Article Text

Abstract
Background As screening methods for colorectal cancer (CRC) are limited by uptake and adherence, further options are sought. A blood test might increase both, but none has yet been tested in a screening setting.
Objective We prospectively assessed the accuracy of circulating methylated SEPT9 DNA (mSEPT9) for detecting CRC in a screening population.
Design Asymptomatic individuals ≥50 years old scheduled for screening colonoscopy at 32 US and German clinics voluntarily gave blood plasma samples before colon preparation. Using a commercially available assay, three independent blinded laboratories assayed plasma DNA of all CRC cases and a stratified random sample of other subjects in duplicate real time PCRs. The primary outcomes measures were standardised for overall sensitivity and specificity estimates.
Results 7941 men (45%) and women (55%), mean age 60 years, enrolled. Results from 53 CRC cases and from 1457 subjects without CRC yielded a standardised sensitivity of 48.2% (95% CI 32.4% to 63.6%; crude rate 50.9%); for CRC stages I–IV, values were 35.0%, 63.0%, 46.0% and 77.4%, respectively. Specificity was 91.5% (95% CI 89.7% to 93.1%; crude rate 91.4%). Sensitivity for advanced adenomas was low (11.2%).
Conclusions Our study using the blood based mSEPT9 test showed that CRC signal in blood can be detected in asymptomatic average risk individuals undergoing screening. However, the utility of the test for population screening for CRC will require improved sensitivity for detection of early cancers and advanced adenomas.
Clinical Trial Registration Number: NCT00855348
- Colorectal Cancer Screening
- Methylation
- Colonoscopy
- Colorectal Adenomas
- Colorectal Neoplasm
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
-
Screening for colorectal cancer (CRC) is commonly done by stool tests and colonoscopy, but uptake and adherence may limit benefit.
-
A blood test alternative might improve uptake and adherence to CRC screening.
-
Plasma methylated SEPT9 DNA (mSEPT9) was shown to be about 70% sensitive and 90% specific for CRC detection in retrospective case control studies.
What are the new findings?
-
This is the first prospective study in a screening population with bloods collected prior to colon preparation. The analytic method was based on analysis of plasma DNA in two PCR replicates, as recommended by the manufacturer at the time the study was performed. Sensitivity of mSEPT9 for detection of CRC was 48.2% sensitive; it was 91.5% specific.
How might it impact on clinical practice in the foreseeable future?
-
With improved performance characteristics to detect early cancer and advanced adenomas, the mSEPT9 assay could play a role in CRC screening.
Introduction
Colorectal cancer (CRC) afflicts 1 35 000 and kills 51 000 Americans every year, with similar rates in most European countries.1 ,2 A blood test that detects asymptomatic CRC could be clinically useful.
Aberrant methylation as a regulator of gene expression has been demonstrated in tumours in general3 and for CRC specifically.4 Aberrantly methylated genes are attractive candidate markers for cancer detection, as cancer specific methylation occurs early in tumorigenesis, appears to be stable, yields an amplifiable signal and can be assayed with high accuracy.5 As methylation occurs in distinct genomic areas, methylated markers in tumour tissue6 and in body fluids7 are likely targets for also detecting cancer in its early forms.
Methylated SEPT9 DNA (mSEPT9) was identified by comparing candidate markers in normal colonic epithelium and CRC tissue samples through methylation sensitive restriction enzyme based marker discovery followed by microarray and real time PCR.8 Over 90% of tumour tissue had relative quantities of mSEPT9 above the highest relative quantities found in normal colon mucosal tissue. Previous independent case control studies using clinically confirmed CRC cases and colonoscopy verified healthy asymptomatic controls suggested that detecting mSEPT9 in plasma may indicate the presence of CRC.8–10 In these studies, the overall sensitivity for CRC using DNA derived from 3–5 ml plasma and a triplicate PCR reaction averaged around 70%, with a false positive rate of approximately 10%.
We therefore prospectively assessed the performance of this marker in a screening setting in a large asymptomatic population undergoing screening colonoscopy.
Patients and methods
The PRospective Evaluation of SEPTin 9 (PRESEPT)11 was a multicentre US and German study, sponsored by Epigenomics AG, to estimate the ability of mSEPT9 to detect invasive adenocarcinoma of the colorectum in asymptomatic individuals, aged 50 years and older, meeting average risk screening guidelines.12 This ability is measured by the sensitivity; additionally, specificity and predictive values of the assay are important to clinical utility. Secondary endpoints included sensitivity for advanced (clinically significant) adenomas (AA) and for non-advanced (clinically insignificant) adenomas (NA). Statistical design, data management and analysis were performed by an independent statistical centre (Health Studies Section, Division of Environmental Health Sciences, University of Minnesota School of Public Health). Other than the statistical centre, all study personnel were fully masked to subject specific assay results. However, for identification of unforeseen workflow errors, laboratory personnel were given assay result distributions, including frequency of positives, negatives and invalids for comparison with historical values.
Ethics committees in Germany and institutional review boards in the USA approved the study, and all subjects were informed and signed a consent form. An independent Clinical Studies Steering Committee (CSSC) made scientific decisions regarding the study and oversaw operations. mSEPT9 assay results were not disclosed to subjects or their physicians and played no role in clinical care.
The PRESEPT Study, Evaluation of SEPT9 Biomarker Performance for CRC Screening, is registered at ClinicalTrials.gov, Trial Registration ID: NCT00855348.11 The protocol is accessible at https://www.healthstudies.umn.edu/trc/presept/presept_protocol_rev_2.pdf (accessed 5 Jul 2012).
Population
Subjects at least 50 years old and scheduled for colonoscopy at one of the participating clinical centres were approached about volunteering for the study. To ensure that only average risk individuals were enrolled, we excluded those with previous lower endoscopy, previous CRC or adenomas; iron deficiency anaemia or haematochezia (blood in the stool) within the previous 6 months; or family history indicating increased risk for the disease (two or more first degree relatives with CRC or one or more with CRC at age 50 years or less; or known Lynch syndrome or familial adenomatous polyposis). To increase accrual, approximately 6 months after study initiation the CSSC revised the initial eligibility criteria to no longer exclude subjects with flexible sigmoidoscopy more than 5 years before enrolment. Eligibility was assessed through authorised medical record review or subject interview, according to the centre.
Clinical procedures
At least 1 day before initiating colonoscopy preparation, enrolled eligible subjects provided informed consent for the study, baseline information and a single whole blood draw into four 10 ml potassium ethylenediaminetetraacetic acid blood tubes. Plasma was isolated from whole blood,10 aliquoted into coded 2 ml cryotubes and stored at −80°C. Aliquot batches were periodically shipped on dry ice to a central repository for −80°C storage.
Because the intent was to evaluate the assay in the context of routine screening and the centres used were experienced at screening, no attempt at study wide control of colonoscopy or pathology procedures or quality was made. Rather, colonoscopy procedures, including polypectomy and biopsy, were performed by board certified endoscopists at each of the participating centres using board specific screening standards and site specific standards for sedation, monitoring, imaging and equipment. This was to mimic actual screening to the extent possible. Histopathology, diagnostic procedures, and staging of biopsy and surgical specimens used routine procedures at each site. Colonoscopy and pathology reports, including completion and preparation quality, were abstracted onto study forms and entered into the database.
Laboratory methods
Assay of samples from subjects with CRC and subjects without CRC randomly selected from each pathology substratum were in turn randomly allocated to one of three independent laboratories (ARUP, Salt Lake City, Utah, USA; Charite, Berlin, Germany; Quest, San Juan Capistrano, California, USA). The number of samples sent to each laboratory was governed by expected throughput. These laboratories, blinded to the subject clinical results, used the first generation commercially available assay, the Epi proColon Assay (Epigenomics AG, Berlin, Germany), comprised of a plasma DNA preparation kit, workflow control kit (containing the positive and negative controls) and real time PCR kit, to perform all of the laboratory assays, and were trained and qualified on the procedures described in the protocol.
The Epi proColon Assay used in this study was previously described by Rösch and Weiss.13 Briefly, free circulating DNA from 3.5 ml of plasma, obtained through pooling of two aliquots of subject plasma each containing ∼2 ml, was captured on magnetic beads, purified and concentrated. To ensure only methylated cytosine was replicated, the unmethylated cytosine in the purified DNA was then chemically converted to uracil using sodium bisulfite. DNA was then captured again on magnetic beads, purified through washing steps and eluted in a final volume of 55 μl. The resulting bisulfite converted DNA was amplified in a duplex PCR comprised of oligonucleotides for an internal control assay, actin β for determining the validity of the result and oligonucleotides for the target analyte, methylated Septin9. Two separate PCR replicates were prepared with the bisulfite converted DNA eluate from each subject sample by adding 15 µl of eluate to each of two wells of a 96 well PCR plate. Prior to adding subject DNA to the PCR plate, 25 µl of a mixture of PCR buffer, oligonucleotides and polymerase were added to the entire 96 well plate. Real time PCR was performed on an LC480 device (Roche Diagnostics, Indianapolis, Indiana, USA). The remaining ∼25 µl of bisulfite converted DNA material was frozen at −80°C and stored. Technical details, including preparation of the master mix, oligonucleotide sequences and concentrations, and the recommended cycling parameters, are available in the supplementary assay information, which is available as an online supplement.
Positive and negative controls from the workflow control kit were processed with each batch of samples. The positive workflow control contained genomic DNA derived from the HeLa cell line, which is methylated in the region of septin 9 targeted by the assay. The negative workflow control contains genomic DNA derived from the Jurkat cell line in which the targeted septin 9 region is not methylated. Results within runs where the workflow controls did not give expected results and individual samples with inadequate DNA were considered invalid.
PCR curves for mSEPT9 were generated. If a curve exceeded the prespecified threshold within 50 PCR cycles, the reaction was positive (see the online supplementary assay information for exceptions). If at least one PCR replicate from a subject was positive, the assay was positive. Theoretically, patients with early onset of CRC could present with mSEPT9 DNA levels approaching one genomic equivalent (∼2 copies) per plasma sample. In order to detect this small amount of circulating DNA, multiple PCR replicates are used to extend the limit of detection of the assay beyond that of a single PCR reaction.
Electronic copies of the results using blind identifiers were forwarded directly to the statistical centre. For samples with invalid results on the initially retrieved samples, two additional cryotubes were retrieved, processed and assayed for a second and final attempt. Some cases with invalid results could not be reassayed due to insufficient sample volume.
Classification of pathology
Based on review of the clinical and histopathological characteristics documented on study data forms, the CSSC, prior to assay, assigned each adequate colonoscopy outcome (those with adequate preparation and complete to the caecum) to one of four clinical classes: CRC, AA, NA or no evidence of disease (NED). In addition, invasive CRC was subclassified into stages I–IV14; AA were subclassified into high grade dysplasia (HGD), villous architecture without HGD or large polyps (≥10 mm) with neither HGD nor villous architecture.
As the accuracy of the mSEPT9 marker for detection of CRC was the primary objective of this study, to identify potential misclassification of invasive CRC as HGD, or vice versa, histopathological diagnoses for all T1 CRC and all HGD and carcinoma in situ diagnoses (which were grouped as HGD if confirmed on reanalysis) from each site's local pathologist were independently reviewed by two study pathologists (an independent CSSC member and a sponsor study team member) using original diagnostic slides or their images. In the case of disagreement with the original diagnosis, the agreement of two out of three pathologists prevailed.
Post hoc study of a third PCR reaction
In order to analyse the effect of a different and possibly improved analysis method, a single post hoc study examined the impact of an additional PCR replicate (ie, three rather than two wells per subject) on sensitivity and specificity. Because the assay target is available in small quantities, particularly for some early stage cancers, the assay clearly has a stochastic component to it and hence a particular PCR reaction may lack adequate numbers of mSEPT9 copies to trigger DNA amplification. By providing another opportunity to generate a positive result, adding a third PCR measurement necessarily increases sensitivity and decreases specificity, but the amount of change depends on the degree of dependence between the individual PCR results for an individual. To estimate this change, we emulated this three PCR replicate assay by performing an additional blinded PCR reaction on the main study subjects with available residual ∼25 μl of the original bisulfite converted DNA, producing a third PCR curve assessed for positivity by the same criterion as for the first two PCR reactions. A subject was positive if any of the three PCR replicates were positive (either of the two original PCR replicates or the third post hoc replicate). As this post hoc study was done in response to initial results from the main study indicating lower than expected sensitivity of the original assay, it is an exploratory analysis and, unlike the main study result, cannot be considered a validation.
Statistical design and analysis
Enrolment of 7500 subjects was intended to produce 50 CRC. Subjects with incomplete colonoscopies or diagnosed with non-CRC were excluded from the analyses. The target population comprised US and German residents at least 50 years old, based on the 2000 US Census Bureau Database15 and 2000 US Census Bureau International Database.16 Both countries have opportunistic CRC screening programmes that include screening colonoscopy without national invitation or incentive systems.
During accrual, successive batches of enrolled subjects meeting analysability criteria (ie, adequate colonoscopy, complete diagnosis, sufficient blood sample) were sampled for laboratory analysis. The planned distribution for the selected samples was 50 CRC, 300 AA, 200 NA and 900 NED (1450 total). This was based on the primary objective, to estimate sensitivity, specificity and predictive values for CRC and secondary objectives to estimate sensitivity for AA and for NA, and to accrue as many HGD as possible. The sample size of 50 CRC was selected to yield a 95% CI for sensitivity of width of no more than 0.29; the number of AA was to produce a CI no wider than 0.12; the number of NA was to yield a CI no wider than 0.14; and the total number of non-CRC (the sum of AA, NA and NED) was to provide a CI no wider than 0.07. All previously unselected CRC and HGD available at the time of batch sample selection and randomly selected subsets of the other diagnostic groups were included in each batch for laboratory analysis. The diagnostic groups were allocated to laboratories proportionately. The blind identifiers of selected subjects were provided to the study sponsor, who managed the shipment of plasma samples to the participating laboratories. As the laboratories processed each batch, they reported mSEPT9 assay results to the statistical centre.
Crude estimates of the probability of a positive assay (‘positivity’) for different subgroups were obtained by simple ratios. Because sampling was not proportional at any level (eg, age groups were sampled with differing proportions, cases without CRC or HGD were under sampled), estimators were standardised to the target population using the direct method17 ,18 and inverse probability weighting.19 The direct method applies the positivity rates seen in the study population to the structure of the target population. Standardising and weighting covariates were age, sex, ethnicity, enrolment date and diagnostic group. Age and sex frequencies for the USA and Germany were used. Specificity was estimated as 1−positivity among subjects without CRC. Estimates of positive (PPV) and negative (NPV) predictive values were based on the sampling scheme described above. The standard non-parametric bootstrap20 was used to produce 95% CI. For extreme binomial outcomes (eg, 5/5), ‘exact’ confidence limits were used.21 Estimates of differences in proportions among subgroups were similarly standardised. V.2.10.1 of the R statistical software system was used for all computations.22 Details of the sampling of subjects for analysis and the data analysis techniques are contained in the Statistical Analysis Plan, available as online supplementary assay information.
Results
Subjects were enrolled from June 2008 until January 2010. Thirty-two clinical sites—22 in the USA and 10 in Germany—participated, enrolling 7941 subjects. Six subjects were diagnosed with cancers other than CRC: one case each of anal squamous cell carcinoma, ovarian carcinoma with positive lymph nodes and invasion into the colon, cloacogenic/basaloid type squamous cell carcinoma of the rectum and hepatocellular carcinoma; and two rectal carcinoids.
The modified STAndards for the Reporting of Diagnostic accuracy studies (STARD) diagram in figure 1 gives the disposition of all subjects enrolled in the study.23 Nine withdrew but their baseline data were used in the calculation of weights; 12 German subjects withdrew and their data were redacted in accordance with German law. The time between sample collection and colonoscopy averaged 14 days (IQR 6–16 days). Samples from 6874 subjects were available for selection into laboratory analysis, including 53 CRC and 3025 adenomas; this represents an adenoma detection rate of 44.8%. Six laboratory batches were generated by the method described above. Among the 53 cancer cases, 66% were men and mean age was 67 years; among the non-CRC subjects, 45% were men and mean age was 61 years. Figure 2 gives the age–sex distribution for the study sample and the target population from the USA and Germany combined. The biggest difference was a higher proportion of younger individuals compared with the oldest age categories in the study sample compared with the target population structure.

Enhanced STAndards for the Reporting of Diagnostic accuracy studies (STARD) diagram of the disposition of subjects in the study,23 based on the template at http://www.stard-statement.org. aGerman law requires that data from subjects in Germany who withdrew cannot be retained or used for study purposes. bCR, colorectal. cSample either had too little volume or was unusable. dHGD, high grade dysplasia. eCases selected for laboratory analysis in a stratified random sampling.
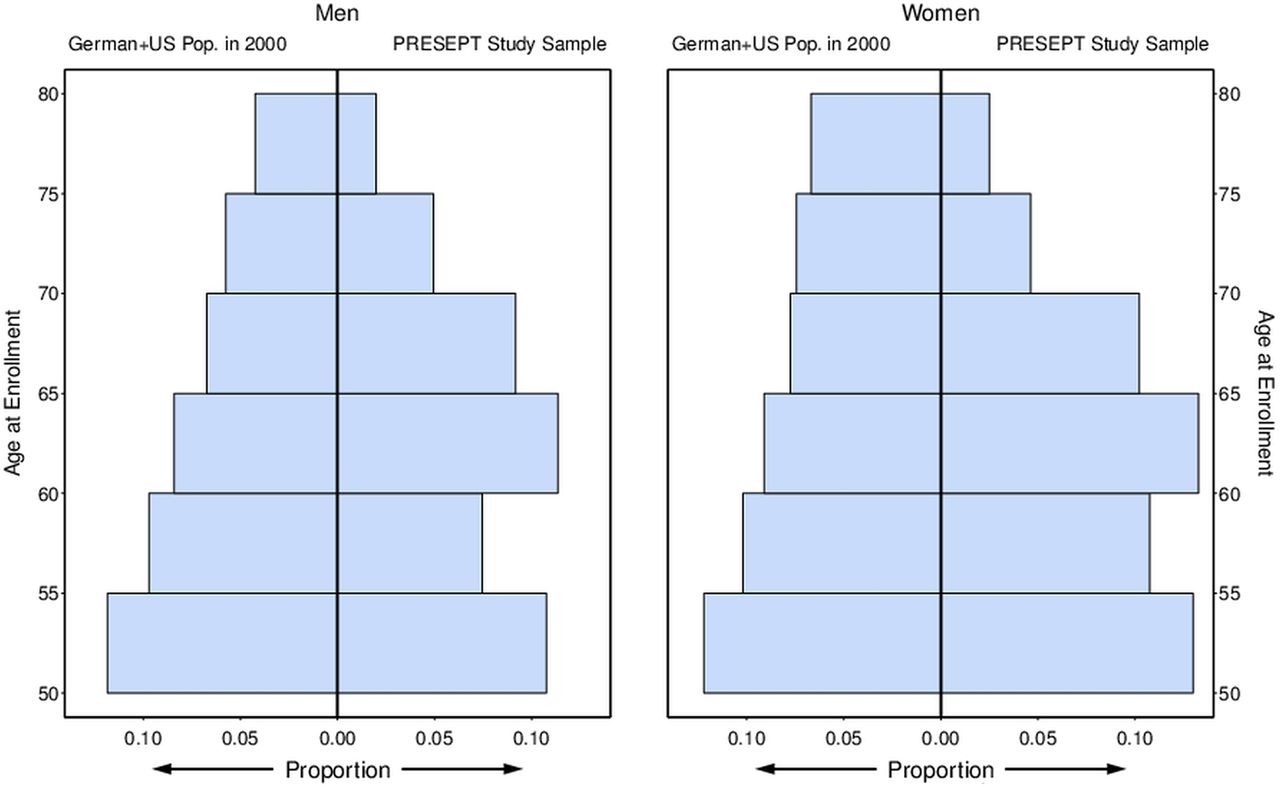
PRospective Evaluation of SEPT (PRESEPT) results: target population and study subjects, age–sex distribution. Target sample and study sample distributions compared by sex and 5 year intervals of age at enrolment from 50 to 80 years (50–54, 55–59, etc). For the PRESEPT study sample (n=1516), the lowest interval of age (50, 55 years) includes one subject aged <50 years. Similarly, the highest interval (75, 80 years) includes 23 subjects who were aged 80 years or more. Proportions extending to the right in each plot represent proportions of the PRESEPT study sample overall; the sum of all proportions from both plots is 1. Proportions extending to the left in each plot represent proportions of the German and US population in the year 2000.
Assay accuracy measures
Figure 3 plots the standardised positivity rates and CI for the mSEPT9 assay results by diagnostic outcome of the colonoscopy. Sensitivity and specificity (1−positivity among ‘non-CRC’ subjects) were 48.2% (95 % CI 32.4% to 63.6%) and 91.5% (95% CI 89.7% to 93.1%), respectively. PPV and NPV were 5.2% (95% CI 3.5% to 7.5%) and 99.5% (95% CI 99.2% to 99.6%), respectively.

Methylated SEPT9 (mSEPT9) positivity rates by clinical findings. mSEPT9 assay positivity estimates and 95% CI by outcome category, standardised to the target population. Dot represents point estimate (Est), bars represent 95% CI. AA, advanced adenomas; CRC, colorectal cancer; HGD, high grade dysplasia; NA, non-advanced adenomas; NED, no evidence of disease; Test, raw result of assay; P, number of positive assays; Tot, number of valid measurements.
With respect to different tumour stages, stage specific sensitivity was 35.0% for stage I, 63.0% for stage II, 46.0% for stage III and 77.4% for stage IV; combined sensitivities for stages I–II versus III–IV were 44.7% vs 54.9%; combined sensitivity for stages I–III (those with any chance of improvement in survival) was 45.1%. For AA, sensitivity was 11.2%, only minimally higher than the positivity rate for subjects without any pathology (9.1%).
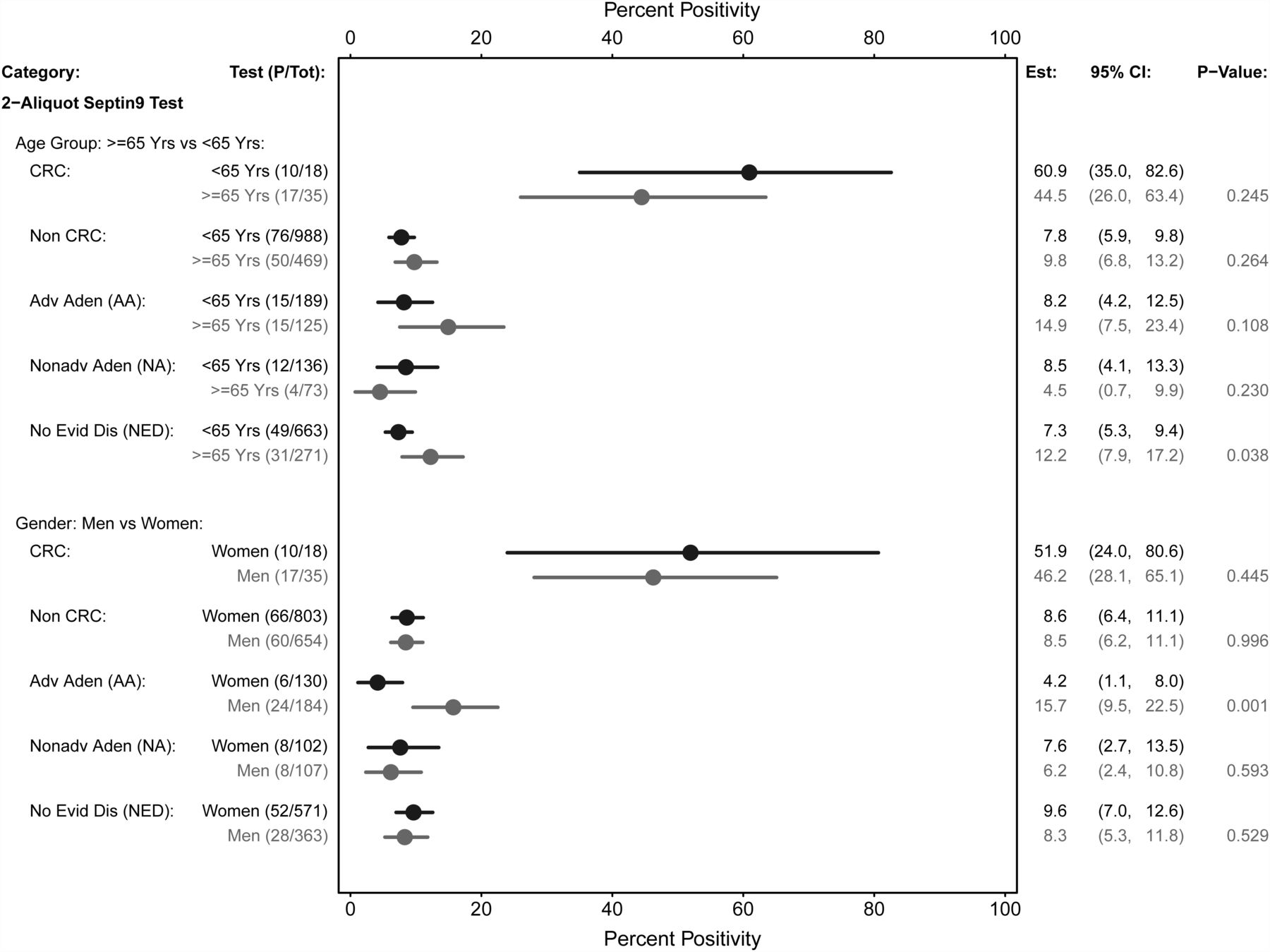
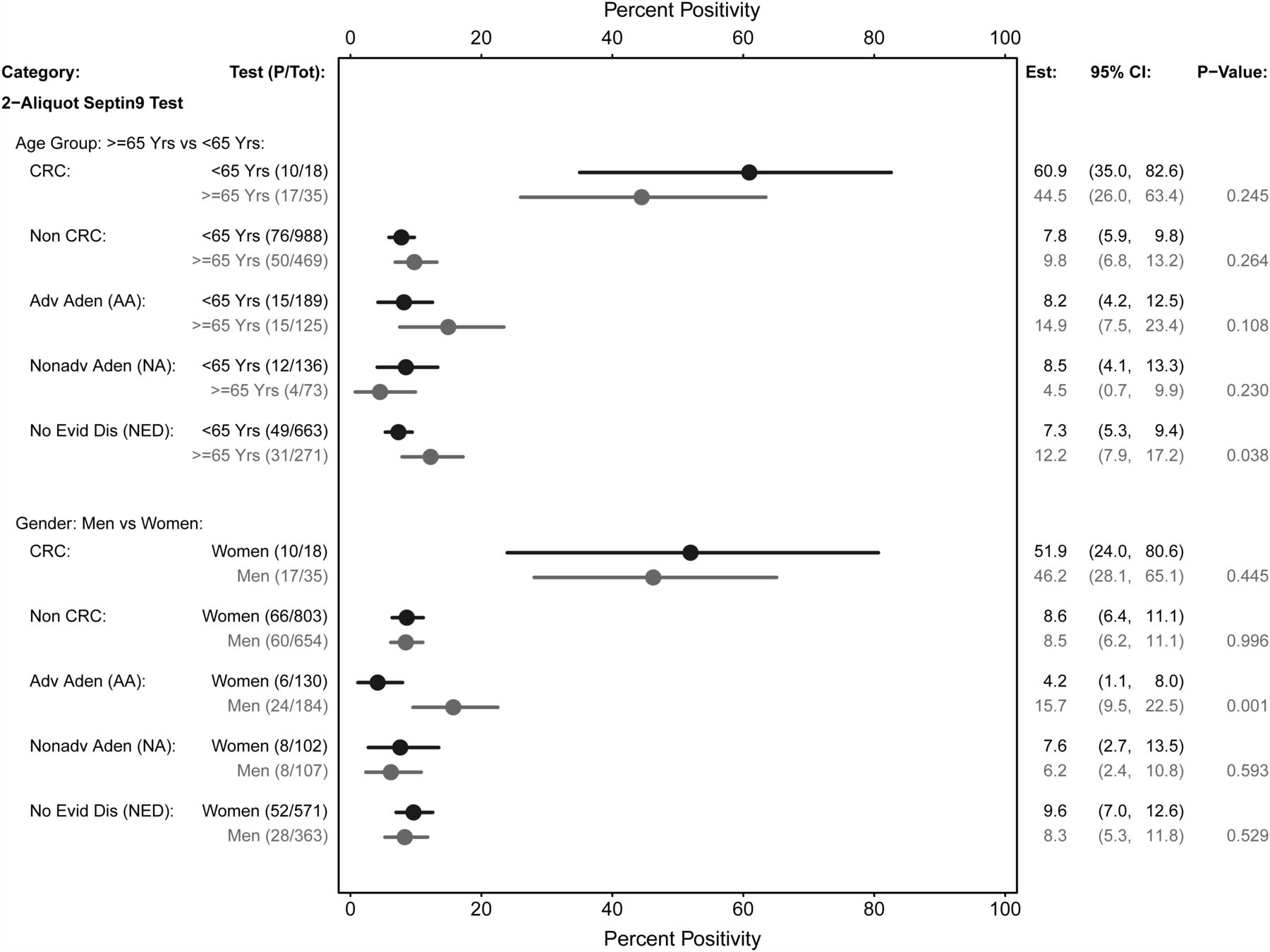
Age and sex
As shown in figure 4, the assay showed greater sensitivity and specificity in younger subjects (<65 years of age) than in older ones, but the differences were not statistically significant. The assay had higher sensitivity in women than in men but specificity was equivalent; again, these differences were not statistically significant.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Methylated SEPT9 (mSEPT9) assay positivity estimates by age, sex and clinical findings. Comparing mSEPT9 assay positivity estimates and 95% CI by age group and outcome category and by sex and outcome category, standardised to the target population. Dot represents point estimate (Est), bars represent 95% CI. AA, advanced adenomas; CRC, colorectal cancer; HGD, high grade dysplasia; NA, non-advanced adenomas; NED, no evidence of disease; Test, raw results of assay; P, number of positive assays; Tot, number of valid measurements.
Distal versus proximal disease
Sensitivities for distal and proximal CRC were 53.3% (95% CI 34.7% to 72.4%) versus 39.4% (95% CI 14.2% to 68.2%), respectively (p=0.282). Note that these analyses did not address different distributions between subgroups by either stage of cancer or polyp subtypes.
Individual PCR results
Among those 53 subjects with CRC, there were 26 (49.1%) who had neither replicate positive, eight (15.1%) who had only one and 19 (35.8%) who had both. The comparable numbers among those 1463 subjects without CRC were 1331 (91.0%), 110 (7.5%) and 16 (1.1%), respectively, with the remaining six (0.4%) invalid.
Post hoc three replicate emulation
Adequate bisulfite converted DNA for a third PCR replicate was available for 51 (of 53) CRC and 1427 (of 1457) non-CRC cases of those previously analysed. Standardised sensitivity and specificity values of the three replicate assay were 63.9% (95% CI 47.5% to 79.2%) and 88.4% (95% CI 86.2% to 90.4%), respectively. PPV and NPV were 4.82% (95% CI 3.53% to 6.73%) and 99.63% (95% CI 99.38% to 99.79%), respectively. For AA, sensitivity was 14.4%, slightly higher than the positivity rate for subjects with no pathology (12.1%).
Discussion
In this prospective study using colonoscopy as the reference standard, we assessed the ability of a plasma based DNA marker, mSEPT9, to detect preclinical CRC in blood samples collected prospectively from an average risk screening population. Retrospective case control studies had suggested that detectable levels of mSEPT9 in plasma identify individuals with CRC with a sensitivity between 52% and 72% and specificity between 90% and 95%.8–10 Another recent case control study by Warren et al24 obtained estimates of 90% for the sensitivity and 88% for the specificity of mSEPT9. These previous study results motivated the present prospective study, which was performed in a screening setting, in contrast with previously published results derived from cases diagnosed symptomatically (thus likely to be qualitatively different from asymptomatic cases) and convenience sample controls (which may not represent the asymptomatic population) and so had limited generalisability.25 Our study design and analysis avoided those pitfalls; our results demonstrated lower sensitivity than the previous case control studies.
The primary assay used for the study, based on the first commercially available mSEPT9 assay, could detect 48.2% of cases of preclinical CRC with 91.5% specificity in the target population. Most of the CRC identified during the course of examination were stages I–III, and sensitivity was lower for earlier tumour stages. Sensitivity was very low for AA and only slightly higher than the false positive rate for all individuals who did not have cancer, indicating that there is at present no utility in detecting important precancerous lesions.
Screening for CRC not only reduces mortality from the disease26–29 but also incidence.30 ,31 However, a national survey in the USA reported that only about 50% of the eligible population had been screened according to guidelines.32 In Germany, a survey among 1808 randomly selected persons revealed that about 40% of those over the age of 50 years had undergone some form of colonoscopy.33 Blood based tests have long been sought in the cancer detection field for their convenience and potential for higher compliance; nevertheless, higher uptake, higher yield of precancerous lesions and finally any effect on mortality would still have to be shown. At present, it can therefore only be speculated whether a blood test with faecal occult blood test (FOBT)-like performance would produce similar reductions in incidence and mortality to those seen in previous randomised FOBT trials.26–29 Our study only assessed performance in a screening setting, and cannot assess other factors such as uptake. In comparison with FOBT, which is still widely used and implemented in some national programmes,34 the mSEPT9 assay yielded a CRC sensitivity of 48%, which is at the lower end of the guaiac FOBT range (37–79%).35 The specificity of mSEPT9 was 92%, compared with a range of 87–98% for the guaiac test.35 PPV for standard rehydrated guaiac FOBT used in the Minnesota study was 5.6%,26 compared with 5.2% for mSEPT9 in this study. However, these comparative performance characteristics would suggest that, even in a programme of repetitive annual screening, use of the mSEPT9 assay would not produce a decline in mortality commensurate to that seen with a sensitive guaiac test.
Furthermore, newer faecal immunochemical stool tests for haemoglobin (FIT) may provide improved performance characteristics36 as well as slightly superior uptake rates37; therefore, FIT is increasingly being used instead of guaiac FOBT in countries introducing screening programmes (eg, The Netherlands).38 A newer faecal DNA test has reported sensitivities of 85% for CRC and 54% for adenomas ≥1 cm (based on a single case control design using a stool bank).39 The same group40 recently evaluated mSEPT9 in parallel with a stool based DNA test in a small retrospective study in CRC and large adenomas. The study also reported a modest sensitivity and very low AA detection rate for mSEPT9. They estimated the sensitivity of mSEPT9 for large adenomas at 14% and for CRC 60%, somewhat higher than our study, but with larger CI. The source of the samples was the Mayo Tumour Registry, but the exact selection criteria for the samples are not given and the mSEPT9 test was not performed in the same manner. In the same study, comparative sensitivity of faecal DNA was higher for cancer (87%) as well as adenomas ≥1 cm (82%). However, evidence from these latter studies is limited as they were neither performed prospectively nor in a screening setting.
As a large proportion of human CRC tissue contains relatively high amounts of mSEPT9 regardless of tumour stage, improvement of DNA isolation or increased PCR efficiency may result in better marker performance. Unfortunately, tissue samples from the current study were not collected for testing to determine whether the tumours contained significant amounts of mSEPT9. Improvements in the test appear to be possible, as shown by our post hoc analysis using the three PCR replicate emulation which mimics the second generation commercially available mSEPT9 assay and which detected nearly two-thirds of cases, but yielded false positives in 12% of non-cases. The three replicate approach needs to be tested prospectively. The emulation used in this post hoc analysis imprecisely reproduced a simultaneous three replicate assay, for three reasons: (1) the decision to look at a third PCR replicate was based on lower than expected two replicate assay sensitivity, leading to lower estimated three replicate assay sensitivity; (2) the third PCR replicates were not done in the same run on the same machine as the first two, unlike an actual three PCR replicate assay, allowing increased run to run variation to lower the assay discrimination; and (3) criteria for invalid results differ slightly because in practice, all three replicates would have common control samples and be subject to the same probability of invalidity. For these reasons, estimated sensitivity of the three replicate assay is likely to be smaller than true sensitivity; the effect on specificity is less clear but probably small. Thus the three replicate results are strictly exploratory. In addition, because the assay is working with what are small quantities, the assay clearly involves a stochastic component, and hence a particular PCR replicate may lack adequate numbers of mSEPT9 copies to trigger DNA amplification. Additional replicates merely provide more opportunities to yield a positive, thus increasing sensitivity while decreasing specificity. Therefore, it can only be speculated whether this more recent assay version might perform better in the screening setting. Similarly, we do not know whether the accuracy of the three replicate mSEPT9 assay might approximate available immunochemical stool tests. Still, detection of adenomas as precursor lesions would also have to be improved. The choice of a blood based assay, such as mSEPT9, in a programme of CRC screening depends on multiple features not assessed in this study, including the potential for increased compliance, the necessary frequency of testing and features of competing tests, such as cost. The current cost of the mSEPT9 test in Europe is approximately 150 Euros, considerably more than faecal tests but less than a colonoscopy. In any event, the comparative effectiveness and cost of various strategies of screening with mSEPT9 requires further evaluation.41 ,42
There are limitations to our study:
-
Because the centres enrolling in the study were not randomly sampled and study subjects were sampled from the study centres disproportionately by clinical findings for laboratory testing, standardisation to some target screening population was necessary to obtain relevant performance estimates. Although in any non-random sample there may be unknown factors for which standardisation is impossible and there is always some error in the standardisation variables, our standardisation included the main determinants of CRC incidence, age and sex, and they had negligible measurement errors.
-
To increase accrual, the entry criterion regarding prior endoscopy was relaxed soon after the beginning of enrolment. This probably reduced the overall prevalence rate, but we believe it had little impact on the assay parameter estimation.
-
Although no split sample quality control was performed to examine consistency between laboratories, there was no statistically significant difference in the frequency of findings between them (data not shown).
-
Although subjects with other cancers found on examination were excluded from the primary analysis, sensitivity analyses including these cases only slightly affected the quantitative results (analyses not shown).
It should also be mentioned that we do not believe that the mSEPT9 results are generalisable to other blood based tests for CRC. To the contrary, each marker should be evaluated not only in isolation but also as an adjunct to other markers, much as Ahlquist and colleagues43 have done with stool based markers.
In conclusion, the blood based mSEPT9 assay detected about half of the preclinical CRC with specificity similar to guaiac based FOBT, in this prospective masked study of screening subjects. Sensitivity of mSEPT9 for advanced adenomas was very low. Although this renders the clinical utility very low, there might be ways to achieve possible improvements, as suggested by our post hoc analysis as well as by a recent case control study.24 The utility of the test for population screening for CRC will require improved sensitivity for detection of early cancers and advanced adenomas. Nevertheless, these and all other tests potentially to be used for CRC screening have to be prospectively tested in the screening setting, where they would finally be applied. One implication of our study is that performance estimates may differ substantially in such settings compared with retrospective case control studies.
Appendix
A list of PRESEPT site principal investigators, coordinating investigator for the German investigative sites, providers of statistical and clinical data support, medical advisors and Clinical Study Steering Committee members is available as an online supplement.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online appendix
Footnotes
-
Contributors TRC had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. TRC, MW, CL-D, SRP, BAB, TR, NO, DS, RWD and DFR were responsible for study conception and design. TRC, MW, CL-D, SJM, MB, SRP, EC-V, TR, NO and DS were responsible for acquisition of the data. Analysis and interpretation of the data was done by TRC, MW, CL-D, SJM, MB, SRP, EC-V, BAB, TR, NO, DS, RWD and DFR. Drafting of the manuscript was done by TRC, MW, CL-D and DFR. Critical revision of the manuscript for important intellectual content was performed by TRC, MW, CL-D, SJM, MB, SRP, EC-V, BAB, TR, NO, DS, RWD and DFR. TRC, SJM, MB and BAB were responsible for statistical analysis. Obtaining funding was the responsibility of MW, CL-D and RWD. Administrative, technical or material support was provided by MW, CL-D, MB, SRP and RWD. Supervision: TRC, MW, CL-D, SRP, TR, NO and RWD.
-
Funding The PRESEPT study was funded by Epigenomics AG, Berlin, Germany. Epigenomics drafted and finalised protocols, training materials and forms, created and maintained study databases and management systems, selected and contracted with study centres, collected and entered clinical study data, stored collected specimens (with blind identifiers), monitored centres and performed site audits. It also organised and attended CSSC meetings, advised on study procedures and recommended study strategies. Two members of the CSSC were employees of Epigenomics, but membership was limited to them to ensure that a majority of the committee were not affiliated with the company.
-
Competing interests TRC's institution received from Epigenomics a grant, travel support, fees for participation in review activities, and payment for writing or reviewing the manuscript. As a former employee of Epigenomics, MW received travel support, fees for participation in review activities and stock options that were not exercised and have now expired. He has also received consultancy fees from Exact Sciences, Inc. For his current compensated employment at Rice University, Houston Area Translational Research Consortium, MW is a co-author of an MD Anderson Cancer Center grant application, which was submitted to the Cancer Prevention Research Institute of Texas (CPRIT) for funds to support pre-commercialisation of a multiplex proteomic assay for early detection of colorectal cancer. CL-D received employment compensation and stock/stock options from Epigenomics. SJM's institution received from Epigenomics travel support, fees for participation in review activities, and payment for writing or reviewing the manuscript. MB received employment compensation from Epigenomics AG. As a previous employee of Epigenomics, SRP received payment for writing or reviewing the manuscript. EC-V was employed by Epigenomics AG, from 2006 to 2011, and received employment compensation. BAB received from Epigenomics consulting fees, travel support, fees for participation in review activities, payment for writing or reviewing the manuscript, and provision of writing assistance, medicines, equipment or administrative support. TR received travel support from Epigenomics and consultancy fees from GI Dynamics. His institution has grants/grants pending with Olympus, Erbe and Storz. DS received from Epigenomics travel support, fees for participation in reviewing activities and consulting fees. RWD received from Epigenomics a consulting fee or honorarium, travel support and stock/stock options. DFR received travel support from Epigenomics.
-
Ethics approval University of Minnesota—institutional review board study No: 807M39501; EU—Charite approval number: EA2/069/08; USA—Western IRB Protocol No: 20080713.
-
Provenance and peer review Not commissioned; externally peer reviewed.