Article Text

Statistics from Altmetric.com
Luminal GI
Promising new approach to treatment of oesophageal cancer
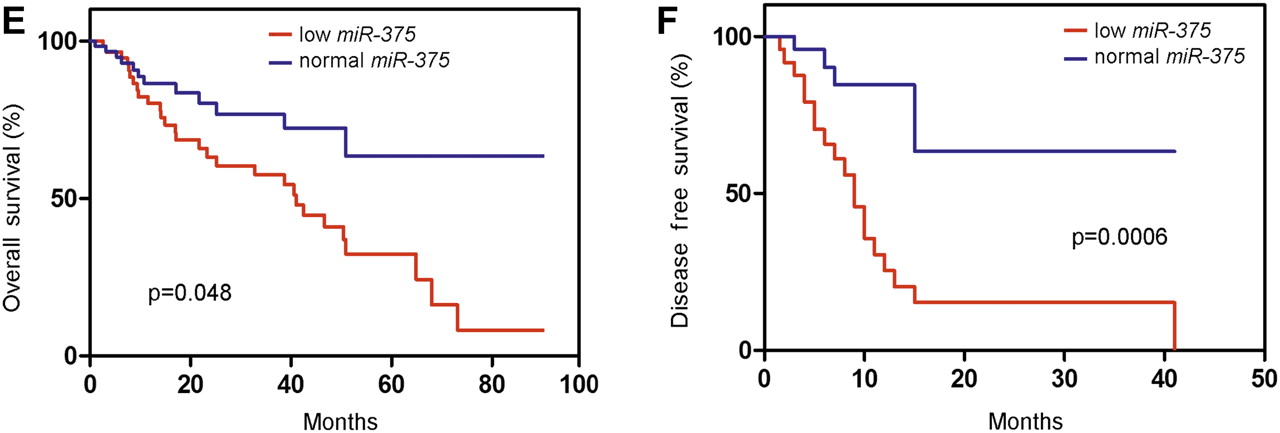
MicroRNA's are a relatively recently discovered form of small RNA's that suppress the expression of target genes. There are over 700 identified microRNAs in humans and each microRNA regulates the expression of multiple target genes. They are often over or under expressed in cancer and they appear to play an important role in the behaviour of many cancers. One of these microRNA's, miR-375, has been shown to be involved in glucose regulation and β-cell growth and is down-regulated in gastric and liver cancer. Kong and colleagues now show that miR-375 is also strongly down-regulated in oesophageal squamous cell carcinoma secondary to DNA methylation and that the decreased expression associates with advanced stage, distant metastasis, and poor overall and disease-free survival of these patients (figure 1). It appears that miR-375 directly targets the insulin growth factor 1 receptor (IGF1R), which activates the AKT signalling pathway. Thus, loss of miR-375 may be a new biomarker for oesophageal squamous cell cancers that will respond to drugs targeting the AKT pathway (see page 33).

(E) Down-regulation of miR-375 is significantly associated with poorer overall survival and (F) disease-free survival.
Coeliac disease and end stage renal disease
Individuals with coeliac disease (CD) suffer increased risk of diabetes mellitus type 1, cancers and possibly renal disease. However, the risk of end stage renal disease (ESRD) in biopsy-verified CD is unknown. In this issue of Gut, Welander et al conducted a population-based prospective cohort study of 29 050 individuals with CD (Marsh III) who were identified through small-intestinal biopsy reports obtained between July 1969 and February 2008 in Sweden's 28 pathology departments. Using Cox regression, they estimated the risk of ESRD in individuals with CD compared with age- and sex-matched reference individuals. Individuals with biopsy-verified CD suffer a threefold increased risk of future end-stage renal disease (see table 2). Increased risk of end-stage renal disease was seen irrespective of age at CD diagnosis. This solid data indicates that clinical guidelines and practice should register a greater awareness regarding renal function in CD patients (see page 64).
| Follow-up | Observed events | Expected events | HR (95% CI) | p Value |
| All | 90 | 31 | 2.87 (2.22 to 3.71) | <0.001 |
| Year <1 | 12 | 3 | 4.73 (2.27 to 9.84) | <0.001 |
| 1–4.99 | 24 | 10 | 2.41 (1.49 to 3.88) | <0.001 |
| 5+ | 54 | 19 | 2.86 (2.04 to 4.01) | <0.001 |
Risk of ESRD in CD according to follow-up
Community acquired intestinal infectious disease
Infectious intestinal disease (IID) is a common cause of illness in the community and results in a high burden of consultations to general practice (GP). Most cases of IID are not reported to national surveillance systems, making it difficult to determine the true burden in the population. Recent interventions and changes in healthcare delivery may have resulted in changes in disease burden in the community and presenting to primary care. As such, population-based studies are needed to monitor such changes. In this issue of Gut, Tam et al estimated, overall and by organism, the incidence of IID in the community, presenting to general practice (GP) and reported to national surveillance in the UK. They targeted 88 GPs across the UK recruited from the Medical Research Council General Practice Research Framework and the Primary Care Research Networks. Every year, there were up to 17 million cases and 1 million GP consultations due to IID. Although IID incidence in the community appears to have increased since the 1990s, consultations to GP have halved. Norovirus was the most common recognised cause of IID, accounting for 3 million cases and 130 000 GP consultations annually, while Campylobacter was the most common bacterial pathogen. Clostridium difficile, an important pathogen in healthcare settings, was a rare cause of diarrhoea in the community. These data are a valuable resource for healthcare planning and suggest that control efforts must focus particularly on reducing the burden due to Campylobacter and enteric viruses (see page 69).
Are we doing a good job with colorectal cancer screening?
Colorectal cancer can clearly be prevented by screening at-risk individuals. The faecal occult blood test (FOBT) was the first screening test shown to reduce mortality from colorectal cancer. Screening programs using FOBT have since been implemented in the UK, and pilot studies have shown these programs are feasible and accepted by a large portion of the general population. However, not all individuals undergo screening and factors such as age, gender, ethnic background and deprivation status strongly affect participation in FOBT screening. Moss et al have now compared performance measures across all three rounds of the English bowel cancer screening FOBT pilot study and their relation to social deprivation and ethnicity. Importantly, they show that FOBT screening in UK populations follows patterns seen in other screening programs. They also found that the effect of deprivation and ethnicity on uptake persisted over the course of all three rounds in the pilot studies. Interestingly, gender differences in uptake were quite substantial at the beginning of the studies but became less apparent over time. These results suggest substantial efforts will be required to ensure that colon cancer screening in ethnic populations and socially deprived populations are effective (see page 101).
Hepatology
MRI challenges the pathologist for quantification of hepatic steatosis
A fatty liver is more susceptible to injury upon resection or transplantation. Therefore, major hepatic steatosis is considered a risk factor for complications following liver surgery. Traditionally histopathology has been used to quantify fat content of the liver. This interesting study from Switzerland developed an MRI technique for quantification of liver fat that is superior to conventional histopathological analysis (figure 2). Liver fat determined by MRI was correlated with liver injury and survival in a mouse model. Moreover, patients with higher proportion of liver fat showed more serious postoperative complications. Obviously, pathologists are still needed to provide information regarding inflammation or fibrosis of the liver. Still these interesting findings deserve further evaluation in prospective clinical studies (see page 117).
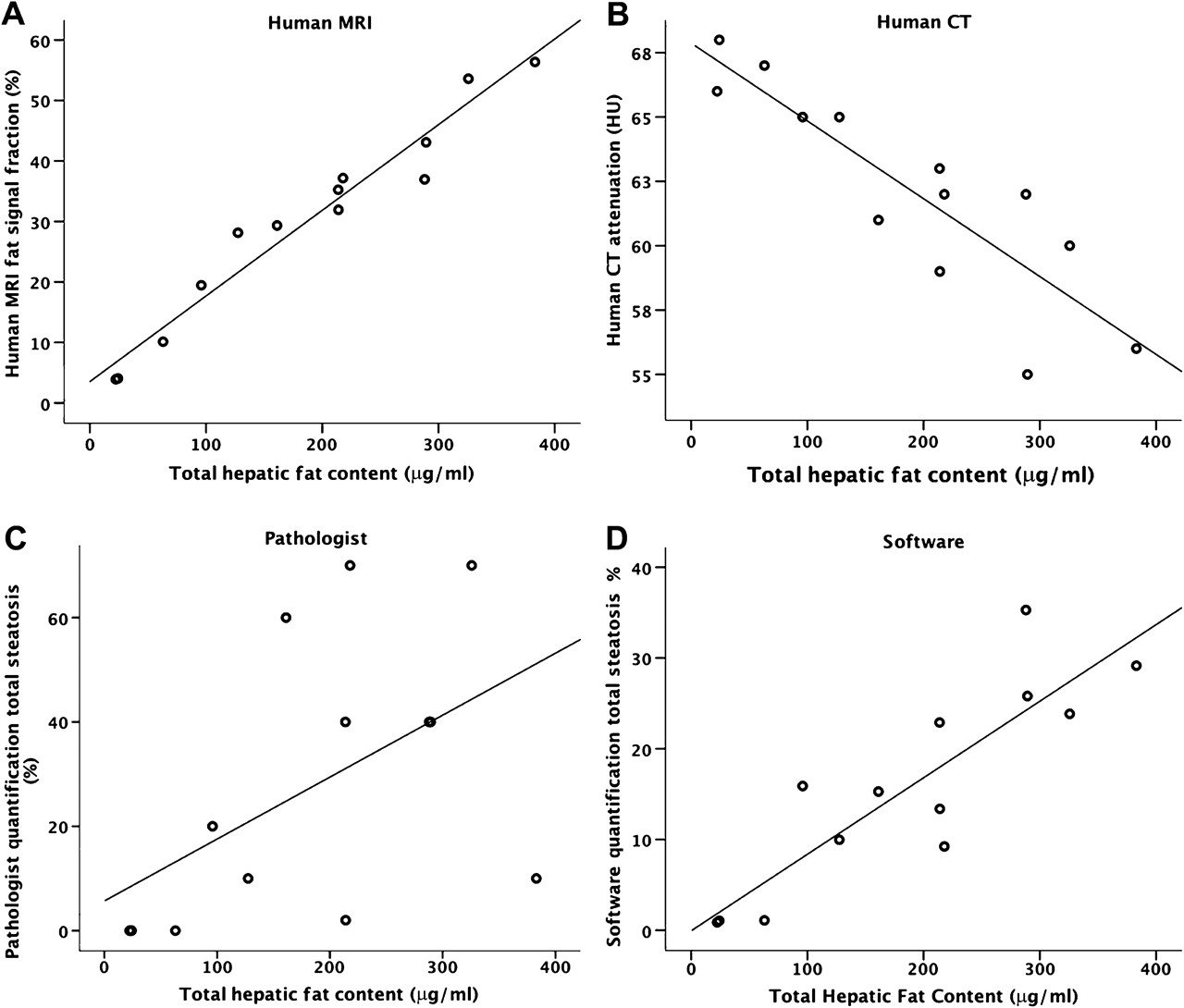
Scatter plot obtained from the mouse fat quantification by the human MRI (A), human CT (B), the pathologist assessment (C) and software (D). Fat contents determined by the accurate chemical assay were correlated with the steatosis quantification techniques.
Vaptans for ascites: an obituary?
Diuretic treatment of ascites in patients with liver cirrhosis is often not effective or is accompanied by complications such as hyponatraemia and hypo- or hyperkalaemia. Recently, vaptans, a new class of drugs, have been introduced which increase free water excretion by antagonising renal vasopressin V2 receptors. Vaptans have been approved for the treatment of hypervolaemic hyponatraemia. In cirrhosis vaptans have been shown to correct hyponatraemia and to reduce ascites in phase II trials. Therefore three long-term randomised controlled trials comparing satavaptan to placebo with a total of more than 1200 pts with ascites were conducted. This important paper by a distinguished group of international authors reports the results of these three trials. Satavaptan increases serum sodium concentration in patients with cirrhosis, provides only minor benefit for the management of ascites and may increase the risk of mortality in patients treated with diuretics following large volume paracentesis (figure 3). This paper is an excellent example for the importance of reporting negative data and should be helpful in designing long-term studies of vaptans for the treatment of hyponatraemia (see page 108).

{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier analysis of all-cause mortality up to 52 weeks in study 2: satavaptan versus placebo in combination with diuretics in the prevention of recurrent ascites after large-volume paracentesis.
Linked Articles
- Colon
- Oesophagus
- Hepatology
- Intestinal infections
- Coeliac disease
- Hepatology