Article Text

Statistics from Altmetric.com
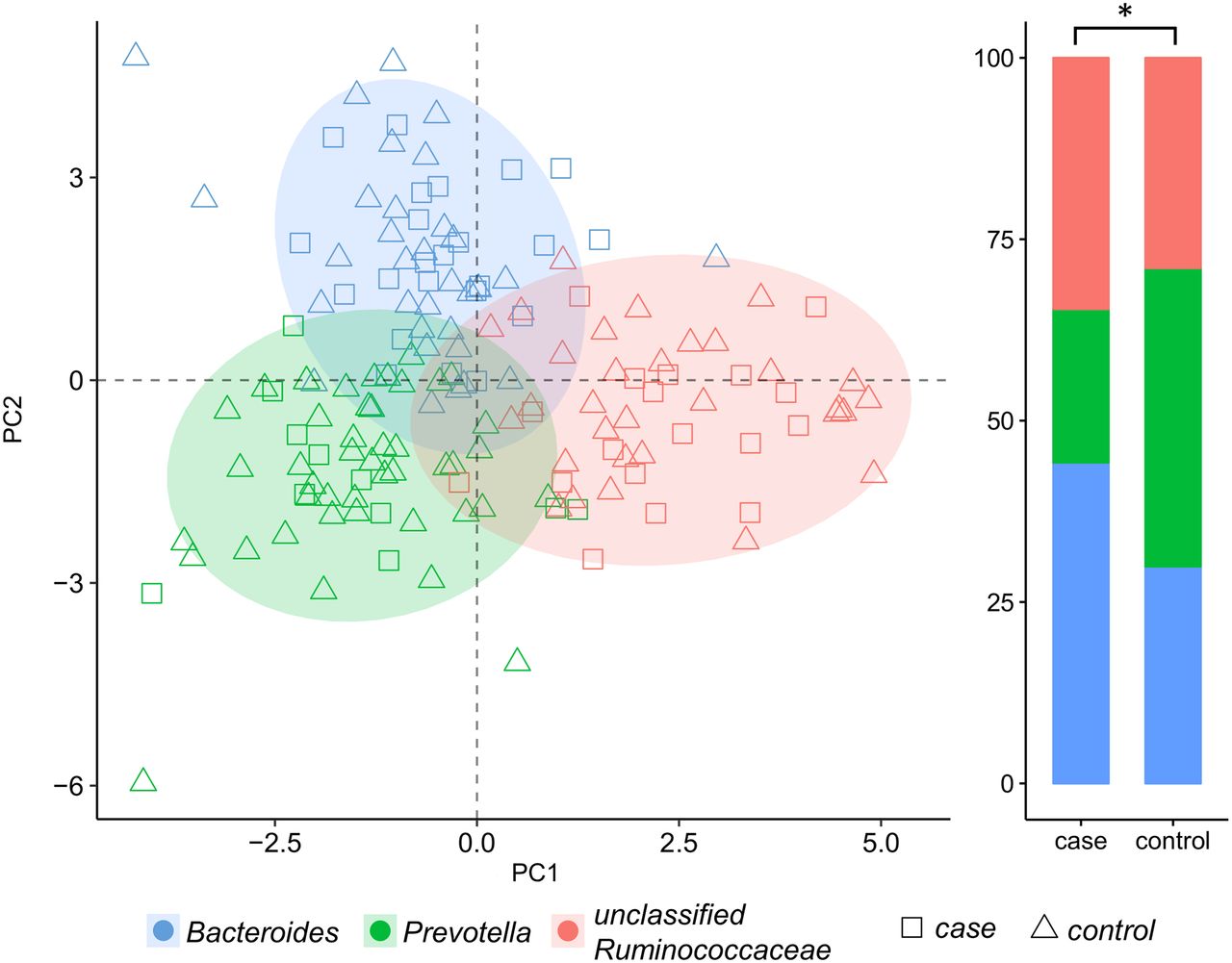
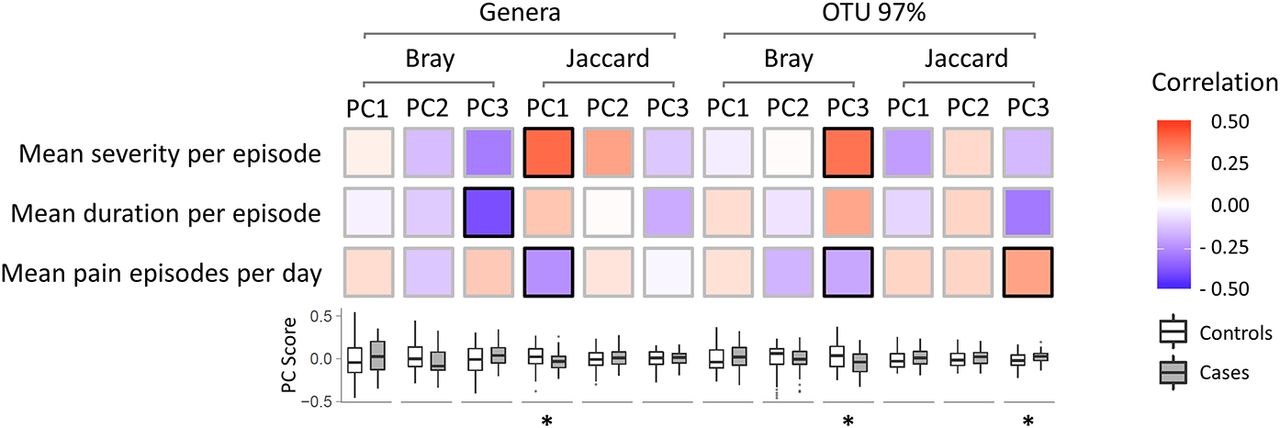
We read with great interest the recent communication by Simrén et al,1 reporting a correlation between visceral hypersensitivity and GI symptom severity in functional GI disorders (FGID). Previously, it has been shown that visceral hypersensitivity can be modulated or even induced in animal models, by altering the composition of their gut microbiota with antibiotics or faecal transplantation from IBS donors.2 3 Hence, while a direct link between gut microbiota composition and visceral pain may need to be conclusively established, this holds great potential for translational exploitation in the treatment of IBS and other FGID. Thus far, the potential association between microbiota and abdominal pain in humans has only been investigated in one study that included 15 individuals.4 For this purpose, we studied 159 individuals (average age 59.1, 39.6% men) from the Swedish Population-based Colonoscopy (PopCol) cohort, previously described and with faecal microbiota 16S sequencing data and daily recordings of abdominal pain (number of episodes, duration and intensity) collected over the same period (7.41±7.91 days).5–7 Among these, 52 individuals (assigned to the case group) reported at least one episode of light, moderate or intense pain (respective scores 1, 2 and 3), while the other 107 (controls) never reported pain. On average, those with pain experienced it 0.30 times per day (range 0.07–1.57), for 2.46 hours each time (range 0.37–9) and on a light-moderate intensity level of 1.39 per episode (range 1–2.1). When compared, both at the level of genus and species-level operational taxonomic units (OTU), β-diversity measures of faecal microbiota from cases and controls significantly differed (figure 1). In addition, significant correlations with microbiota β-diversity were detected for pain indices of frequency, duration and intensity (figure 1). Classifying individuals according to their microbiota profiles clustered into enterotypes (http://enterotyping.embl.de) resulted in three groups, respectively, enriched for unclassified Ruminococcaceae, Prevotella and Bacteroides. As shown in figure 2, a χ2 analysis revealed their distribution to be significantly different in cases and controls (p=0.039), and the Prevotella-predominant enterotype was underrepresented in the pain group (21% vs 41% in controls). When taxa previously associated with abdominal symptoms in animal models and clinical studies (Bacteroides, unclassified Ruminococcaceae, Butyricicoccus, Prevotella, Faecalibacterium, Streptococcus, Bifidobacterium, Blautia, Akkermansia, Lactobacillus, Alistipes and Enterobacter) were compared with a Wilcoxon rank-sum test for their abundance in the pain and control groups, Benjamini-Hochberg corrected significant differences were observed for Prevotella (decreased in cases, p=0.038), Blautia (increased in cases, p=0.045), Streptococcus (increased in cases, p=0.038) and Lactobacillus (increased in cases, p=0.038). In particular, in an indicator value analysis on genus level, Prevotella could significantly predict the absence of abdominal pain (corrected p=0.016, association statistics=0.76 using the multipatt function of the R package indicspecies). Similar results were obtained when testing correlations with pain frequency, duration and intensity and after removal of individuals (n=18) whose questionnaire data were compatible with a diagnosis of IBS according to Rome III criteria (not shown).

Faecal microbiota β-diversity associates with abdominal pain. Top: Heat map of Spearman correlation between pain indices and faecal microbiota β-diversity, based on principal coordinate analysis applied to Bray-Curtis and Jaccard matrices at the level of genera (Genera) and operational taxonomic units with 97% sequence similarity (OTU 97%). The first three principal coordinates (PC) are reported (PC1, PC2 and PC3) and significant correlations (false discovery rate < 0.1) are highlighted by a black frame. Bottom: Box plots of PC scores in cases and controls, where significant differences (corrected p value<0.05) are highlighted with *.
{kind=link}
{kind=link}
Faecal microbiota enterotype distribution differs in individuals with abdominal pain compared with controls. Principal component analysis (left) and relative distribution (right) of enterotypes according to the presence (case) or absence (control) of abdominal pain. Participants were classified into three enterotypes primarily characterised by unclassified Ruminococcaceae, Prevotella or Bacteroides. *p<0.05.
Our results provide novel evidence linking faecal microbiota composition to the occurrence of abdominal pain and its frequency, duration and intensity in the general population. The negative association of Prevotella with pain parallels observations previously made in IBS studies where the Prevotella-predominant enterotype was shown to be less common among patients.8 The information we report at the general population level may contribute to translational opportunities for the identification and treatment of individuals at risk of IBS and other FGIDs and warrants further studies in independent populations.
Footnotes
Contributors MDA had the original idea and designed the study together with FH. SW, ANA, LE, NJT and LA collected material, characterised the study subjects and acquired data. AF, JB, CB and SS performed microbiota sequencing. FH, FB, MB, MV, LB, JR and MDA did the data analysis and interpretation. FH and MDA drafted the manuscript with critical revision from all authors.
Funding Supported by funds from the Swedish Research Council (“Vetenskapsradet”) to MD and the European Union Seventh Framework Program (FP7/2007-2013, grant number 262055, ESGI) to MD, SS and AF; Iranian ministry of health and medical education to FH; FH is a member of the Research Training Group (RTG) 1743 “Genes, Environment and Inflammation”, funded by German Research Foundation (DFG).
Competing interests None declared.
Patient consent None.
Ethics approval Karolinska Institute.
Provenance and peer review Not commissioned; internally peer reviewed.