Article Text

Statistics from Altmetric.com
Luminal GI
Serum ghrelin and risk of oesophageal squamous cell carcinoma
The hormone ghrelin is produced in the stomach and has a variety of metabolic functions including stimulation of gastric acid, regulation of energy balance and control of appetite. Like pepsinogen, ghrelin may be a marker of gastric fundic atrophy. Recent reports have indicated low serum ghrelin is associated with an increased risk of gastric cancer and oesophageal adenocarcinoma but its relationship to oesophageal squamous cell carcinoma remains unknown. In this issue of Gut, Murphy and colleagues from the NCI, NIH, conducted a nested case/control study within the Alpha-Tocopherol, Beta-Carotene Cancer Prevention study. They show a nearly sevenfold increase in the risk of developing oesophageal squamous cell carcinoma among subjects in the lowest quartile of baseline serum ghrelin, compared with those subjects in the highest quartile of serum ghrelin. This association appeared independent of Helicobacter pylori seropositivity or serum pepsinogen concentrations, and it remained in cases diagnosed up to 10 years after baseline ghrelin measurement. These findings suggest that ghrelin may be useful as a biomarker for upper gastrointestinal cancers and may also have an aetiologic role in the development of these cancers but further work is clearly required to confirm these conclusions.
Would you prefer to have a standard colonoscopy or virtual colonoscopy?
CT-colonography is often billed as being less burdensome for primary colorectal cancer (CRC) screening than colonoscopy. Dekker and colleagues carried out a randomised trial (N=8844) comparing the perceived burden of standard colonoscopy to non-cathartic prep CT colonography They found that the full screening procedure was reported as more burdensome in CT colonography than in colonoscopy, and that the bowel preparation received a higher burden score in colonoscopy while related bowel movements were scored more burdensome in CT-colonography. So, in a CRC screening programme, colonoscopy invitees expected the screening procedure and bowel preparation to be more burdensome than CT-colonography invitees. However, in participants, CT-colonography was scored as more burdensome than colonoscopy (figure 1). Despite these differences, the reported intended participation in a next screening round was comparable between standard colonoscopy and CT colonography.⇓

Perceived burden of colonoscopy and CT-colonography. On top of the bars, mean scores, SDs (between parantheses), differences in mean scores and pooled SDs (pSD) are displayed. All items differed significantly between colonoscopy and CT-colonography (p<0.001), except for experienced pain caused by the bowel movements (related to the preparation).
A better way to predict survival in patients with stage II CRC
Several clinical factors have prognostic impact in stage II CRC, but most are suboptimal in their ability to identify a high-risk group of stage II CRC patients who would benefit from adjuvant chemotherapy. Consequently, Agesen have now carried out a study to identify a scoring system using differentially expressed genes to determine a molecular scoring system that more accurately predicts the survival of patients with stage II CRC patients. They have found an optimal gene expression classifier for prediction of relapse among stage II CRC patients. This molecular classifer was developed using a consecutive Norwegian test series from patients treated according to current standard protocols, and its predictive value was successfully validated (figure 2). This classifier has potential to improve our ability to deliver aggressive care to CRC patients most likely to benefit from it.⇓

Kaplan-Meier survival curves illustrating relapse-free survival among stage II CRC patients. (A) In the test series, the two risk-of-relapse groups are well separated, as expected (p<0.001). (B) and (C) In both validation series I and II (B and C, respectively), the prognostic gene expression classifier identifies a low and high risk of relapse groups with statistically significance.
Hepatology
Paradoxical T-cell reaction in responders to HCV genotype-3a therapy
HCV genotype-3a is the most common strain in the UK and in south Asia. Response to therapy is often complete, the reasons for this are not known as yet but may be due to specific T-cell immunity. This interesting study from Oxford (page 1589) provides important new insights into the HCV-specific T-cell response in genotype-3a infection. The authors found that in genotype-3a CD8+ T-cell response predominantly targeted non-structural proteins while in genotype one CD4+ responses commonly targeted HCV core. Paradoxically, sustained viral response to treatment was associated with a marked decline in virus specific and total lymphocyte counts which recovered after treatment (figure 3A,B). These unexpected findings may have important clinical implications: a T-cell decline associated with viral decline during treatment could become an early biomarker of response. Moreover, the findings could aid rational vaccine design.⇓
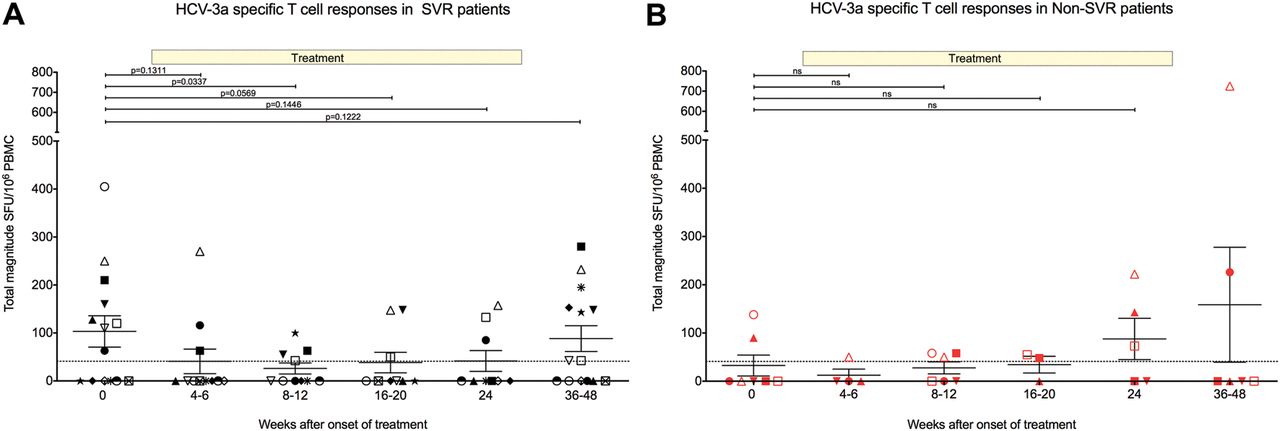
Effect of combination therapy on hepatitis C virus (HCV)-specific T cell responses in genotype-3a patients with sustained virological response (SVR) (A) and non-SVR (B). Total magnitude of genotype-3a HCV-specific T cell response measured by IFN-g ELISpot assay in chronic genotype-3a patients. T cell responses to HCV genotype-3a peptides were measured before treatment, and at multiple timepoints during treatment and post-treatment. Patients achieving SVR are shown on left panel (black symbols) and patients failing to achieve an SVR are shown on right panel (red symbols).
Novel markers for progression of liver fibrosis
MicroRNAs (miRNAs) 221 and 222 are oncogenic and increase markedly in human hepatocellular carcinoma. This comprehensive study from Japan (page 1600) explored miRNAs regulated with the progression of hepatic fibrosis. They identified miRNAs in human livers with HCV and NASH, respectively and validated their findings in two mouse models and in cultured hepatic stellate cells. Among several relevant miRNAs miR-221 and -222 were upregulated in human liver in a fibrosis- but not a steatosis-dependent manner and in parallel to the expression of α1 collagen and of α-smooth muscle actin (figure 4). This was confirmed in mouse models of liver fibrosis and in cultured mouse stellate cells. Thus, miR-221 and -222 could be novel markers of stellate cell activation and of liver fibrosis progression and may be useful as therapeutic targets.⇓

{kind=link}
{kind=link}
{kind=link}
{kind=link}
C