Article Text

Abstract
Objective To investigate the efficacy and safety of two different budesonide formulations (effervescent tablet for orodispersible use (BET) and viscous suspension (BVS)) with different daily dosages for short-term treatment of eosinophilic oesophagitis (EoE).
Design Adults with active EoE (n=76) randomly received 14 days’ treatment with either BET 2×1 mg/day (BET1, n=19) or BET 2×2 mg/day (BET2, n=19), or BVS 2×5 mL (0.4 mg/mL)/day (BVS, n=19) or placebo (n=19) in a double-blind, double-dummy fashion, with a 2-week follow-up. Primary end point was histological remission (mean of <16 eosinophils/mm2 hpf). Secondary end points included endoscopy score, dysphagia score, drug safety and patient's preference for drug formulation.
Results Histological remission occurred in 100%, 94.7% and 94.7% of budesonide (BET1, BET2, BVS, respectively) and in 0% of placebo recipients (p<0.0001). The improvement in total endoscopic intensity score was significantly higher in the three budesonide groups compared with placebo. Dysphagia improved in all groups at the end of treatment; however, improvement of dysphagia persisted only in those treated with BET1 (p=0.0196 vs placebo). There were no serious adverse events. Local fungal infection (stained fungi) occurred in two patients of each budesonide group (10.5%). The effervescent tablet was preferred by 80% of patients.
Conclusions BET or BVS was highly effective and safe for short-term treatment of EoE. The 1 mg (twice daily) dosage was equally effective as the 2 mg twice daily dosage. The majority of patients preferred the effervescent tablet formulation.
ClinicalTrials.gov number NCT02280616; EudraCT number, 2009-016692-29.
- OESOPHAGITIS
- DYSPHAGIA
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Eosinophilic oesophagitis (EoE) incurs a significant symptom burden, with the risk of severe complications, and is typically chronic and persistent.
Placebo-controlled trials have proven that topical budesonide suspension is effective for short-term treatment of EoE, achieving high histological remission rates.
There is no oesophageal-targeted, approved formulation of budesonide or any other topical corticosteroid for oesophageal indications.
What are the new findings?
A double-blind, double-dummy, randomised, placebo-controlled, multicentre trial compared budesonide effervescent tablets 2×1 mg/day (BET1) or 2×2 mg/day (BET2) for orodispersible use versus oral budesonide viscous suspension (BVS) 2×5 mL/day (0.4 mg/mL) for short-term induction treatment of active EoE.
Histological remission occurred in 100%, 94.7%, 94.7% and 0% of patients in the BET1, BET2, BVS and placebo groups, respectively (p<0.0001), with significantly higher improvement in total endoscopic intensity score in the three budesonide groups versus placebo.
Dysphagia improved significantly in all groups by the end of treatment. However, improvement of dysphagia persisted at 2 weeks after the end of treatment only in those treated with BET1 (p=0.0196 vs placebo).
How might it impact on clinical practice in the foreseeable future?
Short-term treatment for active EoE with budesonide, administered either as effervescent tablets or as a viscous suspension, offers effective remission of eosinophilic inflammation and improves endoscopic abnormalities.
Introduction
Eosinophilic oesophagitis (EoE) is a chronic, immune/antigen-mediated oesophageal disease characterised clinically by symptoms of oesophageal dysfunction and histologically by eosinophil-predominant inflammation on oesophageal biopsies.1 ,2 Epidemiological studies from Europe3 ,4 and North America5–8 have demonstrated a rapid rise in the incidence and prevalence of EoE over the past decade, which may be partly caused by increasing disease awareness.7 EoE occurs in all age groups with a predominance in younger men,5 ,8 and is associated with a significant symptom burden and a risk for severe complications such as food impaction and oesophageal perforation.9 Characteristic endoscopic findings of EoE include longitudinal furrows, white exudates and oedema representing signs of acute inflammation, but also fixed oesophageal rings and strictures indicating progression to fibrosis and oesophageal remodelling.10 ,11 The natural course of the disease is, in the majority of patients, chronic and persistent.12 ,13 A recent retrospective study demonstrated that the duration of untreated disease was significantly associated with stricture formation, ranging from 17% within 2 years up to 71% within 20 years.13
The proof of concept that topical corticosteroids are useful in EoE has initially been demonstrated by studies using nebulised fluticasone in paediatric patients with EoE.14 ,15 Subsequently, two placebo-controlled trials have proven that topical budesonide suspension is effective for short-term treatment of EoE in children and adults16 ,17 achieving high histological remission rates as the primary end point. Furthermore, a randomised trial in adult patients with EoE showed that topical budesonide was superior in terms of mucosal contact time and histological and endoscopic responses when administered as viscous suspension compared with nebulised delivery18 underlining the importance of the mode of drug delivery to the oesophagus. So far, all therapeutic trials have been performed using topical corticosteroids from approved inhalants or liquid investigational medicinal products. Despite the widespread use of synthetic steroids in clinical practice, there is no targeted oesophageal, approved formulation of any topical corticosteroids for oesophageal indications.
Budesonide is a highly potent, locally active glucocorticosteroid with an extensive first-pass metabolism in the gut and the liver and low systemic exposure. It is available in various pharmaceutical formulations for a variety of GI and pulmonary indications. Recent studies of budesonide effervescent tablets used as mouthwash in patients with oral chronic graft versus host disease or as effervescent tablet for orodispersible use (BET) in patients with active EoE demonstrated a very low systemic bioavailability of budesonide.19 ,20
The aim of the present study was to compare the efficacy and safety of budesonide BET 2 mg (BET1) and 4 mg (BET2) per day versus oral budesonide viscous suspension 2 mg per day for short-term induction treatment of active EoE.
Methods
Study design and population
This was a double-blind, double-dummy, randomised, placebo-controlled, parallel multicentre Phase IIa dose-finding study, conducted in 21 centres in Germany (n=16), Switzerland (n=3) and Belgium (n=2) (ClinicalTrials.gov number, NCT02280616; EudraCT number, 2009-016692-29).
We included male and female patients between 18 years and 75 years of age with a confirmed clinicopathological diagnosis of active EoE according to the following diagnostic criteria: clinical symptoms of oesophageal dysfunction (dysphagia score ≥3), peak eosinophils (eos) ≥65/mm2 high power fields (hpf) in at least 1 hpf (corresponding to ≥20 eos/hpf), and eosinophilic tissue infiltration with a mean cell density ≥16 eos/mm2, as measured in a total of 30 hpf derived from six biopsies, two each from the proximal, mid and distal segments of the oesophagus.
Patients were not eligible for the study if one of the following exclusion criteria was present: clinical and endoscopic suspicion for GORD, achalasia or scleroderma; history of abnormal pH monitoring of the distal oesophagus or clinicopathological response to a treatment with proton pump inhibitors (PPIs) at a standard dose with a treatment duration of at least 2 weeks; other clinical evidence of causes other than EoE for oesophageal eosinophilia; any concomitant oesophageal disease and relevant GI disease; history of oesophageal surgery at any time or of oesophageal dilation procedures within the last 8 weeks prior to screening; any relevant systemic disease if careful medical monitoring was not ensured; abnormal hepatic function, liver cirrhosis or portal hypertension; abnormal renal function; history of cancer in the last 5 years; upper GI bleeding within 8 weeks prior to screening; systemic therapies for any reason that may have affected assessment of primary and secondary end points (ie, systemic glucocorticoids, histamine antagonists, mast cell stabilisers, leukotriene receptor antagonists, biologics, immunosuppressants) concomitantly or within 4 weeks prior to screening; treatment with topical therapies for any reason that may affect assessment of primary and secondary end points (ie, topical glucocorticoids, inhaled sodium cromoglycate) concomitant or within 2 weeks prior to screening; concomitant therapy for more than 3 days with drugs, which might influence hepatic biotransformation (CYP3A inducers/inhibitors); installation of dietary restrictions within 4 weeks prior to screening or during treatment; intake of grapefruit-containing food or beverages during the study treatment phase; known intolerance/hypersensitivity to study drug; lack of patient's cooperation; existing or intended pregnancy or breast feeding; and positive pregnancy test at screening in women with childbearing potential.
Allocation and conduct of treatment
Following a 5-week screening phase, at baseline eligible patients were allocated to treatment by a computer-generated list of random numbers, using randomly permuted blocks with a block size of 4, which was generated and held by staff at the Contract Research Organisation who were not involved in the planning, conduct or analysis of the study. Patients were centrally randomised in a 1:1:1:1 ratio via an Interactive Web Response System, to receive treatment with either 2x1 mg/day (BET1) or 2x2 mg/day (BET2) or oral BVS 2×5 mL (0.4 mg/mL)/day or placebo, for 14 days. In order to maintain the study blinding when using different pharmaceutical preparations, a double-dummy design was used. Therefore, both formulations, that is, BETs (containing budesonide or placebo) as well as oral BVS (containing budesonide or placebo) were taken by all patients in divided doses twice daily. Depending on the treatment group, either the BET or the oral BVS contained budesonide or placebo, respectively. Patients received the study medication marked with their randomisation number, sufficient for the entire treatment period of 2 weeks, at the baseline visit. Patients were instructed to administer the study drugs after a meal. First, the tablet was to be placed on the tip of the tongue and pressed gently against the hard palate until it had completely disintegrated by contact with saliva. The components dissolved in saliva were then to be swallowed (5–10 swallows within 90–120 s). At least 15 min after ingestion of the tablet, 5 mL of the viscous suspension were swallowed. Patients were further instructed to avoid eating, drinking or oral hygiene procedures for 30 min after study drug administration. Compliance was assessed using patient's diary cards which recorded time of breakfast and evening meal, time of study drug administration and time of oral hygiene on a daily basis. Furthermore, compliance was recorded by counting (blister and tablets) or weighing (bottles) the trial medication returned at the end of treatment (EoT)/withdrawal visit.
Endoscopy
Upper endoscopy was performed at screening and at EoT by the same board-certified gastroenterologist, using conscious sedation with either propofol or midazolam under the decision and responsibility of the physician. The following endoscopic abnormalities were recorded and classified as either absent (0), mild (1), moderate (2) or severe (3): white exudates, furrows, oedema, fixed rings, crepe paper sign, short-segment stenosis, long-distance stenosis. Thus, the total endoscopic intensity score ranged from 0 to 21. In addition, a global assessment of endoscopic appearance was determined using a 100 mm visual analogue scale (VAS).
During both endoscopies, two biopsies each from the distal, mid and proximal oesophagus were obtained, preferably from visible lesions. In addition, two biopsies each from the antrum, corpus and duodenum were obtained during screening endoscopy, unless this had already been done during a previous upper endoscopy within 12 months prior to screening. The biopsies were immediately placed into separate tubes with neutral-pH-buffered 4% paraformaldehyde solution and sent to the primary central pathologist (MV for Germany and Belgium, CB for Switzerland).
Histology
The processing and analysis of the biopsy samples were performed according to a standard operation procedure, to which both pathologists and their team members consented and adhered. From the paraffin-embedded oesophageal biopsies 10 sections were cut for H&E staining, an additional five sections for Van Gieson and five sections for alcian blue (AB) periodic acid-Schiff (PAS). Gastric biopsies were stained with H&E, alcian blue and periodic acid Schiff (ABPAS) and either Warthin Starry stain or Hp-Giemsa stain, and duodenal biopsies with H&E and ABPAS stain.
On each oesophageal biopsy specimen, all levels were surveyed and the eosinophils in the most densely infiltrated area were counted in 5 hpfs and the numbers entered into an electronic database. Biopsies from Switzerland were assessed by CB using a Zeiss-Axio Imager A1 microscope with Carl Zeiss Pl 10×/23 ocular (field number: 23) and a Zeiss EC Plan-Neofluar 40× objective, resulting in an area of microscopic field of 0.260 mm2. MV assessed the biopsies from Germany and Belgium using an Olympus AX70 microscope with Olympus SWH 10×-H/26.5 ocular (field number: 26.5) and PLANAPO 40× objective, resulting in an area of microscopic field of 0.345 mm2. For standardisation within the study, and since we based our sample size calculation on the histological remission rates reported by Straumann et al,16 we back-calculated the cut-off value of <5 eos/hpf for histological remission based on the reported microscopic field of 0.307 mm2 in the study by Straumann et al,16 which corresponds to <16 eos/mm2 hpf. The mean and maximum number of eos/hpf and eos/mm2 hpf derived from each biopsy as well as from all biopsies were automatically calculated and immediately communicated to the investigator.
In patients with suspected local fungal infection, Grocott silver staining was performed in oesophageal biopsy specimen taken at the screening and the EoT/withdrawal visits (post hoc analysis).
Symptom evaluation
Dysphagia symptoms were assessed at screening, baseline, EoT and 2 weeks thereafter using a non-validated dysphagia score, which has however been used in a previous randomised placebo-controlled trial of oral viscous budesonide in adult patients with EoE.16 Briefly, the score assessed frequency of dysphagia ranging from none (0) to several times per day (4) and intensity of dysphagia ranging from unhindered swallowing (0) to long-lasting complete obstruction requiring endoscopic intervention (5). Thus, total scores ranged from 0 to 9. A clinical response was defined as a decrease in the dysphagia score of at least 3 points compared with baseline.
Safety, tolerability and preference for study drugs
Adverse events and laboratory tests were recorded throughout the whole study. Serum morning cortisol (08:00–10:00), reflecting systemic steroid load, was measured by direct chemiluminescence (ADVIA Centaur, Siemens Healthcare Diagnostics, Tarrytown, New York, USA). Tolerability was classified as very good, good, satisfactory or poor by the patient and the investigator independently at the EoT.
The patient's acceptance of study drugs was assessed by questions focusing on the handling, taste and the time necessary for administration. The patient's preference of study drugs was determined by asking which formulation would be favoured if long-term treatment was initiated.
Clinicopathological outcome measures
The primary efficacy end point was the rate of histological remission (mean of <16 eos/mm2 hpf) at EoT. The co-primary efficacy end point was change in the mean numbers of eos/mm2 hpf (eosinophil load) from baseline to EoT. Secondary end points included the endoscopic abnormality score,14 ,16 total endoscopic intensity score and its subscores, endoscopic VAS score, dysphagia score, patient's acceptance and preference of study drugs, adverse events, morning serum cortisol, and assessment of tolerability by investigator and patient.
Statistical analyses, sample size calculation
The primary efficacy variable was subjected to a confirmatory statistical analysis (α=0.025, one-sided testing) in the context of an adaptive two-stage group sequential design with a one-sided significance level of 2.5% for each step. The normal approximation test for the comparison of rates was used for the primary end point. The co-primary end point was only subjected to a confirmatory analysis if the primary efficacy variable showed statistically significant results for all three budesonide groups versus placebo. In this case the Mann-Whitney test was used. The primary and co-primary efficacy variables were evaluated by intention-to-treat and per-protocol analysis. Evaluations of secondary efficacy and safety variables were performed in an exploratory sense.
Based on the histological remission rates of the study by Straumann et al,16 the initial sample size calculation with a Bonferroni adjusted α=0.025/3 yielded that 15.3 evaluable patients per treatment group were needed to achieve 80% power. Based on the statistical analysis plan, a sample size of 15+10 evaluable patients per group were considered justified by ensuring a power of more than 80%. An interim analysis by an Independent Data Monitoring Committee was planned after observation of 60 patients, and the final analysis was planned after observation of an additional 40 patients evaluable for the full set analysis set. The statistical analyses were performed using the software package SAS V.9.3 or higher (SAS Institute, Cary, North Carolina 27513, USA). Results reported in the context of the adaptive design were calculated using ADDPLAN V.6.0.4 (Addplan GmbH, Cologne, Germany).
Results
Patient disposition and baseline characteristics
In total, 109 patients were screened for the study (see online supplementary figure S1) and 77 patients were randomised (first-patient-in June 2011, last-patient-completed April 2013). One randomised subject did not take at least one dose of study medication and was excluded from all analysis sets. Based on the results of the interim analysis of 61 observed patients (16 patients in the BET2 group and 15 patients each of the other three treatment groups) which revealed significant differences in the primary and co-primary end point for all three budesonide groups versus placebo, the Independent Data Monitoring Committee recommended termination of the study. Recruitment was stopped after the results of the interim analysis became available. Since recruitment continued during the interim analysis, 16 patients were still in the study resulting in a total of 76 evaluable patients for the final analysis set (19 patients per treatment group).
The demographic characteristics of the 76 study patients are summarised in table 1. Age, gender and other demographic variables were typical for an adult patient population with EoE. About two-thirds of patients had an established EoE diagnosis at study entry. The mean duration since EoE diagnosis was 2.2 years. The mean duration of oesophageal symptoms was 8.5 years. About a third of the patients had a history of steroid exposure, while 13% of patients had a history of endoscopic dilatation. There were no statistically significant differences in the baseline characteristics between the four treatment groups.
Demographic characteristics at baseline
Table 2 summarises the histological variables and the scores for endoscopic abnormalities and dysphagia at baseline. Overall, the total mean peak number of eos/mm2 hpf was 263 with a total mean of 126 eos/mm2 hpf (eosinophilic load). The eosinophilic inflammation was evenly distributed throughout the oesophagus in all four treatment groups. The mean total endoscopic intensity score was 6.4 and the mean dysphagia score was 4.6. There were no statistical significant differences between the four treatment groups with regards to eosinophilic counts, the total endoscopic intensity scores and their subscores (data not shown), and the dysphagia scores.
Histological and clinical characteristics at baseline
Effect of treatment on histology
The final analysis set revealed histological remission (mean <16 eos/mm2 hpf) for nearly all patients in the budesonide groups, while no histological remission was observed in the placebo group (0/19). The corresponding remission rates by intention-to-treat and per-protocol analysis are shown in figure 1. The rates of histological remission were not significantly influenced by the presence or absence of concomitant allergic diseases, concomitant PPI use or disease duration (data not shown).

Histological remission (mean <16 eos/mm2 hpf). BET1, effervescent tablets for orodispersible use 2×1 mg/day; BET2, effervescent tablets for orodispersible use 2×2 mg/day ; BVS, budesonide viscous suspension 2×5 mL (0.4 mg/mL)/day; ITT, intent-to-treat; PLA, placebo; PP, per protocol.
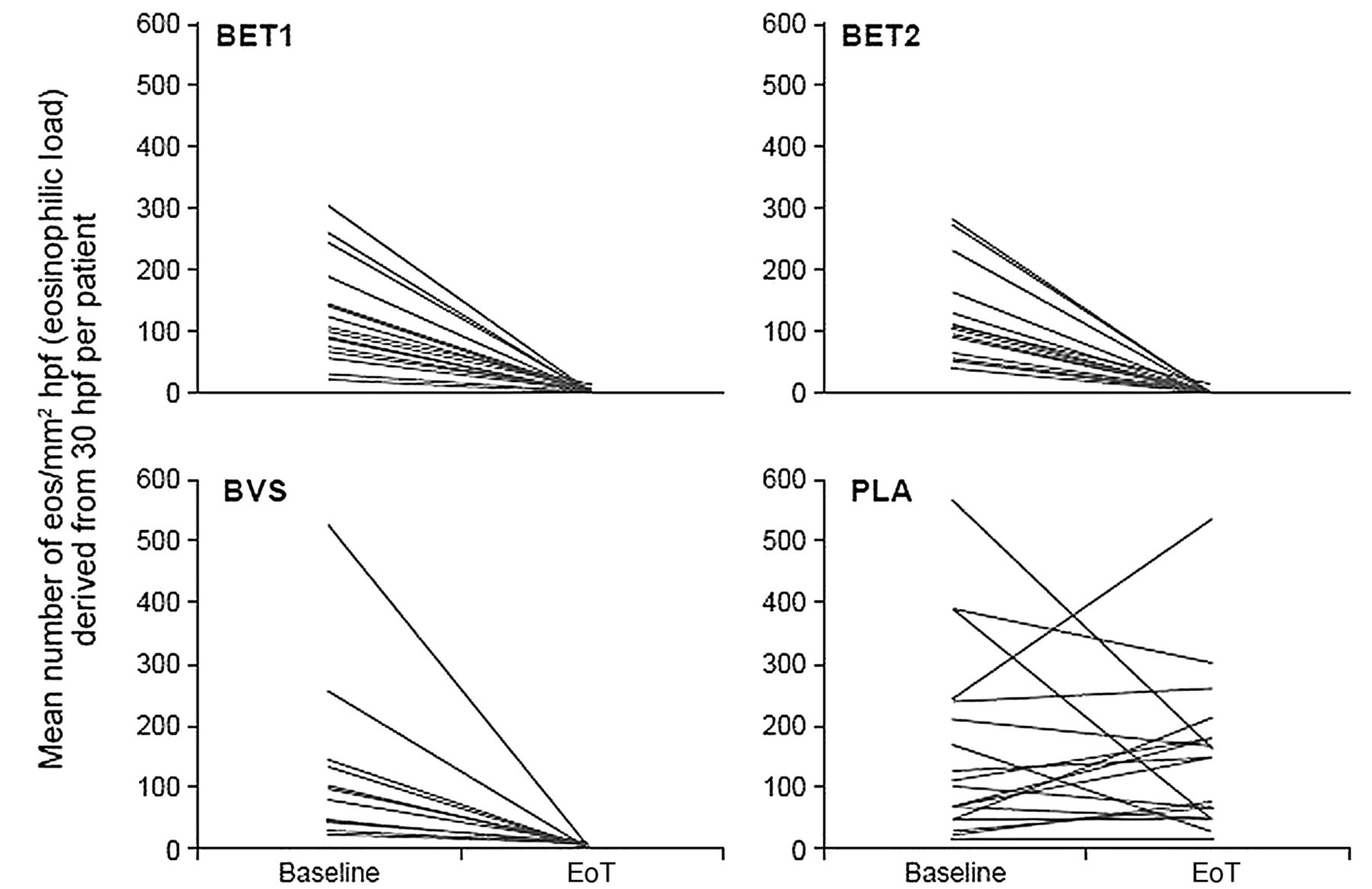
The co-primary end point, that is, the change from baseline to end-of-treatment in the mean number of eos/mm2 hpf (eosinophilic load), also showed superiority for all budesonide groups versus placebo (BET1: p=0.0003; BET2: p=0.0003; BVS: p=0.0020). In all three budesonide groups a relevant decrease was observed (BET1: −120, BET2: −128, BVS: −97) while no relevant change (−8) was observed in the placebo group (figure 2). In the three budesonide groups, the eosinophilic load decreased significantly in all oesophageal segments in a similar fashion (figure 3).
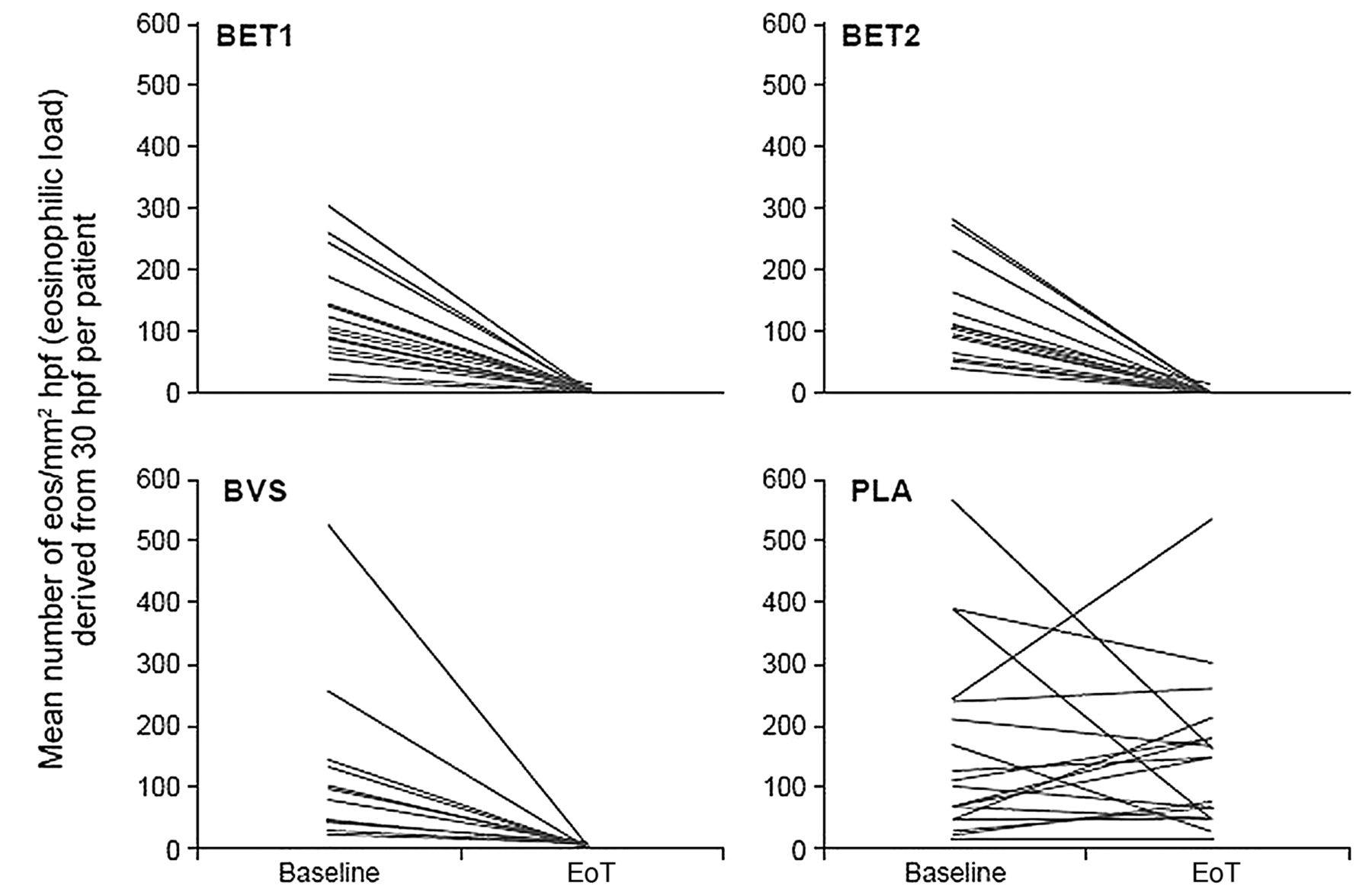
Effect of treatment on eosinophilic load. BET1, effervescent tablets for orodispersible use 2×1 mg/day; BET2, effervescent tablets for orodispersible use 2×2 mg; BVS, budesonide viscous suspension 2×5 mL (0.4 mg/mL)/day; EoT, end of treatment; PLA, placebo.

Effect of treatment on eosinophilic load by oesophageal segment. BET1, effervescent tablets for orodispersible use 2×1 mg/day; BET2, effervescent tablets for orodispersible use 2×2 mg/day ; BVS, budesonide viscous suspension 2×5 mL (0.4 mg/mL)/day; EoT, end of treatment; PLA, placebo.
Additionally, the mean peak number of eos/mm2 hpf decreased significantly from baseline to end-of-treatment in all three budesonide groups (BET1: −227, p=0.0006; BET2: −287, p=0.0002; BVS: −180, p=0.0037) while no significant decrease was observed in the placebo group (−30). The corresponding histological remission rates, defined as peak of <16 eos/mm2 hpf, were 84.2%, 89.5%, 73.7% and 0%, respectively. A histological response, defined as a mean of <65 eos/mm2 hpf, was observed in nearly all patients treated with budesonide (BET1: 19/19, BET2: 18/19, BVS: 18/19) and in 6 of 19 placebo recipients (31.6%).
Effect of treatment on endoscopic abnormalities
The mean change from baseline to EoT in the total endoscopic intensity score was significantly superior in all three budesonide groups compared with the placebo group, that only showed a decrease of 0.7 points (BET1: −4.1, p=0.0001; BET2: −3.4, p=0.0011; BVS: −3.6, p=0.0017) (figure 4). The proportions of patients with improvement of the endoscopic abnormality score were higher in the budesonide groups (BET1: 73.7%, BET2: 57.9%, BVS: 57.9%) compared with the placebo group (26.3%). Accordingly, the mean endoscopic VAS score improved in all budesonide groups (BET1: −37.4, BET2: −31.7, BVS: −25.2) and changed only slightly in the placebo group (−9.6).
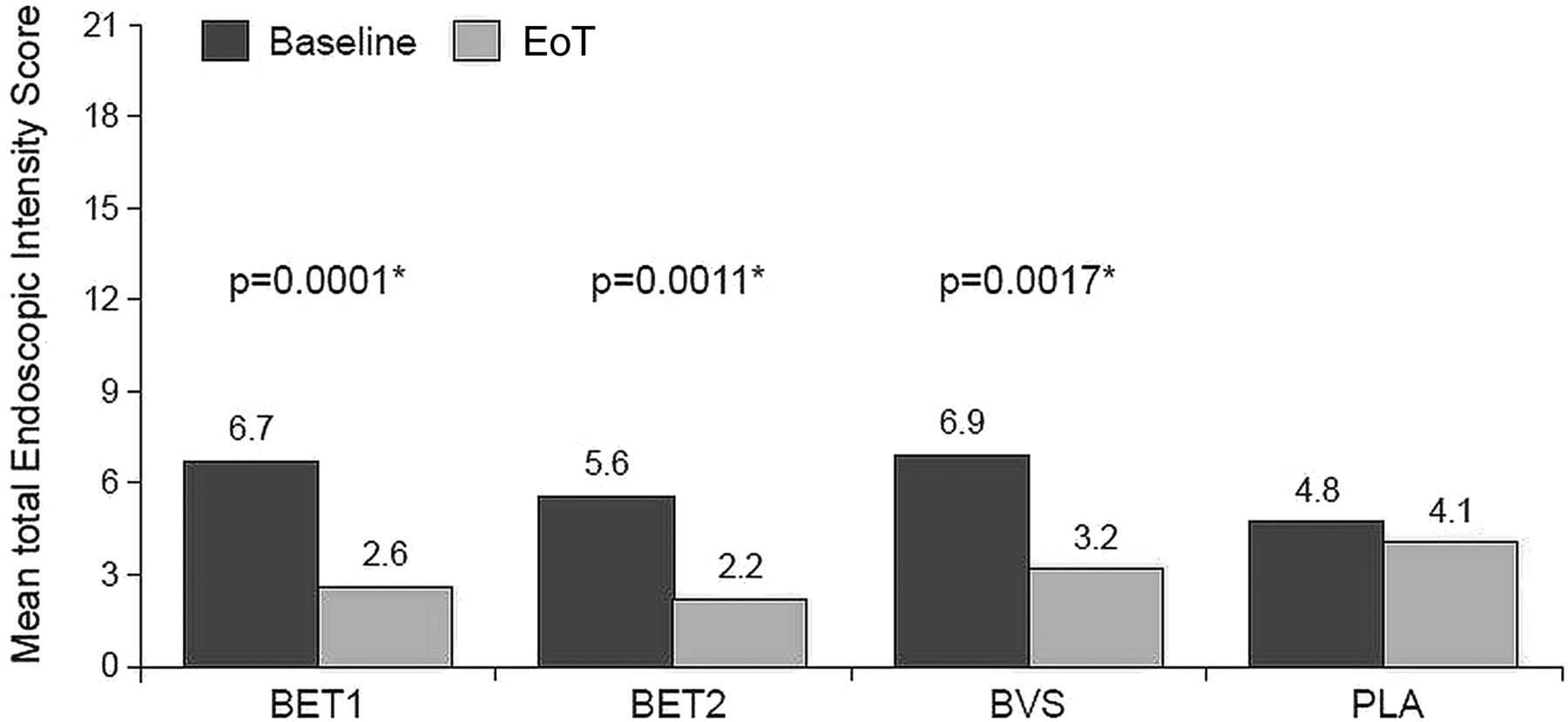
Total endoscopic intensity score (* vs change in placebo). BET1, effervescent tablets for orodispersible use 2×1 mg/day; BET2, effervescent tablets for orodispersible use 2×2 mg/day; BVS, budesonide viscous suspension 2×5 mL (0.4 mg/mL)/day; EoT, end of treatment; PLA, placebo.
The endoscopic intensity scores for exudates and furrows decreased significantly versus placebo in all three budesonide groups (figure 5). Improvement of oedema was observed in all three budesonide groups, but statistical significance versus placebo was reached only in BET1 and BVS recipients. A significant improvement versus placebo for fixed rings was only observed in the BET2 group, while the other budesonide groups showed a numerical but not statistical superiority over placebo. In the placebo group, none of the endoscopic intensity scores changed significantly. Other endoscopic abnormalities, such as crepe paper sign and short-segment or long-distance stenoses, were infrequent in all four groups and did not show any statistically significant changes after treatment (data not shown).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Endoscopic intensity scores for white exudates (A), furrows (B), oedema (C) and fixed rings (D) (* vs change in placebo). BET1, effervescent tablets for orodispersible use 2×1 mg/day; BET2, effervescent tablets for orodispersible use 2×2 mg/day ; BVS, budesonide viscous suspension 2×5 mL (0.4 mg/mL)/day; EoT, end of treatment; PLA, placebo.
Effect of treatment on symptoms
The mean dysphagia score, which was used as a primary metric of symptom response, decreased significantly from baseline to EoT in all four treatment groups (BET1: –2.7, p=0.0001; BET2: –1.8, p=0.0004; BVS: −2.4, p=0.0001; placebo: −2.0, p=0.0001) without statistically significant differences between the groups (see online supplementary figure S2).
However, sustained improvement 2 weeks after EoT was only observed in patients who were treated with budesonide. This was statistically significantly superior versus placebo only in the BET1 group (p=0.0196 vs placebo).
Safety, tolerability and patient's preference for study drug
There were no serious adverse events. The proportions of patients with suspected treatment-emergent adverse drug reactions were higher in the three active treatment groups (BET1: 4/19; BET2: 5/19; BVS: 6/19) than in the placebo group (0/19) (for details see online supplementary table S1). One patient prematurely stopped administration of the budesonide suspension due to lip oedema, which resolved completely 2 days after drug withdrawal without any need of medical intervention. The most frequent suspected adverse drug reactions were local fungal infections, confirmed by positive Grocott stain in two patients in each budesonide group (10.5%). There were no statistically significant changes in serum morning cortisol levels (screening vs EoT) in any of the treatment groups (see online supplementary figure S3). A decrease in serum morning cortisol from normal at screening to a value below the lower limit of normal (4.3 µg/dL) was recorded only in one patient on 4 mg budesonide per day (BET2).
Tolerability and acceptance of the budesonide formulations were high among patients. Eighty per cent of patients preferred the BET, while 17% preferred the BVS.
Discussion
EoE is a chronic disease requiring anti-inflammatory treatment. Oral topical corticosteroids have been proven efficacious in children and adults and are therefore considered to be first-line medical treatment in patients with active EoE.
This multicentre, randomised controlled trial is the first study examining efficacy and safety of two different formulations of budesonide which target the oesophagus—BET and BVS—for treatment of adult EoE. Furthermore, this is to date the largest trial, including 76 patients in total, and compares two different dosages of the drug. The results of this study clearly demonstrate that short-term treatment with budesonide administered either as BET or as BVS has a profound anti-inflammatory effect throughout the entire oesophagus and, additionally, significantly improves endoscopic abnormalities.
Up to now, the traditional primary end point in EoE trials has been the degree of eosinophilic inflammation of the oesophagus. In this trial we have adopted this concept and have also used the histological response as the primary end point, despite the knowledge that symptoms have to be respected as the key end point. We have used the mean number of eosinophils per mm2 hpf as the key metric for the primary and co-primary end points, calculated from a large number of histological slides obtained from biopsies from the entire oesophagus. We used this extensive assessment strategy to be as accurate as possible in determining the anti-inflammatory effects of treatment throughout the oesophagus. On the other hand, the histological remission rates based on the peak number of eos/mm2 hpf were quite similar in our study, suggesting that the more extensive determination of mean number of eosinophils per mm2 hpf might not be necessary in clinical routine practice.
Of note, comparisons between individual trials in EoE are hampered by differences in study designs, definitions of histological response, and even technical differences such as the area of high power fields among different microscopes. Nevertheless, the histological remission rates observed in our study confirm, or even seem to exceed, those from previous randomised controlled trials in adult and paediatric EoE which essentially studied swallowed nebulised corticosteroid formulations originally designed for pulmonary treatment.15–18 Interestingly, all patients in this trial who received budesonide effervescent tablet 1 mg twice daily achieved histological remission, and therefore no additional benefit could be shown for the higher dose of 2 mg twice daily. Similarly, all patients who completed treatment with the viscous suspension reached histological remission. This impressive effect could be explained by the higher dose of budesonide (2 mg twice daily) used in our study compared with previous studies examining viscous suspensions.16–18
So far, three randomised controlled trials of budesonide in EoE have been published. Major differences between these trials include mode of drug delivery, treatment duration and patient selection. In the study by Straumann et al,16 18 adult or adolescent patients with EoE were exposed to a viscous budesonide suspension at a dose of 2×1 mg per day given for 15 days. The patient population (including the number of patients with previous steroid exposure), the histological remission and response rates as well as the improvement in endoscopic abnormalities were comparable with our observations. Dohil et al17 reported on 15 paediatric patients exposed to viscous budesonide suspension for 3 months at a daily dose of 1 mg or 2 mg depending on the patient's body weight. Importantly, all patients received concomitant lansoprazole. In that trial, 13 patients (87.5%) were classified as responders based on the mean peak eosinophil count per hpf, which may not be the optimal histological metric to determine histological response. Nevertheless, the differences to placebo were striking. Finally, Dellon et al compared topical budesonide 2×1 mg per day delivered either as viscous suspension or in a nebulised form taken orally by 25 adult, steroid-naive patients with EoE for a duration of 8 weeks.18 This elegant study clearly demonstrated superiority of the viscous suspension over the nebulised application form with regards to the mucosal contact time of the drug as well as histological and endoscopic responses.
With respect to endoscopic abnormalities, we observed significant improvement in endoscopic signs of acute inflammation, that is, white exudates, furrows and oedema, in all three budesonide groups. Fixed rings, which are regarded as an endoscopic sign of long-standing EoE, improved numerically in all three budesonide groups, but statistical significance versus placebo was only observed in the high-dose effervescent tablet group. Overall, the endoscopic response to budesonide treatment was very similar between our trial and previous trials in adult patients with EoE.16 ,18
The evaluation of dysphagia in EoE remains a challenge as long as validated scores are lacking. Poor correlation between severity of symptoms and histological activity is a well-recognised problem and has been described in various EoE trials.18 ,21–24 In our study we used the same dysphagia score that was used in the study by Straumann et al16 and observed significant improvement of dysphagia at the EoT in all four groups, including the placebo group. The reasons for the significant symptom response in the placebo group remain obscure, but illustrate that in EoE meaningful readouts should include biological markers as well as patient-reported outcomes.25 However, the endoscopic score for fixed rings at baseline was somewhat lower in the placebo group compared with the active budesonide group, which could have influenced at least the symptom response to placebo. Of note, sustained improvement of dysphagia 2 weeks after termination of treatment was only observed in patients exposed to budesonide, indicating a symptomatic benefit for active treatment over placebo, and suggesting that treatment with topical steroids for longer than 2 weeks may be necessary to differentiate the effects of budesonide and placebo on symptom relief.
In our study, short-term topical treatment with two new budesonide formulations was safe up to a daily dose of 4 mg budesonide. The very low frequency of systemic side effects, including adrenal suppression, is clearly the pharmacodynamic result of the favourable pharmacokinetic profile of the study drugs. Previously, it has been shown that only about 9% of budesonide from the effervescent tablet reaches the systemic circulation in patients with active EoE.20 In contrast, oesophageal fungal infection (hyphae) occurred in some patients receiving budesonide. It is noteworthy that not all macroscopically suspected fungal infections were confirmed by the Grocott staining. White exudates in EoE might be taken as fungal plaque and vice versa. Therefore, it is prudent to examine patients with EoE carefully by histopathology. The frequency of oesophageal fungal infection in our study was similar to those frequencies reported in previous EoE trials of topical steroids.16 ,18 ,24
Our study may have a potential limitation because we did not incorporate the definition which is currently proposed for exclusion of PPI-responsive oesophageal eosinophilia (PPI-REE), that is, PPI administered twice daily for 8 weeks. At the time of planning the study, the PPI-REE issue had just been addressed and summarised in the consensus guideline by Liacouras et al1 However, at that point it remained entirely unclear whether PPI-REE represents a distinct disease entity that differs from classic EoE, or is just a subphenotype of EoE. Moreover, no valid criteria with regards to the type, dose and duration of PPI treatment were available; indeed, randomised placebo-controlled trials of PPI in EoE are still lacking and PPI therapies are not formally approved for the treatment of EoE. Finally, recent studies have shown EoE and PPI-REE to be indistinguishable based on clinical, endoscopic, histological and biochemical assessments.26 ,27 Very recently, extensive transcriptome analyses have demonstrated a significant molecular overlap between PPI-REE and EoE, suggesting that PPI-REE is likely to represent a continuum of the same pathogenic allergic mechanisms that underlie EoE and thus may constitute a subphenotype of EoE.28
Another limitation of our study may be that it focuses exclusively on the induction of remission of an active eosinophilic inflammation. It does not address the issue that EoE is a chronic inflammatory disease which untreated may show a progressive course resulting in fibrosis and consequently stricture formation. It therefore requires a long-term therapeutic strategy. However, the problem of finding an efficient and safe long-term medical therapy is still unsolved. First studies indicate that long-term treatment with low-dose budesonide may be efficient in maintaining a long-term remission and in preventing bolus obstructions.29 ,30 Based on the promising results of the present study, further prospective studies are warranted in order to define the optimal schedules for long-term treatment in paediatric and adult patients with EoE.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figures
- Data supplement 2 - Online table
Footnotes
SM and PH contributed equally.
Correction notice This article has been corrected since it published Online First. The sixth author's name has been corrected to Monther Bajbouj.
Contributors SM and PH: development of the study protocol, patient recruitment, data analysis and interpretation, manuscript preparation; MV and CB: development of the study protocol, and central pathologists; AM: development of the study protocol, patient recruitment; UvA, MB, CS, CF, HW, HDA, MR, SS, JT, MM, PK, and JA: patient recruitment; RM and RG: development of the study protocol, data analysis and interpretation, support for manuscript preparation; KD: drug safety, data analysis and interpretation, support for manuscript preparation; AS: development of the study protocol, patient recruitment, data analysis and interpretation, support for manuscript preparation. All authors had access to the study data and reviewed and approved the final manuscript.
Funding The study was sponsored by Dr Falk Pharma GmbH, Freiburg, Germany. Caroline Dunstall provided proofreading and editorial support with funding from Dr Falk Pharma GmbH.
Competing interests SM has received speaker's honoraria from Dr Falk Pharma GmbH. MV, MB, AM, HW, HDA and MR have received speaker's honoraria from the Falk Foundation. SS has received speaker's honoraria from Abbvie, the Falk Foundation and MSD. RM, KD and RG are employees of Dr Falk Pharma GmbH. AS is a consultant to Dr Falk Pharma GmbH and has received consulting fees and/or speaker fees and/or research grants from Actelion, AG, Switzerland, AstraZeneca, AG, Switzerland, Aptalis Pharma, Glaxo SmithKline, AG, Nestlé S. A., Switzerland, Novartis, AG, Switzerland, Pfizer, AG, and Regeneron Pharmaceuticals.
Patient consent Obtained.
Ethics approval The study was conducted in accordance with the International Conference on Harmonisation (ICH) Guideline for Good Clinical Practice and was approved by the Ethics Committee of the Physician's Chamber Hamburg, Germany, as well as by the national ethics committees in the participating countries.
Provenance and peer review Not commissioned; externally peer reviewed.