Article Text

Abstract
Background and aim Colorectal cancer (CRC) is a multifactorial disease with both environmental and genetic factors contributing to its development. The incidence of CRC is increasing year by year in Japan. Patients with CRC in advanced stages have a poor prognosis, but detection of CRC at earlier stages can improve clinical outcome. Therefore, identification of epidemiologial factors that influence development of CRC would facilitate the prevention or early detection of disease.
Methods To identify loci associated with CRC risk, we performed a genome-wide association study (GWAS) for CRC and sub-analyses by tumour location using 1583 Japanese CRC cases and 1898 controls. Subsequently, we conducted replication analyses using a total of 4809 CRC cases and 2973 controls including 225 Korean subjects with distal colon cancer and 377 controls.
Results We identified a novel locus on 6q26-q27 region (rs7758229 in SLC22A3, p=7.92×10−9, OR of 1.28) that was significantly associated with distal colon cancer. We also replicated the association between CRC and SNPs on 8q24 (rs6983267 and rs7837328, p=1.51×10−8 and 7.44×10−8, ORs of 1.18 and 1.17, respectively). Moreover, we found cumulative effects of three genetic factors (rs7758229, rs6983267, and rs4939827 in SMAD7) and one environmental factor (alcohol drinking) which appear to increase CRC risk approximately twofold.
Conclusions We found a novel susceptible locus in SLC22A3 that contributes to the risk of distal colon cancer in an Asian population. These findings would further extend our understanding of the role of common genetic variants in the aetiology of CRC.
- Cancer susceptibility
- colorectal cancer
- genetic polymorphisms
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Significance of this study
What is already known about this subject?
Inherited susceptibility was thought to account for ∼35% of all colorectal cancer (CRC).
Genome-wide association studies (GWASs) among European populations have identified a subset of CRC susceptibility loci.
Different genetic factors may contribute to the pathogenesis of distal colon cancer and proximal colon cancer.
What are the new findings?
A GWAS for CRC was conducted for the first time in an Asian population and identified a novel susceptible locus in SLC22A3 that was significantly associated with distal colon cancer.
Genetic and environmental factors play a crucial role in the development of CRC in this Asian population.
Interesting racial diversity between Asian and Caucasian populations in the pathogenesis of colorectal cancer was suggested.
How might it impact on clinical practice in the foreseeable future?
Our findings would contribute to the understanding of the cumulative role of genetic and environmental factors in colorectal carcinogenesis in the Asian population and also establish personalised medical treatment.
Introduction
Colorectal cancer (CRC) is the third most common cancer and the fourth leading cause of cancer death worldwide. The recent development of novel drugs and therapeutics has remarkably improved overall survival, and the 5-year survival rate is around 90% for patients who are diagnosed at stage I.1 However, the prognosis of patients with CRC in an advanced stage is still disappointing. Hence, identification of epidemiologicalfactors that influence development of the disease would facilitate its prevention or early detection and subsequently provide better prognosis.
Family history is acknowledged to be one of the strong risk factors, and an approximately twofold increased risk for CRC was observed among patients who have a first-degree relative with CRC.2 Thus, nearly 15% of patients with CRC have a positive family history of disease.3–5 Although inherited susceptibility was thought to account for ∼35% of all CRC,6 high-risk germline mutations in APC, DNA mismatch repair genes, MUTYH, SMAD4, BMPR1A, and LKB1 account for <6% of all cases.7 Therefore, the remaining heritable CRC risk (approximately 30%) would be caused by the combination of common variants with modest effects.
Recent genome-wide association studies (GWASs) among European populations have identified a subset of CRC susceptibility loci in 8q24,8 9 8q23.3 (EIF3H),10 10p14,10 11q23,11 15q13,12 18q21 (SMAD7),11 13 14q22.2 (BMP4),14 16q22.1 (CDH1),14 19q13.1(RHPN2),14 and 20p12.3.14 However, no GWAS for CRC in an Asian population has been performed. To explore the variants that predispose to the disease in an Asian population, we conducted a GWAS for CRC and sub-analyses by tumour location.
Methods
Study population
In this study, we used a total of 6167 CRC cases and 4494 control subjects from a Japanese population. CRC patients were categorised into two main groups (colon and rectal cancers) according to the tumour location. For the colon cancer, we further categorised into proximal colon (caecum, ascending colon, and transverse colon) and distal colon (descending colon, and sigmoid colon) cancers. Characteristics of each cohort are shown in table 1. Case samples of the Japanese population were obtained from BioBank Japan (http://biobankjp.org/).15 Control DNA samples in the screening stage were obtained from healthy volunteers (n=904, 74.4% males, mean age at diagnosis=52.5 years, SD±14.3) as well as from BioBank Japan (n=994, keloidosis, chronic hepatitis B, pulmonary tuberculosis, and drug rash). To increase the power to detect genetic factors related with CRC, we used cases with higher hereditary predisposition in our screening stage. CRC cases who developed the disease at a younger age (≤60 years old) or had at least one first-degree relative with a history of CRC were enriched in our screening stage cohort (62.80% and 35.5%, respectively) compared to the first replication (21.17% and 3.62%, respectively) and the second replication cohorts (21.62% and 8.28%) (supplementary table 1). Genotyping results of 2596 individuals that were registered in BioBank Japan were used as the controls for the first (ischaemic stroke and myocardial infarction) and the second (peripheral artery disease and arrhythmia) replication analyses. We excluded the subjects with cancers or diabetes from control groups. Patients with inflammatory bowel diseases (ulcerative colitis and Crohn's disease) were not included as either cases or controls. Cases and controls (healthy volunteers) for the third replication (n=225 and 377, respectively) were collected at Cancer Research Institute, Seoul National University College of Medicine, Korea. All the participants provided written informed consent.
Characteristics of study populations
SNP genotyping and quality control
Platforms used in each stage are shown in table 1. Analyses using Illumina Beadchip (Illumina, San Diego, California, USA) were conducted at the Center for Genomic Medicine, The Institute of Physical and Chemical Research. In the first and the second replication analyses, genotyping of case samples was conducted by the multiplex polymerase chain reaction-based Invader assay (Third Wave Technologies, Madison, Wisconsin, USA).16 Korean samples in the third replication analysis were genotyped using the Taqman assay (Applied Biosystems, San Francisco, California, USA). To evaluate the quality of each genotyping methods, we analysed rs7758229 in 96 CRC cases. Consequently, we observed more than 99% concordance between the result from direct sequencing and those from three genotyping systems (invader, Taqman, and Illumina Human610-Quad BeadChip). These findings indicated that different genotyping methods are not likely to cause the inflation of association in our study.
In the screening stage, we genotyped 1595 CRC cases and 1903 control subjects. These samples were genotyped using the Illumina Human610-QuadBeadChip in cases and the Illumina HumanHap550v3 BeadChip in controls. In fact, genotype concordance between these two BeadChips was 99.99% among 182 duplicate samples, indicating a low possibility of genotype error. The samples with a call rate of < 0.98 were excluded from our analysis (12 cases and five controls). Then we applied SNP quality control as follows: call rate ≥0.99 in cases and controls, Hardy–Weinberg p≥1×10−7 in controls. Finally, 496 531 common SNPs between Human610-Quad Beadchip and HumanHap550v3 Genotyping BeadChip on autosomal chromosomes passed the quality control criteria. We selected 391 749 SNPs with minor allele frequency (MAF) of ≥0.05 in either case or control samples for further analyses, considering statistical power in the replication analyses.
Statistical analysis
In the screening stage, the associations between each SNP and CRC were assessed using the Cochran–Armitage trend test. Thirty-six SNPs that exhibited false discovery rate Q value ≤0.2 (p≤2.5×10−5) were further analysed using an independent cohort consisting of 3099 CRC cases and 1777 controls. Sub-analyses by tumour location were also performed applying the same criteria (p≤2.5×10−5). The significance thresholds were set to be 0.05 in the first, second and third replication study, and 1.27×10−7 (0.05/391 749) in the meta-analysis. When we take account of the sub-group analyses for multiple testing correction, the genome-wide significance threshold is 2.54×10−8 (0.05/(391 749×5)). The statistical powers to detect a variant with OR of 1.3 and MAF of 0.2 were estimated to be 62.6%, 99.9% and 94.2% (screening stage, first and second replication) for CRC, and 19.1%, 95.8%, and 77.2% for distal colon cancer, respectively. ORs and CIs were calculated using the major allele as a reference. Since alcohol intake of more than two standard drinks (28 g of pure alcohol per day) was shown to increase the risk of CRC,17 we classified the subjects into three categories: non-drinkers (0–1 g/day of alcohol), light drinkers (1–28 g/day of alcohol), or heavy drinkers (≥28 g/day of alcohol). Multiple logistic regression analysis was used to assess the contributions of the confounding factors with the R program (version 2.8.1). Age and gender were designated as regulatory factors, and the following explanatory variables were included in the analysis: alcohol consumption status (0=non-drinker, 1=light drinker, 2=heavy drinker), tobacco smoking (0=never smoker, 1=smoker) and rs7758229 genotype (0=GG, 1=TG, 2=TT).
Imputation analysis
To investigate the region including SNP rs7758229, imputation of ungenotyped SNPs was conducted by MACH v1.0 (see URLs) using first screening GWAS dataset with reference to the release 27 JPT (Japanese in Tokyo, Japan) from the HapMap Project website. Imputed SNPs with an Rsq value <0.3 were excluded. We also genotyped two exonic SNPs (rs668871 and rs2292334) in 48 cases and 48 controls by direct sequencing and found that the results from imputation analysis were completely consistent with those from sequence analysis.
SNP discovery
We performed re-sequencing of the promoter region and all exons of the SLC22A3 gene using genomic DNA from 48 individuals with distal colon cancer and 48 healthy controls. Primers used for amplification and sequence analyses were indicated in the supplementary table 9.
Results
To identify common variants that influence CRC risk, we genotyped 1583 Japanese individuals with CRC and 1898 control individuals (supplementary figure 1A). To overcome the relatively low statistical power in the screening stage, patients under 60 years old who developed cancer or who had a positive family history were preferentially enrolled in the screening stage, as mentioned in the methods section. We also performed sub-analysis by tumour location (colon, proximal colon, distal colon and rectal cancer) to explore common variants that predispose to some subsets of CRC (supplementary figure 1B–E). Application of the Cochran–Armitage trend test to all the tested SNPs indicated that the genomic inflation factor λ was 1.05, 1.04, 1.02, 1.03 and 1.02 for the colorectal, colon, proximal colon, distal colon and rectal cancers, respectively (supplementary figure 2A–E). For CRC, the inflation factor λ was 1.05 in our study. Since the inflation factor is highly dependent on sample size,18 19 we calculated it by using 1000 cases and 1000 controls. As a result, the inflation factor becomes as small as 1.03, implying a low possibility of false positive associations due to population stratification.
SNPs with a false discovery rate Q value ≤0.2 (p≤2.5×10−5) in the screening stage were considered as candidates. Thus, 36 SNPs for CRC, 27 SNPs for colon cancer, 20 SNPs for proximal colon cancer, 18 SNPs for distal colon cancer, and nine SNPs for rectal cancer were selected for further analyses (supplementary tables 2–6). In the first replication study, we genotyped these candidate SNPs using independent cohorts consisting of up to 3099 cases and 1777 controls (table 1). Two SNPs for CRC (table 2) and one SNP for distal colon cancer (table 3) exhibited a p value lower than 0.05. Then we analysed these SNPs in 1485 CRC cases, 489 distal colon cancer cases, and 819 controls, respectively. As a result, all three SNPs showed a p value lower than 0.05 in the second replication study. Consequently, we identified a significant association between CRC and SNPs on 8q24 (rs6983267 and rs7837328, p=1.51×10−8 and 7.44×10−8, respectively; table 2), which have been reported to be associated with CRC in studies of Caucasian subjects.8 In addition, we identified a novel locus (rs7758229 on 6q26-q27) that was significantly associated with distal colon cancer. Meta-analysis of all stages showed a Mantel–Haenszel p value of 1.07×10−8 and OR of 1.29 (table 3). Since rs7758229 did not associate with any disease that was used in the control group in our study (supplementary figure 4), the case-mix cohort is not likely to affect the association between rs7758229 and distal colon cancer.
The combined results of screening stage, first replication and second replication analyses for colorectal cancer
Results of replication studies and meta-analyses for distal colon cancer
For this novel locus, we conducted a replication study using 225 Korean subjects with distal colon cancer and 377 controls. Although the association was not significant, we observed a similar trend in the samples from the Korean subjects (p=0.286 with OR of 1.16) and Mantel–Haenszel p value for independence had improved from 1.07×10−8 to 7.92×10−9 (OR of 1.28, Pheterogeneity=0.20; table 3) when we conducted a meta-analysis of the Japanese and Korean study with a fixed-effects model. Interestingly, rs7758229 exhibited a much stronger effect on the risk of distal colon cancer among younger populations and the patients with a family history of the disease (supplementary figure 5). Taken together, this association appears to be true.
SNP rs7758229 is located within an intron 5 of SLC22A3 (the solute carrier family 22, member 3), one of the organic cation transporter genes. Organic cation transporters are critical for the elimination of some drugs and environmental toxins. This SNP is located within a recombination hot spot between two linkage disequilibrium blocks spanning an approximately 350-kb region on chromosome 6q26-q27 (figure 1). To further investigate this candidate region, we conducted imputation analysis using a screening stage genome-wide dataset. As a result, many SNPs within the SLC22A3 gene locus indicated strong association (supplementary figure 3), suggesting a possible role of SLC22A3 in the pathogenesis of distal colon cancer. To identify the causative variant(s) that might alter the function or expression level of SLC22A3, all exons and the promoter region of SLC22A3 gene were re-sequenced using genomic DNA from 48 cases and 48 healthy controls. As a result, we identified three novel SNPs consisting of one non-synonymous SNP (novel v1, Serine106Glycine) in exon 1 and two synonymous SNPs (novel v2, novel v3) in exon 3 and 8 (supplementary table 7). In addition to these three novel SNPs, 19 tag SNPs were genotyped using 1916 distal colon cancer cases (screening stage, the first and the second replication studies) and 1818 controls (screening stage). Although three SNPs in intron 1 (rs884742) and intron 5 (rs3123636 and rs3106164) exhibited suggestive associations with distal colon cancer; no variants indicated stronger association than marker SNP rs7758229 (supplementary table 7).
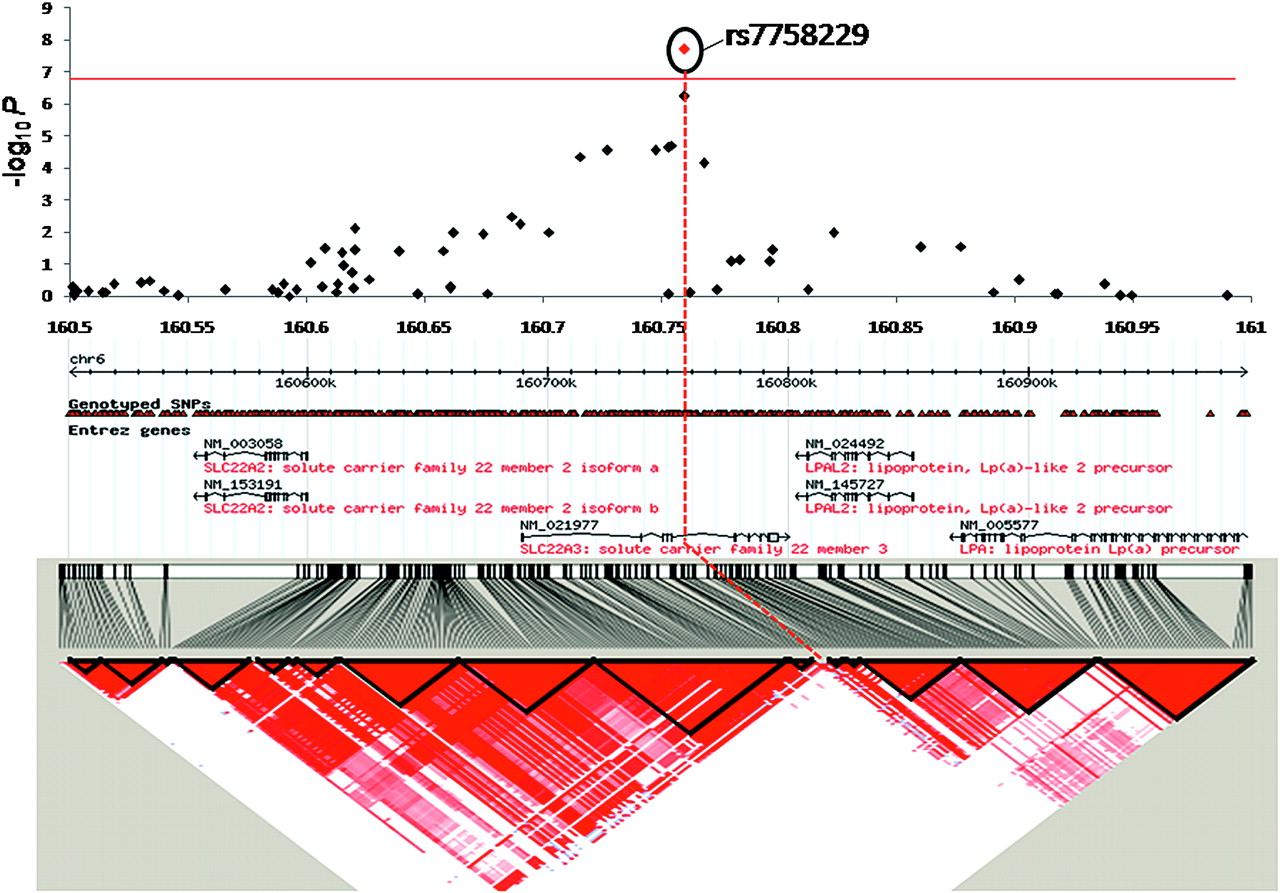
Case–control association results, genomic structure, and linkage disequilibrium map of chromosomal region of 6q26-q27. The top panel shows single-marker association results calculated by Cochran–Armitage trend tests. Results from the screening stage and combined analysis (screening stage, first and second replication studies) are indicated by black and red dots, respectively. The bottom panel shows the pairwise linkage disequilibrium for SNPs in HapMap JPT. The red line indicates the significance threshold after Bonferroni's correction for multiple testing (p=1.27×10−7).
The cumulative epidemiological evidence revealed that various environmental factors such as alcohol drinking, tobacco smoking, physical activity and diet would affect the risk of CRC.17 20 Since histories of alcohol drinking and tobacco smoking were available for most of case and control subjects, we performed multiple logistic regression analysis using alcohol drinking and smoking as covariates. As shown in table 4, rs7758229 and alcohol consumption are independent risk factors for distal colon cancer (p=5.61×10−9, OR of 1.31 and p=1.53×10−6, OR of 1.21, respectively) after adjustment of age and sex.
Logistic regression analysis
To assess the impact of SNP rs7758229 on CRC predisposition, we genotyped this variant using all CRC cases. As a result, this variant indicated suggestive association with colon cancer (p=7.40×10−7 with OR of 1.21; supplementary table 10) and CRC (p=1.31×10−5 with OR of 1.16; supplementary table 11), respectively.
We also analysed CRC loci that were reported in Caucasian GWASs using our screening stage cohort. Among the nine SNPs evaluated, SNP rs6983267 (p=1.08×10−5, OR of 1.25) and rs4939827 (p=9.54×10−5, OR of 1.25; SMAD7) indicated strong association. In addition, SNP rs10795668 showed moderate association (p=2.47×10−2, OR of 0.90), while the other six SNPs did not associate with CRC. Similar results were observed for all the nine SNPs when we used only 904 healthy subjects as control, and MAFs of all the nine SNPs in screening stage control samples were almost the same as those in the healthy control samples (supplementary table 8). These results suggest that these three variants are common CRC susceptible loci between Caucasian and Asian populations.
Then we assessed the combined impact of three genetic factors (rs6983267;8q24, rs4939827;SMAD7, and rs7758229;SLC22A3) and alcohol consumption on the risk of CRC. We assigned a score of 0, 1 or 2 for non-, light, and heavy drinkers, as well as a score of 1 for each risk allele of each SNP. Since patients with a score of 2 were most common in control subjects (30.6%), we used these subjects as a reference (figure 2A). As a result, individuals with a score of 5 or above have an approximately twofold higher risk of developing CRC compared with individuals with a scores of 2 (figure 2B). These results indicate that genetic and environmental factors play a crucial role in the development of CRC.

{kind=link}
{kind=link}
Impact of genetic and environmental factors on CRC susceptibility. Three genetic factors (rs6983267, rs4939827, and rs7758229) and alcohol consumption were used in the scoring system. We assigned a score of 0, 1, or 2 for non-, light, and heavy drinker, as well as a score of 1 for each risk allele. (A) Distribution of scores in CRC cases (white bars) and controls (black bars). (B) The OR and 95% CIs were indicated relative to the subjects with a score of 2. Horizontal line marks the null value (OR=1). The distribution of scores follows a normal distribution in both cases and controls, with a shift towards higher scores in cases.
Discussion
CRC that arises proximal or distal to the splenic flexure exhibits differences in incidence according to age, gender and ethnicity. For example, distal colon cancers predominantly occur in white males, while proximal colon cancers are frequent among older African–Americans females.21 22 The hereditary familial forms of CRC, familial adenomatous polyposis (FAP) and hereditary non-polyposis CRC (HNPCC) also exhibit markedly different clinical features.23 Nearly 100% of individuals with FAP will develop CRC in the distal colon.24 In contrast, approximately 70% of large bowel tumours in individuals with HNPCC arise in the proximal colon.25 In addition, mutations in TP53 are approximately 1.5- to 3-fold more frequent in distal colon cancer compare with proximal colon cancer.26 Recently, the incidence of colon cancer in Japan has been increasing.27 In addition, CRC occurs more frequently in the proximal colon and less frequently in the rectum among the Japanese–American population in Hawaii compared to native Japanese in Japan.28 These facts suggest that different genetic and environmental factors contribute to the pathogenesis of rectal, distal and proximal colon cancer, respectively.
To date, many studies have shown the associations between various polymorphisms and the risk of CRC, but few have analysed cancer risk by tumour location. In this study, we have identified a novel locus on 6q26-q27, tagged by rs7758229 in SLC22A3 which was significantly associated with distal colon cancer in Asians. The 6q26-q27 region contains four genes, including SLC22A2, SLC22A3, LPAL2 and LPA. Imputation analysis of 6q26-q27 region indicated that SNPs around SLC22A3 revealed strong associations. Interestingly, SNP rs9364554 in intron 5 of SLC22A3 was shown to associate with prostate cancer in Caucasian populations.29 Thus SLC22A3 is likely to be associated with multiple cancers.
SLC22A3 is a member of the organic cation transporter family that is highly expressed in liver, kidney, intestine and brain.30 This family members play a critical role for the transport of cationic drugs, toxins, and endogenous metabolites.31 SLC22A3 is expressed in many cancer cell lines, such as colorectal and kidney cancers, and its expression level is correlated with the sensitivity to chemotherapeutic agents.32 33 Since several toxins or endogenous metabolites such as lipopolysaccharide34 and linoleic acid metabolite35 were shown to induce tumour formation, SLC22A3 might be involved in colorectal tumorigenesis through the clearance of some carcinogen.
Numerous studies have indicated that alcohol drinking could be positively associated with CRC risk. In addition, alcohol intake increases the risk of distal colon cancer17 and/or rectal cancer36 37 than proximal colon cancer. Furthermore, the effect of alcohol drinking is stronger among Asian populations because of their relatively high prevalence of a slow-metabolising aldehyde dehydrogenase variant.15 38 Similarly, our study validated that alcohol consumption was strongly associated with distal colon cancer in the Japanese population.
In summary, we have identified a novel susceptible locus in SLC22A3 that contributes to a risk of distal colon cancer. The incidence of CRC was increasing with the Westernisation of lifestyle and dietary habit in Japan.39 However, only three of nine CRC susceptibility loci from studies of Caucasians exhibited a p value of less than 0.05 in our study. These results suggest an interesting racial diversity between Asians and Caucasians in the colorectal pathogenesis. Although further functional studies are essential, our findings extend the understanding of the cumulative role of genetic and environmental factors in the colorectal carcinogenesis in the Asian population.
URLs for items used in the imputation analysis
R statistical environment, http://cran.r-project.org/; PLINK, http://pngu.mgh.harvard.edu/∼purcell/plink/; MACH 1.0, http://www.sph.umich.edu/csg/abecasis/mach/.
Acknowledgments
We are grateful to members of The Rotary Club of Osaka-Midosuji District 2660 Rotary International in Japan for supporting our study. We thank technical staff of the Laboratory for Genotyping at RIKEN for their technical assistance. We also thank A Matsui for her helpful technical assistance.
References
Supplementary materials
online only appendix
Files in this Data Supplement:
Footnotes
Funding This study was funded by the Ministry of Education, Culture, Sports, Science, and Technology, Japan.
Competing interests None.
Ethics approval This project was approved by the ethics committees at the Institute of Medical Science, the University of Tokyo, the Center for Genomic Medicine (formerly, SNP Research Center), Institutes of Physical and Chemical Research (RIKEN), and Seoul National University College of Medicine.
Provenance and peer review Not commissioned; externally peer reviewed.