Article Text

Statistics from Altmetric.com
INTESTINAL TYPE UPPER GI ADENOCARCINOMA DEVELOPS EARLIER IN SCOTTISH MALES
Chronic mucosal damage resulting from either reflux in the oesophagus or H pylori infection in the stomach leads to intestinal type adenocarcinoma with a strong male predominance, greatest in the oesophagus and least in the antrum. Since subtype varies by site it is unclear which of these variables is the strongest predictor of male predominance. The current study addressed this question using the West of Scotland Cancer Registry covering 3 million people. Histology was reviewed in 812 randomly selected cases and the subtype determined using the Lauren classification. Overall 63.8% of cancer patients were male, 55.1% non-cardiac stomach, 22% gastric cardia and 26.6% oesophageal. The male predominance was greatest in the oesophagus, the male/female ratio being 3.5, 2.0 in the cardia and 1.65 for non-cardiac gastric cancers. Multivariate analysis showed that the gender effect was lost when age and subtype were included. As the figure shows, the male predominance is largely due to males developing the intestinal subtype 17 years earlier than females, while the diffuse subtype showed no gender bias. The authors speculate that oestrogen may delay carcinogenesis by suppressing the inflammatory response.
See pages 16

ABNORMAL SMALL INTESTINAL BARRIER FUNCTION IS NECESSARY FOR COLITIS TO OCCUR IN IL10–/– MICE
Increased intestinal permeability has been found to be associated with inflammatory bowel disease, but whether it is aetiologically important is a matter of debate. Interleukin 10 gene deficient (IL10–/–) mice develop patchy, chronic colitis, similar to Crohn’s disease in humans. These mice have impaired intestinal barrier function, but its causative role in the development of colitis is unknown. Arrieta et al present a study in which they demonstrate that increased small intestinal permeability precedes colonic disease (assessed with TNFα and IFNγ) in IL10–/– mice (see fig). Furthermore, by treating the mice with AT-1001, an inhibitor of zonulin (a peptide secreted into the gut lumen, where it opens the tight junctions), the small intestinal permeability was reduced, which clearly attenuated colitis in these mice. Additional experiments also demonstrated that AT-1001 was active only in the small intestine. Therefore, as abnormal small intestinal permeability is aetiologically important in the development of colitis in IL10–/– mice, it seems plausible that increased small intestinal permeability may be involved in the aetiology of inflammatory bowel disease.
See pages 41


THE FICE MODE IS NOT SUPERIOR TO STANDARD COLONOSCOPY WITH TARGETED INDIGOCARMINE CHROMOENDOSCOPY FOR THE DETECTION OF ADENOMA
The substantial miss rate of colonic lesions during standard colonoscopy is a clinically important problem. Computed virtual chromoendoscopy with the “Fujinon intelligent colour enhancement” system (FICE), which narrows the bandwidth of light components to enhance mucosal contrast, has been proposed to reduce this miss rate. In the present issue of Gut, Pohl et al present a randomised multicentre trial where the adenoma detection rate with colonoscopy in the FICE mode was compared with standard colonoscopy with targeted indigocarmine chromoscopy (control group) (see fig). The adenoma detection rates were found to be similar in the groups. Moreover, for the differential diagnosis of adenomas and non-neoplastic polyps the two techniques were comparable (sensitivity 93% vs 90%; NS). Contrary to expectations, FICE did not shorten the procedural time. To conclude, no superiority for FICE over colonoscopy with targeted indigocarmine chromoendoscopy could be detected. Therefore, the place for FICE in clinical practice remains to be determined.
See pages 73
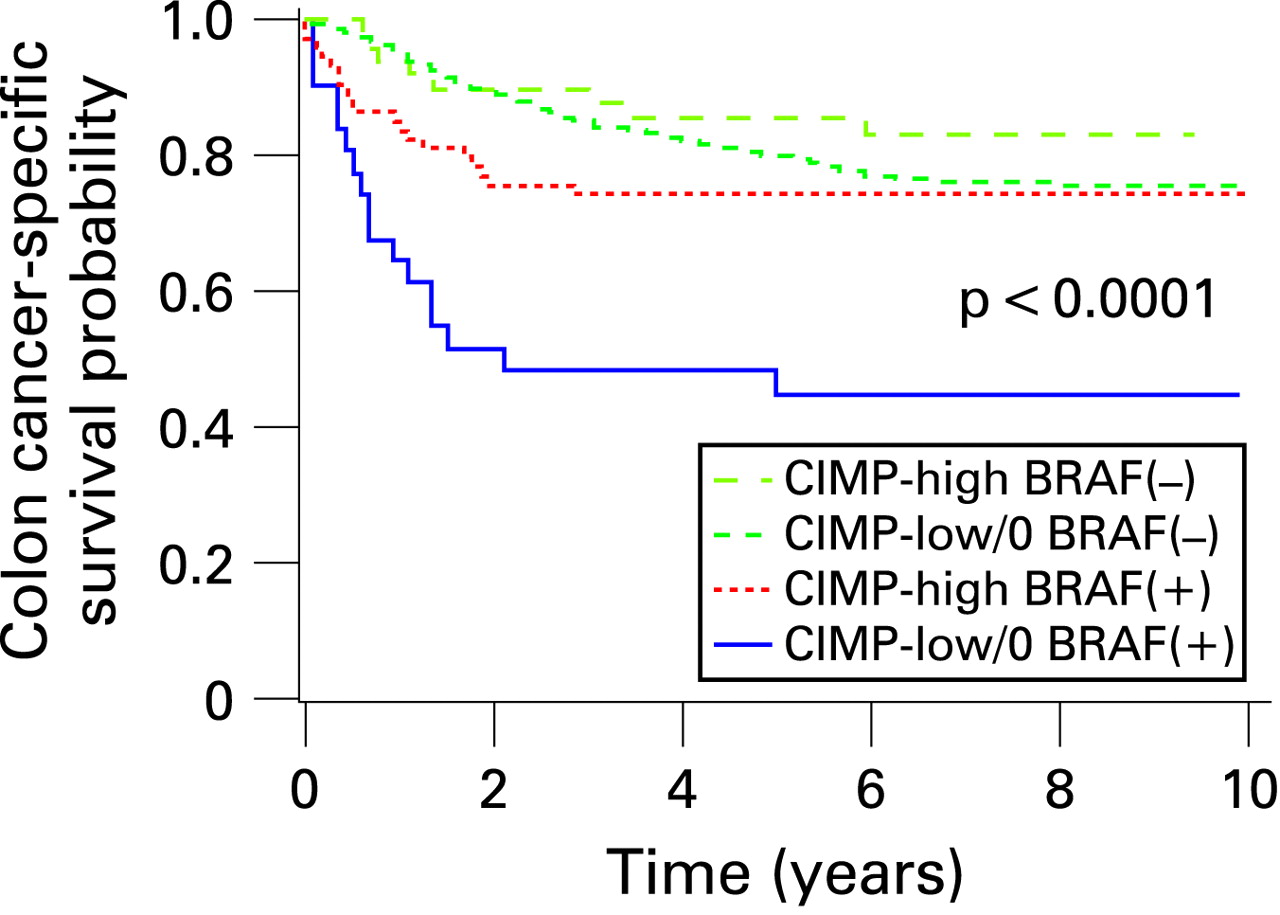
CPG ISLAND METHYLATOR PHENOTYPE (CIMP-HIGH) PREDICTS LOWER COLON CANCER SPECIFIC MORTALITY
CpG islands are genomic areas that contain a high frequency of cytosine and guanine dinucleotides. They are frequently found in promoter regions, where methylation is thought to inhibit gene expression. A subset of colorectal cancer (CRC) showing widespread promoter methylation are called CpG island methylator phenotype (CIMP) high. While microsatellite instability (MSI) is associated with better prognosis and mutation of the BRAF gene has an adverse effect, the effect of CIMP is unclear since CIMP-high is associated with BRAF mutation. This study examined 649 CRCs derived from two long term population cohorts containing 121 700 women and 51 500 men. Pathology slides were retrieved and DNA analysed. The commonest mutation was KRAS (37%), with 19% MSI high, 19% CIMP high and 17% with a BRAF mutation. As the figure shows, the CRC specific survival was worse in CIMP-low, BRAF+ tumours and best in CIMP high, BRAF– patients. The multivariate analysis showed that KRAS status had no independent effect on prognosis. The adverse effect of BRAF+ remained but was ameliorated by being CIMP high. Defining just how these mutations interact will improve our ability to predict prognosis in CRC.
See pages 90

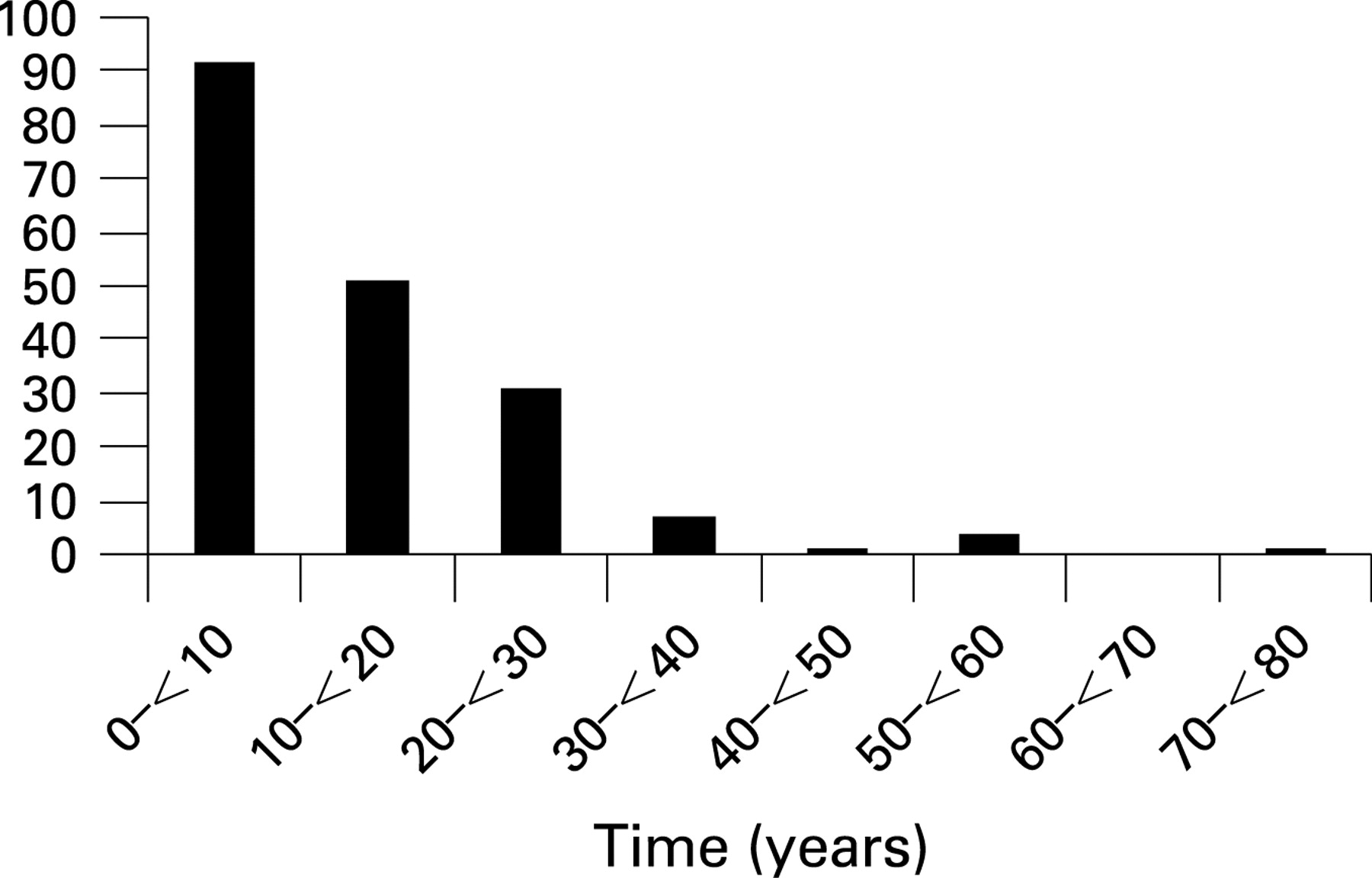
HEREDITARY PANCREATITIS IN FRANCE—A VERY RARE BUT ULTIMATELY FREQUENTLY FATAL GENETIC DISORDER
Hereditary pancreatitis (HP) is a rare autosomal dominant genetic condition and so most reports to date have been small. This population-based study attempted to describe all HP patients in France and identified 200 patients within 78 families, giving a prevalence of 0.3 per 100 000 of the French population. As the figure shows, most patients develop symptoms before the age of 30 though the diagnosis was often delayed. The cationic tripsinogen gene (PRSS1) mutation accounted for 68% of cases with mutation of the serum protease inhibitor KAZAL type 1 (SPINK1) in 13% and a mutation of the CFTR (cystic fibrosis transmembrane conductance regulator) in 2%. The main symptoms were abdominal pain in 83% and acute pancreatitis in 69%. Exocrine and endocrine pancreatic insufficiency developed in 32% and 26% at a median age of 29 and 38 years, respectively. The presence or absence of a PRSS1 mutation did not influence the development of pancreatic insufficiency. 16% had endoscopic procedures while 24% had surgery, mostly splenopancreatectomy. 10 (5%) developed adenocarcinoma, the risk increasing with age, reaching 53% by the age of 75. Pancreatic adenocarcinoma accounted for 42% of the 19 deaths and is thus the largest single cause of mortality in HP.
See pages 97
METABOLIC SYNDROME—AN INDEPENDENT RISK FACTOR FOR LIVER CIRRHOSIS IN CHRONIC HEPATITIS B
Metabolic syndrome, comprising type 2 diabetes, hypertension, central obesity and dyslipidaemia, is a negative prognostic factor for patients with various chronic liver diseases. However, the role of the metabolic syndrome in patients with chronic hepatitis B (CHB), the most common cause of liver cirrhosis worldwide, is unknown. In this issue of Gut, Wong and co-workers convincingly demonstrate that metabolic syndrome is an independent risk factor of liver cirrhosis in CHB. This was true for patients with histological liver cirrhosis, as well as for patients with possible and probable liver cirrhosis, assessed with liver stiffness measurement (see fig). Moreover, the odds ratios for development of probable and possible cirrhosis had an increased trend with increasing numbers of components of the metabolic syndrome. In a subset of the patients the accuracy of liver stiffness measurements was assessed and found to be good. Based on the findings in the present study assessment of the benefit of therapy for the metabolic syndrome in patients with CHB seem warranted.
See pages 111

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Linked Articles
- Upper gastrointestinal cancer
- Inflammatory bowel disease
- Endoscopy
- Colorectal neoplasia
- Pancreas
- Hepatology