Article Text

Abstract
Objective: This study investigated the effects of oral supplementation of resistant starch (RS) on tumour cell and colonic mucosal cell kinetics and on gene expression in patients with colorectal cancer (CRC), and its potential role in colon cancer prevention.
Methods: 65 patients with CRC were randomised to treatment with RS or ordinary starch (OS) and were given starch treatment for up to 4 weeks. Pretreatment and post-treatment biopsies were obtained from the tumour and colonic mucosa, and the effects of the starch treatment on cell proliferation and expression of the cell cycle regulatory genes CDK4 (cyclin-dependent kinase 4) and GADD45A (growth arrest and DNA damage-inducible, alpha) were investigated.
Results: The proportion of mitotic cells in the top half of the colonic crypt was significantly lower following RS treatment (3.1 (1.5), mean (SEM)) as compared with OS treatment (13.7 (3.2)) (p = 0.028). However, there was no effect of RS treatment on crypt dimensions and tumour cell proliferation index. There was significant upregulation in expression of CDK4 (p<0.01) and downregulation in expression of GADD45A (p<0.001) in the tumour tissue when compared with macroscopically normal mucosa. Following RS treatment, CDK4 expression in tumours (0.88 (0.15)) was twofold higher than that in the OS group (0.37 (0.16)) (p = 0.02). The expression of GADD45A, which was downregulated in the presence of cancer, was significantly upregulated (p = 0.048) following RS treatment (1.41 (0.26)) as compared with OS treatment (0.56 (0.3)). However, there were no significant differences in the expression of these genes in the normal mucosa following starch treatment.
Conclusions: Cell proliferation in the upper part of colonic crypts is a premalignant marker and its reduction by RS supplementation is consistent with an antineoplastic action of this food component. Differential expression of the key cell cycle regulatory genes may contribute to the molecular mechanisms underlying these antineoplastic effects of RS.
Trial registration number: ISRCTN93586244.
Statistics from Altmetric.com
Resistant starch (RS) is defined as the fraction of dietary starch which resists digestion in the small intestine of healthy individuals.1 This undigested starch forms a major substrate for microbial fermentation in the large bowel, leading to the production of short chain fatty acids (SCFAs) including acetate, propionate and butyrate.2 3 RS has a number of physiological effects in the colon, most of which are thought to be due to the SCFAs, particularly butyrate. There is compelling evidence that butyrate causes a dose-dependent suppression of proliferation of colon cancer cell lines,4–8 and RS has antineoplastic effects against colon cancer in animal models.9–11 Recent studies in rat have shown that feeding RS reduced the incidence and multiplicity of azomethane-induced colon cancers and reduced the tumour-enhancing effects of indigestible protein and red meat.12–14 These protective effects of RS were thought to be secondary to fermentation of RS to butyrate in the colon.
A limited number of studies have investigated the antineoplastic effects of RS in vivo in humans. The results of these studies, which included mostly healthy human volunteers, have been inconclusive. Van Munster et al3 reported a significant reduction in colonic mucosal cell proliferation. Although most of the other human studies reported an increase in the concentrations of SCFAs and reduction in the concentration of bile salts in the colonic lumen, there were no significant effects on mucosal cell proliferation.15–17
The mechanism(s) responsible for the antineoplastic effects of butyrate is not known with certainty, but butyrate influences several processes important in tumourigenesis, including cell proliferation, apoptosis, angiogenesis, immunosurveillance and inflammation. These effects of butyrate have been attributed to changes in gene expression17–20 possibly as a consequence of epigenetic processes including hyperacetylation of histones H3, H4, H2A and H2B. Our recent work investigating the possible mechanisms for chemoprevention of DNA mismatch repair-deficient colorectal cancer (CRC) highlighted the enhanced antineoplastic effects and differential gene expression in such tumour cells following butyrate treatment.21
This study was undertaken to investigate the effects on cell kinetics and gene expression in both colonic tumours and the adjacent macroscopically normal appearing flat mucosa following oral supplementation of RS in patients with CRC. Gene expression changes were investigated in two cancer-related genes, cyclin-dependent kinase 4 (CDK4) and growth arrest and DNA damage-inducible, alpha (GADD45A). These two genes are differentially expressed following butyrate treatment in in vitro studies on colon cancer cells.20–22
PATIENTS AND METHODS
Patient enrolment
Adult patients undergoing colonoscopy or a flexible sigmoidoscopy with sympoms highly suspicious of CRC and patients with a histology-proven CRC amenable for surgical treatment were considered for the study. Enrolment of patient volunteers was undertaken at two District General Hospitals in North East England from July 2005 to May 2006. Patients who had a previous subtotal colectomy or ileostomy, pregnant women, patients receiving long course preoperative chemo-radiotherapy for rectal cancers, patients with symptoms suggestive of bowel obstruction and patients needing emergency surgery for their cancer were excluded from the study.
Study protocol
This was a randomised double-blind placebo-controlled intervention trial using two different study protocols—that is, Study 1 and Study 2. In Study 1, patients were consented and recruited at the time of colonoscopy before the diagnosis of CRC. Pretreatment biopsies were obtained from the normal mucosa and from the suspected cancer at the time of colonoscopy, and only patients with histology-proven CRC amenable for surgical resection were retained in the study. Patients were then randomised (www.randomizer.org) into two groups: (1) treatment (resistant starch (RS)) group and (2) placebo (ordinary starch (OS)) group. Volunteers were allotted to treatment and placebo groups in a ratio of 2:1, respectively, and were given starch treatments as explained below. In Study 2, volunteers were consented and recruited into the study after the histological diagnosis of CRC, and no preoperative biopsies were obtained in this group of volunteers. Volunteers were randomised into treatment (RS) and placebo (OS) groups as described above. Post-treatment biopsies from the tumour and from the macroscopically normal mucosa at least 5 cm from the tumour margin were obtained from the resected colectomy specimens. Biopsies were placed in three sets of cryovials containing RNAlater (Ambion, Applied Biosystems, Warrington, UK), Carnoy’s solution (ethanol:acetic acid 75:25) (Sigma Aldrich, York, UK) and formalin (Sigma Aldrich), respectively. Tissue in RNAlater was kept at 4°C for 4–6 h, snap-frozen in liquid nitrogen and stored at −80°C until required for studying gene expression. Tissue in Carnoy’s solution was transferred to 70% ethanol within 12–24 h of collection and stored at 4°C until used for measurements of crypt cell kinetics. Formalin-fixed paraffin-embedded tissues were used for immunohistochemical studies.
Study intervention: starch treatment
The starches used in this study were food-grade starches provided by the National Starch and Chemical Company, New Jersey, USA (www.nationalstarch.com). The test starch (RS) was a 1:1 blend of Novelose 240 and Novelose 330. Novelose 240 contains approximately 70% amylose and 30% amylopectin, and is a rich source of granular resistant starch. Novelose 330 is a good source of non-granular resistant starch. The placebo starch (OS) was Amioca waxy starch which contains only amylopectin. Because of its branched and open structure, amylopectin is rapidly and completely digested in the small bowel. In contrast, amylose has a linear molecular structure which forms helical structures and, without gelatinisation, is resistant to pancreatic amylase.23 Study participants were provided with presealed boxes containing the appropriate starch sachets (RS or OS) and were asked to take 30 g of starch (two sachets) per day until the day before the planned surgery. Patients were provided with 4 weeks supply of starch and were contacted weekly to ensure compliance with treatment. Subjects who took the starch treatment for <2 weeks were excluded from the final analysis.
Processing and analysis of biopsies
Tissue sections (3 μm thick) were cut from formalin-fixed paraffin-embedded tissue blocks and stained with H&E and immunohistochemical staining using methods described previously.19 MIB1 (mindbomb homologue 1 (Drosophila)), a monoclonal antibody against the Ki-67 antigen (1:250 dilution), was used to identify proliferating cells within the tumour tissue. The proliferating cell index (PCI) of the tumours was estimated by examining the stained slides using a square graticule at high magnification (×100) as described previously.24 25
Biopsies from flat mucosa stored in Carnoy’s solution were processed, stained and microdissected as described previously.26 Ten intact, non-bifid crypts were counted. The length and breadth of each crypt were measured and the crypt was divided into 10 equal compartments starting from the base to the luminal surface of the crypt. The numbers of mitotic figures in each of the 10 compartments were identified and counted. Crypt microdissection and cell counting were performed by a single histopathologist who was blinded to the patient and treatment details.
A two-step real-time reverse transcriptase-PCR (RT-PCR) using the LightCycler480 SYBR green I Master (Roche Diagnostics, Burgess Hill, Sussex, UK) was used to quantify gene expression in response to starch treatment. RNA was extracted from tissues stored in RNAlater using the SV total RNA isolation system (Promega, Southampton, UK) as described by the manufacturer. Gene expression, relative to expression of the housekeeping gene 18S, was studied for two genes, CDK4 and GADD45A (table 1). In step 1, the reverse transcription of RNA into cDNA was performed outside the LightCycler system using the Moloney murine leukaemia virus RNase H+ reverse transcriptase enzyme (Promega). Standard curves for real-time RT-PCR were obtained using Caco 2 cell cDNA at dilutions ranging from 1:5000 to 1:80 000 for the housekeeping gene (18S) and dilutions from 1:5 to 1:160 for the target genes CDK4 and GADD45A. A melting curve was programmed into the LightCycler 480 protocol to access the specificity of the amplified PCR product and to look for any primer dimers, which have a lower melting point when compared with the target product.
RT-PCR amplification of the target genes CDK4 and GADD45 and the housekeeping gene 18S was carried out using the primer oligonucleotides (0.5 μmol) detailed in table 1 (VH Bio, Gateshead, UK) and the SYBR Green I master kit (Roche). The LightCycler 480 was programmed for one preincubation cycle at 95°C for 5 min, 45 amplification cycles at an annealing temperature of 55°C, one melting curve at 65°C and a cooling cycle at 40°C. The samples were run in duplicate and the amplification curves were compared with the standard amplification curves to obtain the normalised ratio of expression levels of the target genes in the samples.
Data collection and statistical methods
Data were collected in Excel (Microsoft) and Access (Microsoft) databases and analysed using MINITAB version 14 (Minitab, Coventry, UK) and SPSS version 15 (SPSS, Woking, UK) software. The normality of data distribution was tested, and Box Cox transformation was used if the data were not normal. Univariate analysis of variance and covariance were performed using the general linear model. Results are expressed as least square means (SEM), and p<0.05 was considered significant. For Study 1, the effects of the intervention were assessed using analysis of covariance with pretreatment values as a covariate. For Study 2, analysis of variance was used to compare the outcomes in patients receiving treatment starch (RS) as compared with placebo starch. In both studies, the outcomes were adjusted for potential confounding factors including age, sex, site of cancer, preoperative radiotherapy and preoperative immunonutrition by including them as covariates. For post-treatment data only, the results from both studies were pooled and re-analysed with the addition of “study” as a factor in the analysis.
RESULTS
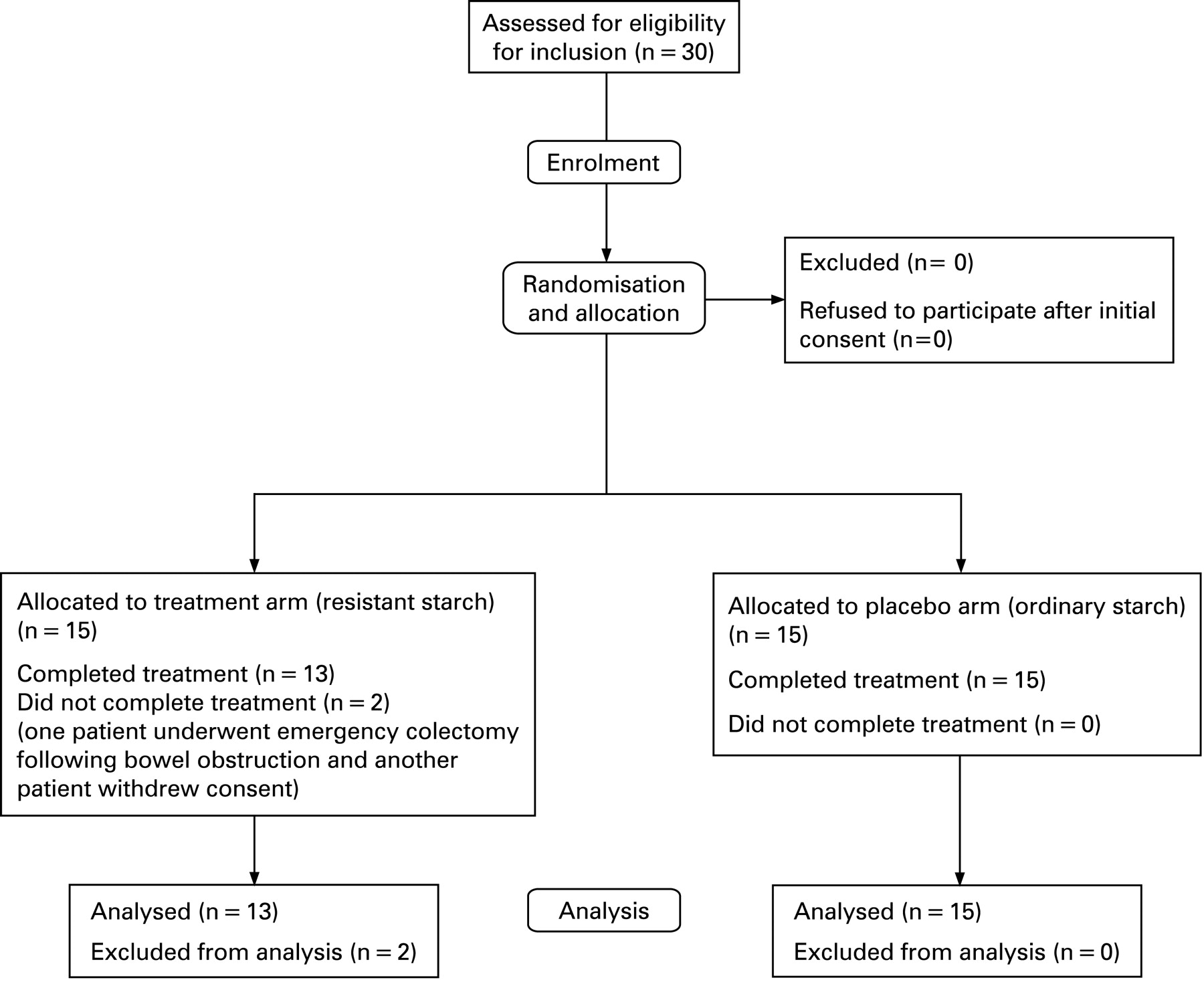
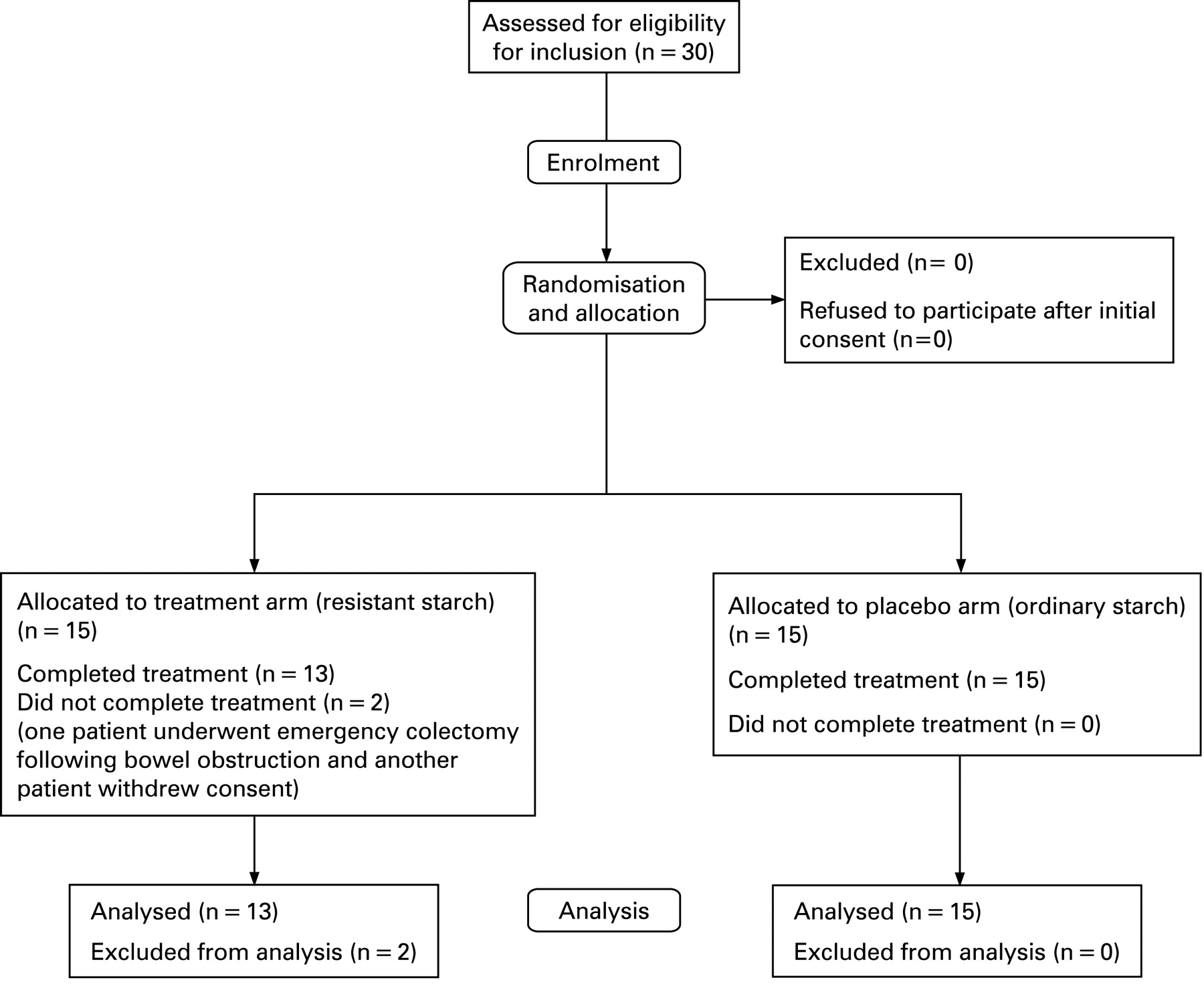
Of the total 65 patients who were randomised, 62 (95.4%) patients (35 male; 27 female) completed the starch treatment, of which 34 patients were in Study 1 and 28 patients in Study 2. The details of randomisation and patient flow through the studies have been illustrated in figs 1 and 2. Two patients who stopped taking starch as they did not like the taste and the third patient who underwent emergency surgery were excluded from the final analysis. The demographics, tumour location, details of preoperative treatment and histology of tumours are summarised in table 2. The subjects randomised to each of the two treatment groups (RS and OS) in both studies (Study 1 and Study 2) were comparable in their age and sex distribution, tumour location, preoperative short course radiotherapy and preoperative immunonutrition. Of the 34 patients in Study 1, 26 (76%) patients took starch treatment for ⩾3 weeks and 8 (24%) patients took starch for 2 weeks. In Study 2, 18 (64%) patients took the starch treatment for ⩾3 weeks and 10 (36%) patients took it for 2 weeks. Following starch treatment, 7 (23%) patients, of whom 4 patients were on RS and 3 patients were on OS treatment, complained of minor symptoms including a feeling of bloating, flatulence and bad taste, but there were no major side effects. These patients completed the starch treatment after reducing the dose of starch supplements to one sachet per day.

RS and tumour cell proliferation
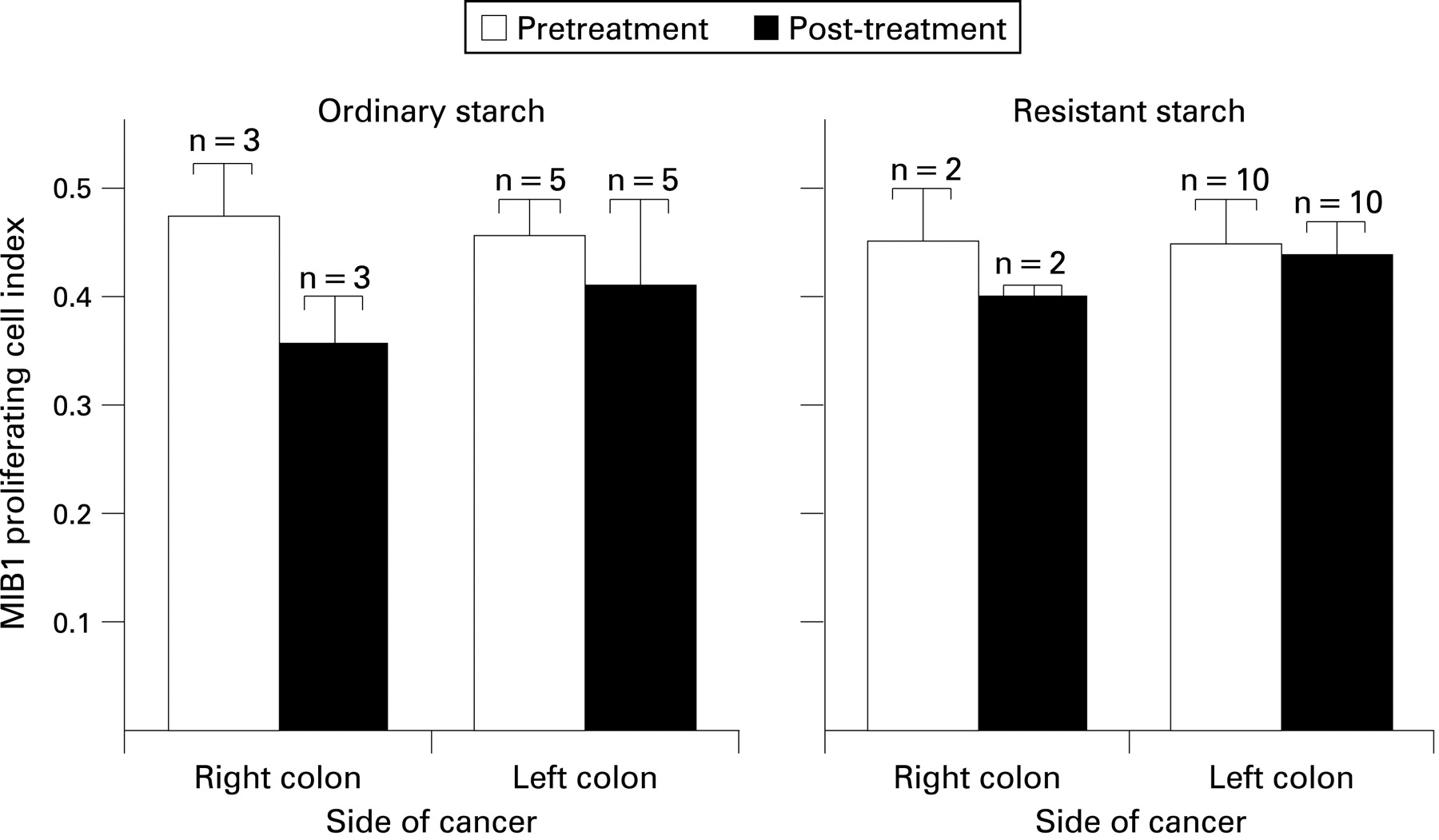
In Study 1, paired samples (pretreatment and post-treatment biopsies from each volunteer) were available from 34 patients, of whom 24 were randomised to treatment with RS and 10 were randomised to OS treatment. Across the groups there were no significant differences in the pretreatment (baseline) PCI of tumours (table 3). Following starch treatment, the covariates, site of cancer and percentage of proliferating cells in the pretreatment samples significantly influenced the PCI of tumours, whereas age and sex of the patients had no effect on these measurements. The reduction in PCI was greater for right-side colon cancers (cancers proximal to the splenic flexure) when compared with left-side colon cancers (cancers at and beyond the splenic flexure), and this reduction was seen in both treatment and placebo groups (fig 3). Overall, there was no effect of RS treatment (when compared with OS treatment) on the PCI of tumours in Study 1 (p = 0.84) (table 4).
In Study 2, post-treatment biopsies from tumours were available for 28 patients, of whom 15 were randomised to OS and 13 to RS treatment. There was no significant effect of RS when compared with OS on tumour PCI after adjusting for age, sex, preoperative radiotherapy and preoperative immunonutrition (p = 0.5) (table 5). Following analysis of pooled data from Studies 1 and 2, there was no significant effect of RS on tumour PCI (p = 0.42) (table 6).
RS and crypt cell kinetics
The pretreatment crypt dimensions, mitotic cells per crypt and percentage of mitotic cells in the top half of the crypt for patients in Study 1 have been detailed in table 3. There were more mitotic cells per crypt in the right colon when compared with the left colon (p<0.01), and this intersite difference was seen in both treatment and placebo groups. Following treatment for a median duration of 4 weeks, there were no detectable effects of RS when compared with OS on crypt length, crypt breadth and mean mitotic cell counts per crypt after adjusting for differences in age, sex, site of cancer and pretreatment measurements (table 4).
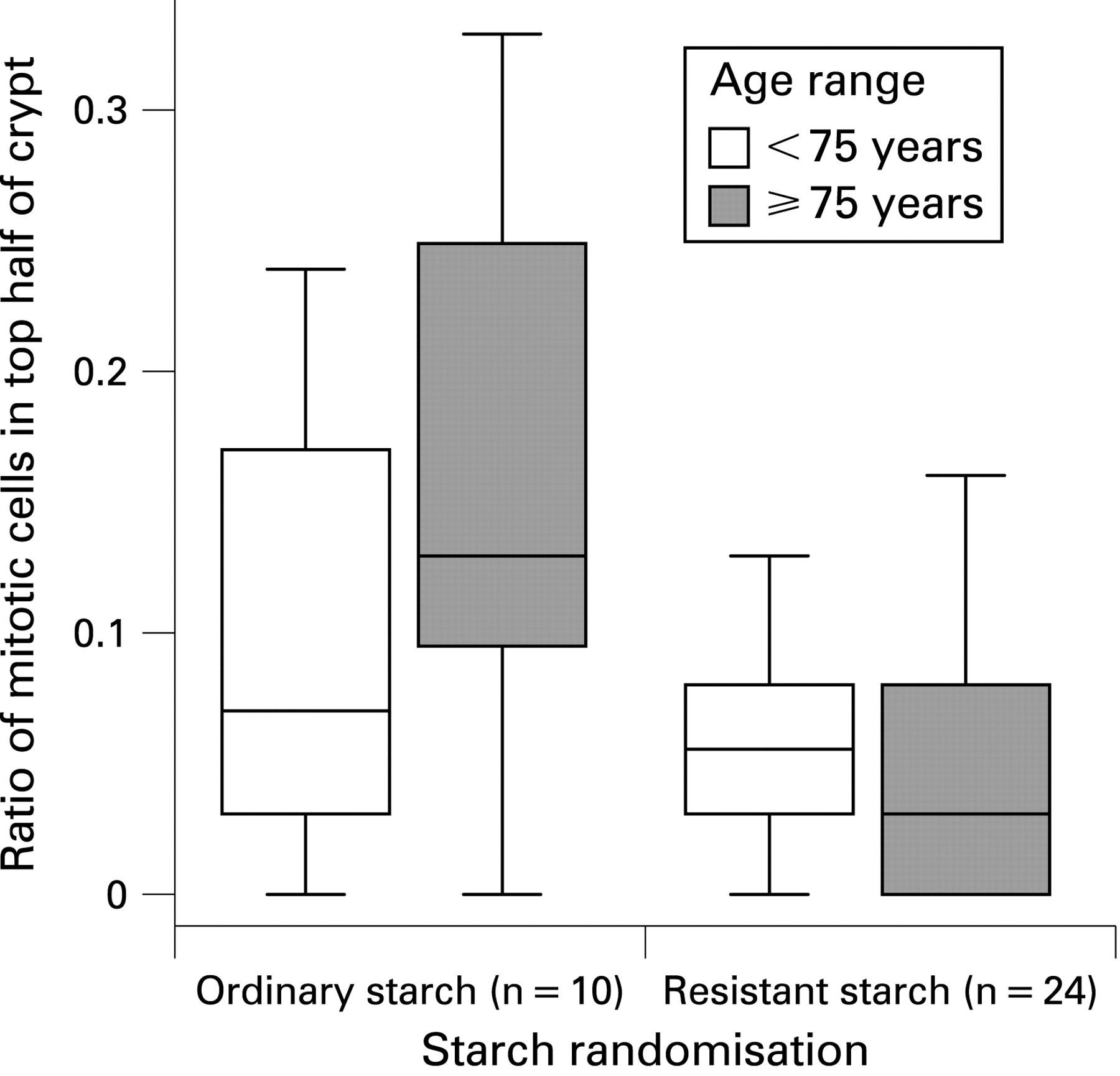
The proportion of mitotic cells in the top half of the crypt was reduced markedly by RS treatment when compared with placebo, and these differences were statistically significant (p = 0.028) after adjusting for differences in age, sex, site of cancer, duration of starch treatment, crypt dimensions and pretreatment measurements (table 4). Further post hoc analysis showed that this reduction in the proportion of mitotic cells in the top half of the crypt following RS treatment was greater in patients aged ⩾75 years when compared with patients <75 years (p = 0.011) but, since this was not a predefined analysis, this observation should be treated with caution (fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
In Study 2, RS treatment had no significant effect on crypt length, crypt breadth and total number of mitotic cells within the crypts (table 5). The proportion of mitotic cells in the top half of the crypt was 37% lower in the RS- compared with the OS-treated subjects, but this difference was not statistically significant (p = 0.14) (table 5). When data from Studies 1 and 2 were pooled, the proportion of mitotic cells in the top half of the crypt was 44% lower in the RS group when compared with the OS group but again the difference was not significant (p = 0.07) (table 6).
RS treatment and gene expression
In Study 1, paired samples were available for RT-PCR analysis from 26 patients, of whom 9 were randomised to OS treatment and 17 were randomised to RS treatment. Samples from the remaining patients in the study could not be used for RT-PCR analysis due to either inadequate quantity of tissue or poor quality of the extracted RNA. Overall there were no differences in the pretreatment expression of CDK4 and GADD45A genes in the tumours from the two treatment groups (table 7). Following RS treatment for a median duration of 4 weeks, expression of both CDK4 and GADD45A genes was markedly upregulated, but these effects failed to achieve statistical significance after adjusting for the differences in age, sex, site of cancer, preoperative radiotherapy and preoperative immunonutrition (p = 0.076 and 0.064 for CDK4 and GADD45A genes, respectively) (table 8).
In Study 2, poststarch treatment biopsy samples from tumour and from apparently normal flat colonic mucosa were available for RT-PCR analysis from 15 patients randomised to OS and 13 patients randomised to RS. There was significant upregulation in expression of CDK4 (p<0.01) and downregulation in expression of GADD45A (p<0.001) in the tumour tissue when compared with macroscopically normal mucosa (data pooled across both RS and OS treatment groups) (table 9). However, there were no significant differences in the expression of either of these genes following RS treatment when compared with OS treatment both in the tumour tissue and in the flat mucosa (table 10). Analysis of pooled data from both Studies 1 and 2 showed a more than twofold upregulation in expression of both CDK4 and GADD45A genes in tumour tissue in the RS treatment group when compared with the placebo group, and these effects were statistically significant (p = 0.02 and 0.04 for CDK4 and GADD45A genes, respectively) (table 11).
DISCUSSION
RS treatment and colorectal cancer cell kinetics
This is the first randomised human intervention study to investigate the antineoplastic effects of RS in patients with CRC. In animals, RS was shown to decrease mucosal cell proliferation, increase apoptosis and induce changes in gene expression.27 28 Few studies have attempted to replicate these effects using RS in humans (table 12). Although most of these studies reported an increase in the concentrations of SCFAs and, particularly, butyrate in the colonic lumen, only one study3 reported that RS supplementation produced a significant (but small) decrease in total crypt cell proliferation. This has not been confirmed in other studies, including the present study. Alteration in the distribution of mitotic cells in the crypts in normal flat mucosa is one of the earliest detectable premalignant changes occurring in the colon and is observed in the macroscopically normal appearing flat colonic mucosa in patients with CRC.26 29–31 In the present study, the proportion of mitotic cells in the top half of the crypt was reduced markedly (p = 0.028) following RS treatment, and adds support to the hypothesis that RS has antineoplastic effects in the human large bowel.32
In tumours, the proportion of mitotic cells, usually expressed as the PCI, is a major determinant of the biological behaviour of cancers, including tumour doubling time, metastatic potential and the response to chemotherapy and radiotherapy.33 We detected no effect of RS treatment when compared with OS treatment on tumour PCI, and studies of longer duration and/or larger scale may be necessary to detect such an effect.
It should not be assumed that the observed differences in crypt cell kinetics and PCI of tumours before and after treatment are due entirely to the starch intervention. The pretreatment samples were collected during colonoscopy while the post-treatment samples were obtained from the resected surgical specimens. Some of the study subjects had received preoperative immunonutrition. Although preoperative immunonutrition may reduce postoperative complication rates and length of hospital stay,34 there is no evidence for an effect of immunonutrition on tumour PCI. While all patients undergoing colonoscopy received bowel preparation, most patients having surgery for right-side cancers did not receive bowel preparation. Bowel preparation can affect the colonic microflora, which in turn has been shown to cause an increase in the metaphase index of aberrant crypt foci in normal colonic mucosa,35 but the effects (if any) of bowel preparation on tumour PCI are not known.
RS treatment and gene expression
Alterations in gene expression patterns have been reported in both colon cancer cells and the normal appearing colon mucosa of human colon cancer patients when compared with colonic mucosa from disease-free individuals.36–38 In the present study, we investigated the effects of oral supplementation with RS on the expression of two key butyrate-responsive, cell cycle regulatory genes, CDK4 and GADD45A, in CRC tissue and in the normal flat colonic mucosa.
CDK4 is a key cell cycle regulator gene which is overexpressed in a variety of human cancers,39 whilst reduced expression of GADD45A is associated with genomic instability and impaired growth control, and promotes tumourigenesis Results from the present study are consistent with this, showing that the baseline expression of CDK4 was significantly higher whereas the expression of GADD45A was significantly lower in tumour tissue compared with normal flat mucosa (table 9). Analysis of pooled data from Studies 1 and 2 revealed that CDK4 expression in tumours following treatment with RS for a median duration of 4 weeks was twofold higher than that in the OS group (p = 0.02) (table 11). It has been shown that butyrate can reduce tumour cell proliferation by inducing cyclin-dependent kinase inhibitors (CKIs), leading to G1 phase cell cycle arrest.40 Furthermore, these RS-treated CDK-enriched tumour cells may be targets for CKIs, leading to cell cycle arrest and reduction in cell proliferation.
Similarly, pooled data from both studies showed that GADD45A expression in tumour tissue was more than twofold higher following RS treatment as compared with OS treatment (p = 0.04) (table 11). In colorectal cancer cells in vitro, butyrate treatment results in GADD45A induction41 and GADD proteins are shown to play a vital role in maintaining genomic stability.42 The significant upregulation of its expression in tumour tissue following RS treatment in the present study suggests that GADD45A induction may play an important role in the molecular mechanisms underlying the antineoplastic effects of RS. In a recent study, GADD45A was one of 12 genes which were downregulated in primary colorectal tumours when compared with adjacent normal mucosa in patients with hepatic metastasis.43 Similarly, GADD45A was downregulated significantly in colonic tumours resistant to 5-flurouracil treatment.44 The role of RS in these patient subgroups needs to be investigated.
CONCLUSIONS
In summary, this study showed that RS supplementation for up to 4 weeks in patients with CRC reduced the proportion of mitotic cells in the top half of the crypt in macroscopically normal mucosa. Since cell proliferation in the upper part of the crypt is considered as a premalignant marker, its reduction by RS is consistent with an antineoplastic action of this food component. Furthermore, this study showed that RS treatment significantly induced expression of the key cell cycle regulatory genes CDK4 and GADD45A. These changes in gene expression may contribute to the molecular mechanisms underlying the antineoplastic effects of RS.
Acknowledgments
The authors thank Gail Barker and the staff of The CAPP2 Study for their help in providing starch samples for this study, Julie Coaker, Human Nutrition Research Centre, Newcastle University for her help with immuohistochemistry and crypt microdissection, and Allison Howard, Institute of Cell and Molecular Biology, Newcastle University for her help and advice in performing real-time RT-PCR. This study was undertaken as a part of the MD thesis of SSD who conducted the clinical study and wrote the first draft of this article. SSD will be acting as the guarantor of this submission. JMC contributed to real-time RT-PCR assays. SBK co-supervised the project and JB provided support, advice and starch samples. JCM was the principal investigator for the study and was responsible for study design. All authors have contributed towards drafting the manuscript and have approved the final draft submitted.
REFERENCES
Footnotes
-
See Commentary, p 327
-
Funding: This project was funded by the Biotechnology and Biological Sciences Research Council (BBRSC), UK (grant no. 13D/20173).
-
Competing interests: None.
-
Ethics approval: The study protocol and the subsequent amendments were approved by the local regional ethics committees and the research and development department of the local NHS Trust.
-
Patient consent: All patients enrolled in the study gave a written informed consent for their participation in the study and for the biopsies to be used exclusively for this study. No individual patient-identifiable information was used and all the patient data collected for this study were anonymised.