Article Text

Abstract
Introduction Patients with Crohn’s disease (CD) often have low levels of vitamin D (Vit D). Initially considered to be secondary to active disease, there is growing evidence that Vit D has a role in immune regulation and that deficiency might contribute to flares of disease. If this hypothesis is correct, CD should exhibit discernible seasonal fluctuations in activity, associated with changing Vit D levels, but studies over three decades have produced conflicting results.
Method Severely active CD requires hospitalisation. We retrospectively analysed consecutive admissions over 44 months (Feb 2010-Sept 2013) to our two district general hospitals in outer North East London, where the primary diagnosis was CD. Admissions lasting less than two days were excluded, to avoid counting patients attending for elective investigations or treatment. Variation in Vit D levels in our locality was modelled from the proportion of primary care patients deficient in Vit D (serum total 25(OH)D <25 nmolL) each month from Oct 2012 to Sept 2013. 31,000 requests for Vit D levels were made by GPs during this period. Seasonal variations in and associations between Vit D levels and admissions for CD were assessed by Hewitt’s test1and Spearman rank correlation, respectively.
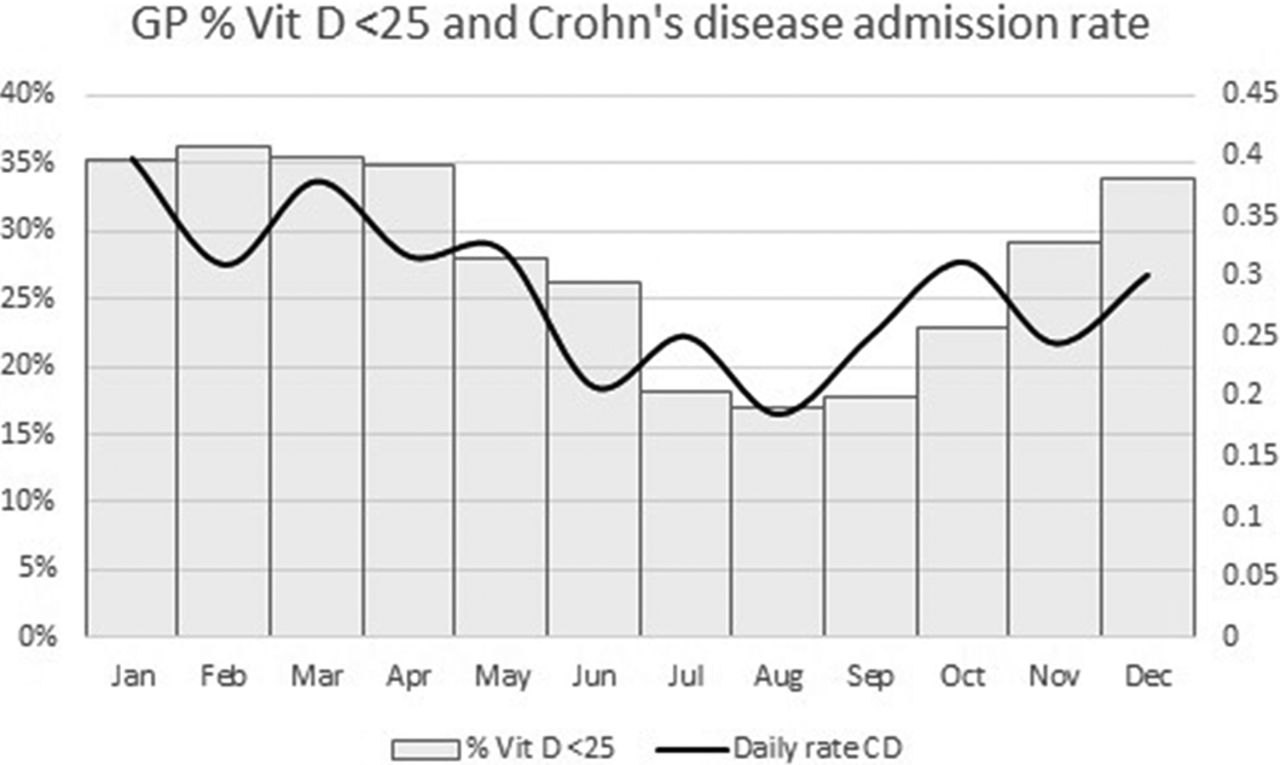
Results 385 admissions for CD were recorded in the 44 month period. 40% more admissions occurred December–May than June–November (p < 0.05). We observed the expected seasonal variation in Vit D levels (p < 0.01). The curves for monthly admissions plotted alongside percentage of Vit D deficiency coincide, with a correlation coefficient of 0.65, p < 0.05, see Figure 1.

{kind=link}
GP% Vit D < 25 and Crohn’s disease admission rate
Conclusion Our study confirms seasonal variation in admissions to hospital for CD in outer NE London and suggests for the first time in the UK that more than 40% of this fluctuation might be accounted for by changes in Vit D levels. Since we used community levels as a surrogate for the Vit D levels of our patients, the influence of active disease secondarily lowering Vit D can be discounted. Our results justify the systematic assessment of Vit D levels in patients with CD and give further impetus to evaluation of Vit D supplementation.
Disclosure of interest None Declared.
Reference
Walter SD. Exact significance levels for Hewitt’s test for seasonality. J Epidemiol Community Health 1980;34:147–149