Article Text

Abstract
Introduction Infliximab (IFX) is an important agent in the treatment of inflammatory bowel disease (IBD). However, its use may be limited by the development of antibodies to infliximab (ATI). The aim of this study was to assess the timing and significance of ATI development in clinical practice.
Method Since May 2016, all IBD patients receiving intravenous IFX for maintenance treatment, at a large, single, referral centre, have undergone therapeutic drug monitoring (TDM). Serum IFX trough levels and ATI were both measured by drug-tolerant enzyme-linked immunosorbent assays (Biohit, UK) from 199 patients at a variable interval following the start of IFX treatment. IFX trough levels were considered undetectable (<0.8 mg/L), low (0.8–2.9 mg/L), therapeutic (3–7 mg/L) and supratherapeutic (>7 mg/L). ATI were considered positive if >10 mg/L. Clinical remission was defined as a Harvey Bradshaw Index or Simple Colitis Activity Index≤4. Risk factors for ATI development were assessed by binary logistic regression model, using 522 sera taken from patients on maintenance therapy. Time to develop ATI, undetectable IFX levels and loss of response to treatment was assessed by Cox regression and Kaplan-Meier analysis.
{kind=link}
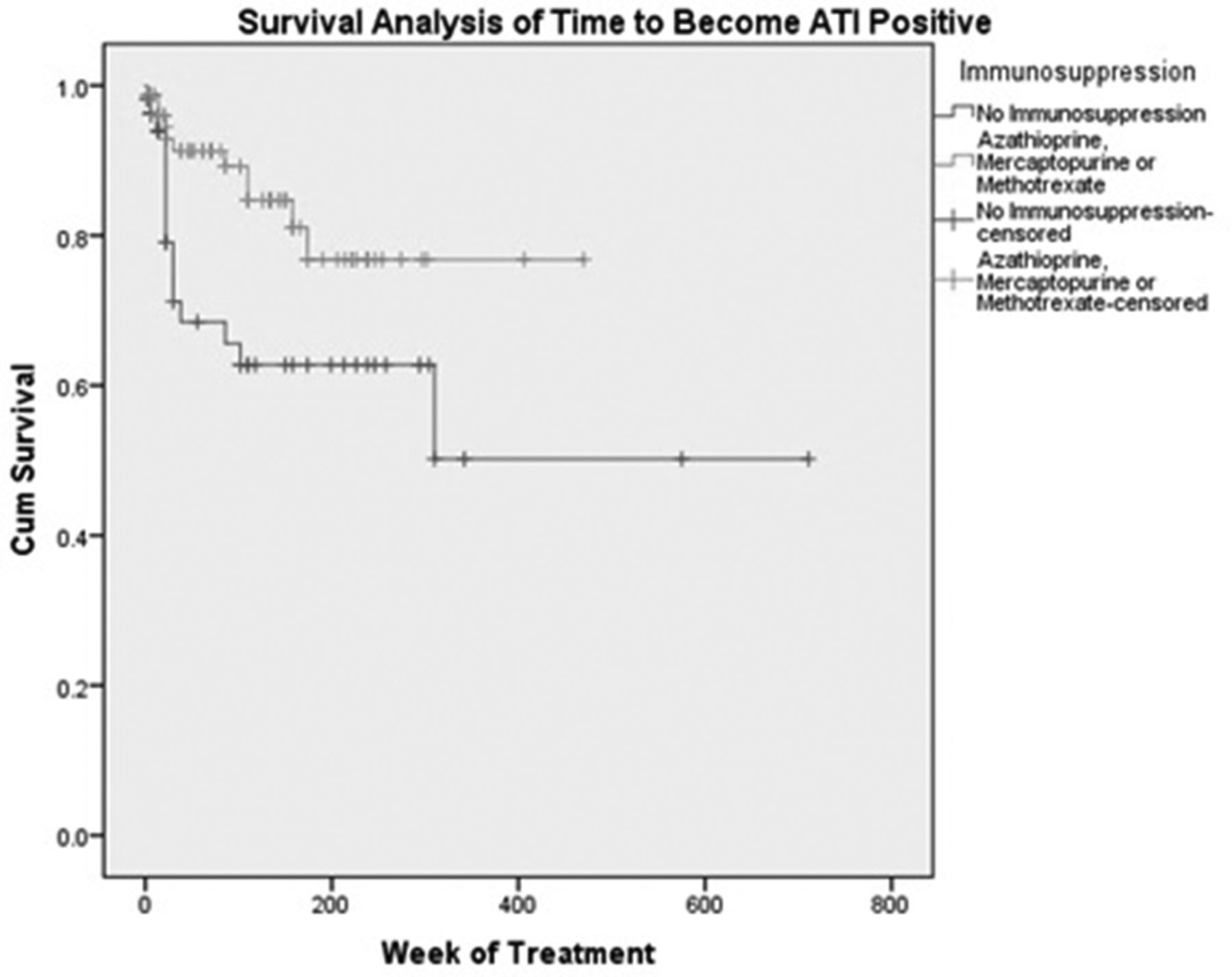
Results Male sex (OR=2.1; p<0.001), week of treatment (OR for each extra week of treatment=0.999; p<0.038) and use of concomitant immunosuppression (IS) (OR=0.373; p<0.001) were associated with ATI formation. During the period of observation, those not taking IS were more likely to develop ATI at any time throughout their IFX treatment (Hazard Ratio=2.4; p=0.03). 59/199 patients were ATI positive at their first TDM, of whom 2 were in their first 6 months of IFX treatment. 140/199 patients were ATI negative at their first TDM. During follow-up, we observed 32 patients develop ATI (19 patients developed antibodies within 6 months of starting IFX treatment, 5 between 6–12 months treatment and 8 after 12 months). At any given time, patients with positive ATI are 3.4 times as likely (p=0.002) to develop undetectable levels than ATI negative patients. Transient ATI formation was seen in only 5/162 patients.
Conclusion Although IS therapy protects against ATI formation, the risk of antibody development continues throughout treatment. If concomitant IS is aimed at reducing ATI formation, then this also needs to be continued for the duration of IFX therapy.
Disclosure of Interest None Declared
- Antibodies to Infliximab
- Infliximab