Article Text

Statistics from Altmetric.com
Drinking green tea associated with decreased risk for distal gastric cancer in Japanese females
There are numerous studies of the impact of drinking green tea on gastric cancer risk with conflicting results. This may well be due to confounding by associated factors like smoking or because some factors such as drinking scalding hot tea increase cancer risk while other features of green tea decrease the risk, including its inhibitory effect on Helicobacter pylori, together with anti-oxidant and phytoestrogenic effects. This meta-analysis attempts to overcome this by using data from over 2 million person-years follow-up with a large (3577) number of gastric cancer cases. The authors found that while green tea consumption in men is associated with no reduction in the risk of gastric cancer, in females there is a clear dose–response with increasing consumption of green tea reducing the risk (see fig). The effect was even stronger when just considering distal gastric cancers, with a relative risk of 0.70 (0.05–0.96) for those with the highest intake. A similar differential effect of green tea by sex has also been seen in cardiovascular disease, which has been attributed to phytoestrogenic components of green tea including lignan polyphenols and flavonoids that may also mediate the benefit in gastric cancer.
See pages 1323

Relative risk of gastric cancer for different levels of green tea consumption (drawn from table 4).
TRPA1 blockade attenuates visceral pain induced by gastric distension
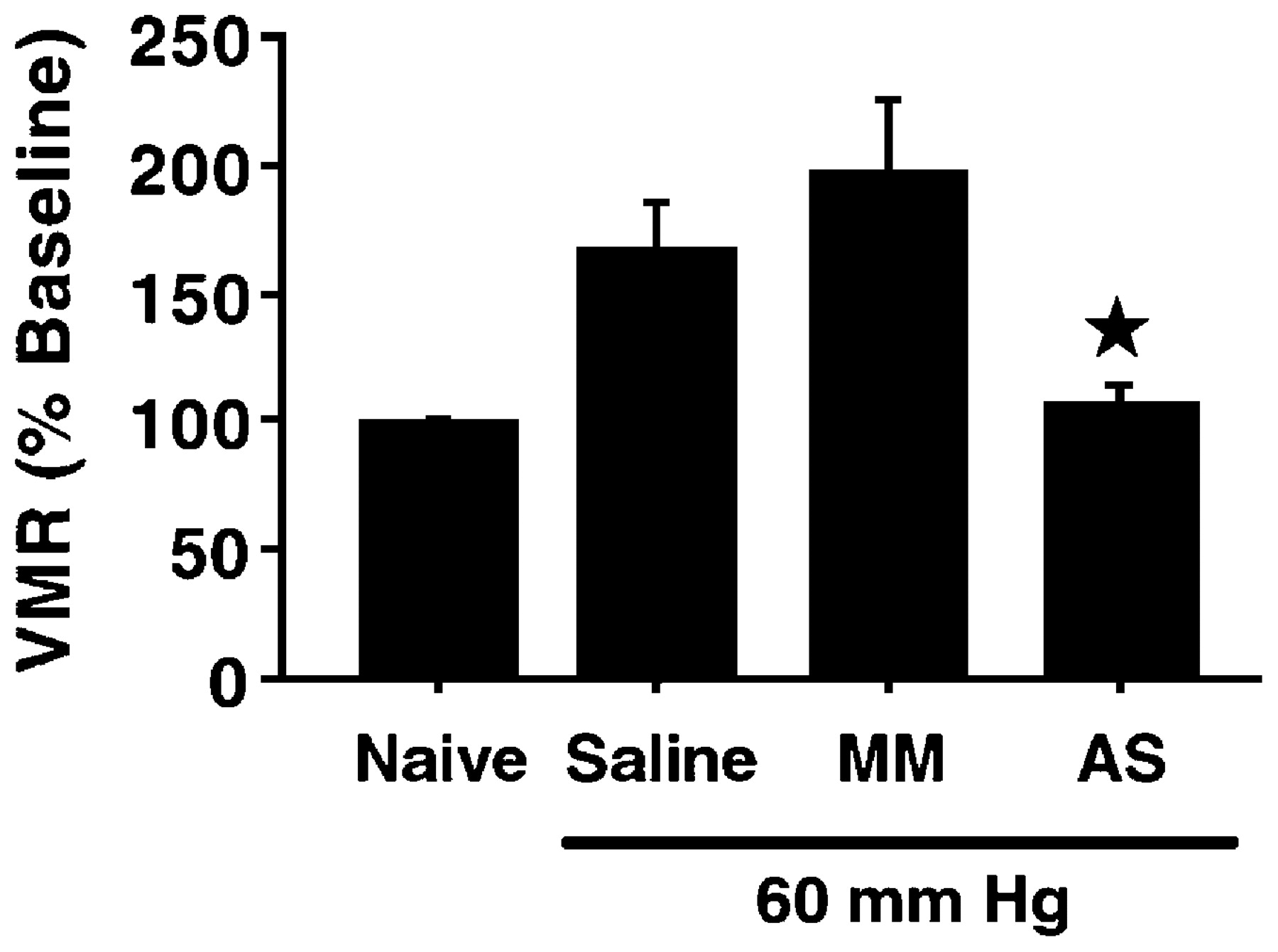
Transient receptor potential channels are a family of widely distributed ion channels that respond to temperature, touch and a range of chemical agents, including most famously capsaicin, which activates transient receptor potential vanilloid 1, a heat-sensitive ion channel found in many afferent nerves. Transient receptor potential A1 (TRPA1) is activated by noxious cold (<17oC) and by pungent chemicals including allicin from garlic. By injecting fluorescent fluorogold (FG) into the stomach from where it spreads via the nerve to the nodose ganglia (NG) and dorsal root ganglia (DRG), the authors were able to identify FG positive neurones within the NG and DRG, the majority of which were TRPA1 positive. By co-localisation with other markers, the authors conclude that TRPA1 is found in the unmyelinated peptidergic neurones. Using balloon distension as a means of inducing visceral pain the authors showed that knockdown of TRPA1 by injecting antisense oligodeoxynucleotide intrathecally could block the visceral motor response to distension (see fig). Similarly, a novel selective TRPA1 inhibitor was also able to inhibit this response. These studies should encourage the development of TRPA1 antagonists as possible visceral analgesics.
See pages 1343
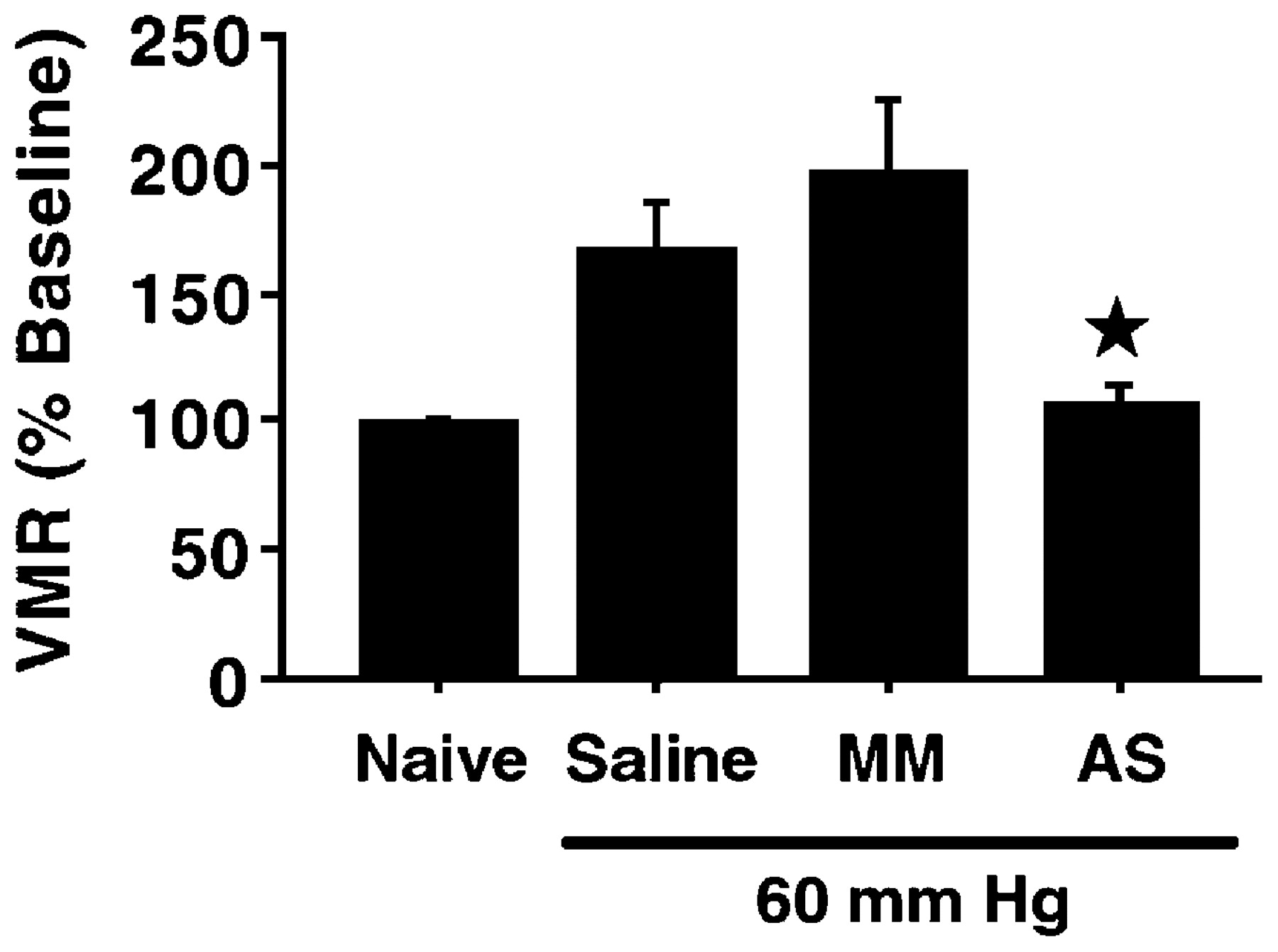
Visceromotor response (VMR) to gastric balloon distension was reduced by the antisense (AS) but not the control mismatched (MM) oligodeoxynucleotide nor the saline control. Naïve animals were exposed to 0 mm Hg distension.
Randomised controlled trial on steroid-sparing properties of sargramostim in Crohn’s disease
Corticosteroids are an effective treatment for induction of remission in up to 80% of patients with Crohn’s disease (CD). However, prolonged exposure to these drugs is undesirable for reasons of toxicity. Moreover, 20% of patients become refractory within 1 year and approximately one-third develop steroid dependency. Defects in the innate immunity underlie the pathophysiology of CD. Therefore, the authors hypothesised that enhancement of intestinal innate immunity might be beneficial in treating patients with CD. This randomised controlled study evaluated the efficacy of sargramostim (granulocyte-macrophage colony-stimulating factor) 6 μg/kg via subcutaneous injection daily or placebo in patients with corticosteroid-dependent CD. The primary endpoint was corticosteroid-free remission 4 weeks after corticosteroid elimination. A total of 87 patients with CD were randomised to sargramostim and 42 to placebo. Results showed that corticosteroid-free remission was higher among sargramostim-treated patients than placebo patients (18.6% vs 4.9%; p = 0.03). These findings need confirmation in larger studies but if consistent results are obtained, sargramostim may provide significant benefit in this patient population.
See pages 1355

Corticosteroid (CS)-free remission and response at treatment observation week 4.
Anti-CTLA-4 treatment induces IL-10-producing ICOS regulatory T cells displaying IDO-dependent anti-inflammatory properties
T cell co-stimulation is one of the mechanisms controlling immunity and tolerance in vivo. The monovalent homodimer CD28 and cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) are very important players in this mechanism. Previously, it was suggested that CD28 and CTLA-4 had opposing effects on the response of T cells and that CTLA-4 could function as a negative regulator of T cell activation. In this murine model of colitis, the authors tested if anti-CTLA-4 treatment would alter polarisation of naive T cells in vivo. Mice were treated with anti-CTLA-4 monoclonal antibodies (mAB) at the time of immunisation or colonic instillation of trinitrobenzene sulfonic acid. The injection of anti-CTLA-4 mAb induced the development of adaptive CD4+ regulatory T cells, which expressed high levels of inducible co-stimulator secreted IL-4 and IL-10. This treatment inhibited Th1 responses and repressed intestinal inflammation. The amelioration of disease correlated with indoleamine 2,3 dioxygenase (IDO) expression and with infiltration of Foxp3+ T cells in the intestine, suggesting that anti-CTLA-4 acted indirectly through the development of regulatory T cells producing IL-10 and inducing IDO. This study shows the synergy between IL-10 and IDO as anti-inflammatory agents and highlights anti-CTLA-4 treatment as a potential novel immunotherapeutic approach for inducing adaptive regulatory T cells.
See pages 1364

Increased numbers of inducible co-stimulator (ICOS)high T regulatory cells in the mesenteric lymph nodes of anti-cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) treated mice (similar findings for colon shown in manuscript). TNBS, trinitrobenzene sulfonic acid.
Prospective screening of high risk individuals from familial pancreatic cancer families
Pancreatic cancer (PC) has a bad prognosis with a 5-year survival <5%. This is due to the late presentation, low resection rates and poor response to treatment. Early detection would improve outcome, especially in high-risk individuals such as patients with familial PC. In this prospective study, the authors evaluated the diagnostic yield of a screening programme in high risk individuals from familial PC. Screening included clinical examination, laboratory tests, endoscopic ultrasound (EUS) and MRI with magnetic resonance cholangiopancreaticography (MRCP) and MR angiography. Between 2002 and 2007, 76 families took part in the screening programme. Of the 76 families, 28 patients revealed abnormalities in EUS (n = 25) and/or MR/MRCP (n = 12). Six underwent limited resections and histopathological examination showed serous oligocystic adenomas (n = 3), pancreatic intraepithelial neoplasia (PanIN) 1 lesions with lobular fibrosis (n = 1), PanIN 2 lesions (n = 1) and PanIN 1 lesion plus a gastric type intraductal papillary mucinous neoplasm (n = 1). In conclusion, an EUS/MR-MRCP-based screening programme leads to detection of potential precursor lesions of PC. However, given the low yield, the yet undefined tumourogenic value of low grade PanIN lesions, the psychological stress for the tested individual and the high costs, a general PC screening programme is not justified.
See pages 1410
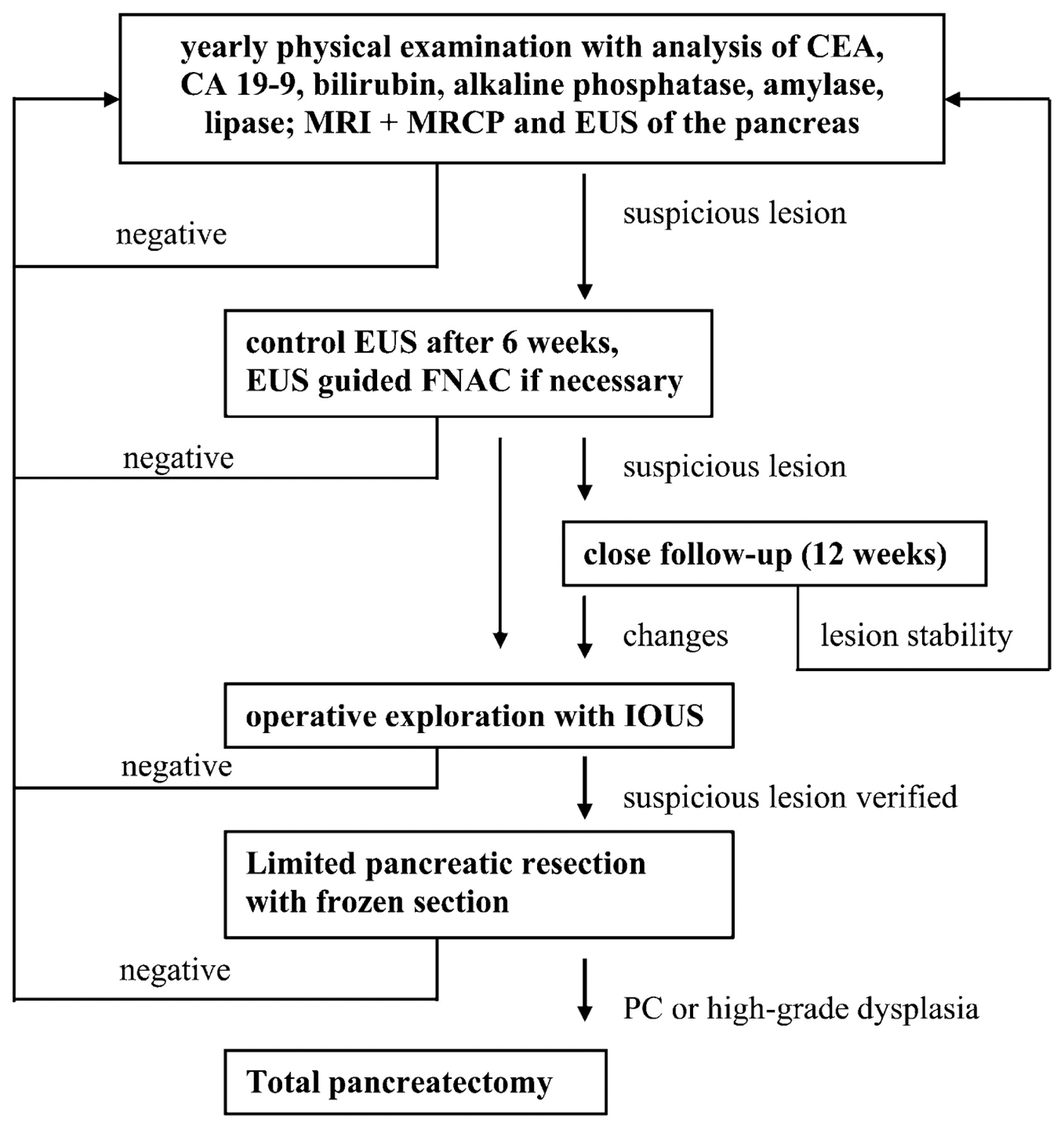
Screening algorithm. CEA, carcinoembryonic antigen; EUS, endoscopic ultrasound; FNAC, fine needle aspiration cytology; IOUS, intraoperative ultrasound; MRI+MRCP, MRI combined with magnetic resonance cholangiopancreaticography; PC, pancreatic cancer.
Even modest weight gain increases the risk of fatty liver
The international epidemic of obesity, diabetes and metabolic syndrome means that non-alcoholic fatty liver disease (NAFLD) is an ever increasing problem. Chang and colleagues describe a large cohort of industrial workers who were required to undergo periodic health examinations in Korea. More than 15 000 workers aged 30–59 years were weighed and had serum lipid and alanine aminotransferase (ALT) levels measured, together with abdominal ultrasound. Fatty liver was diagnosed ultrasonographically based on liver brightness and hepatorenal contrast. After excluding pre-existing hepatitis and other known liver diseases or those taking medication that could cause NAFLD, 5053 workers were available for follow-up for a mean of nearly 4 years. As the figure shows, a weight gain of more than 2.7 kgs increased the risk of developing ultrasonographically diagnosed fatty liver by nearly 50%. The deleterious effect of weight gain, even while within the normal weight range, points to the importance of insulin resistance in accumulating fat in the liver rather than body weight per se. Interestingly, even a small weight reduction reduced the risk significantly in those who also had elevated ALT.
See pages 1419

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Adjusted HR for developing ultrasonographically detected fatty liver and elevated alanine aminotransferase compared for groups based on weight change over approximately 4 years.
Linked Articles
- Neurogastroenterology
- Hepatology
- Pancreatic cancer
- Gastric cancer
- Inflammatory bowel disease
- Inflammatory bowel disease