Article Text

Abstract
Several aspects of the management of Crohn's disease (CD) are shared between patients. The goal of all therapies should be to achieve clinical and endoscopic remission in a timely manner to avoid disease progression and abdominal resections. The way this goal is achieved may differ and predicting how the disease will evolve, what the most appropriate therapy with the highest chance of success will be, how long a therapy needs to be continued, and what the intensity of follow-up should be are more difficult questions and require an individualised approach. Clinical parameters have been suggested to aid in the therapeutic decision process but lack specificity. Although much promise has been put in molecular markers, these have not yet found their way to the clinic. More recently, clinicians have started to gain interest in drug level monitoring to adapt doses of immunomodulators and/or anti-tumour necrosis factor antibodies in an individualised manner. An increasing number of studies show that therapeutic drug monitoring can help physicians to improve and personalise the management of their patients. What is needed now are pharmaco-economic studies showing that personalised management of CD is cost effective.
- IBD
- IBD CLINICAL
Statistics from Altmetric.com
Introduction: why should not all patients with Crohn's disease receive the same therapy?
Personalised use of therapeutic options has many facets: it may imply an individualised selection of medication, also the decision on a more or less intense follow-up for a given patient, and more recently, individual adaptation of therapeutic dosing by serum drug monitoring was added to the personalised management of Crohn's disease (CD).
The main reason for not applying one and the same management for CD is the complexity of phenotypes: the extent, localisation and disease severity may vary substantially from patient to patient, and may change over time in a given patient. This means that the available drugs will only have their optimal effect when used in the right indication and patient population.
Nevertheless there are some common recommendations when it comes to managing patients with CD. First, it is important to get a complete map of the disease before any therapy is started. Magnetic resonance (MR) enterography and ileocolonoscopy have become the gold standard for assessing small and large bowel and MR imaging (MRI) of the pelvis is the method of choice for the assessment of perianal CD. Second, the goal of all treatments should be remission and mucosal healing without steroids, and third, this goal should be achieved in a timely manner. Recent clinical trials in CD have clearly illustrated that treatment with anti-tumour necrosis factor (TNF) agents in combination with azathioprine early in the disease course results in higher steroid-free remission rates and higher mucosal healing rates.1 Nevertheless, intolerance, contraindications, lack of response, interest and timing of pregnancy, and concerns around infection and/or malignancy risks means that the choice of treatment is not always as easy as it seems.
Individualised choice of treatment: prognostic factors
Once a diagnosis of CD is made, the best therapeutic strategy needs to be chosen to reach the aforementioned goals. This can go from no treatment in rare cases, to one induction course of steroids in patients with very mild disease, to maintenance medical treatment in most patients, and even primary surgery in patients with very limited stenotic disease and/or complications.2
Medical maintenance treatment can imply an accelerated step-up approach or a more proactive top-down strategy. A number of prognostic factors have been proposed to aid in this decision process. Clinical factors that have been associated with more aggressive CD include young age at diagnosis, the presence of deep (colonic) ulcers, extensive small bowel involvement, significant weight loss and perianal disease3––8 (table 1). In two independent studies using population-based cohorts from New Zealand and Olmsted County, perianal involvement at diagnosis was confirmed as predictive of complicated disease behaviour and of more rapid progression of CD.7 ,8 In the original study by Beaugerie et al,3 the necessity to start steroids at diagnosis was also indicative of a disabling disease course in the subsequent 5 years, but this decision highly depends on the physician and on regional habits. In contrast, an older age at diagnosis and absence of rectal (and perianal) involvement would indicate more mild disease6 (table 1).
Reported clinical parameters with prognostic value
Although several of these factors have been confirmed in retrospective studies, patients often have a combination of mild and aggressive prognostic factors, which complicates the therapeutic decision. Also, most of the parameters published about disabling disease included patients attending specialty inflammatory bowel disease centres who may not be representative of a typical patient, and therefore all patients with disabling features may not require combination therapy.
Molecular prognostic markers: hope or reality?
Molecular (genetic, serological, immunological and/or tissue) markers have been the subject of study but have not yet found a place in aiding the therapeutic decision process, in contrast to other fields such as oncology, in which molecular markers have demonstrated clinical utility in predicting response to chemotherapy. So is the response to cetuximab, a monoclonal antibody to epidermal growth factor receptor in metastatic colorectal cancer, influenced by the KRAS mutation status, as the benefit of cetuximab seems limited to patients with KRAS wild-type tumour?9 Likewise, germline mutations may also correlate with clinical outcome to chemotherapy. A subanalysis of a large phase III study with bevacizumab (Avastin), a humanised monoclonal antibody to vascular endothelial growth factor (VEGF), in metastatic pancreatic cancer showed that overall survival and progression-free survival were influenced by single nucleotide polymorphisms (SNPs) in the tyrosine kinase domain of the VEGF receptor 1.10 Genome-wide association study (GWAS) technology has been successfully applied to identify genetic risk variants for flucloxacillin-induced hepatotoxicity. With only 51 cases of flucloxacillin-induced liver injury and 282 controls, a clear association was seen for the major histocompatibility complex region at rs2395029, a marker in linkage disequilibrium with HLA-B*5701.11 Likewise, a GWAS in 85 subjects with statin-induced myopathy and 90 controls identified common variants in SLCO1B1 that were strongly associated with an increased risk of statin-induced myopathy.12
In CD, NOD2/CARD15 remains not only the gene with the largest effect size but also with the most convincingly replicated association with disease phenotypes. Mutations have been associated with terminal ileitis, with a shorter time to onset of structuring disease and the need for surgery.13–15 Specifically, Seiderer et al16 demonstrated a strong risk increase for 1007 fs homozygotes for ileal stenoses and risk for surgery. The same group confirmed these findings in a prospective study.17 In a large Dutch cohort, Weersma et al18 described a higher OR for more severe CD, a greater need for surgery and a younger age at onset with increasing number of risk variants.
Why have genetic studies in CD not been more successful in translating the identified mutations to clinical applications? The SNPs tested are mostly known susceptibility markers for IBD compared with healthy controls, and might thus be more generally applicable to all patients with IBD and less useful to differentiate patients. It is also hypothesized that CD genetics consists of disease susceptibility genes/loci on the one hand, and disease-modifying genes/loci on the other. Work from the international IBD genetics consortium underscores this idea: reanalysis of GWAS data in function of disease behaviour (mild versus aggressive disease) identified a number of SNPs that specifically predisposed a person to a more aggressive disease course in CD. However, the same SNPs were not associated with the disease overall in the original GWAS.19
For serology, higher antimicrobial (OmpC, anti-flagellin cBir1, anti Pseudomonas i2) and/or antifungal (anti saccharomyces cerevisiae antibodies (ASCA), anti laminaribioside antibodies (ALCA), anti mannobioside antibodies (AMCA), anti chitobioside antibodies (ACCA)) antibody titres have been found in patients with fistulising and/or stenosing CD.20–22 Also these markers have not been widely implemented in clinical practice given their limited availability, the fact that they are expensive and above all the lack of prospective studies showing the stability of these markers. The observed increased antibody responses in patients with CD with longer disease duration highlight the importance of prospective longitudinal studies.22 One relatively small paediatric longitudinal study reported a relation between the presence and titre of antibodies (ASCA, anti-OmpC, anti-I2, anti-CBir1) at a time when no fistula or strictures were clinically apparent, and the subsequent development of complicated disease behaviour during a median follow-up of 18 months.23 Similar conclusions were drawn by Rieder et al24 in an adult population.24
In oncology, gene expression profiling has been successfully used to identify transcriptional signatures that predict several aspects of disease behaviour, including risk of metastasis and response to chemotherapy.25 ,26 These gene expression-based biomarkers have also been translated into clinical practice. In autoimmune and inflammatory conditions, such techniques have generally not detected signatures with equivalent prognostic utility. We studied colonic mucosal gene expression to provide a predictive response signature for infliximab (IFX) treatment in ulcerative colitis. A combination of five differentially expressed genes (osteoprotegerin, stanniocalcin 1, prostaglandin-endoperoxide synthase 2, interleukin (IL)-13 receptor α2 and IL-11) separated responders from non-responders with 95% sensitivity and 85% specificity.27
Researchers from the University of Cambridge reported a transcriptional signature in separated CD8 T cells which predicted prognosis in patients with CD.28 Interestingly, the same signature was previously also found to predict disease prognosis in systemic lupus erythematosus and in patients with antineutrophil cytoplasmic antibody associated vasculitis.29 There was a higher incidence of relapsing disease in the subgroup of patients who had an elevated expression of genes involved in antigen-dependent T-cell responses, including signalling initiated by IL-7 and T-cell receptor ligation. The fact that this signature could be found across several autoimmune and immune-mediated diseases suggests that, although being distinct autoimmune and inflammatory conditions, the course of these diseases may be influenced by common pathways. These subgroups, which can be identified by measuring expression of only three genes, raise the prospect of individualised therapy and suggest new potential therapeutic targets in autoimmunity. A prospective study to confirm these findings is ongoing.
Optimising treatment: role of measuring drug levels and metabolites
6-TGN and 6-MMP metabolite testing
Once the therapeutic decision has been made, therapy adjustment is often needed to improve or restore efficacy and has shown to be efficacious. 6-Thioguanine nucleotide (6-TGN) levels, the active metabolites of azathioprine/6-mercaptopurine, correlate with response to azathioprine/6-mercaptopurine, although the sensitivity and specificity towards predicting response is suboptimal (around 70%). The metabolism of azathioprine/6-mercaptopurine also takes place via the enzyme thiopurine methyl transferase with formation of 6-methylmercaptopurine (6-MMP) metabolite levels.30 High 6-MMP levels have been associated with a higher risk of hepatotoxicity.31 The combination of 6-TGN (efficacy) and 6-MMP (hepatotoxicity) levels may help the clinician in the individual dose adaptation of azathioprine/6-mercaptopurine (table 2). This may in particular apply to patients with insufficient or no healing despite 16 weeks or more of azathioprine/6-mercaptopurine treatment.
Value of 6-TGN and 6-MMP levels in optimising the dose of azathioprine/6-mercaptopurine
A recent study from London, UK showed that in patients not responding to azathioprine, measuring metabolites lead to a change in treatment in 73% of patients.32 In their adult cohort, the authors found that only 6% of patients were non-adherent with very low to absent levels, 25% were under dosed and 29% were over dosed by 6-TGN. Also, 12% of patients predominantly methylated thiopurines and were at high risk of hepatotoxicity. Optimisation of therapy based on TGN resulted in improvement in 90% of patients. Another interesting finding of this study was that, in responders, TGN-guided dose reduction was possible without precipitating relapse. This is an example of how therapy could be really individualised and how possibly side effects can be minimised, or even better, avoided. So has allopurinol been suggested in patients who preferentially metabolise azathioprine/6-mercaptopurine to 6-MMP to deliberately shunt metabolism towards 6-TGN and improve clinical responses?33 This should of course be done with caution and with follow-up of the 6-MMP and 6-TGN levels. Finally, the question also comes to mind, when considering studies on metabolite testing, would previous randomised studies with azathioprine/6-mercaptopurine have yielded better results with knowledge (and adaptation) of the metabolite levels?
Anti-TNF serum levels and antibodies
Anti-TNF antibodies play a pivotal role in maintaining remission and in inducing complete mucosal healing, and also in the management of perianal fistulas they have shown unprecedented results. Nevertheless, more than half of the patients will have a reduced efficacy over time due to formation of neutralising antibodies in most cases.34 ,35 These antidrug antibodies (ADAs) lead to a decrease of the active drug concentration and to the formation of drug–antibody complexes, which will be taken up by liver and spleen enhancing drug clearance. Loss of response is usually managed clinically by decreasing the interval between infusions or injections, by increasing the dose, by adding immunosuppressives (methotrexate, azathioprine) or by switching within the same class to more humanised or human antibodies.36 However, these therapeutic interventions are often done in vain, only leading to higher costs and a potential increasing risk for side effects. Despite interventions, still a significant proportion of patients drop out per year.35 An optimal use of anti-TNF agents implies the correct dosage, which also means that peak levels and average levels should not exceed concentrations which are associated with increased toxicity.
A number of retrospective studies have demonstrated that sustained good anti-TNF trough levels (TLs) are associated with better mucosal healing rates and a better long-term outcome and will lead to a better quality of life, fewer disease-related surgeries and fewer hospitalisations.37–40 Theoretically, levels may also be supratherapeutic and lowering the dose in those patients could reduce costs for the healthcare payer. However, this should be shown by prospective comparative randomised trials. One small study in 32 patients with spondylarthropathy in which IFX dosing was adjusted based on TL and ADA measurements showed an inverse relationship between IFX TL and the Bath ankylosing spondylitis disease activity index (BASDAI): patients with a higher BASDAI (reflecting more active disease) had lower TL and vice versa.41 In August 2011 we initiated a 1-year randomised prospective TL monitoring study with real-time therapeutic adaptations (Trough Level Adapted Infliximab Treatment (TAXIT)). A total of 275 patients with CD or ulcerative colitis on IFX maintenance therapy were included and randomised to an active arm, in which IFX infusions were adjusted according to a developed algorithm with the aim of keeping all patients in a therapeutic TL window, or a control arm, in which the interval between infusion was adjusted based on clinical grounds (symptoms, C-reactive protein).42 The adjustments in the active arm included increases and decreases of the dose and frequency of the infusions. The primary aim was to assess the impact of personalised therapeutic drug monitoring and dose optimisation on clinical and biological remission rates after 12 months. Secondary aims included safety, efficacy and tolerability issues. Other prospective studies (eg, Tailorix, an investigator-initiated multicentre study from Holland, Belgium and France) will study whether dosing based on serum levels may improve outcome while not increasing the costs.
When to measure metabolites and drug levels?
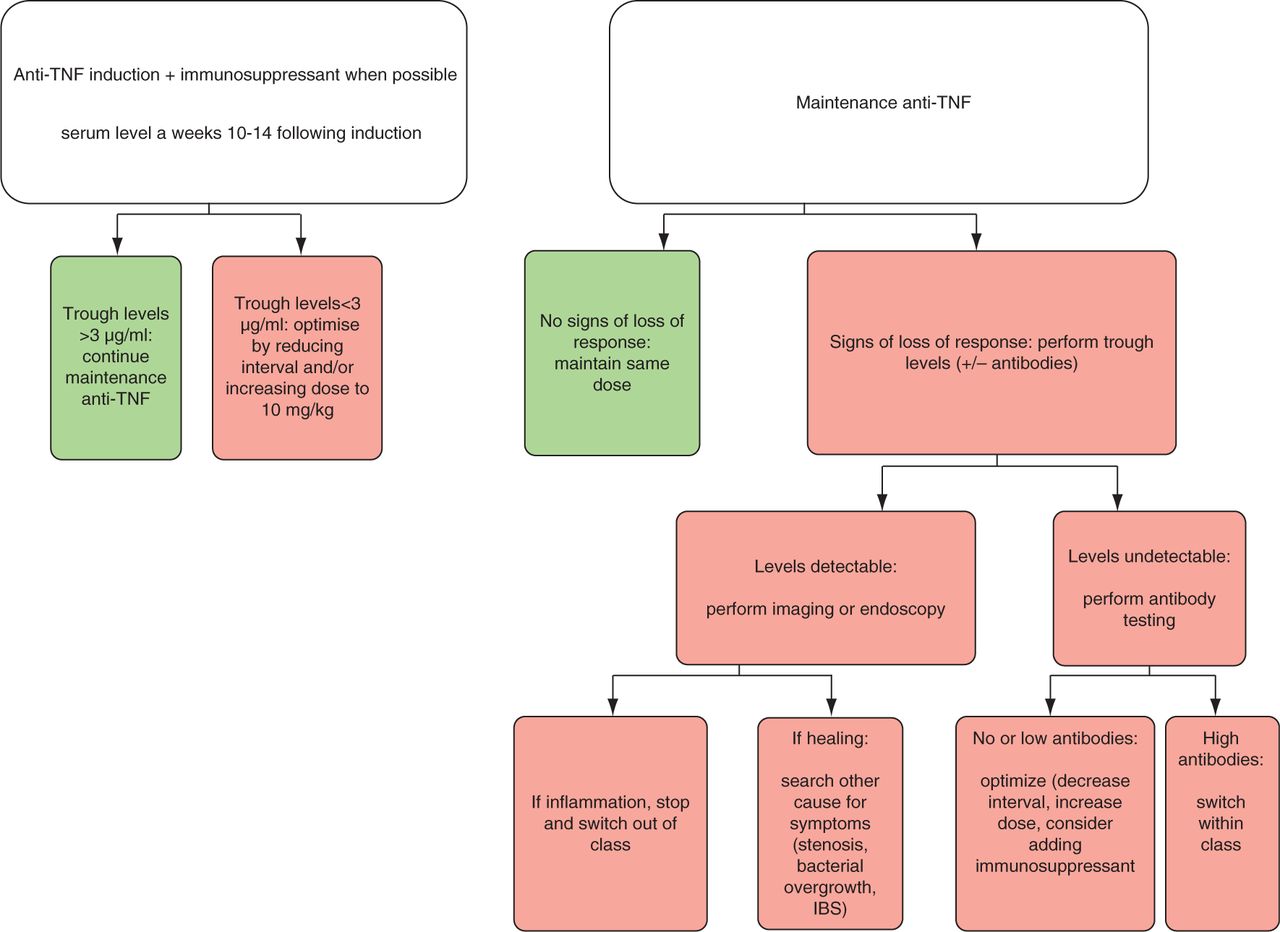
In the absence of studies showing that drug-level monitoring and adaptation based on the levels leads to improved outcomes and/or reduced costs, routine measurements of TLs and ADAs cannot be recommended yet (figure 1). A post hoc analysis of ACCENT1 suggests that measuring TLs early after induction has a prognostic value.43 The authors re-analysed the sustained response rates in function of week 14 serum IFX TLs and showed that the median week 14 IFX TL was 4.0 μg/ml in the sustained responders compared with only 1.9 μg/ml in patients without sustained response (p=0.0331). A week 14 IFX TL of 3.5 μg/ml discriminated best the sustained response with sensitivity, specificity, positive and negative predictive values of 54%, 72%, 39% and 82%, respectively. We previously also showed that in patients who develop significant antibodies to infliximab (ATIs) during follow-up, the IFX levels 4 weeks after the first infusion were significantly lower than in patients who did not develop ATIs on follow-up.44 Therefore, it may be proposed that obtaining a TL early after induction and optimising early on if needed can avoid development of antibodies with subsequent loss of response.

{kind=link}
Proposed algorithm of when to perform anti-tumour necrosis factor (TNF) drug monitoring. IBS, irritable bowel syndrome.
Definitively, when patients treated with anti-TNF are reporting symptoms and signs of inflammation suggestive of loss of response, determining TLs, and when no TLs are detected measuring ADAs, is helpful. TLs should always be measured just before the next dose (just prior to starting the next infusion). As proposed in figure 1, patients with undetectable TLs and low ADAs should be optimised with the same drug. There does not seem to be a preferred way of dose optimisation and decreasing the interval between infusions, increasing the dose, or adding an immunosuppressive drug have all been associated with increasing levels and recapturing response.45 A recent study reported that, in patients with detectable antibodies to IFX, adding an immunosuppressant decreased the antibodies and restored IFX TLs and clinical response.46 Patients with undetectable TLs and high ADAs, however, should be switched to a drug within the same class. In the case of symptoms with adequate TLs, endoscopy or MR enterography should be checked, and if this confirms significant lesions, therapy should be stopped and a switch to a drug with a different mode of action, if at all possible, is the preferred option. However, a wide implementation of TL and ADA determinations in clinical practice requires a rapid assay that can be performed at home by the patient or at the clinic or infusion centre. Meanwhile, the available assays need to be standardised and validated. There is also a need to improve current assays within economic margins.47
Conclusion
As for many other chronic inflammatory diseases, the advances of pathogenesis and therapeutic options have been substantial for CD. The approach to the individual patient has changed to meet better endpoints such as healing and sustained remission. Therapy for CD has become a tailored therapy and anti-TNF drug-level monitoring is the most recent example of this individualised management. The hope is that this approach translates itself in the coming years to a more cost-effective care with fewer side effects and a better cure rate.
Key messages
-
The treatment goal in Crohn's disease (CD) does not need to be personalised and should be striving for remission with healing of large ulcers.
-
The approach to achieve this goal is not the same in all patients. Clinical parameters such as perianal disease, deep ulcers and an extensive small bowel involvement dictate more aggressive management with early anti-tumour necrosis factor (TNF) antibodies.
-
Monitoring of 6-thioguanine nucleotides and 6-methylmercaptopurine levels in patients treated with thiopurines has shown to improve efficacy and reduce side effects.
-
Drug-level monitoring of anti-TNF antibodies has increasingly been promoted recently as anti-TNF levels correlate with remission and healing rates.
-
Pharmaco-economic studies should be performed before therapeutic drug monitoring in CD can become a generalised practice in all patients.
-
With new biological agents on the horizon, future studies should focus on identifying molecular markers and/or pathways driving disease in individual patients and treatment should be chosen accordingly.
References
Footnotes
Contributors SV drafted the article, and MF and PR revised it critically. All three authors approved the final version.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.