Article Text

Statistics from Altmetric.com
Mechanisms underlying basal cell hyperplasia in eosinophilic oesophagitis
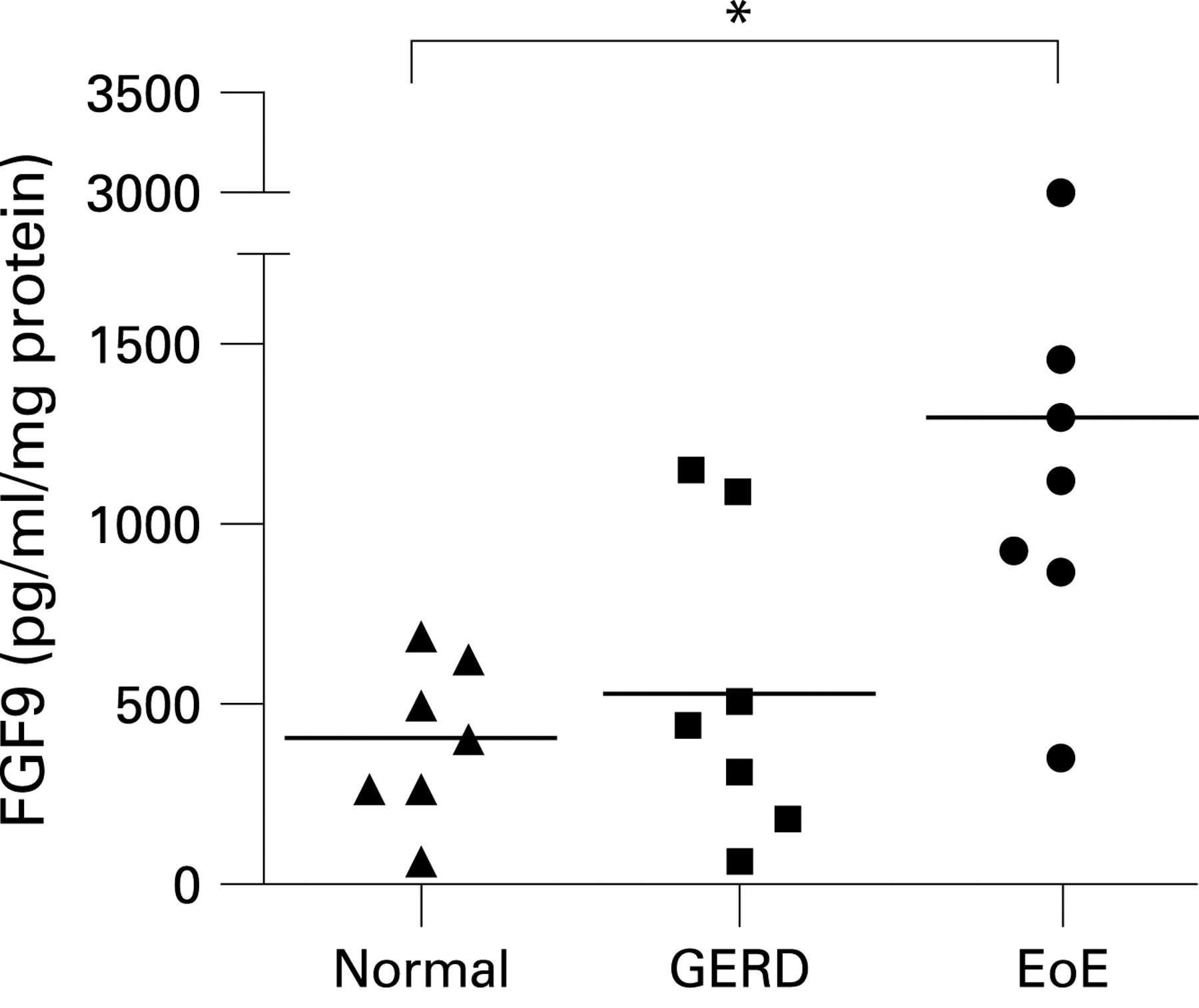
Eosinophilic oesophagitis is an increasingly recognised cause of dysphagia, characterised by >15 eosinophils/high powered field, basal zone hyperplasia and elongation of vascular papillae. Eosinophils release inflammatory mediators, the most abundant of which is major basic protein (MBP). The extracellular calcium sensing receptor (CaSR) is a G-protein-coupled receptor. The present study using an oesophageal cell line (HET-1A) showed that CaSR responds to MBP-peptide. Furthermore, when HET-1A cells were incubated with MBP-peptide there was a marked increase in fibroblast growth factor 9 (FGF9). Transfecting the cells with short interfering siRNACaSR blocked the production of FGF9 showing this was a CaSR dependent process. The authors also showed that FGF9 stimulates cell proliferation and that paediatric patients with a eosinophilic oesophagitis had a substantial increase in FGF9 in homogenates of oesophageal mucosal biopsies (see fig). Finally, the FGF9 was shown by immunohistochemistry to be increased in eosinophilic oesophagitis. By defining the mechanism whereby eosinophils act this study opens the way to more specific rational therapy of this newly recognised condition. See page 166.

The metabolic syndrome increases the risk of progression from non-erosive to erosive reflux disease
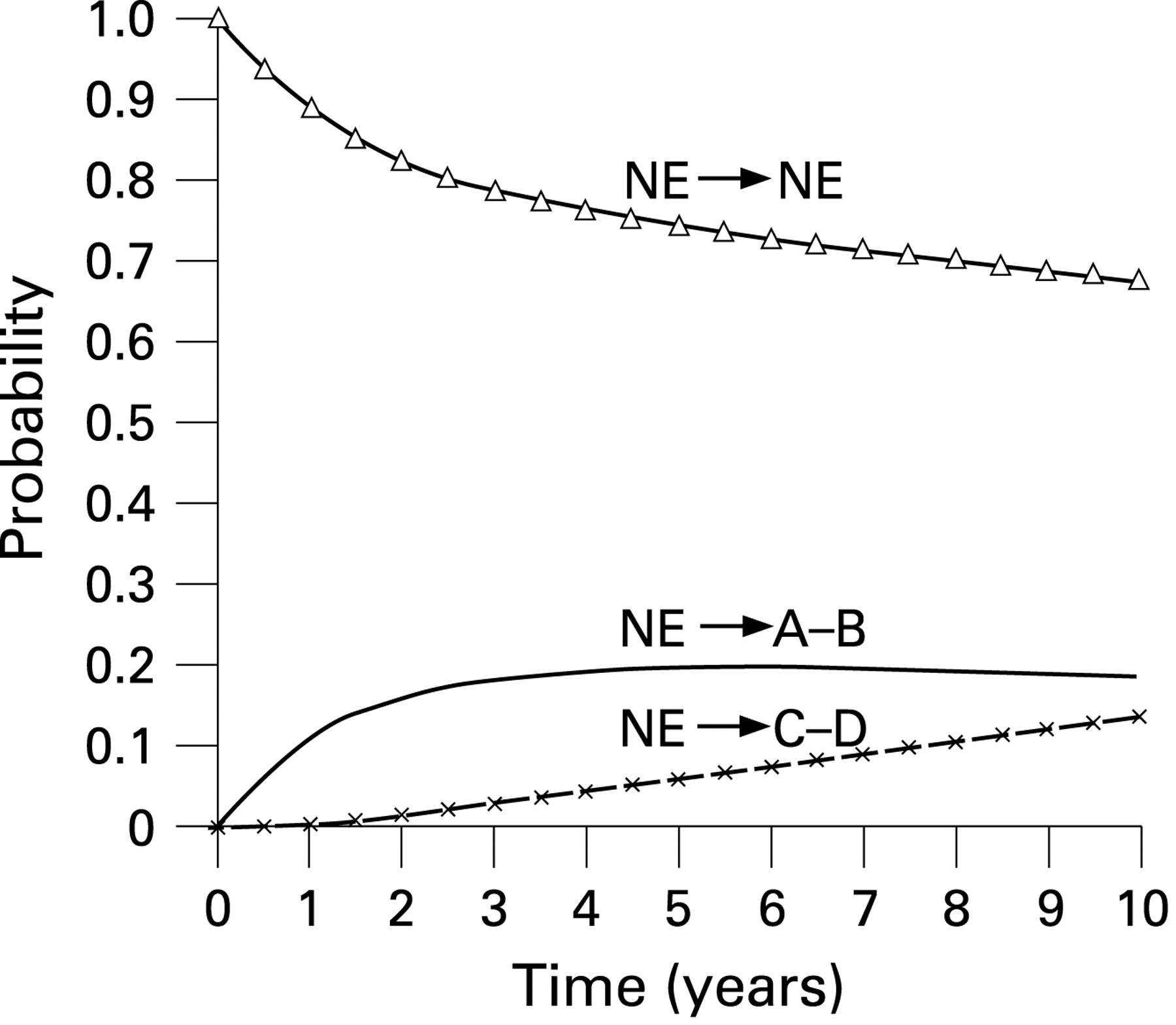
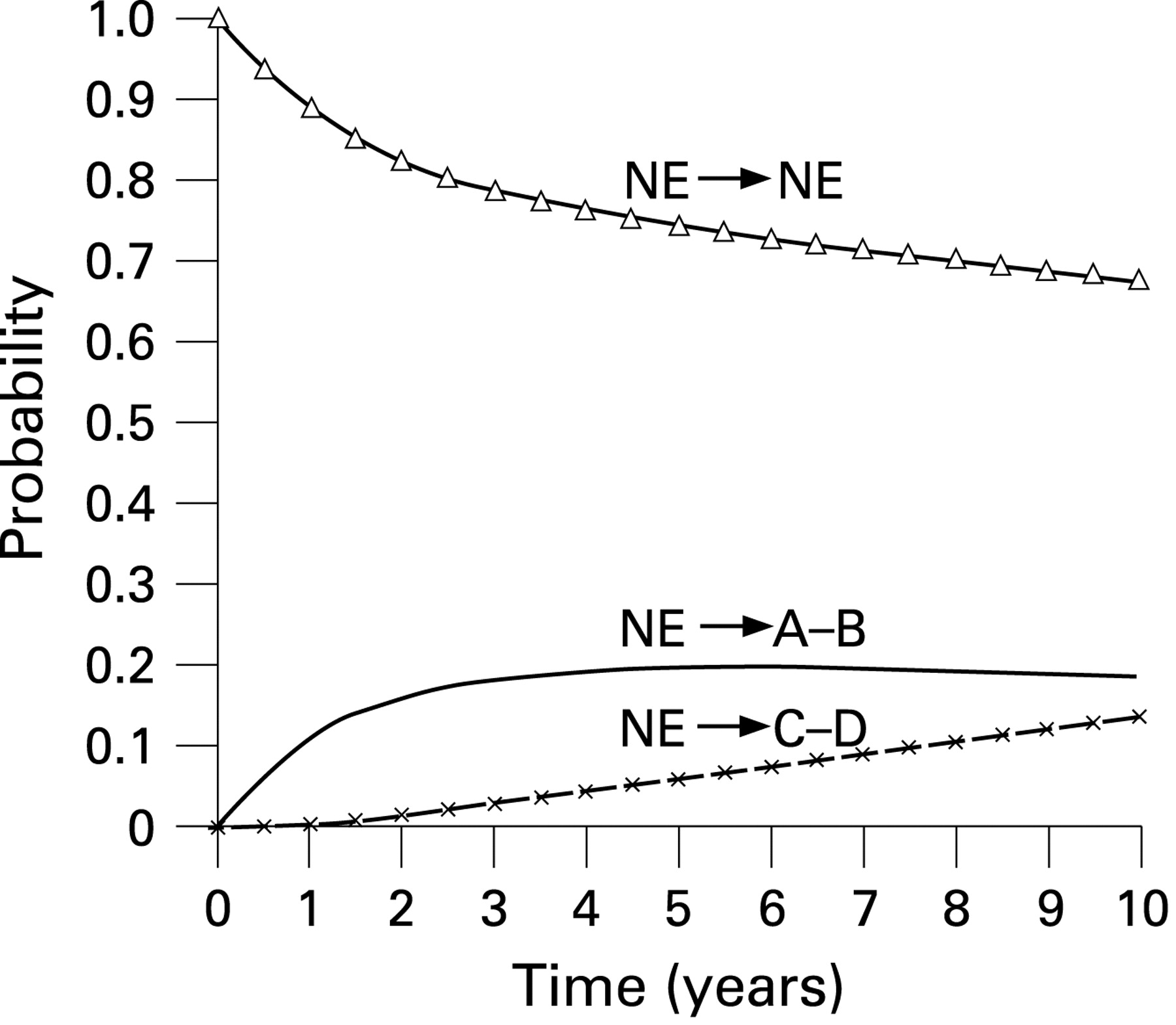
The natural course of gastro-oesophageal reflux disease (GORD) is incompletely known. This is also true for risk factors for the progression from a non-erosive to an erosive state. In this issue of Gut, Lee et al report a study of 3669 subjects who underwent repeated upper GI endoscopy as part of a voluntary health promotion programme in Taiwan. They found that during the three consecutive study periods 12%, 15% and 18%, respectively, progressed from non-erosive to erosive disease (see fig), and 43%, 37% and 35%, respectively, regressed to the non-erosive stage. Male gender, smoking and the metabolic syndrome were found to independently increase the likelihood of progression from non-erosive to erosive disease, and/or to lower the likelihood of disease regression. Moreover, the short-term use of acid suppression (long-term use was an exclusion criterion) increased the likelihood of disease regression. This study provides important information on the natural course of GORD, as well as on different risk factors for progression from non-erosive to erosive disease, which could be included in future preventive strategies. See page 174.
Highly active antiretroviral therapy in HIV restores the impairment in gut barrier function
Evidence suggests that intestinal barrier function is important in disease progression in HIV, and several studies have demonstrated increased permeability of the intestinal epithelium of HIV patients. In the current issue of Gut, Epple et al show that altered permeability and villous atrophy is seen only in untreated HIV patients, whereas patients treated with highly active antiretroviral therapy (HAART) do not differ from control subjects (see fig). Moreover, the alterations in permeability seem to be due to altered tight junction proteins, such as pore-forming claudin-2 and sealing claudin-1, as well as elevated epithelial apoptoses. They also found evidence suggesting that different mucosal cytokines may mediate the barrier defect in these patients. Specifically, interleukin 2 (IL2), IL4 and TNFα were found to be increased in untreated, but not in treated, HIV patients, and incubation with IL2, IL4, TNFα and IL13 reduced the transepithelial resistance in the small intestine of the rat. Therefore, the effect of HAART on intestinal permeability may be one of the mechanisms involved in reducing disease progression in HIV patients. See page 220.

Mesalazine for active ulcerative colitis: once daily as good as three times daily
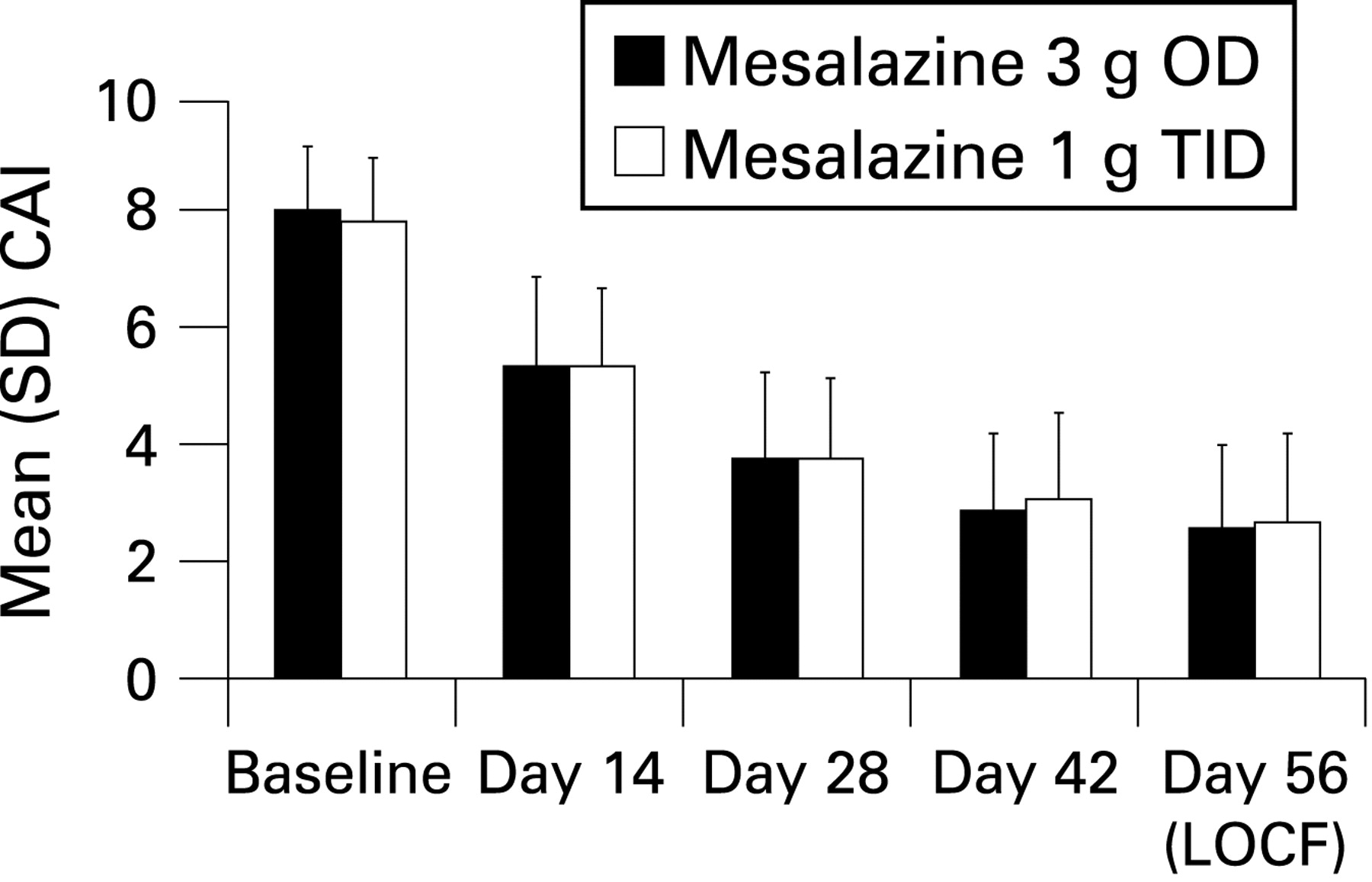
Aminosalicylates have traditionally been given as three times a day (TID), though the logic of this is dubious, as the current study shows. Used as enteric coated capsules, they are designed to deliver drug to the colon, whose slow transit and relatively effective mixing makes the TID regimen superfluous for most subjects. For busy patients the TID regimen is onerous and substantially increases the risk of non-compliance. This 8-week study was a randomised double-blind, double dummy parallel group trial comparing 3 g once daily (OD) versus 1 g TID of mesalazine. 391 patients with an endoscopically confirmed diagnosis of ulcerative colitis extending >15 cm from the anal margin were enrolled. The primary end point (percentage of patients achieving clinical remission, defined as Clinical Activity Index (CAI) <14) was reached in 79% in the OD and 76% in the TID dosage group (see fig) indicating non-inferiority, p<0.001. However, the vast majority of patients, 82%, preferred the OD dosage and only 2% preferred the TID dosage. Adverse events related to the drug were found in 3% of the OD and 5% of the TID dosage, suggesting that OD should be the preferred regimen. See page 233.

High-resolution and low-dose CT colonography is a feasible tool for colorectal cancer screening
Colorectal cancer is a major public health issue in the Western world. Screening of asymptomatic and average risk population is therefore recommended in many countries today. However, the optimal method for colorectal cancer screening remains to be determined. In this issue of Gut, Graser and colleagues present a head-to-head comparison between five different screening modalities: CT colonography (CTC) (see fig), colonoscopy (OC), flexible sigmoidoscopy (FS), faecal immunochemical stool testing (FIT) and faecal occult blood test. The sensitivity to detect advanced colonic neoplasia (invasive cancer, adenoma ⩾10 mm, presence of a villous component of at least 25% or high-grade dysplasia) was 100% and 97% for OC and CTC, respectively, whereas it was 83% for FIS and only 32% and 20% for FIT and FOBT. CTC was preferred by 46% of patients, versus 37% who preferred OC. The radiation exposure with CTC was found to be low, only 4.5 mSv. On the basis of these data, high-resolution and low-dose CTC seems to be a good alternative to colonoscopy as a primary colorectal cancer screening test. See page 241.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Blockade of vascular endothelial growth factor receptor 2 reduces vascular leakage in serotic rats with ascites
Advanced liver disease is associated with ascites and increased vascular leakage within the liver and mesentery. This study used rats in whom cirrhosis had been induced with carbon tetrachloride to study the role of vascular endothelial growth factor type A (VEGF-A) in the induction of vascular leakage. VEGF-A acts via vascular endothelial growth factor receptor 2 (VEGFR2) to increase vascular permeability (50 000 times more potent than histamine); however, this effects requires the presence of angiopoietin-2. Leakage of Evans Blue was markedly increased in the liver and the mesentery but markedly decreased in the pancreas in cirrhotic animals with ascites. This was associated with a rise in mesenteric, pancreatic and small intestinal blood flow and systemic hypotension. mRNA of VEGFR2 and angiopoietin-2 were increased in the liver and mesentery but decreased in the pancreas. Immunohistochemistry showed that VEGF-A and angiopoietin-2 were much increased throughout the liver in cirrhotic animals but decreased in the pancreas. The functional significance of this was shown by the markedly reduced vascular leakage in the liver and mesentery induced by a VEGFR2 antagonist (see table). Whether these pathways can be manipulated for therapeutic benefit remains to be determined. See page 285.
Linked Articles
- Oesophageal disease
- Oesophageal disease
- Inflammatory bowel disease
- Inflammatory bowel disease
- Colonic cancer
- Hepatology