Article Text

Statistics from Altmetric.com
Luminal
Bringing the effects of antibiotics on the gut microbiome into focus
Although it is well known that antibiotics alter the bacteria that live in the colon and that these changes can predispose individuals to disease (eg, C difficile colitis), the specific aspects of these changes are relatively uncharacterised. The importance of a detailed understanding of how antibiotics affect the gut microbiota is obvious given the common use of antibiotics throughout the world. In order to obtain a detailed assessment of these effects, Dr Pérez-Cobas and colleagues have carried out the first comparative OMIC investigation of gut microbial communities in faecal samples taken at different times from an individual subjected to β-lactam therapy. They have found that there is an early reduction in Gram negative bacterial populations followed by re-growth of ‘resistant’ bacterial populations and then Gram-positive bacteria. They also observed major metabolic changes after one week of therapy and alterations in bacterial transport of a variety of metabolites, including bile acids, cholesterol, hormones, and vitamins. Their results demonstrate the profound effects of antibiotics not only on the bacterial populations in the colon but also on the associated metabolic processes of the microbiome. (see page 1591 )

Total and active bacterial composition based on 16S rDNA and 16S rRNA analysis, respectively, in the follow-up study. Samples FS-0, FS-3, FS-6, FS-11 and FS-14 correspond to the collections made on days 0, 3, 6, 11 and 14 during AB treatment, respectively.
Magnetic Resonance Colonography (MRC) for UC
MRI enables accurate assessment of disease activity, quantification of severity and extension of lesions in Crohn's disease but its utility in UC is not established. In this issue of Gut, Ordás et al prospectively assessed the diagnostic accuracy of magnetic resonance colonography for detecting activity and grading severity in 50 patients with UC using endoscopy as the reference standard. Endoscopic activity was evaluated globally and on a segment basis using the modified Baron score, and also classified as absent, mild to moderate or severe. MRC parameters evaluated in each segment were: wall thickness, pre- and post-contrast wall signal intensity, relative contrast enhancement, mural oedema, ulcers, enlarged lymph nodes and the comb sign. Of these variables, contrast enhancement, the presence of oedema and extramural changes such as enlarged lymph nodes and the comb sign were able to determine activity and severity of UC. A simple MRI UC index closely correlated with an endoscopic quantitative index of severity. This simplified MRC index might be used as an objective measure of therapeutic response in UC in clinical practice and research. (see page 1566)
Endoscopy
3D reconstruction of endomicroscopy for oesophageal cancer
Confocal laser microscopy, also called endomicroscopy, has been shown to visualise cellular structure with a precision close to histology in some studies. In this issue of Gut, Li et al have advanced this story a little further. They used special software to reconstruct confocal images of normal squamous epithelium and early neoplasia including intrapapillary capillary loops which, when distorted, are a hallmark of neoplasia. They successfully obtained and interpreted 3D confocal images of the human oesophageal epithelium for the first time. Image criteria were developed in normal subjects and then scores tested in a collective of patients with suspected oesophageal lesions consisting of low and high grade dysplasia. Two observers had sensitivities around 80% and specificities around 90%. This new technique may play a role in differentiating lesions found during conventional screening; further studies will define its role in comparison to other techniques of advanced imaging and 2 D confocal microscopy. ( see page 1547)
Hepatology
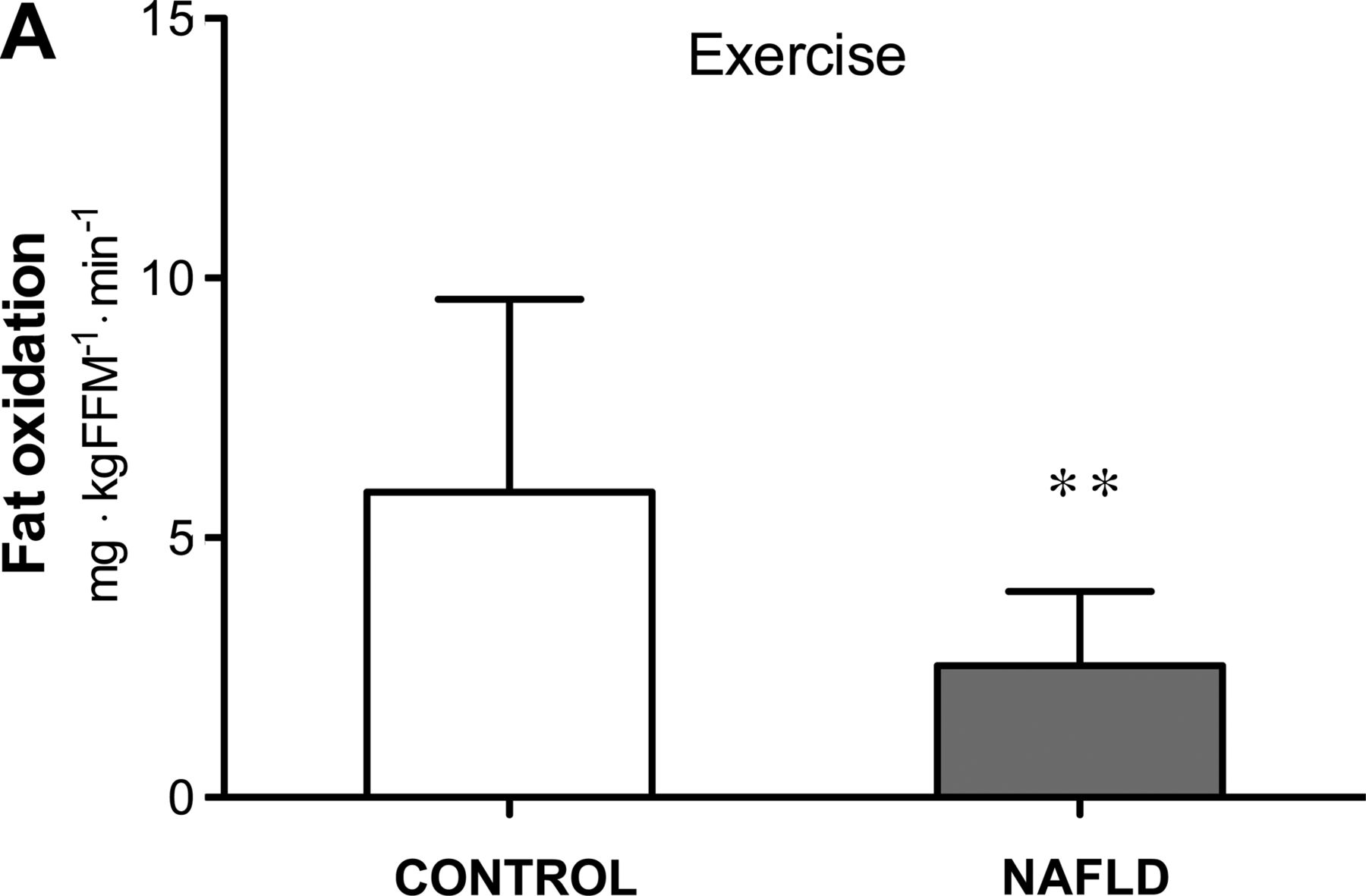
Fat oxidation plays a key role in non-alcoholic fatty liver disease (NAFLD)
NAFLD is one of the most prevalent liver diseases and is associated with several metabolic derangements. This interesting paper from Australia (see page 1625) is the largest study yet to assess disease severity by liver histology in conjunction with whole body substrate metabolism and insulin resistance in these patients. Substrate oxidation was measured in three different physiological states: basal, insulin-stimulated and exercise, an ideal setting to study whole-body energy homeostasis and to understand mechanisms of dysfunction. NAFLD patients with a broad spectrum of steatosis were studied. NAFLD patients had reduced fat oxidation under basal conditions, associated with histological severity of disease, but also during exercise (figure 2). Therefore therapeutic approaches to enhance basal and exercise fat oxidation seem the logical consequence for the management of NAFLD.

Fat oxidation during exercise is markedly reduced in NAFLD patients as compared to controls.
Which is the best beta-blocker to reduce portal hypertension?
Non-selective beta-blockers are the treatment of choice for preventing variceal bleeding in patients with cirrhosis and oesophageal varices. Unfortunately, a substantial proportion of patients do not respond with the desired decrease of portal pressure. This important study from Austria ( see page 1634) switched non-responders from propranolol, the most widely used beta-blocker for this indication, to carvedilol which provides additional alpha-adrenergic blockade. Interestingly, more than half of propranolol non-responders exhibited a significant decrease of portal pressure (figure 3). This was associated with improved clinical outcomes. Thus, carvedilol seems the beta-blocker of choice, certainly in non-responders to propranolol.
Please also read the insightful commentary by Jaime Bosch. ( see page 1529)

{kind=link}
{kind=link}
{kind=link}
Haemodynamic response to propranol and carvedilol.
Linked Articles
- Hepatology
- Inflammatory bowel disease
- Hepatology
- Endoscopy
- Gut microbiota
- Commentary