Article Text

Abstract
Background Lifestyle interventions focusing on weight loss remain the cornerstone of non-alcoholic fatty liver disease (NAFLD) management. Despite this, the weight losses achieved in research trials are not easily replicated in the clinic and there is an urgent need for therapies independent of weight loss. Aerobic exercise is not well sustained and the effectiveness of the better tolerated resistance exercise upon liver lipid and mediators of liver lipid has not been assessed.
Methods Sedentary adults with clinically defined NAFLD were assigned to 8 weeks of resistance exercise (n=11) or continued normal treatment (n=8).
Results 8 weeks of resistance exercise elicited a 13% relative reduction in liver lipid (14.0±9.1 vs 12.2±9.0; p<0.05). Lipid oxidation (submaximal RQ ∆ −0.020±0.010 vs −0.004±0.003; p<0.05), glucose control (−12% vs +12% change AUC; p<0.01) and homeostasis model assessment insulin resistance (5.9±5.9 to 4.6±4.6 vs 4.7±2.1 to 5.1±2.5; p<0.05) were all improved. Resistance exercise had no effect on body weight, visceral adipose tissue volume, or whole body fat mass (p>0.05).
Conclusion This is the first study to demonstrate that resistance exercise specifically improves NAFLD independent of any change in body weight. These data demonstrate that resistance exercise may provide benefit for the management for non-alcoholic fatty liver, and the long-term impact of this now requires evaluation.
- Liver disease
- physical activity
- glucose control
- body composition
- fat oxidation
- diabetes mellitus
- fatty liver
- glucose metabolism
- lipid oxidation
- obesity
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
- Liver disease
- physical activity
- glucose control
- body composition
- fat oxidation
- diabetes mellitus
- fatty liver
- glucose metabolism
- lipid oxidation
- obesity
Significance of this study
What is already known about this subject?
Lifestyle interventions incorporating weight loss improve liver fat in NAFLD.
Weight loss is difficult to achieve in clinical practice.
Evidence on the effect of exercise on liver fat is insufficient, limiting the effective use of exercise in clinical care.
What are the new findings?
Resistance exercise reduces liver fat independent of weight loss in people with NAFLD.
Resistance exercise improves fat oxidation independent of weight loss in people with NAFLD.
Resistance exercise improves glucose control independent of weight loss in people with NAFLD.
How might it impact on clinical practice in the foreseeable future?
Helping people achieve and sustain a physically active lifestyle is one of the most pressing clinical needs for NAFLD management.
This study demonstrates that resistance exercise holds clinical benefits, independent of weight loss, and provides an alternative to aerobic exercise.
The lower cardiorespiratory demand may also make resistance exercise more accessible to patients than aerobic exercise, improving long-term sustainability.
Non-alcoholic fatty liver disease (NAFLD) represents a spectrum from asymptomatic steatosis to potentially life-threatening non-alcoholic steatohepatitis, with an overall prevalence of NAFLD in western countries of 20–30%.1 Patients with simple steatosis have a relatively benign ‘liver’ prognosis with a 1–2% risk of developing clinical evidence of cirrhosis over 15–20 years. Patients with non-alcoholic steatohepatitis and fibrosis can progress to cirrhosis at a rate of approximately 12% over 8 years.2 Once cirrhosis develops, patients are at a high risk of developing hepatic decompensation and of dying from a liver-related cause.
To date, weight loss is the only confirmed therapy for the treatment of NAFLD, and lifestyle interventions remain the cornerstone of management.1 2 Thiozolidinedione therapy has shown promise in providing a temporary reduction in liver fat,3 4 although progressive weight gain, side effects and cost have prevented them from being used in routine care. Lifestyle interventions have been shown to reduce markers of liver lipid and metabolic control5–7 in addition to reducing intrahepatic lipid (IHL).8–11 However, weight loss is difficult to achieve and sustain. Physical activity and exercise in NAFLD management could potentially be effective in decreasing IHL. Cross-sectional studies have shown that higher levels of physical activity are associated with lower levels of IHL.5 12 13 To date, two studies have reported a beneficial effect of aerobic exercise regimes upon liver function, independent of weight loss.14 15 However, the use of aerobic exercise may not be optimal as the high cardiorespiratory demand is associated with fatigue and discomfort, and long-term compliance is poor. Population-based studies13 suggest that resistance exercise is associated with lower levels of IHL. Resistance exercise has a lower cardiorespiratory demand and is associated with similar metabolic benefits. There have been no previous studies of the direct effect of resistance exercise upon IHL and metabolism, even though it has clear advantages in terms of acceptability and sustainability.16 17
The primary aim of this study was to determine the effect of resistance exercise without weight loss, on IHL in adults with NAFLD. The secondary aims were to determine the effect of resistance exercise on mediators of IHL; glucose tolerance and insulin sensitivity, fat oxidation, abdominal adiposity and body composition.
Experimental procedures
Twenty-eight people with NAFLD were screened for this study. Seven were excluded after screening (two transpired to be taking insulin for their diabetes; one was excluded due to an abdominal hernia; four due to <5% IHL on baseline MRI). Twenty-one sedentary (≤60 min vigorous activity per week) adults with clinically defined non-advanced NAFLD were therefore randomly assigned to either exercise (n=11) or standard care (n=10). The study was powered to detect a 2.02% absolute change (∆) in intrahepatic lipid between the treatment and control groups (SD 2.8%, α 5% and β 50%), based on changes reported from an aerobic exercise study in NAFLD.14 Non-advanced NAFLD was defined as greater than 5% IHL and a score of less than −1.445 on the NAFLD fibrosis scoring system,18 which indicates a lower percentage chance of having stage 3/4 fibrosis. General descriptions can be found in table 1. Exclusion criteria included heart or kidney disease, implanted ferrous metal, pre-existing medical conditions preventing participation in the exercise programme, insulin sensitising treatment or dietary change (for people with type 2 diabetes mellitus, diet and metformin were acceptable for inclusion if stable for 6 months) and alcohol intake above 21 units for men or 14 units for women. Subjects would be excluded from analysis if body weight changed more than 2.5% from baseline during the study as this could have an independent effect on IHL. The study protocol was approved by County Durham and Tees Valley 2 Research Ethics Committee. All participants provided written informed consent. Following an initial screening visit, glucose control, lipid oxidation, abdominal lipid depots and liver lipid were measured at baseline and after the 8-week intervention.
Subject characteristics
Progressive exercise test/screening visit
At baseline, a medical history, full physical examination and progressive exercise test were used to screen for undiagnosed cardiac disease. Resting 12-lead ECG (Custo med GmbH, Ottobrunn, Germany) and blood pressure (Suntech Tango+, Suntech Medical Ltd, Oxford, UK) were measured, in a seated position, to determine normal cardiac function. Peak oxygen consumption was determined using an electronically braked recumbent cycle ergometer (Corival Lode BV, Groningen, The Netherlands). Following a 5 min warm up at 25 W, resistance was increased by 1 W per 8 s until the participant could no longer maintain a cadence of 60 rpm, chose to stop, or continuing was contraindicated. The ECG was used to monitor heart rhythm continuously and blood pressure was measured every 2 min during the exercise test. Expired gases were collected using a Hans Rudolf breathing mask and analysed online for oxygen consumption, carbon dioxide elimination and ventilation (CORTEX Biophysik, Leipzig, Germany).
Physical activity
Physical activity and energy expenditure were assessed objectively using a validated19 multisensor array (SenseWear Pro3, Bodymedia Inc, Pennsylvania, USA) worn on the right upper arm for 7 days before random assignment and for the final 7 days of the intervention. The armband provided estimates of daily energy expenditure, average metabolic equivalents, sedentary time, duration and intensity of physical activity, number of steps, sleep duration and duration armband worn.
Anthropometry
Body weight and body composition were measured using an electronic scale and air displacement plethysmography (BodPod, Life Measurement Inc, California, USA).20–22 Height was measured with a stadiometer (SECA 799; SECA, Birmingham, UK). Waist circumference was measured at the midpoint between the lower costal margin and the level of the anterior superior iliac crests. Hip circumference was measured at the level of the greater trochanter.
Liver and abdominal fat measurement
Magnetic resonance studies were performed using a 3 Tesla Philips Achieva scanner (Philips Medical Systems, Best, The Netherlands). Following an 8 h fast, IHL was measured by localised 1H-MRS (PRESS, TR/TR 3000 ms/35 ms, 3×3×3 cm voxel, SENSE torso array). Blinded quantification of the spectra (water and CH2 resonances) was performed using the java-based magnetic resonance user interface (jMRUI version 3.0).23 24 Following manual first and second order phase correction, spectra were analysed using a non-linear least squares algorithm (AMARES).25 IHL was expressed as a percentage of liver volume, corrected for proton density of water and lipid.26
Subcutaneous and visceral fat content was performed by acquiring images at the L4/L5 junction using a three-point Dixon sequence (TR/TE/number of averages/flip angle 50 ms/3.45, 4.60, 5.75 ms/1/30°, matrix 160×109, median field of view (FOV) 440 mm, range 400–480 mm to suit subject size with 70% phase FOV). The slice was acquired during a breath-hold and with slice thickness of 10 mm.27 28 Fat and water were separated, and binary gating applied to produce a map of structures containing more than 50% fat, identified as subcutaneous and visceral fat. A watershed algorithm was used to divide the binary image into distinct areas and allowed easy separation of the subcutaneous and visceral fat. ImageJ29 was used to subtract the two areas to produce the area of visceral fat.
Glucose control
Following an 8 h overnight fast a cannula was inserted into a forearm vein. A 75 g glucose load (Lucozade Original; GlaxoSmithKline, Brentford, UK) was consumed within 5 min. Blood samples were taken at times 0, 5, 10, 15, 20, 30, 40, 50, 60, 75, 90 and 120 min. Samples were analysed for whole blood glucose (YSI 2300 Stat Plus-D; Yellow Springs Instruments, Yellow Springs, Ohio, USA), plasma non-esterified fatty acid (NEFA) (NEFA-HA; Wako Ltd, Osaka, Japan) and plasma insulin (Coat-A-Count Insulin RIA kit; Diagnostic Products Corporation, California, USA). The area under the curve for the resulting glucose response profile was calculated using the trapezoidal rule30 and insulin resistance determined using the homeostasis model assessment insulin resistance (HOMA–IR).31 NEFA suppression was assessed during the frequently sampled oral glucose tolerance test (fsOGTT) and the 0–30 min change used as a measure of NEFA suppression.32
Fasting samples were also analysed in a clinical pathology accredited laboratory (Newcastle Upon Tyne Hospital NHS Foundation Trust, Department of Clinical Biochemistry) for: ALT, total cholesterol, triacylglycerols and haemoglobin A1c (HbA1c). Serum samples were collected in silica clot activator polymer gel containing vacutainers (BD Diagnostics, Plymouth, UK)—total cholesterol, triacylglycerols and ALT were measured using a Roche Modular P and test kits (Roche Diagnostics Ltd, Burgess Hill, UK), respectively. HbA1c was measured using a TOSOH HLC-723G7 (Tosoh Corporation, Tokyo, Japan).
Lipid oxidation at rest and submaximal exercise
Resting substrate oxidation was determined by expired gas analysis using a Hans Rudolf breathing mask while participants lay supine for 30 min in a quiet room. The first 15 min were an acclimatisation period and the second 15 min were used to determine resting substrate oxidation. Following a 5-min warm up on the recumbent cycle ergometer at 25 W, resistance was increased to 50% of the maximal oxygen uptake determined at screening and maintained for 60 min. Expired air was collected every 15 min. Respiratory quotient was calculated from oxygen consumption/carbon dioxide elimination.
Study intervention
Resistance exercise was performed three times per week on non-consecutive days for 8 weeks. The programme consisted of eight exercises: biceps curl; calf raise; triceps press; chest press; seated hamstrings curl; shoulder press; leg extension and lateral pull down (Precor, Woodinville, USA). Each session lasted between 45 and 60 min and consisted of a 10 min warm-up at approximately 60% maximum heart rate on a cycle ergometer followed by resistance exercise done as a circuit, ending with a repeat of the warm-up described. The one repetition maximum was measured33 at baseline and following the intervention. Initially, participants did two circuits using 50% of their one repetition maximum, progressing to three circuits, using a minimum 70% of their one repetition maximum by week 7. Participants were encouraged to increase the resistance used each week when possible. Biweekly supervised sessions were used to encourage adherence and progression and to resolve any problems. Heart rate was recorded during each session (Polar RS400; Polar Electro Oy, Kempele, Finland) and was used alongside exercise logs to assess adherence.
Statistics
Following tests for normal distribution, between-group differences were evaluated using an unpaired t-test and within-group differences using a paired t-test (two way). Treatment group × time interactions were assessed using a two-way analysis of variance. Analyses were performed using Minitab version 15 (Minitab Inc., State College, Pennsylvania, USA). Statistical significance was set at p<0.05. Data are mean±SD unless otherwise stated.
Results
No subjects withdrew during the trial and all subjects allocated to the exercise group completed all 24 sessions of resistance exercise training. Two subjects (controls) were excluded from analysis (one individual lost >5% of his body weight during the 8-week period and one had a change in his diabetes medication). Nineteen subjects (eight control; 11 exercise) completed the study. The groups were well matched for weight, body mass index and waist/hip circumference (table 1). The exercise group were younger (52±13.3; range 33–72 years) compared with the control group (62±7.4; range 51–71 years; p=0.05). There was no correlation between age and change in IHL (p>0.05).
Anthropometry and body composition
Body mass index remained constant in both groups during the study (32±4.9 to 32±4.5 vs 32±4.8 to 32±4.2 kg.m2 in exercise and control). There were no significant changes in weight, waist or hip circumference, waist to hip ratio, body composition, visceral or subcutaneous fat in either group (see tables 1 and 2).
Intrahepatic lipid concentration, subcutaneous and visceral adipose tissue, body composition, glucose control, insulin sensitivity, NEFA suppression index and substrate oxidation during submaximal exercise
Intrahepatic lipid
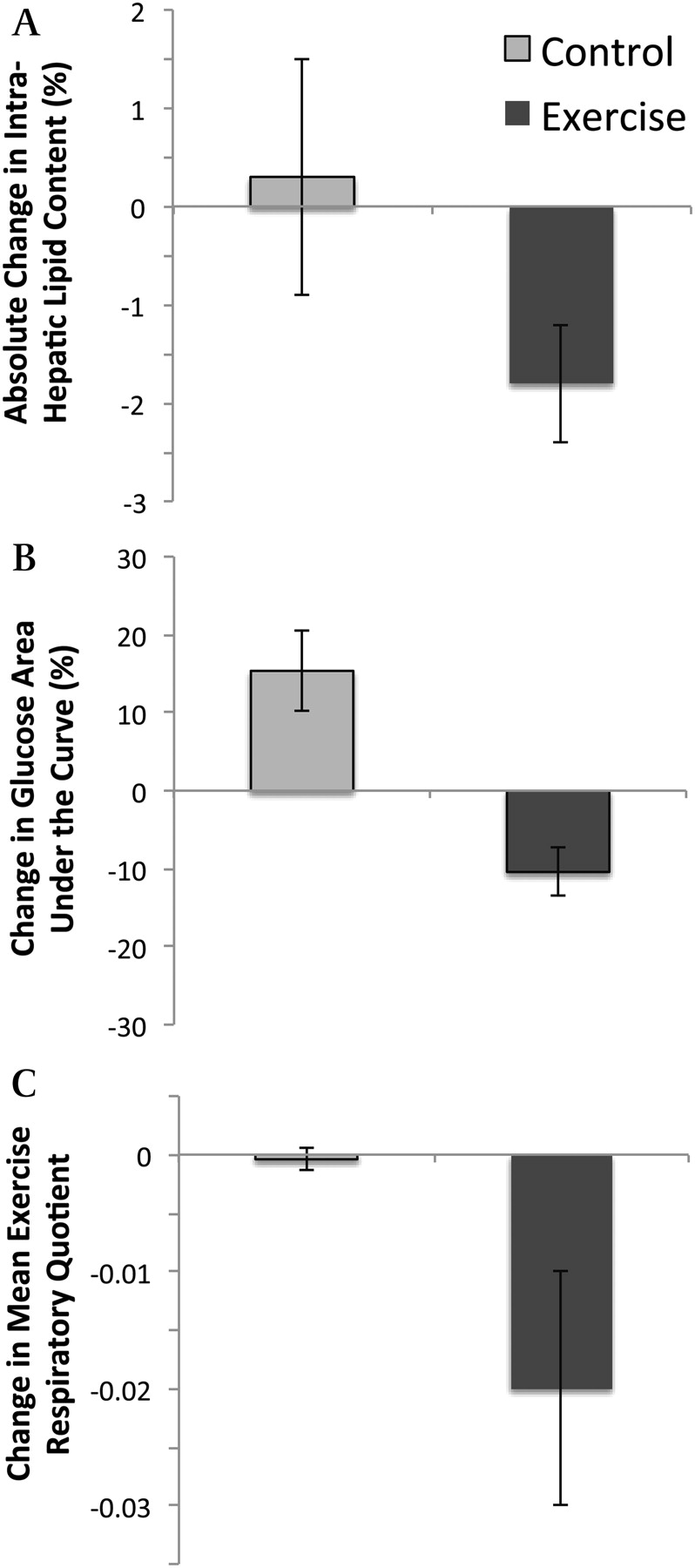
Resistance exercise elicited a 13% relative reduction in IHL with no change in the control (p<0.01; table 2, figure 1A). There was a significant time by treatment interaction for resistance exercise (p<0.05; table 2, figure 1A) although the significant fall in IHL did not achieve a significant difference between the two groups at the end of the intervention. However, three of the participants in the exercise group moved from having clinically significant NAFLD to being within normal limits (<5% IHL). No control subject moved into the normal liver fat range. The change in IHL with both groups combined was weakly associated with the change in the number of steps walked per day (R2=0.28, p<0.05), but not with active energy expenditure (R2=0.06, p>0.05).

{kind=link}
Effect of 8 weeks resistance exercise training (Exercise) or continued standard care (Control) on intrahepatic lipid (A), glucose control from the frequently sampled oral glucose tolerance test (B) and respiratory quotient during submaximal exercise (C); values are means±SE. *Significantly different from control (p<0.05). **Significantly different from control (p<0.01).
Blood lipids and liver enzymes
There were no significant changes in blood lipids or ALT in either group (table 1).
Glucose control
The exercise group demonstrated improved glucose control after 8 weeks as indicated by a decrease in glucose area under the curve during the fsOGTT compared with control (p<0.01; figure 1B; table 2). The exercise group showed a significant improvement in insulin sensitivity after 8 weeks, as demonstrated by a decrease in HOMA–IR (5.9±5.9 to 4.6±4.6 vs 4.7±2.1 to 5.1±2.5; p<0.05; table 2), although time by treatment interaction for resistance exercise and insulin resistance just missed statistical significance (p=0.055). Fasting insulin levels remained relatively unchanged in both groups (table 2). Fasting glucose levels were reduced in the exercise group after the intervention compared with the control but this was not statistically significant (6.0±2.1 to 5.2±0.9 vs 5.9±2.3 to 6.4±3.3 mmol/l; p=.086). Time by treatment interaction for resistance exercise and change in fasting glucose was just outside statistical significance (p=0.06). HbA1c remained relatively unchanged in both groups (table 1).
NEFA suppression
Fasting plasma NEFA remained unchanged by the intervention. Similarly, the extent of NEFA suppression during the fsOGTT remained constant in both groups (table 2).
Fat oxidation
Resistance exercise brought about an increase in fat oxidation during the submaximal exercise test (respiratory quotient 0.93±0.02 to 0.90±0.01 vs 0.90±0.02 to 0.89±0.02, p<0.05; p<0.05 time by treatment interaction; table 2; figure 1C). Resting fat oxidation remained constant in both groups (table 2).
Physical activity
There was a wide range of habitual daily activity (number of steps taken daily measured by Sensewear) in both groups at baseline (range 5046–12 479 exercise, mean 8692; range 2781–9159 control, mean 5682). The total number of steps taken on a daily basis was significantly higher in the exercise group post-intervention when compared with the controls (9848±3338 vs 5883±3073; p=0.028).
Discussion
This is the first study to examine the effects of resistance exercise on IHL and its mediators in adults with NAFLD. An 8-week resistance exercise programme brought about an approximately 13% reduction in liver fat. This was accompanied by an approximately 12% increase in insulin sensitivity, and increased fat oxidation during submaximal exercise in the absence of any change in body weight.
Although lifestyle modification combining dietary change and exercise produces a robust reduction in IHL,1 the data on exercise alone is less definitive. We demonstrated that resistance exercise without weight change is effective in reducing IHL in people with NAFLD. Resistance exercise provides an alternative to aerobic exercise; it improves muscular strength, muscle mass and metabolic control, safely and effectively, in vulnerable populations independent of weight loss.16 It places less of a demand on the cardiorespiratory system and may therefore be accessible to more patients.17 All participants completed the 8-week programme, showing good adherence and tolerance.
To date, only two studies have reported the effect of exercise alone on liver health in adults with NAFLD, both having used aerobic exercise, but only one reported a direct measure of IHL. A 4-week aerobic exercise intervention showed a similar absolute reduction in IHL (1H-MRS) as seen during the present study. The aerobic exercise brought about a reduction in IHL from 8.6% to 6.8%.14 A 12-week intervention reported a 47% (47 U/l) and 48% (30 U/l) reduction in ALT and AST, respectively.15 However, these biomarkers can be elevated in the absence of excess liver fat and within the normal range in the presence of elevated liver fat, making them poor indicators for IHL.34–36 Interestingly, the present study is the first to monitor habitual physical activity alongside exercise therapy. These data suggest that changes in physical activity habits and the brief aerobic warm up accompanying resistance exercise contributed to the change in IHL only to a small extent. Although the changes in IHL following exercise therapy are significant, the absolute change (∼2% IHL) was modest compared with the approximately 10% reduction reported after an 8 kg weight loss from caloric restriction.37 Therefore, the clinical value of exercise in NAFLD appears likely to be as an adjunct to caloric restriction.
Our observed improvement in glucose control is consistent with findings in populations with impaired glucose control or type 2 diabetes mellitus.38 39 The aerobic exercise studies in NAFLD have either reported no change14 or not reported measures of glucose control.15
We observed a pure exercise effect on IHL, which did not involve any change in visceral fat in the patients. There is increasing evidence that the two depots are not mechanistically linked but both tend to reflect adiposity.3 Recent findings from the Framingham Heart Study,40 and a much smaller cohort,41 show IHL to be associated with dyslipidaemia and dysglycaemia independently of visceral fat. Our observation of decreased IHL in the absence of any observable change in visceral or subcutaneous fat provides further information on the separate regulation of IHL and visceral fat.
The mechanisms underlying the change in IHL following exercise are likely to reflect changes in energy balance, circulatory lipids and insulin sensitivity. Insulin sensitivity plays a significant role in IHL homeostasis. High levels of circulatory insulin upregulate SREBP-1c and ChREBP expression in the liver,42 43 stimulating de novo lipogenesis and increasing IHL. In healthy normoglycaemic humans, hepatic de novo lipogenesis contributes approximately 5% and 18–23% of IHL in the fasted and postprandial states, respectively.44 Whereas de novo lipogenesis is constantly elevated in those with NAFLD contributing approximately 26% of IHL irrespective of feeding state,45 elevated circulating triacylglycerols exacerbate this problem by impeding insulin-stimulated glucose uptake.46 This creates a vicious cycle in which elevated IHL levels impede hepatic insulin action, causing increased portal insulin levels and further increasing IHL.47
Our findings suggest that the introduction of resistance exercise breaks this cycle by improving glucose control and fat oxidation. Our observations would support other reports that resistance exercise increases whole-body glucose disposal48 at least partly due to increases in skeletal muscle GLUT4, glycogen synthase expression and activity, insulin receptor and glycogen storage.49 Skeletal muscle in the resistance exercising individual can thus act to sequester circulating fatty acids and glucose safely, reducing the impact of insulin-stimulated de novo lipogenesis in the liver. Aerobic exercise has been shown to increase intramyocellular triacylglycerol synthesis,50 51 while decreasing the accumulation of fatty acid metabolites and suppressing the proinflammatory state associated with insulin resistance.52 It remains to be determined whether exercise has any direct transcriptional effects on the liver. Furthermore, as patients with fibrosis were excluded, the benefits of resistance exercise upon the progression of liver disease versus metabolic control cannot be disentangled. It is also important to highlight that IHL is part of the early adaptive response to stress rather than a first hit in disease progression. As such, IHL represents a biomarker of NEFA flux, oxidative, endoplasmic reticulum (ER) and cytokine-mediated stress that results in steatosis and progressive liver damage.53
In conclusion, well-tolerated resistance exercise reduced IHL, increased insulin sensitivity, and improved metabolic flexibility in NAFLD independent of weight loss. The absolute effect of resistance exercise studied in isolation was modest but similar to that of aerobic exercise. The benefits of resistance exercise combined with caloric restriction in the clinical management of NAFLD will depend upon long-term maintenance and sustainability of exercise—this now needs to be investigated.
References
Footnotes
Funding The research leading to these results has received funding from the European Union Seventh Framework Programme (FP7/2007-2013) under grant agreement no Health-F2-2009-241762, for the project FLIP; the Medical Research Council; the UK National Institute for Health Research Biomedical Research Centre on Ageing and Age-Related Diseases and Diabetes UK.
Competing interests None.
Ethics approval This study was conducted with the approval of the County Durham and Tees Valley 2 Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.