Article Text

Statistics from Altmetric.com
ROLE OF IMPAIRED BILE ACID ABSORPTION IN POST-INFECTIVE GUT DYSFUNCTION

Infection with Trichinella spiralis induces acute inflammation that resolves as the worms leave the gut, 1–2 weeks post infection. Although the inflammation subsides, persistent abnormalities remain which have been used as a model of post-infectious irritable bowel syndrome (PI-IBS). The current study showed that 18 days post infection there was a striking increase in ileal secretion, both basal and bile acid-stimulated. This was associated with a marked reduction in bile acid absorption but paradoxically an increase in expression of the apical sodium dependant bile acid transporter (ASBT). While bile acid malabsorption (BAM) had resolved 1 week later, ileal water absorption remained depressed. The bowel distal to the ileum, which BAM would cause to be exposed to increased bile acids, continued to show increased basal secretion at 25 days, though the response to bile acids appeared depressed, possibly a compensatory mechanism. The authors speculate that increased delivery of bile acids to the colon may contribute to colonic hypermotility and secretion, and hence some of the symptoms of PI-IBS.
See pages 41
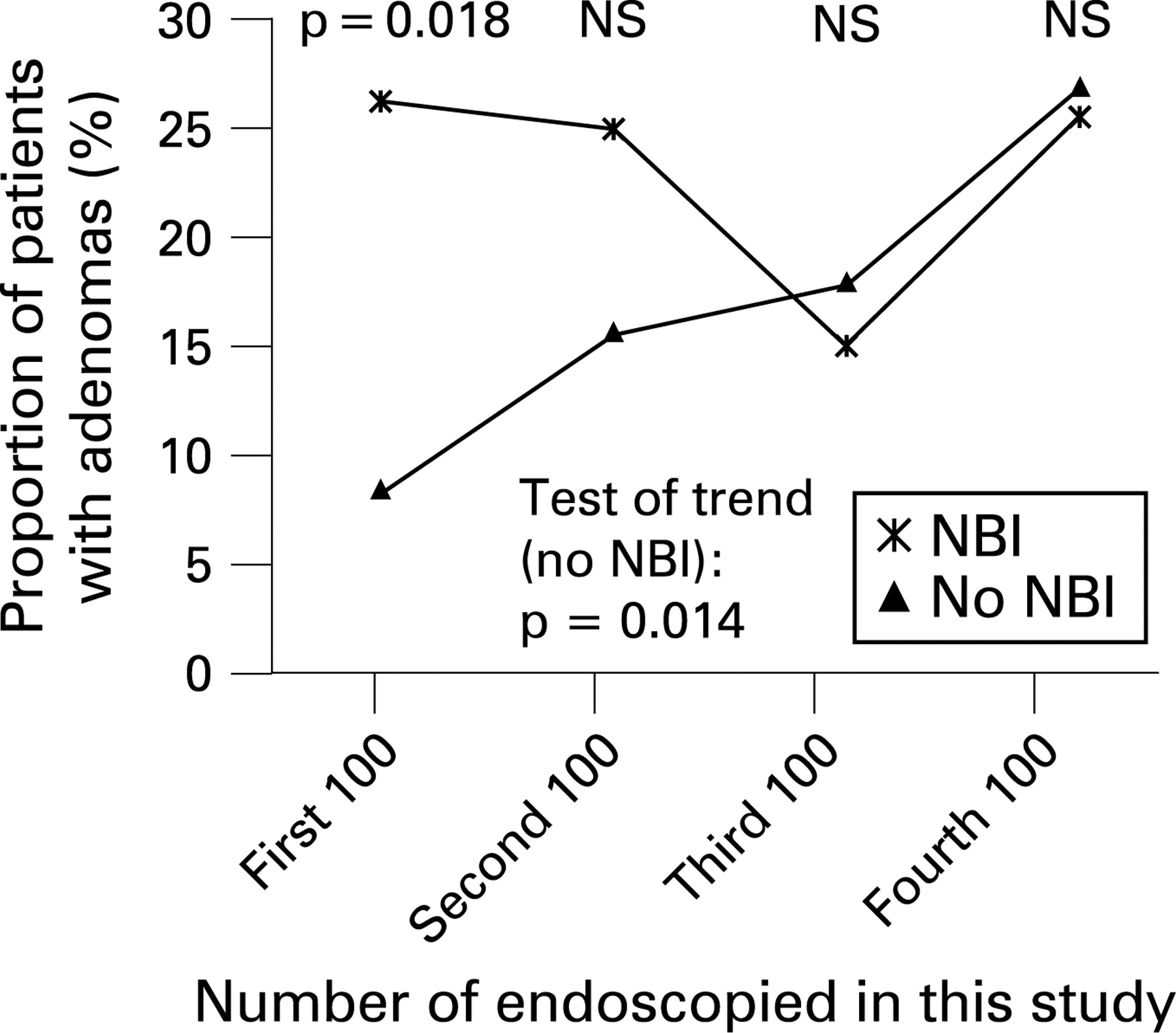
IMPROVING POLYP DETECTION BY NARROW-BAND IMAGING: A LEARNING EFFECT?

Much attention has recently been given to improving the detection rate of polyps at colonoscopy. Narrow-band imaging (NBI) uses special filters to exclude red frequencies so that vascular structures appear black, thereby enhancing contour detection. The present study randomised patients undergoing colonoscopy to either conventional high-resolution or NBI colonoscopy. A total of 401 patients were examined by seven experienced examiners with a caecal intubation rate of 98%. There was a striking difference in detection rate of all polyps between NBI (41.4%) and conventional imaging (25.8%) (p<0.001). The difference for adenomatous polyps was less, 22.7% versus 16.7% respectively (p = 0.13), but more for hyperplasic polyps, 28.3% versus 11.6% (p<0.0001). There was a striking time trend (see fig) which showed that the difference between NBI and controls was much greater in the first 100 endoscopies, disappearing in the third 100 cases. This suggests that improved results with conventional high-resolution endoscopes can be obtained by training using NBI and that these benefits will persist.
See pages 59
LONG-TERM OUTCOME OF CHRONIC HEPATITIS B IN CAUCASIAN PATIENTS: MORTALITY AFTER 25 YEARS

This unique study from Padova enrolled 70 hepatitis B patients between 1972 and 1984, who were positive for both surface antigen (HBsAg+) and e antigen (HBeAg+). Follow up was achieved at least annually, and all but two of the 70 were traced for a median of 25 years. Eighty-seven per cent underwent spontaneous HBeAg seroclearance in the first 10 years. The nine who failed to clear were older and more likely to have cirrhosis. Twenty-one of the 61 with HBeAg seroclearance continued with active hepatitis, one with HBeAg reversion and eight with co-infections with hepatitis C and or D. Twenty-five year survival was significantly worse in those with HBeAg persistence or those with persistent hepatitis of any cause (see fig). Forty inactive carriers had normal ALTs and low levels of HBV DNA, with 18 of them also losing HBsAg. The study demonstrates that the majority of patients with chronic hepatitis B become inactive carriers after spontaneous HBeAg seroconversion, which significantly decreases the risk of liver-related mortality.
See pages 84
ASSOCIATION OF GASTRIC LEPTIN WITH OESOPHAGEAL INFLAMMATION AND METAPLASIA
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Gastric leptin has been shown to contribute to both mucosal homeostasis and abnormal proliferation. The relationship of leptin to oesophageal pathophysiology has not been studied. Francois et al evaluated the presence of leptin receptors in human oesophageal mucosa in normal, inflamed or Barrett’s tissue, and determined whether circulating or gastric leptin levels were associated with particular oesophageal pathology. Receptors for leptin were highly expressed on oesophageal epithelial cells, with similar density and staining pattern in all three conditions, and plasma and antral leptin levels did not differ significantly. Patients with Barrett’s had significantly higher fundic leptin levels compared with normal or inflamed oesophagus. In multivariate analysis, for every twofold increase in fundic leptin, the odds of having Barrett’s was 3.4 times (95% CI 1.5 to 7.6) higher compared with having a normal oesophagus (see table). The authors conclude that leptin receptor expression on oesophageal epithelial cells provides a pathway for leptin-mediated signal transduction, and that variation in gastric leptin production could contribute to differential oesophageal healing and metaplasia progression.
See pages 16
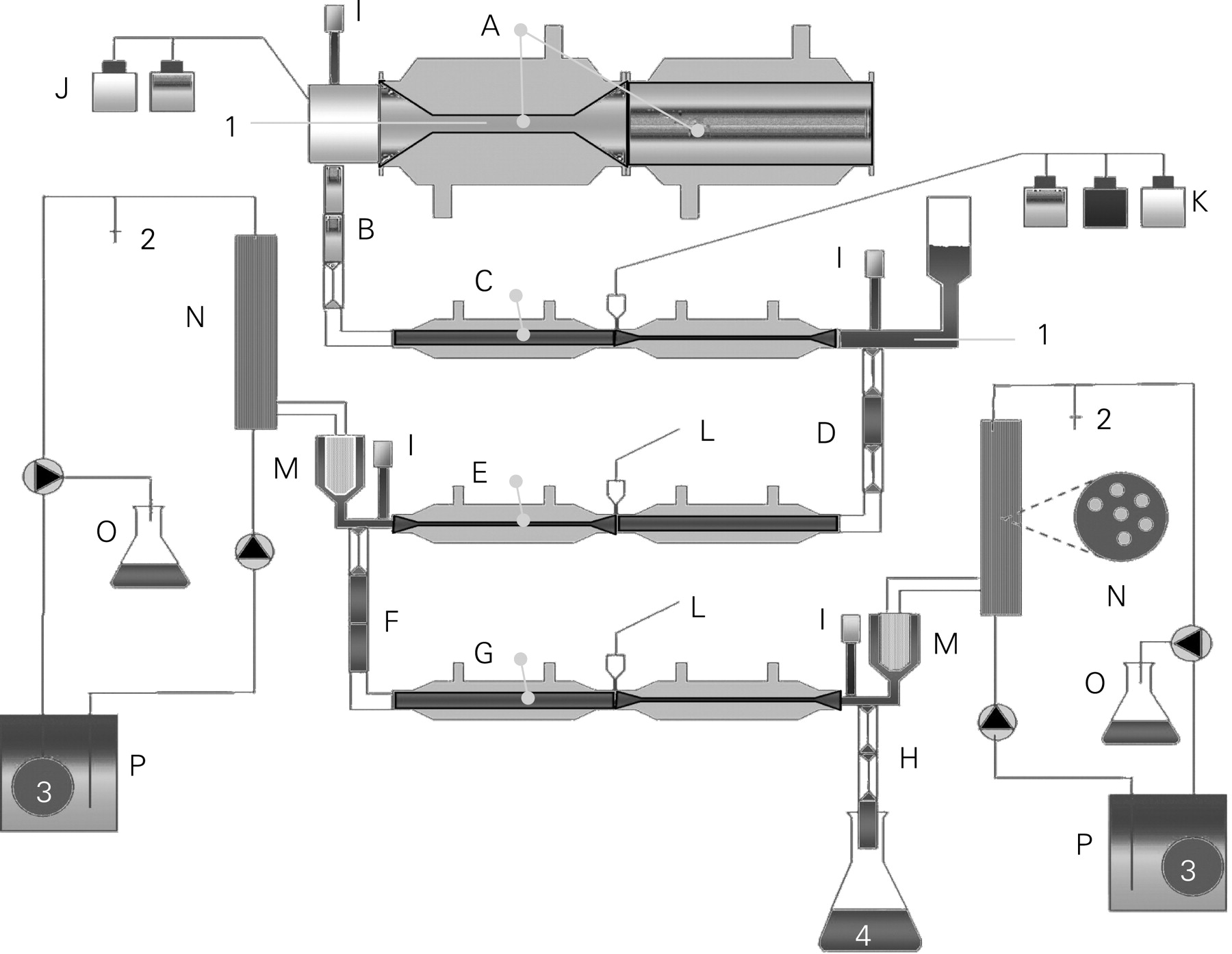
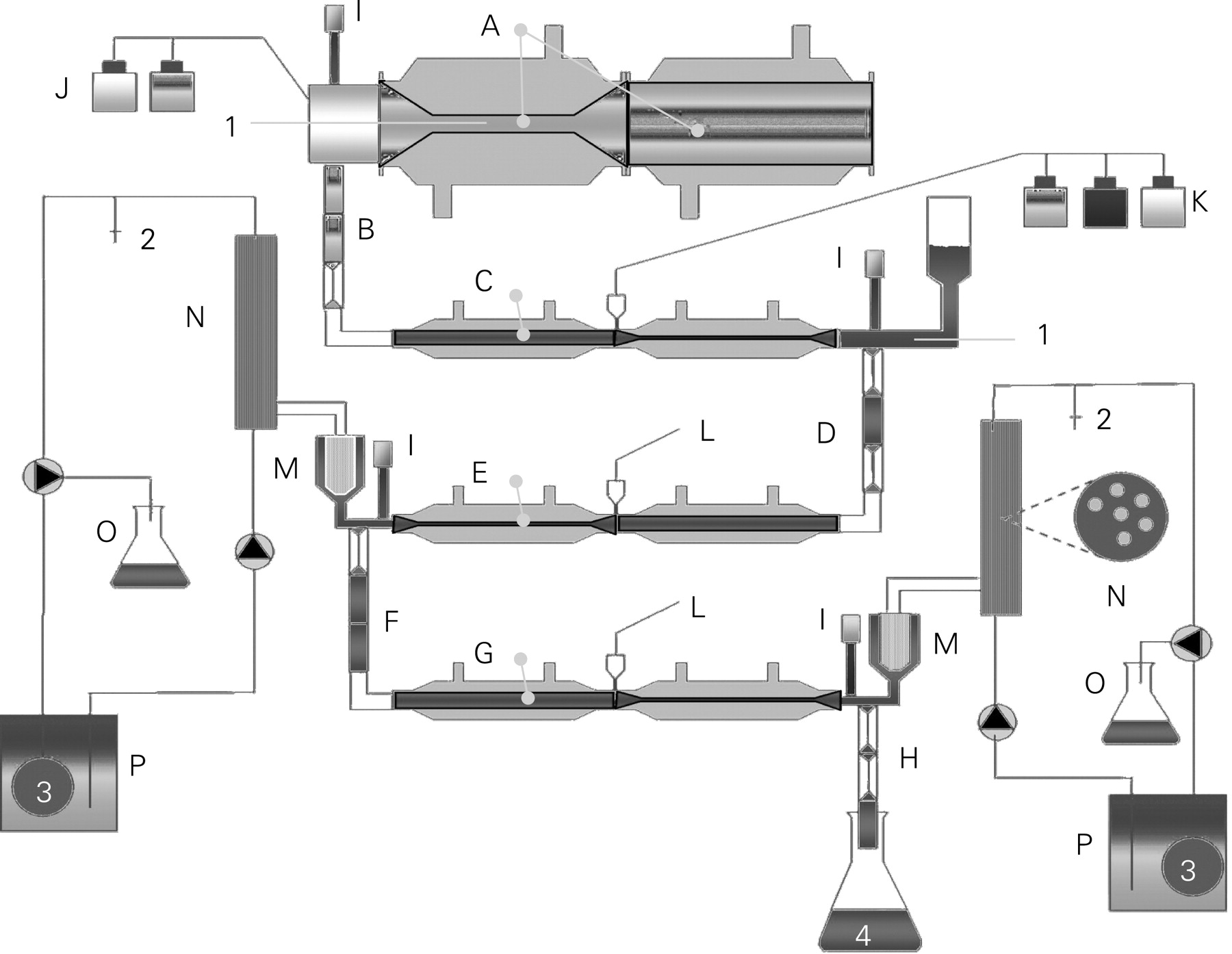
EFFICIENT DEGRADATION OF GLUTEN BY A PROLYL ENDOPROTEASE IN A GASTROINTESTINAL MODEL: IMPLICATIONS FOR COELIAC DISEASE
Gluten proteins are proline rich making them resistant to enzymatic digestion in the gastrointestinal tract and contributing to their immunogenic nature. In this elegant study utilising a dynamic system that closely mimics the human gastrointestinal tract (TIM system, see fig), Mitea et al determined the efficiency of gluten degradation by a post-proline cutting enzyme, Aspergillus niger prolyl endoprotease (AN-PEP). They processed a simple meal (slice of white bread) and a complex standard fast food meal in the TIM system with and without co-administration of AN-PEP. Samples of the digesting meals were taken from the stomach, duodenum, jejunum and ileum compartments at time zero until 4 hours after the start of the experiment. They used a variety of methods to measure the levels of immunogenic peptides from gliadins and glutenins. AN-PEP accelerated the degradation of gluten in the stomach compartment to such an extent that hardly any gluten reached the duodenum compartment. These interesting results imply that the co-administration of AN-PEP with a gluten-containing meal might eliminate gluten toxicity and call for appropriate clinical trials to begin.
See pages 25
Linked Articles
- Intestinal inflammation
- Colon
- Hepatitis
- Oesophagus
- Coeliac disease