Article Text

Abstract
Introduction Reports of patients returning to drinking after orthotopic liver transplantation (OLT) for alcoholic liver disease (ALD) remain a source of unease for professionals and the public. Recidivism rates of 10%–16% are reported with a low rate of alcohol-related graft loss.1 2 In 2005, the UK Transplant liver advisory group recommended an “alcohol contract” in which ALD patients listed for OLT confirmed in writing their commitment to abstinence.3 The purpose of our study was to measure the rates and consequences of post-OLT alcohol intake in a UK transplant program and assess the effect of the “alcohol contract” on rates of post-transplant drinking.
Methods Prospectively collected data were reviewed for 100 randomly selected patients transplanted for ALD—32 patients transplanted since the “alcohol contract” was implemented (February 2007) and 68 patients transplanted before.
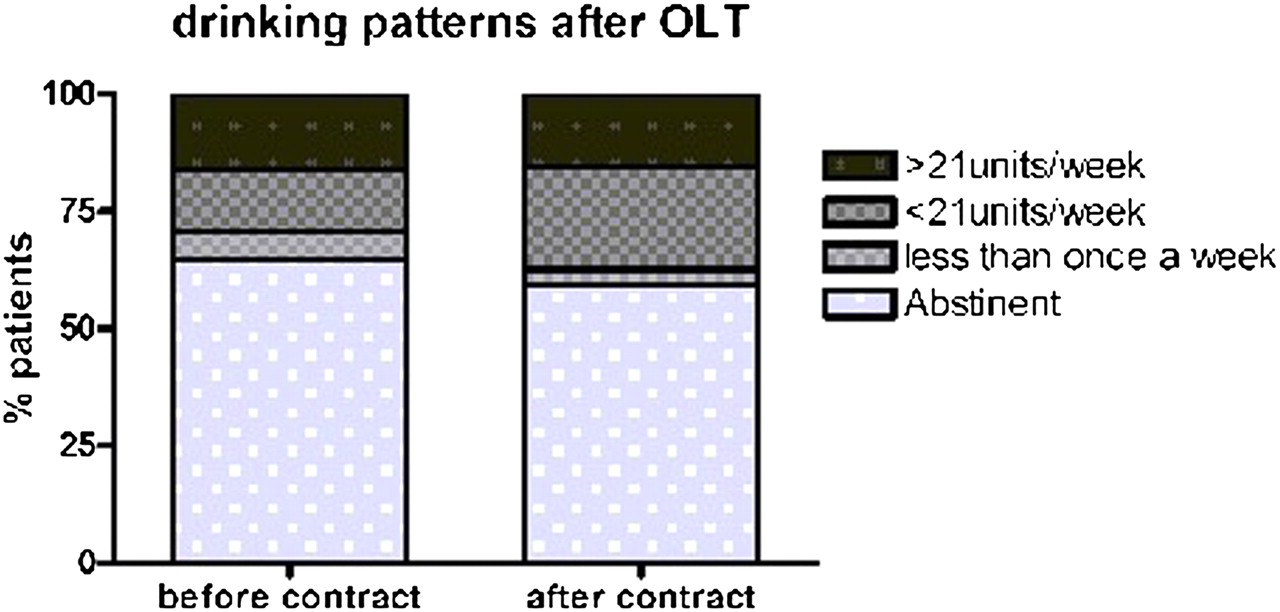
Results Overall (n=100; 62 male, median age 54), 37 patients reported some alcohol intake post-OLT. The proportion of patients returning to any alcohol was 35.3% before the “alcohol contract” and 40.6% after (NS; p=0.66). For heavy drinking (>21 units [168 g ethanol]/week) this was 16.2% and 15.6%, respectively (NS; p=1.0). Four patients underwent OLT despite pre-transplant liver histology consistent with active ALD. After OLT, one of these returned to heavy drinking and another denied drinking but had a positive blood alcohol. At explant, 10 patients had features of active ALD: six of these returned to drinking post-OLT. Blood alcohol was measured in only 24 of 63 patients reporting abstinence. Two had positive tests; one of these subsequently disclosed heavy drinking. During follow-up, 23 patients died. Most deaths (87%) occurred in those (63%) who did not return to drinking. Only one death in 673 patient-years of follow-up could be directly attributed to alcohol intake.
Conclusion Post-OLT recidivism is higher in our cohort than other published series but the impact of drinking on post-transplant survival remained low. The introduction of an “alcohol contract” may have value in improving public perception of transplantation in ALD patients but is insufficient to alter rates of recidivism. Random blood alcohol testing is inadequate to detect post-transplant drinking. More robust abstinence support and better assessment measures might improve outcomes.
{kind=link}
Competing interests None declared.
References 1. Tomé, et al. J Hepatol 2002;36:793–8.
2. Wells, et al. Liver Transplantation 2007;13:1728–35.
3. Bathgate, et al. Lancet 2006;367:2045–6.