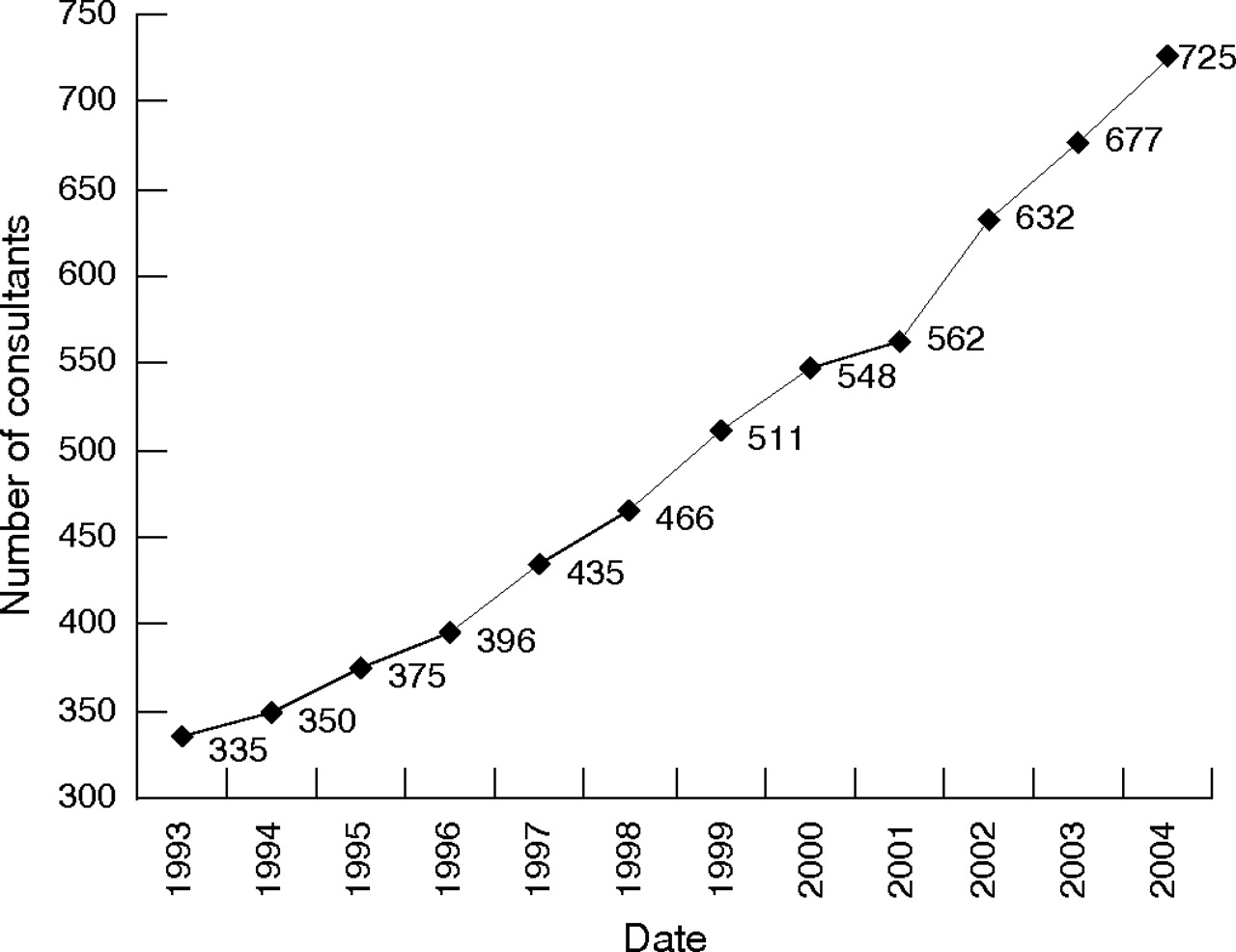{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
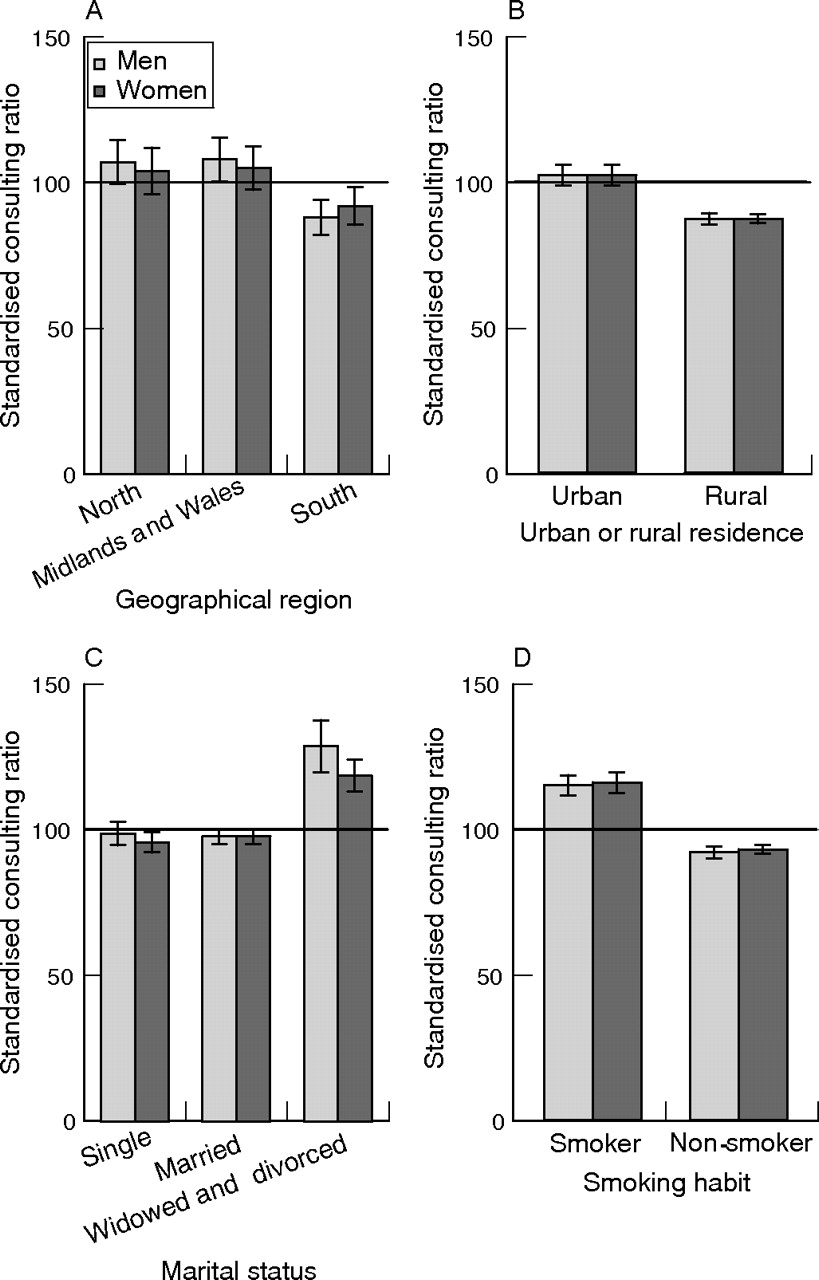{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
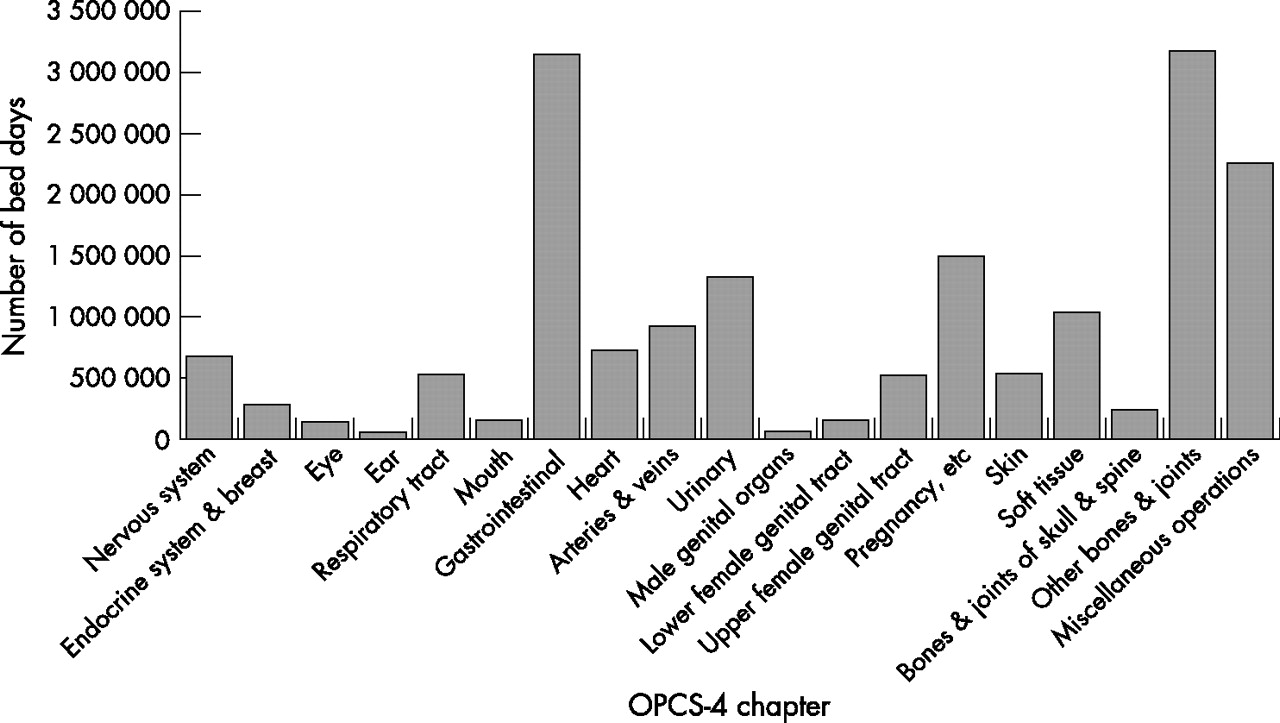{kind=link}
{kind=link}
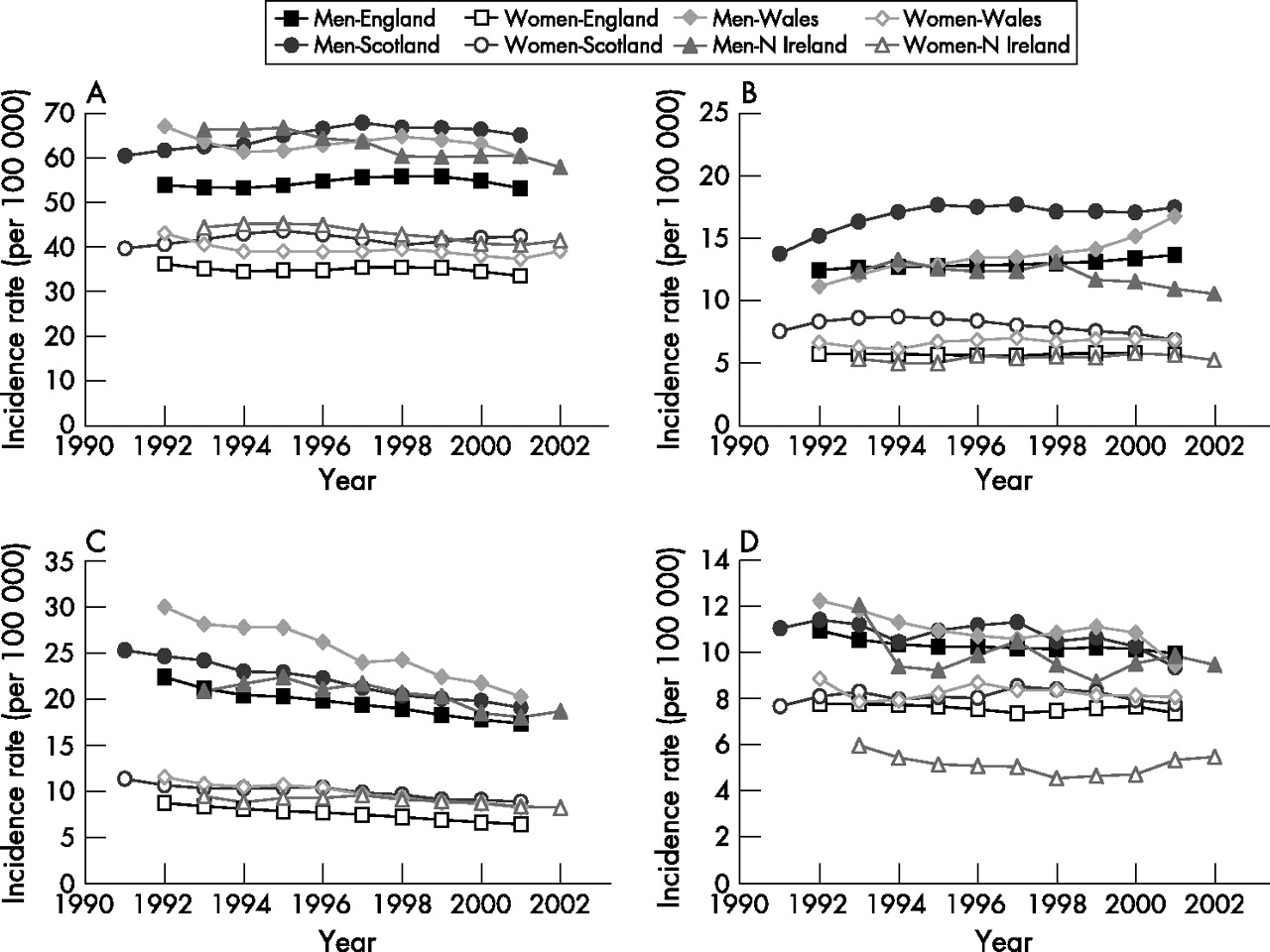{kind=link}
{kind=link}
{kind=link}
Search strategy.
The primary sources of literature are shown in table 5.1.2. Most of these are electronic databases available via the internet where the search strategy described above is implemented. Although these provide comprehensive coverage of relevant sources of information, further searches were carried out of other sources (such as general internet searching, citations from relevant articles, and articles identified by existing GI projects within the department) using the same stipulations on content as described above.
Table 5.1.2 Primary literature sources
Search criteria for service provision
After the general search, a separate search strategy was developed for the key area of the report: the provision of services and their effectiveness for GI treatment. Among the criteria, attention was placed on specifying the literature with a more appropriate set of search terms. Inevitably, there would be a degree of overlap between this and the general search described in the previous section owing to certain similarities in the nature of content. But because search strategies are rarely foolproof and do not find all the desired material, this search helped to identify a greater number of relevant articles.
The definition of new keywords for the key area was established by using those shown in table 5.1.1 and after a further consultation with subject experts. The revised search terms shown in table 5.1.3 are similar to those for the general search, with the differences being four columns as opposed to five (the burden of disease is excluded, thus making this search broader than the previous one), and four additional keywords relating to the subject of effectiveness. This aside, all other stipulations are the same as those described in the previous section: characteristics of literature; use of keywords from each of the four columns with Boolean operators (as before, the number of columns can be reduced to allow coverage to be broadened as necessary); literature sources; and the process of inclusion and exclusion. The new search strategy was brought together using the technique shown in fig 5.1.2.
Table 5.1.3 Keywords for key areas of report
Quality assessment and grading of evidence
Techniques of quality assessment are commonly applied to gain insight into the credibility and reliability of studies being examined. Although the measurement of quality (in this case, the likelihood of the methods generating unbiased results) is inherently difficult,657 numerous techniques have been developed to enable the quality of research methodology to be gauged with better clarity (see Verhagen et al663 for discussion). Given the time frame and resources permitted for this study, it was decided that an extensive examination of quality would not be feasible. Nevertheless, it was deemed necessary that a tool be adopted to analyse and ensure that the literature used is of an acceptable level of quality during the synthesis of evidence. In addition to quality, there was also a need to establish a means of grading the evidence (for example, systematic reviews, cohort studies, and expert opinion) in order to measure the overall strength of recommendations. Used together, the two techniques allowed studies to be assessed independently irrespective of study design, and graded collectively for the purpose of formulating clear and evidence based recommendations for GI service delivery. The following two subsections outline the methods used in this study.
Quality assessment
The purpose of this exercise is to provide a quantitative assessment of the quality of studies irrespective of their study design. Given that some study types are generally considered to be more reliable than others (for instance, systematic reviews are generally regarded as more reliable evidence than, say, consensus opinion—see next section), it was important that each study included in this report be assessed for its individual quality, rather than its design. The benefit of this approach is that extra weighting (if indeed justified) can be assigned to studies which are regarded as of a lower level of evidence, but which are nevertheless carried out with sufficient rigour to justify the findings carrying greater significance. The result is that the true quality of the evidence can be captured with greater clarity and the interpretation of recommendations can be enhanced.
Possible instruments available for this purpose include the Maastricht, Delphi, and Jadad lists (designed predominantly for randomised controlled trials (RCTs) and experiments), and the AGREE tool (for the assessment of clinical practice guidelines developed by the Appraisal of Guidelines Research and Evaluation Collaboration664). These are typically measurement/rating scales which share broad themes in an examination of the appropriateness, transparency, relevance, and hence quality, of the chosen methodology for the research question. Of those instruments suitable for this report, the AGREE tool seemed to be the most appropriate. Designed as a generic and relatively compact scale, it measures the quality of reporting and recommendations of clinical guidelines, and has been used by a wide range of medical institutions for evaluative purposes. Similar to tools such as the Delphi and Jadad lists, it covers various aspects of quality concerning clinical research. Some of the advantages of this tool include a concise 23 question/item scale as compared with the 40-plus items in the Delphi list665 and the comparatively simplistic three item Jadad list666, a wide range of general components (as opposed to strict requirements on specific study designs such as RCTs), and its easy modification to suit the requirements of this study. Statistical tests conducted by Cluzeau et al667 also found a good level of reliability for individual sections and of the scale as a whole (Cronbach’s α between 0.64 and 0.88, which exceeds or is close to the recommended value of 0.7668).
The AGREE tool evaluates quality via questions within each the following sections:
-
Scope and purpose
-
Stakeholder/participant involvement
-
Rigour of methodological development
-
Clarity and presentation
-
Applicability and relevance
-
Editorial independence.
As can be elicited from the above, all parts of the tool can be made directly applicable through minor adjustments of terminology for a quality appraisal of the literature used in this report. Through a consultation with subject experts and those with relevant expertise, such as statisticians and questionnaire designers involved with the project, appropriate modifications, mostly involving minor changes to words and phrases to make them relevant to literature, were made: the final instrument consists of 22 questions/items, and can be found in Appendix 2. The decision was made to use a three point Likert scale to measure the agreement, disagreement, or undisclosed information (such as methodology) for each item: 0 = not specified (little or no evidence); 1 = disagree (some evidence); 2 = agree (good or strong evidence). A total score for each article was then calculated to obtain an indication of overall quality.
As a means of piloting the tool for validity and consistency, 20 articles were chosen at random and appraised by two project researchers. Scores for each item were assigned after reading the articles in detail and further discussion, and then total scores were calculated for each article included in the report; this score was simply a percentage calculated as the sum of scores for each of the 22 items divided by the maximum possible score, 44—thus, a paper with a total score of 22 obtained 50%. The next step was to determine how these scores could be usefully interpreted as an indication of quality. Although there are no clear guidelines for this, the general observation was that the higher the score, the greater the rigour and quality of the article, and hence the following intervals were used as a general indicator of quality (S = score):
-
S⩽45%—generally poor quality of evidence; falls short in a few key areas of quality (see (a) to (f) above)
-
45%<S<65%—generally reliable quality of evidence; falls short in one or more key areas of quality
-
S⩾65%—good quality of evidence; falls short only in a few items of quality.
Next, Cohen’s κ669 was calculated in SPSS (Statistical Package for the Social Sciences) to determine the degree of agreement between the two assessors. Interrater reliability between two assessors was 0.894 for the 20 articles, indicating a strong degree of consistency. Because of resource limitations, the decision was then made for one assessor to appraise all the remaining articles in the study.
Grading of evidence
In addition to quality assessment, a means of classifying the evidence needed to be established in order to reflect the strength and type of evidence that has been used to formulate recommendations. The appropriateness of this approach, however, depends on the study question. Evidence hierarchies typically used for this purpose, being focused on effectiveness, may not fully acknowledge the validity of other studies which, despite taking into account a much wider range of issues, may be considered to be of a lower level.670 As this study focuses on service delivery, which encompasses a broad range of subject matter, which cannot always be measured or assessed easily by intervention studies of effectiveness, it would not be a complete surprise to find that the evidence collected for it reflects those studies which are placed lower down in the hierarchy, hence reducing the overall grades of recommendation. Nevertheless, it was thought that used in conjunction with quality appraisal, the grading of evidence would help to provide a wholesome reflection of existing research, and would provide a conventional framework within which to proceed.
The hierarchy used in this study is based on that documented in the Centre for Reviews and Dissemination (CRD)660 and NICE.671 But in light of the issues raised above, some minor modification (mainly to reduce the number of groups in the hierarchy) was made to allow for a wider range of studies to be graded with greater ease (table 5.1.4).
Table 5.1.4 Hierarchy of evidence
Using this hierarchy, recommendations can be classified by the strength of evidence on which they were based (see table 5.1.5—adapted from CRD660; NICE671). However, in this document conclusions have been drawn, but recommendations have not specifically been made.
Table 5.1.5 Classification of recommendations
5.0.2 Focus group with patient and carer representatives
A discussion session with the Patient and Carer Network was held at the Royal College of Physicians, London, on 8 December 2004. Its aim was to highlight some of the key problems associated with the delivery of services in gastroenterology based on the review of evidence described above, and to get views on these from patients and carers which could be reflected in this report. Three researchers from the project team attended and designed the objectives for the session—JGW (observer/GI expert), HS (facilitator), and BI (scriber). After the review of evidence described above, four main topics for discussion were identified and presented by the facilitator for discussion. These were:
-
Greater self management by patients
-
Endoscopy outside hospitals
-
Should endoscopy be carried out by nurses or doctors?
-
Where should services be located—for example, primary, secondary, tertiary, specialist care?
A total of 11 patient and carer representatives were present on the day, and gave permission for the discussion to be recorded electronically for transcription. Two independent observers were also present, but did not partake in the debate. Discussions on each topic lasted for around 20 minutes, and participants were encouraged to raise their views. It was felt by the research team that a number of important concerns were raised in this session, and these have been incorporated into the results sections of this report.
5.1 Results
5.1.1 Literature search and synthesis
Using the methods described in section 5.0.1, a total of 5039 articles (1830 for search 1 and 3209 for search 2) were identified by the literature search for potential inclusion in the report. Further screening by two project researchers for inclusion and exclusion (see section 5.0.1) reduced the final number of articles included to 394. A further 38 articles and reports were identified through hand searching of related sources (such as reports, the internet, and periodicals), which gave a final total of 432 for the main sections of the document. Articles obtained but not used are given in table A.14 in Appendix 4.
Given the broad nature of topics covered in the report, and that some articles cover many subjects, the next stage was to categorise each article into its main areas of relevance. This was performed by one researcher who, for each included article, skim-read and recorded the topics covered (for example, incidence, mortality, quality of life). From here, the recording of evidence was compiled by assigning each of the articles to an appropriate section of the report, and then into summary tables. Details of each article (such as topics covered, quality score, grade of evidence, and key findings) were recorded so that an overall synopsis (or where appropriate, a recommendation) of the main topics could be derived.
5.1.2 Economics of GI services
A total of 153 articles were identified which dealt with some aspect of the economics of GI disease. The review was limited to studies undertaken in the UK, partly to keep the number of studies manageable but also because of recognised problems in transferring cost and cost effectiveness results between countries.672
The main overall message from the review is that there is a paucity of high quality economic studies in this area. The evidence for the economic burden of gastrointestinal disorders, and the cost effectiveness of treatment is summarised in section 5.5. Articles obtained but not used are given in table A.15 in Appendix 4.
5.2 Developments in service delivery
Shared care
Both the Department of Health673,674 and the British Society of Gastroenterology jointly with the Royal College of Physicians489 recommend that high quality services should be delivered locally whenever possible, with blurring of the traditional primary/secondary care divide, and should aim at promoting independence and self management when appropriate. An analysis of routine data suggests that more efficient use of services would result from greater integration between primary and secondary care,675,676 and this is recommended by the Royal College of Physicians of London, Royal College of General Practitioners, and the NHS Alliance for the improved management of chronic disease.677 The evidence for this, however, is from a study which examined the 11 leading causes of bed use—that is, it did not focus on GI disease. Two studies included an economic component for palliative care schemes for patients with cancer. Neither showed a difference between control and intervention groups.517,621
A rapid review of strategies to facilitate transferring specialised care into the community found some evidence to support moving diagnostic testing and outpatient follow-up to primary care, but the studies did not deal with GI disorders.678
For inflammatory bowel disease, there is a strong evidence that patients benefit, and there is less demand on conventional services when comprehensive patient education is combined with easy and rapid access to specialist care when needed,679–683 although overall costs are broadly unaffected.679,682 Possibly, these findings could be extrapolated to other chronic gastrointestinal disorders, particularly irritable bowel syndrome.684 The particular problems faced by adolescent people with inflammatory bowel disease and the need for support in the transition from paediatric to adult care has been emphasised by the National Association for Colitis and Crohn’s Disease (NACC).685
Total parenteral nutrition can be delivered at home686 and is a safe alternative to early surgery in complicated Crohn’s disease. It can also be cheaper,687 but increased resources will be needed if it is to be implemented for inoperable cancer.688 There are no economic evaluations of home parenteral nutrition for malignant disease and AIDS.687
Treating patients at home is not a cheaper alternative to inpatient care. The evidence for this, however, is from studies that did not focus on GI disease. Further research is needed, and treatment at home as an alternative to inpatient care cannot, at the present time, be recommended.689
The Royal College of Pathologists set recommendations on specimens of limited or no clinical value, which might lead to a reduction of pathology workload,603 but the cost effectiveness of this remains to be assessed.
Table A.1 summarises the articles examined for shared care.
Table A.1 Developments in service delivery: summary of articles examined for shared care
Primary care
NHS policy supports the development of the concept of general practitioners with special interest,690 though endoscopy is the only facet of gastroenterology that is covered in the recommendations.691 However, although 16% of GPs were already providing specialist interest services in 1998,692,693 there is currently no evidence to support the cost effectiveness of these changes.693,694
Few studies have examined the economic implications for primary care of H pylori testing and eradication.695 It is unclear whether such a strategy would be cost effective as an initial management strategy in primary care.696
Outreach educational interventions have been shown to improve appropriateness of referral to secondary care of patients with dyspepsia.580 However, before it is more widely used, further investigation is required to assess the overall cost effectiveness of this expensive intervention.697 A self help guidebook has been shown to reduce the number of primary care consultations for IBS, with cost savings.681
There is a high level of patient satisfaction with those units that currently offer endoscopy in primary care.698 Currently, no evidence exists to support the clinical and cost effectiveness of such roles,693,699 and the professional view is that they should be additional to, rather than a substitute for, secondary care.699 More research is needed. The problem of training136,700,701 and governance702,703 will need to be examined carefully.
There is, as yet, no published evidence for the safety, clinical or cost effectiveness of undertaking endoscopy or minor gastrointestinal surgery in diagnosis and treatment centres. Research is needed.
Table A.2 summarises the articles examined for primary care.
Table A.2 Developments in service delivery: summary of articles examined for primary care
Secondary services
A review of the literature published between 1980 and 1998 found a paucity of high quality studies that dealt with the effectiveness of specialised care in general hospitals.704 However, there is some evidence that patients admitted with gastrointestinal bleeding, acute pancreatitis, and acute liver disorders fare better when looked after by appropriate specialists.704–707
Six studies looked at access to specialist care; there is a serious underprovision of a colonoscopy service in most NHS hospitals. Training in colonoscopy is often inadequate and improved practice should result from better training. Unless there is a dramatic increase in manpower and resources available for lower GI investigations, the introduction of a national screening programme would rapidly overburden already inadequate facilities.556 A shortage of resources for coloproctology also exists708; some assessments of resource needs have been performed in cancer services.709 Although there is very little evidence on the cost effectiveness of CT colonography, this technique is widely available in the UK, although experience and throughput vary considerably. Limited CT scanner facility is the major barrier to further dissemination.710 There is also some evidence that greater access to specialist paediatric gastroenterology services for children with a suspicion of IBD should be sought.576 None of the above literature included proper economic evaluation, apart from the MINuET study of nurse endoscopy, which concluded that there would be no cost benefit, when compared with doctors.491
Notwithstanding the absence of cost benefit, there is now strong evidence that there should be a shift from doctors to nurses for diagnostic upper and lower GI endoscopy in hospitals.491,560,711–715 Other studies with an economic component which have examined the role of the nurse in undertaking tasks traditionally performed by doctors include upper GI endoscopy,174,529 managing children with GI disease,103 screening for colorectal cancer,716 running dyspepsia clinics,542 and administering propofol during endoscopy.717 Again, none included a proper economic evaluation. Research to evaluate the clinical effectiveness of other professionals in roles traditionally filled by doctors, such as dietician-led coeliac clinics, is needed. The need for governance and accountability issues to be examined as roles change has been emphasised by the BSG.718
Long term follow-up of patients with extensive ulcerative colitis, or patients receiving immunomodulators, or patients with Crohn’s disease is appropriate.584 Colorectal cancer complicating ulcerative colitis is most commonly identified in patients who have been lost to hospital follow-up.719,720
Table A.3 summarises articles examined for secondary services.
Table A.3 Developments in service delivery: summary of articles examined for secondary services
Tertiary services
The Senate of Surgery of Great Britain and Ireland recommends that surgical care should be provided locally, but that patients should be moved to a centre of excellence for further specialist care when appropriate.721 It is the view of professional societies that complex hepatology, hepatobiliary surgery, and liver transplantation should also be delivered in specialist, tertiary centres.214,722 For complex hepatology the expert opinion is that this should be supplemented by clinical networks of specialists in secondary care.214
Many individual studies suggest that complex surgery for cancer, including upper723,724 and lower gastrointestinal,559,560,725 hepatobiliary,373,726–728 and pancreatic malignancy,716,729–732 should be performed at specialist centres which look after larger numbers of patients with these diseases. A systematic review by the NHS Centre for Reviews and Dissemination confirms this view.557 However, an analysis, also from the NHS Centre for Reviews and Dissemination, points out that the evidence comes from methodologically weak studies which do not sufficiently take account of differences in case mix, and thus probably overestimate the impact of volume of activity on the quality of care. It also highlights the fact that there is very little research (and none in the UK) that directly evaluates the effects of mergers on costs.733 An international literature review suggests that it is not possible, on present evidence, to define the optimal configuration of services for oncology.734 A retrospective analysis of routinely collected data by surgeons in a district general hospital concluded that pancreatic surgery could be performed safely in such locations with good short and long term outcomes.735 Conversely, there is no clear evidence that distance from specialist services is associated with poorer outcomes.733
The implications for district hospitals of increasing concentration of specialist services in tertiary centres have not been formally modelled and a detailed review of concentration and choice warns of increasing costs without proven improvements in quality for all patients.733 Other evidence shows that after adjusting for prognosis and treatments, cost-volume relationships become U-shaped, reflecting more active intervention by higher volume doctors along with little activity and long stays for low volume doctors. This non-linear relationship between cost and volume suggest that highly concentrated cancer care might lead to inefficient resource allocation.716 Furthermore, it may denude secondary care of the expertise needed to manage less serious gastrointestinal and hepatic disorders.733 A systematic review of more than 100 studies in the international literature found little evidence to suggest that merging hospitals will result in better patient outcomes.736
Thus the optimum configuration of secondary and tertiary services remains uncertain on present evidence, and it cannot be assumed that improvements in outcome or efficiency will be achieved by increasing the number of patients seen by a unit or individual practitioner through concentration of specialised skills on a single site. An equally valid conclusion is that improvements are derived from better training and experience of practitioners, with access to well trained colleagues in other disciplines, and supported by adequate facilities. An overwhelming conclusion is that high quality research is needed, and that either radical change should await the findings, or be rigorously evaluated as it is implemented.
Table A.4 summarises articles examined for tertiary services.
Table A.4 Developments in service delivery: summary of articles examined for tertiary services
5.3 Patient perspectives on service delivery
Topics discussed at the patients’ workshop centred on four subjects identified from the review of policy and research evidence as of current concern (the brief sent to the participants is attached in Appendix 3):
-
Greater self management by patients
-
Provision of endoscopy services outside hospitals
-
Changing roles: should nurses or doctors carry out endoscopies and care of patients with chronic conditions?
-
Location of services: specialisation versus local care.
Greater self management by patients
Workshop participants were generally positive about the idea of greater self management, which would bring the benefits of a greater sense of control, and reduce anxiety about wasting the time of health professionals. Information and access to services when needed were felt to be key.
“As long as people are informed…[they] are very happy to self manage their conditions; they don’t want to keep going off to hospitals, GPs etc, which are all getting more difficult to see these days anyway (participant 14).
For the access to services, it’s all very well saying “if you’re unwell, give us a call and arrange an appointment”, but if you do that you may not be able to get in through the door.” (participant 21)
Ability to self care was seen as more than simply being informed, however, and concern was expressed about those people who may agree to look after themselves but may not actually be able to achieve this without some support.
“The consultation is 10 or 20 minutes in hospital, how are you able to assess if the person is suitable for self management?” (participant 21)
Flexibility and continuity of care were considered important, with different patients having varying levels of need for support, and a perception that in a self management model, patients may be more likely to be treated by new professionals when they seek care than in a traditional model.
“Continued care is totally lost and frustration comes in for the patient, especially endoscopies. You know, different people doing endoscopies at different visit and giving different information to the patients” (participant 27)
Further to this, concern was expressed that GPs or others coming into contact with a patient attempting to achieve a greater level of self management may not understand the patient’s level of control and may undermine the model.
“I find that difficult because when you go into the hospital you have your plan of treatment and what your input is, and you go to your GP and you don’t get the same level of interaction.” (participant 21)
Provision of endoscopy services outside hospitals
Primary concerns expressed by participants in the workshop centred around risk and safety.
“There’s obviously a risk factor. The one concern is there’s got to be the backup to deal with that and the safety issues that come with it.” (participant 12)
“I have great concerns about this. There are GPs with special interests operating and carrying out endoscopy in smaller hospitals and patients are not offered sedation because, leaving out whether it is safe or not, they don’t have resuscitation facilities.” (participant 14)
Participants were quite cautious about this model, and questioned whether, again, continuity of care would be adversely affected. There was a feeling that it might take time for patients to develop confidence in a system outside hospital.
“just because when you go into an endoscopy unit… it gives you that little bit of reassurance. I suppose it’s just that you’re not used to going down to the GP to have that done, but maybe over time people will get more used to it. There’s bound to be lots of hesitation.” (participant 21)
Some benefits were mentioned, related to local access and quality of facilities:
“I think location has quite a bit to do with it because there are some parts of the country where hospitals are a long way away, whereas the local centre may be down the road. That would affect you and your ability to get to hospital when there’s no public transport and you don’t have a car.” (participant 11)
“Most people that I talk to really accept the diagnostic centres and …think they are excellent because most people do not want to go into hospital and don’t like the atmosphere of hospitals. They find the centres to be more accessible, attractive, comfortable to be in…” (participant 23)
A distinction was made between minor, routine procedures that could be done locally and more complex investigations that needed to be carried out by specialist staff. There was concern that the most important thing was that the operator had the appropriate training and expertise.
“Is there not a difference between what are fairly minor things and very major things where I think most people will travel to a centre of excellence but for a slightly lower level of access? If I had cancer I would want to go to a centre of excellence.” (participant 23)
“Things like screening could be done at GPs for convenience, but anything more than that… needs expertise…in an ideal situation, then yes, I would like the endoscopy done near my home…but under the prevailing conditions, I think it would be dangerous to have a blanket statement saying that it’s safe to do endoscopies in GPs surgeries.” (participant 27)
Changing roles: should nurses or doctors carry out endoscopies and care of patients with chronic conditions?
There was cautious support for changing roles in relation to endoscopies and aftercare, with an emphasis again on training, safety, and continuity of care. The importance of management of the “whole” patient was emphasised, whether this be done by a nurse or doctor.
Although some participants were positive:
“I want to support the role of nurses because they have a good track record in specialist roles in diabetes, cancer.” (participant 25)
there was still some anxiety about the safety of care by nurses:
“Presumably the nurses would have a backup of a doctor within the vicinity while this was taking place should something go wrong? That would be my worry.” (participant 19)
One participant seemed to sum up the feelings of the group:
“At the end of the day the label’s pretty irrelevant in some ways. I could go to a doctor and get really good care and say doctors are brilliant, but you go to the doctor and not be happy. Or you could go to a nurse and it’s brilliant. The label is irrelevant so long as the standard of training is equal to what they are doing.” (participant 21)
Location of services: specialisation versus local care
Views on this topic were mixed, and participants referred to their own experiences of specialist or local care to illustrate associated problems. This was clearly a complex topic, with many considerations and varied personal preferences.
“I think local expertise is important to me… the family has to be involved, it should be easier for them to visit, and should be nearby. For those reasons I am prepared to put up with slightly less expertise, but adequate and safe enough.” (participant 27)
“I’ve had a complicated gastric operation that had to be in [remote specialist centre]. That causes me a lot of problems because I’m isolated from my family and friends and that worries me.” (participant 24)
On the other hand, specialist care was valued by others, even at a distance:
“On a personal level, I’d be happy to go to the specialist centre because I have a specialised condition and I have confidence in the unit that I go to. So I’m prepared to travel rather than go local.” (participant 19)
It was seen as an important subject that may be eventually decided through local and national policy rather than on the basis of research evidence.
“It’s such a major debate, not just for GI… on the whole because the people for local hospitals are so vocal in their campaign, that I think it is going to happen. And that may mean that there won’t be those centres of excellence that there should be. It’s a huge issue which, at the end of the day, will be decided politically.” (participant 23)
Participants understood the complexity of the debate:
“I don’t think taking expertise away from hospitals is a good thing because you are narrowing down the number of people who can get access. Locality is important.”
“I think I’d support that view in terms of access, because if you have to have emergency access and go by ambulance, you may not be able to go to the specialist centre… [but] to the [local] hospital. So if they didn’t have that expertise, it would be a disadvantage, but I agree that complex surgery needs to be done at specialist centres.” (participants 21, 25)
There was concern that some may benefit at the expense of others, with increased specialisation of services.
“I think it’s got the potential of affecting people differently. You take somebody who’s got a diagnosis of mental health, learning, old age, whatever—there’s less likelihood of early diagnosis. The issue of having somebody to support them in hospital may be more of an issue. My concern is that …selection out of particular groups because you have a highly specialised service which doesn’t actually want them…is a price paid by the minority of the population for having a better service for other people.”
Summary of key findings from the patient workshop
Greater self management by patients
-
Cautious support was expressed for greater self management—as long as care was taken to assess the ability of patients to self manage, continuity of care could be maintained, and services could be accessed when required.
Provision of endoscopy services outside hospitals
-
Views were mixed, with benefits of local access being recognised but concerns expressed about safety and continuity of care.
Changing roles: should nurses or doctors carry out endoscopies and care of patients with chronic conditions?
-
Participants agreed that appropriate training and skill level were more important than who delivers care, and the policy was supported if nurses were able to manage the “whole” patient safely.
Location of services: specialisation versus local care
-
Little consensus was reached across the group, with some participants expressing a preference for local care and others valuing specialist care, even at a distance. The needs of minority groups were emphasised.
5.4 Economic burden of GI disease
Studies which attempted to estimate the burden of GI disease tended to focus on individual conditions or on specific elements of the total burden. Only one study483 attempted a comprehensive costing of GI disease. It estimated the total burden in 1997 to be roughly £8000m, which included £3000m to the NHS and personal social services.
A further 20 studies attempted specifically to cost GI conditions: IBD,737,738 IBS,739–741 GI cancer,324 upper gastrointestinal disease (UGI),697,742–744 traveller’s diarrhoea,653 non-specific abdominal pain,745 colic,746 GERD,16 and dyspepsia.747,748 A further paper examined the economic consequences of waiting time for gallbladder surgery.749 Estimated costs are not presented here because of wide variations in the methods used and in the quality of the studies. Even the better studies, such as that on dyspepsia,747 pointed out the limitations of the study’s external validity.
Modelling exercises dominated. Studies which extrapolated local results to the UK as a whole failed to deal with the geographical differentiation across the country. Most used a prevalence based approach, whereas an incidence based approach would have sought to estimate the lifetime costs of managing a cohort of patients first diagnosed in a given year. Most studies were merely “snapshots” based on national statistics and aimed only at indicating the possible scale of the problem without claiming precision. Suggestions for future research focused on ways to improve the quality/accuracy of routinely collected data, and on the need for prospective cohort multicentre studies to confirm results from modelling exercises.
Table A.5 summarises the articles examined for economic burden of GI disease.
Table A.5 Summary of articles examined for economic burden of GI disease
5.5 Cost effectiveness of GI services
One hundred and twenty seven articles examined the cost effectiveness of alternative forms of service delivery. As with the burden of illness studies, these were also of varying quality.
Primary care
Fifteen studies looked at management of GI disease in primary care.
Few studies have examined cost effectiveness and no studies of sufficient power have yet been performed in general practice populations to investigate the role of H pylori and the implication for primary care.582 No attempt has been made to measure quality of life after eradication therapy in patients with peptic ulceration. Further research is needed to quantify the risks and to test the value of screening elderly patients for H pylori before using NSAIDs. To determine whether or not a subgroup of patients with H pylori related chronic gastritis and non-ulcer dyspepsia would benefit from eradication therapy a longer follow-up period is needed. Until this is determined, the treatment of non-ulcer dyspepsia with eradication therapy should remain a research activity.582
The available clinical and economic information about NSAIDs is limited, and the publication of numerous poor quality studies has corrupted the knowledge base. However, there does seem to be enough evidence to indicate that expenditure on NSAIDs could be considerably reduced and adverse effects avoided if practitioners were persuaded to change their behaviour.514 A growing body of evidence suggests that information provision on its own does not lead to substantial changes in practice. More active strategies, such as “academic detailing” using evidence based educational outreach, show promise, but their cost effectiveness has not yet been evaluated rigorously.514
Educational intervention concerning GPs’ management of patients with dyspepsia, to control dyspepsia costs without increasing demand for endoscopy, could lead to a £25m saving each year.750 However, proper multicentre RCTs are needed to support the cost effectiveness of this approach.
It is unclear whether a strategy to test for H pylori and then eradicate it is as cost effective as initial management strategy in primary care. Future trials should evaluate the cost effectiveness of this strategy compared with empirical prescribing.751
The remainder of the studies, although they investigated the management of GI patients in primary care, were mainly based on either qualitative or review work exploring the safety of endoscopy performed in primary care, the effect of guidelines for the management of IBD, the development of GPwSI (GPs with special interests in gastroenterology); a survey of GPs requirements for support from secondary care; the effect of bulletin findings on patient’s management; and the effect of H pylori testing results on referral rate. None of the studies included an economic measurement.
Table A.6 summarises the articles examined for primary care.
Table A.6 Cost effectiveness of GI services: summary of articles examined for primary care
Specialist care
Nine studies looked at access to specialist care; there is a serious underprovision of colonoscopy service in most NHS hospitals. Training in colonoscopy is often inadequate and improved practice should result from better training. Unless there is a dramatic increase in manpower and resources available for lower GI investigations, the introduction of a national screening programme will rapidly overburden already inadequate facilities.752 There is a shortage of resources for coloproctology753; some assessment of resource needs has been performed in cancer services.754 Although there is very little evidence on the cost effectiveness CT colonography, this techniques is widely available in the UK; however, experience and throughput varies considerably. Limited CT scanner facility is the major barrier to further dissemination.755 There is also some evidence that greater access to specialist paediatric gastroenterology services for children with suspected IBD should be sought.756
None of the above publications included a proper economic evaluation.
Table A.7 summarises the articles examined for access to specialist care.
Table A.7 Cost effectiveness of GI services: summary of articles examined for access to specialist care
Role of nurses
Four studies with an economic component examined the role of nurses in performing a variety of GI services, including upper GI endoscopy,712 managing children with GI disease,757 screening for colorectal cancer,758 running dyspepsia clinics,759 administering propofol during endoscopy.717 Again, none included a proper economic evaluation. A multicentre RCT comparing nurses and doctors undertaking diagnostic upper and lower GI endoscopy has shown that doctors are more cost effective than nurses in carrying out these procedures.491
Table A.8 summarises the articles examined for the role of nurses in GI services.
Table A.8 Cost effectiveness of GI services: summary of articles examined for the role of nurses in GI services
Home parenteral nutrition
Two studies760,761 looked at the cost effectiveness of home parenteral nutrition (HPN). There is some evidence that home parenteral nutrition (HPN) is a cheaper alternative than hospital care. No economic evaluations of HPN for malignant disease and AIDS have been made.760
Table A.9 summarises the articles examined for HPN.
Table A.9 Cost effectiveness of GI services: summary of articles examined for home parenteral nutrition
Surveillance programmes
Nine articles with an economic component were identified. Intensive follow-up after resection for colorectal cancer was shown to be more effective and more cost effective than conventional follow-up,601 producing an incremental cost for each life year saved of £3402 over conventional follow-up. This is very low compared with other life extending interventions, indicating that on economic grounds, intensive follow-up after curative resection for colorectal cancer should become normal practice. Large RCTs are needed to evaluate the cost effectiveness of specific surveillance tools.
A number of economic modelling exercises have examined population screening/eradication programmes for H pylori. One modelling exercise estimated that a programme to screen for and eradicate H pylori in a population of one million 45 year olds would produce an incremental cost for each life year saved of £14 200,614 which again is low compared with other life extending programmes. Another619 showed that population screening for H pylori was a cost effective way of preventing gastric cancer and peptic ulcer disease, producing an incremental cost for each life year saved at age of 40 of £5860, but this result was sensitive to H pylori prevalence, the degree of opportunistic eradication, the discount rate, the efficacy of eradication on gastric cancer risk, the risk of complicated peptic ulcer disease and gastric cancer associated with H pylori infection, and the duration of follow-up. Many assumptions are required in modelling exercises of this type. However, when these assumptions were varied in sensitivity analyses, the incremental cost for each life year saved rarely exceeded £20 000 over an 80 year follow-up, although it did for shorter periods. Population H pylori screening may be cost effective in the long term (over 25 years). However, before it can be recommended further evidence is needed to resolve some of the uncertainties, particularly about the efficacy of eradication on risk of gastric cancer, the risk associated with complicated peptic ulcers, and the effect of more widespread opportunistic testing of patients with dyspepsia. The long duration between the age of screening and the incidence of gastric cancer means that screening does not become cost effective for several decades. Before screening can be recommended on economic grounds further evidence is needed to resolve some of the uncertainties, particularly with regard to the time horizon and the discount rate.
Table A.10 summarises the articles examined for surveillance programmes.
Table A.10 Cost effectiveness of GI services: summary of articles examined for surveillance programmes
Dyspepsia and endoscopy
Quite a few studies examined endoscopy. One used modelling to examine a wide range of different situations in which endoscopy is given for patients with dyspepsia.34 Results showed that endoscopy is not cost effective in patients with low risk of malignancy, but targeting had major impacts on cost effectiveness ratios. Restricting endoscopy to those with continuous epigastric pain or symptoms of less than one year’s duration, or both, improved the incremental cost for each life year saved from £50 000 to £8400. Estimates of incremental cost per life year saved for men of various ages ranged from £454 000 at age 40 to £15 779 at age 70. Results for women showed similar reductions at older ages, which provides good evidence of the need to restrict endoscopy in younger age groups.34 When the initial strategies for managing dyspepsia were examined, a comparison of early endoscopic investigation with acid suppression showed that the cost of additional endoscopies was offset by a significant reduction in the number of PPIs prescribed and outpatient attendance. The overall management cost of prompt endoscopy was £420 compared with £340 for empirical management.697
Table A.11 summarises the articles examined for dyspepsia and endoscopy.
Table A.11 Summary of articles examined for dyspepsia and endoscopy
This review shows that economic evidence on the delivery of GI services is patchy and of variable quality. Very few studies were full economic evaluations and the limited economic evidence they produced—for example, of potentially large cost savings to be gained by changing from one model of service delivery to another—emphasises the need for comprehensive economic evaluations in this area.
Summary points
-
Multicentre studies are needed
-
Studies should take the societal perspective
-
Methodological problems/challenges of economic evaluations of primary/secondary care interphases have been highlighted
-
Insufficient evidence is available to support a positive correlation between volume and patients outcomes. This relationship needs further assessment.
Table A.15, Appendix 4, lists the references not used for the economic review and the reason why.
5.6 Information infrastructure
The requirements for information and IT support for gastroenterology have been published by the British Society of Gastroenterology.762 This describes the need for patient focused records that will provide access to appropriate information in the increasingly wide variety of contexts in which patients will receive health care, including self management. The most pressing immediate need is for universal support for the widespread introduction of systems to support gastrointestinal endoscopy. The requirements include booking, patient information, consent, results, reporting, and quality assurance. A survey of gastrointestinal units in 2001 found that one third of respondents from the UK were still using paper reporting systems.763 Many other aspects of gastroenterology need better information support, including all contacts with professionals and specific clinics, where acquisition of data should be used to monitor quality of care. It is hoped that patient focused systems will be developed in the future, which will enable support for patient care through a wide variety of situations in which the patient receives care.
There is presently no national dataset to enable comparative monitoring of activity and performance in gastroenterology. There are concerns about the quality of routinely captured data.11 Common standards for records and for data collection are needed to improve this,764 and to enable performance monitoring, monitor quality and training, inform service developments, and enable high quality clinical and health services research.765 There is evidence that routinely captured clinical data would enable health technology assessment by RCT if the data were more widely available and of improved validity.766,767 The data required to support gastrointestinal endoscopy are available on the British Society of Gastroenterology website (http://www.bsg.org.uk, accessed 26 December 2006), and requirements are being developed for other areas of the specialty.
6. DISCUSSION
6.1 Strengths and weakness of methods used
As detailed in the methods chapter and at the start of each chapter, four main methods of data collection were used to gather evidence for this review: review of published evidence; use of routinely available data; patient workshop; and consultation with professionals in gastroenterology. The strengths and weaknesses of each of these methods are considered below, with implications for strength of recommendations made in this report assessed in section 6.2.
Review of published evidence
As we applied currently defined and accepted standards to the review of effectiveness of service delivery, this section of the report is comprehensive and systematic. Validated tools were used to assess the quality of papers and level of evidence provided, with more than one reviewer independently grading papers. Full details of the search and of papers retrieved are presented through search results and tables. Other sections of the report are comprehensive and have retrieved key data and publications, although the methods used to identify sources have relied to some extent on existing knowledge and collections of materials. With extensive feedback sought from a variety of specialist professional and patient groups it is unlikely that key sources have been either overemphasised or overlooked.
Routine data
Several main sources of routine data were used in compiling this report: cancer surveillance and registry units across the UK; the Office of National Statistics (ONS) and its predecessor, the Office of Population Censuses and Surveys (OPCS); the Department of Health; and communicable disease surveillance units across the UK. In addition to well described generic limitations of routine data, the different data sources have their own particular strengths and weaknesses.
Limitations of cancer surveillance and registry data include concerns about variability in case ascertainment and completeness of registrations over time and between different registry regions. The major limitation of mortality data from the ONS and the OPCS is that it is based on underlying cause of death alone, and therefore underreports true mortality for many gastrointestinal diseases; major concerns have also been raised about the accuracy and completeness of hospital episode statistics from the Department of Health. The main limitation of data on hepatitis B and C infections from communicable disease surveillance units is that they are based on reported laboratory diagnoses only. As most people who are infected with these viruses are undiagnosed, the reported laboratory data are thought to account for only about one quarter of all cases.
Despite these limitations, these are the best data that are available for portraying the burden of gastrointestinal disease in the UK. Coverage is national, with standardised definitions and inclusion criteria agreed. They have provided the empirical basis for many publications in scientifically acclaimed international clinical journals, as well as National Service Frameworks and other policy documents.
Patient workshop
The limitations of the focus group carried out with patient representatives recruited from the RCP volunteers are acknowledged. The views reported in this document can only be taken to represent a flavour of the views of patients. Participants included patients and patient representatives, who were perhaps unusually articulate and able to interact as members of a group. Nevertheless, the findings complement the review findings, presenting a different side of the picture on the problems of service delivery arrangements that are currently undergoing change, which were discussed at the workshop.
Consultation with professionals from within the specialism of gastroenterology
Feedback has been sought through the BSG membership, and other societies, and has been collated from individual responses as well as from a wide range of specialty and patient groups that support the care of patients with GI disorders. Only that feedback which was supported by further evidence has been incorporated.
6.2 Strengths and weaknesses of evidence presented in report
Using a mixed methods approach in this review has allowed any weaknesses inherent in one method to be complemented by the strengths of another approach.
The systematic review of effectiveness of models of service delivery has been enriched through contextualisation, with the national policy agenda described; presentation of data describing burden of disease, current activity, economic costs, and workforce implications; and the views of patients and professionals represented. This has allowed a comprehensive document to be developed. Some aspects of the review—such as the perspective of patients to current developments in service delivery—would be more comprehensively and rigorously pursued through primary research, and the data presented in this report can only be taken as a taster of views. This has resulted in recommendations for further research, as existing evidence is thin. Indeed, an overwhelming conclusion of the report is that the evidence base for the development of services needs to be strengthened before further investments are made in shaping the delivery of services.
6.3 Research in gastroenterology
Although over 900 references have been used to inform this review, the evidence identified has often been weak and there are many gaps in areas where evidence is needed. The annual reports of the Health Technology Assessment and NHS Service Delivery and Organisation Research Programmes document relatively few studies in gastroenterology.
A coordinated approach to clinical and health services research in gastroenterology, such as the one being introduced for cancer, in gastroenterology would improve the identification of research questions and priorities, funding strategies, patient and carer involvement, and the research infrastructure. It is hoped that the UK Clinical Research Collaboration will promote and enable more research into the diagnosis, treatment, and care of patients with GI and hepatic disorders.
7. CONCLUSIONS
7.1 Burden of disease
-
The burden of gastrointestinal and liver disease is heavy for patients, the NHS, and the economy (sections 3.2–3.4, 3.7, 4.3–4.5, 4.7.2, 4.7.3, 5.5).
-
Gastrointestinal disease is the third most common cause of death, after circulatory and respiratory disease (section 3.3).
-
Gastrointestinal cancer is the leading cause of death from cancer (section 3.3).
-
Gastrointestinal disease is the most common cause of admission to hospital for both the total number of people admitted and the total number of episodes of care (section 4.3).
-
There have been large increases in the incidence of liver diseases, such as alcoholic liver disease, non-alcoholic fatty liver disease, biliary cirrhosis, and hepatitis C infection, which have major implications for future healthcare needs (section 3.2).
-
There have also been increases for most other gastrointestinal diseases—in particular, for oesophageal and colorectal cancers, acute and chronic pancreatitis, gallstone disease, upper gastrointestinal haemorrhage, diverticular disease, and Barrett’s oesophagus (section 3.2).
-
Chronic gastrointestinal disorders such as dyspepsia, gastro-oesophageal reflux disease, and irritable bowel syndrome are highly prevalent; and coeliac disease is far more common than previously considered (section 3.2).
-
Socioeconomic deprivation is linked to a number of gastrointestinal diseases, including increased risks of gastric and oesophageal cancers, hepatitis B and C infections, liver cirrhosis, peptic ulcer, upper gastrointestinal haemorrhage, and poorer prognosis for colorectal, gastric, and oesophageal cancers (section 3.6).
-
There is substantial variation in the incidence and prevalence of many gastrointestinal disorders in the UK. For example, peptic ulcer, Helicobacter pylori infection, upper gastrointestinal haemorrhage, alcoholic liver disease, acute pancreatitis, and oesophageal cancers are all more common in Scotland and northern England than in southern regions (section 3.5).
-
Impact on patients is neither fully nor accurately reflected in statistics describing mortality and activity (sections 3.3, 4.3).
-
The burden on patients health related quality of life has been found to be substantial for their symptoms, activities of daily living, and employment (section 3.4).
-
Conditions with a high level of disruption to patients’ lives include: gastro-oesophageal reflux disease (GORD), dyspepsia, irritable bowel syndrome, anorectal disorders, GI cancers, and chronic liver disease (section 3.4).
-
Overall, the burden of GI disease on health related quality of life (HRQoL) in the general population seems to be high, although the burden is not systematically nor comprehensively described (section 3.4).
7.2 Service delivery
-
An extensive and systematic study of the problem of access for the delivery of GI services has yet to be carried out (section 4.6.1; level of evidence: 2− at best).
-
There is a lack of significant literature relating to inequalities in the delivery of GI services (section 4.6.2; level of evidence: 4).
-
Waiting times form the bulk of patients’ concerns. There seems to be great difficulty in meeting government standards for referral and treatment (section 4.6.3; level of evidence: 2− at best, and guidelines by the Association of Coloproctology of GB and Ireland).
-
Most studies show that GI related drugs and procedures are safe. There is a need for more research on the safety of patient initiated drugs and procedures for the treatment of GI disease (section 4.6.4; level of evidence: 1).
-
There is a need to increase awareness and the implementation of initiatives aimed at improving the information flow between patients and practitioners (section 4.6.5; level of evidence: 2− at best).
-
There is a strong body of evidence on diagnostic services, and the need to develop and implement appropriate training and stringent assessment to ensure patient safety (section 4.6.6; level of evidence: 2+).
-
There is a substantial amount of work detailing guidelines for care, but there is a distinct paucity of rigorous, evidence based studies dealing with service provision (section 4.7.1; level of evidence: 1).
-
There is strong support for the development and use of widespread screening programmes for a wide variety of GI diseases. These need to be properly researched to determine how they are managed, their effectiveness, and their cost effectiveness (section 4.7.4; level of evidence: 1, section 5.5).
-
Emphasis should be given to developing interventions to increase preventative activities in primary care, and more research to determine their effectiveness and cost effectiveness (section 4.7.6; level of evidence: 1).
-
More research is needed to establish a robust evidence base for models of service delivery (section 5.2).
-
Overall there remains a paucity of cost effectiveness evidence particularly from multicentre studies in GI service delivery (section 5.5).
-
There is strong evidence for a shift in care towards greater patient self management for chronic disease in appropriate circumstances, and supported by adequate circumstances and access to services (section 5.2; level of evidence: 1).
-
The development of GPs with a special interest in gastroenterology is supported in primary care but the clinical and cost effectiveness needs to be researched (section 5.2).
-
In hospital, patients with gastrointestinal disorders should be looked after by specialists (section 5.2; level of evidence: 2+).
-
More diagnostic endoscopy should be undertaken by trained nurses, although such procedures are not more cost effective than when carried out by doctors (section 5.2; level of evidence: 1).
-
Complex surgery for gastrointestinal and hepatobiliary cancer should be performed by specialists who operate on large numbers of patients (section 5.2; level of evidence: 2+).
-
There is insufficient evidence to support a greater concentration of specialists in tertiary centres. More research is needed, especially on the impact on secondary services, before further changes are implemented (section 5.2; level of evidence: 2+).
-
The solution proposed for hepatology is to combine tertiary specialist centres for complex liver disease and transplantation with a network of specialists in secondary care, but we found no evidence for the clinical or cost effectiveness of this approach (section 5.2; level of evidence: 4).
-
There is an urgent need for better IT and information support for clinical care in gastroenterology (section 5.6; level of evidence: 2−).
7.3 Workforce
-
Consultant gastroenterologist numbers need to increase to about 1900 posts (1625 WTE). Six consultants are required to provide full services and emergency cover for a typical district general hospital population of 250 000 (section 4.2; level of evidence: 2−).
-
Gastroenterology teams led by consultants, but including appropriate non-consultant career grade staff, dieticians, and specialist nurses, need to be developed in all hospitals, with integrated specialist training where appropriate (section 4.2; level of evidence: 4).
-
More nurses should be trained to undertake upper and lower diagnostic endoscopy (section 5.2; level of evidence: 1).
7.4 Future research
More research is needed into delivery and organisation of services for patients with gastrointestinal and liver disorders, in particular:
-
The clinical and cost effectiveness of GPs with a special interest in gastroenterology and endoscopy (section 5.2).
-
The clinical and cost effectiveness of undertaking endoscopy or minor gastrointestinal surgery in diagnostic and treatment centres (section 5.2)
-
The reconfiguration of specialist services and the potential impact on secondary and primary care and on patients (section 5.2)
-
The clinical and cost effectiveness of clinical networks (section 5.2).
-
The relationship between volume and patient outcome needs further assessment (section 5.2).
-
To account for geographical differences, future research should be based mainly on multicentre studies.
The establishment of the UK Clinical Research Collaboration will provide an opportunity to increase clinical and health services research in gastroenterology. It is important that the investment that is being made supports the growth of research into the care of diseases which are responsible for high morbidity and mortality, and are a significant burden on the patient, the NHS, and the economy (section 6.3).
8. ANNEX: SUMMARY OF ARTICLES USED
Note on methodology – rationale for presentation of results in tables
The review of evidence of effectiveness of service delivery arrangements followed the CRD methods for systematic reviewing, with the primary literature search designed to identify papers concerned with service delivery. Results of the search are presented in section 5.2. All papers identified through this search were screened, and those that were relevant to any section of the report were summarised and graded. Papers cited in section 5.3, concerned with effectiveness of models of service delivery, are matched with tables (A.1–A.11) which provide further details of the research setting, study design, and key results, as well as their AGREE score and grading for level of evidence where relevant.
Additional papers for other sections of the report were identified through topic-specific searches (burden of disease; quality of life; health economics of GI) and through existing collections of publications. These papers are included, where relevant, in various sections of the report, and where identified through the primary literature search are matched in summary table A.12. Table A.13 summarises the articles examined after consultant feedback.
Table A.12 Summary of articles identified through systematic search by section
Table A.13 Summary of articles examined after consultation feedback
9. APPENDICES
Appendix 1: Charities with an interest in the care of patients with gastroenterological and liver disorders (through patient support or research or both)
Appendix 2 AGREE tool for quality assessment
Score each of the following questions using a three-point Likert scale:
-
0—Not specified (little or no evidence)
-
1—Disagree (some evidence)
-
2—Agree (good or strong evidence)
Scope and purpose:
-
The overall objective(s) of the research is (are) clearly described.
-
The research question(s) covered by the methodology is (are) clearly described.
-
The recipients to whom the research is meant to apply are clearly described.
Stakeholder/participant involvement:
-
The research is carried out by relevant professional groups.
-
The participants’ views and preferences have been sought.
-
The target users of the research are clearly defined.
-
The research has been piloted among participants.
Rigour of development:
-
Methods to search for evidence have been specified (for example, systematic review, unbiased screening, search strategy).
-
The techniques for formulating the results have been specified.
-
The advantages, disadvantages, and risks are considered in the results.
-
There is an explicit link between the results and the supporting evidence (sufficient relevant references).
-
The research has been externally reviewed before its publication, or published in peerb reviewed sources.
-
A procedure for updating the research is provided, or for primary studies, a clear indication of what further research is needed.
Clarity and presentation:
-
The results are clear and unambiguous.
-
The different options for conducting the research are clearly presented, or for primary studies, a description of the pros and cons of each method.
-
Key points in the results are easily identifiable.
-
The research is supported with tools for application (for example, computer support, documentation, reference guide for reviews/guidelines), or for primary studies, a clear path for dissemination and potential implementation.
Applicability:
-
The potential barriers in applying the results have been discussed.
-
The potential cost implications of applying the results have been considered.
-
The research presents key (review) criteria for monitoring and/or audit purposes (for example, cost should be <£100; time <7 days).
Editorial independence:
-
The research is editorially independent from the funding body.
-
Conflicts of interest among research members have been recorded.
Appendix 3: Brief sent to participants for the patient workshop
Specific questions to be answered
(a) Greater self management by patients
There is good evidence to show that if patients with chronic illnesses such as inflammatory bowel disease or irritable bowel syndrome are given enough information and are supported by expert services that are easy to reach, they can manage with fewer hospital and GP appointments. This could be used for a wide variety of chronic illnesses, which would reduce demand on NHS services.
What is your view on such an approach?
(b) Endoscopy outside hospitals
It has been suggested that more endoscopies (internal examination of the gut through a tube) should be carried out in special centres or in local GP surgeries instead of hospital, which may be easier for patients but may mean that these tests would be less available in hospital. Research is needed to find out whether these tests would be safe and effective, if undertaken outside hospitals.
What is your view on such tests being carried out in places other than hospitals?
(c) Nurses or doctors?
There is good evidence that nurses do a good job when undertaking endoscopy to help make a diagnosis. Also, patients prefer nurses doing the test to doctors. This suggests that nurses should take over routine diagnostic endoscopy from doctors. There is some evidence (that is less strong) that nurses should also take over the continuing care of certain patients with chronic gastrointestinal problems.
What would you feel about seeing a nurse rather than a doctor for these tests and appointments?
(d) Where should services be located?
There is some evidence that major operations for gastrointestinal problems should be performed at specialist centres that serve large populations because the results may be better. However, this would take away expertise from local hospitals, where specialist care will still be needed, particularly for emergency problems.
What is more important to you—having services available locally or being treated by specialists, even if it is further away?
Open discussion
What else would be important to you about the way services for gastrointestinal problems are provided?
Appendix 4: Articles not used in this report
Table A.14 lists the articles not used in this report, and table A.15 the articles not used for economic analysis.
Table A.14 Articles not used in this report
Table A.15 Articles not used for economic analysis
Appendix 5: Glossary
Table A.16 Glossary
Appendix 6: Specialists who provided comments and feedback
Table A.17 Specialist who provided comments and feedback
Acknowledgments
10.
We are grateful to the British Society of Gastroenterology (BSG) for funding this project and to the BSG Steering Group (Dr Mike Hellier, Professor Elwyn Elias, Dr Tony Morris, and Dr Jeremy Sanderson) for providing additional commentary and feedback throughout its development. We are also grateful to the many other colleagues who have given constructive feedback on the draft report. We thank Professor Michael Goldacre and the Unit of Health-Care Epidemiology, University of Oxford, for the provision of linked hospital admission data, and Lori Havard and other members of the UWS Library and Information Services who obtained references for us. We would like to acknowledge the contribution of Professor Robert Allan, who was the inspiration for the development of a strategic view of services in gastroenterology during his time as president of the British Society of Gastroenterology. Dr Michael Hellier took up this challenge when he was elected president, and we would also like to acknowledge the encouragement and support he has given us.
11. Principal team members
This study was conducted during 2004–05. Principal team members were:
Dr Faiz Ali, specialist registrar in gastroenterology/research fellow, Centre for Health Information, Research and EvaLuation (CHIRAL), School of Medicine, University of Wales Swansea.
Dr Wai-Yee Cheung, senior lecturer in health service research, Centre for Health Information, Research and Evaluation (CHIRAL), School of Medicine, University of Wales Swansea.
Professor David Cohen, professor of health economics, School of Care Sciences, University of Glamorgan.
Mrs Gaynor Demery, personal assistant to Professor John Williams, School of Medicine, University of Wales Swansea.
Dr Adrian Edwards, reader in primary care, Centre for Health Information, Research and Evaluation (CHIRAL), School of Medicine, University of Wales Swansea.
Mrs Margot Greer, library and information services manager, National Public Health Service.
Dr Mike Hellier, president, British Society of Gastroenterology.
Dr Hayley Hutchings, statistician, Centre for Health Information, Research and Evaluation (CHIRAL), School of Medicine, University of Wales Swansea.
Dr Barry Ip, research officer, Centre for Health Information, Research and Evaluation (CHIRAL), School of Medicine, University of Wales Swansea.
Mrs Mirella Longo, research fellow, School of Care Sciences, University of Glamorgan.
Dr Stephen Roberts, lecturer of epidemiology, Centre for Health Information, Research and Evaluation (CHIRAL), School of Medicine, University of Wales Swansea.
Professor Ian Russell, professor of public health and director of Institute of Medical and Social Care Research, University of Wales Bangor.
Dr Helen Snooks, senior lecturer in health and social care research, Centre for Health Information, Research and Evaluation (CHIRAL), School of Medicine, University of Wales Swansea.
Professor John Williams, Project leader, consultant gastroenterologist/professor of health services research, Centre for Health Information, Research and Evaluation (CHIRAL), School of Medicine, University of Wales Swansea.
Mrs Judy Williams, clerical officer, Centre for Health Information, Research and Evaluation (CHIRAL), School of Medicine, University of Wales Swansea.
12. Contributors
Dr Giles Croft, research fellow, Royal College of Physicians iLab, School of Medicine, University of Wales Swansea.
Dr Ian Frayling, director, all Wales Genetics Laboratory Service and consultant in genetic pathology, Institute of Medical Genetics, University of Wales Cardiff.
Ms Norma McGough, Coeliac UK.
Dr Alistair McIntyre, consultant gastroenterologist, Wycombe General Hospital, High Wycombe.
Dr Roland Valori, consultant gastroenterologist, Gloucester.
Professor Anne Williams, professor of nursing, School of Health Science, University of Wales Swansea.
Members of the Patient and Carer Network, Royal College of Physicians, London.
Mr Richard Driscoll, National Association for Crohn’s and Colitis.
REFERENCES
- ↵
- ↵
- ↵
- ↵
-
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
-
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
-
-
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
Footnotes
-
Competing interests: This was an independent study undertaken by the School of Medicine of the University of Wales Swansea, in collaboration with colleagues at the University of Glamorgan and University of Wales Bangor. Professor John Williams, Dr Mike Hellier, Dr Alistair McIntyre, and Dr Roland Valori are practising gastroenterologists and members of the British Society of Gastroenterology. Dr Hellier is currently president of the Society (2004–05). Dr Faiz Ali is a trainee in gastroenterology.
-
All rights reserved. No part of the publication may be reproduced, stored on retrieval system or transmitted in any form or by any means, electronic, mechanical photocopying, recording or otherwise, without the prior permission of the copyright, except for brief, acknowledged quotations embodied in critical articles or reviews. ©University of Wales Swansea.
Published by the Centre for Health Information, Research and Evaluation, School of Medicine, University of Wales Swansea, SA2 8PP. ISBN – 1-85987-017-1
Team roles
Professor John Williams led the project throughout, devised the original research proposal, wrote some sections and edited the report. Professor Ian Russell and Professor David Cohen provided invaluable advice and guidance on the development of research methodology, and wrote or edited some sections.
Dr Helen Snooks was responsible for the day-to-day management of the project, provided methodological input and analyses, and wrote some sections. Dr Adrian Edwards and Mrs Margot Greer gave advice on the systematic literature search. Dr Hayley Hutchings and Dr Wai-Yee Cheung provided methodological and statistical input. Dr Stephen Roberts, Dr Faiz Ali, and Dr Barry Ip provided methodological input and analyses, reviewed the literature and wrote various sections. Working with Professor David Cohen, Ms Mirella Longo carried out economic analyses, reviewed the health economics literature and wrote the health economics sections.
Mrs Gaynor Demery and Mrs Judy Williams provided clerical support. Mrs Anne Seagrove proof read the report. Mrs Kymberley Thorne assisted with the appraisal of the research literature.