Article Text

Abstract
Objective The global burden of colorectal cancer (CRC) is expected to increase by 60% to more than 2.2 million new cases and 1.1 million deaths by 2030. In this study, we aim to describe the recent CRC incidence and mortality patterns and trends linking the findings to the prospects of reducing the burden through cancer prevention and care.
Design Estimates of sex-specific CRC incidence and mortality rates in 2012 were extracted from the GLOBOCAN database. Temporal patterns were assessed for 37 countries using data from Cancer Incidence in Five Continents (CI5) volumes I–X and the WHO mortality database. Trends were assessed via the annual percentage change using joinpoint regression and discussed in relation to human development levels.
Results CRC incidence and mortality rates vary up to 10-fold worldwide, with distinct gradients across human development levels, pointing towards widening disparities and an increasing burden in countries in transition. Generally, CRC incidence and mortality rates are still rising rapidly in many low-income and middle-income countries; stabilising or decreasing trends tend to be seen in highly developed countries where rates remain among the highest in the world.
Conclusions Patterns and trends in CRC incidence and mortality correlate with present human development levels and their incremental changes might reflect the adoption of more western lifestyles. Targeted resource-dependent interventions, including primary prevention in low-income, supplemented with early detection in high-income settings, are needed to reduce the number of patients with CRC in future decades.
- COLORECTAL CANCER
- EPIDEMIOLOGY
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Colorectal cancer (CRC) is the third most commonly diagnosed malignancy and the fourth leading cause of cancer-related deaths in the world, and its burden is expected to increase by 60% to more than 2.2 million new cases and 1.1 million cancer deaths by 2030.
CRC is considered one of the clearest markers of the cancer transition, whereby countries undergoing rapid societal and economic changes show rapid increases in cancers already more frequent in high-income countries.
Understanding the current patterns of CRC and its evolution from an international perspective is imperative in order to direct future prospects of reducing the burden through cancer prevention and cancer care.
What are the new findings?
CRC incidence and mortality rates vary widely worldwide, with distinct gradients across human development levels and trends point towards widening disparities and an increasing burden in countries in transition.
We identified three patterns of CRC incidence and mortality trends and ascertained that CRC incidence and mortality rates are still rising rapidly in many low-income and middle-income countries, linked to ongoing societal and economic development; stabilising or decreasing trends tend to be seen only in highly developed countries where rates remain among the highest in the world.
How might it impact on clinical practice in the foreseeable future?
Without targeted resource-dependent actions based on this evidence, the number of patients with CRC will continue to increase in future decades.
Improvements in treatment options and accessibility are vital, particularly in low-income and middle-income countries that face an increasing burden of CRC.
Prioritisation of primary prevention and early detection are necessary, alongside their integration into existing healthcare plans.
Introduction
Colorectal cancer (CRC) is the third most commonly diagnosed malignancy and the fourth leading cause of cancer death in the world, accounting for about 1.4 million new cases and almost 700 000 deaths in 2012.1 The distribution of CRC burden varies widely, with more than two-thirds of all cases and about 60% of all deaths occurring in countries with a high or very high human development index (HDI).1 CRC is considered one of the clearest markers of the cancer transition, replacing infection-related cancers in countries undergoing rapid societal and economic changes together with other cancers predominantly linked to western lifestyles, which are already frequently found in high-income countries.2–4
Rapid increases in both CRC incidence and mortality are now observed in many medium-to-high HDI countries particularly in Eastern Europe, Asia and South America.2 In contrast, CRC incidence and mortality rates have been stabilising or declining in a number of the highest indexed HDI countries: the USA, Australia, New Zealand and several Western European countries.2 The reasons for the recent declining trends in incidence in these countries are ill-defined and likely numerous but may partially reflect increased early detection and prevention through polypectomy (at least in the USA). Together with the factors that have brought about declines in incidence, improvements in perioperative care, as well as chemotherapy and radiotherapy, will have contributed to the uniformly decreasing trends in CRC mortality in many high-income settings.5 ,6
Given the temporal profiles and demographic projections, the global burden of CRC is expected to increase by 60% to more than 2.2 million new cases and 1.1 million cancer deaths by 2030.1 Understanding the current patterns of CRC and its evolution from an international perspective is therefore imperative, and in this study, we describe the geographical variations in CRC incidence and mortality in 184 countries and time trends in 37 countries, linking the findings to the future prospects of reducing the burden through cancer prevention and care.
Methods
Incidence and mortality estimates of malignant neoplasms of the colon and rectum (ICD-10 C18-21) by country for 184 countries in 2012 were extracted from the GLOBOCAN database.1 Data on HDI for the same year were obtained from the United Nations Development Programme.7
To assess time trends in CRC incidence and mortality, we used data from two different sources with the requirement of at least 15 consecutive years of data, and the availability of both incidence and mortality data for each country included. For CRC incidence, data series from high-quality regional and national population-based cancer registries were extracted from the Cancer Incidence in Five Continents (CI5) series Volumes I–X,8 complemented with publically available data from European countries,9 ,10 ,11 Australia,12 New Zealand,13 and the USA14 for more recent years. Of the 37 countries studied, national incidence data were available for 25 countries. For the remaining countries, data from regional registries were pooled to obtain a proxy of the national incidence (see online supplementary annex table S1). National mortality data series were extracted from the WHO mortality database, with the minimal inclusion criteria set at the WHO-defined medium data quality level, ensuring a reasonable degree of population coverage, completeness and accuracy.15 Rates were age-standardised (ASR) to the world standard population.16
To analyse incidence and mortality trends, we used joinpoint regression,17 which involves fitting a series of joined straight lines to ASR trends. A logarithmic transformation of the rates, calculation of SEs using the binomial approximation, and a maximum number of three joinpoints were specified as options in the analysis. To estimate the magnitude and direction of recent trends, we calculated the average annual percentage change (AAPC) and the corresponding 95% CI for the last available 10 years. The AAPC is a geometrically weighted average of the different annual percentage changes from the joinpoint trend analysis, for which weights are equal to the length of each segment during the specified time interval.
Results
Incidence and mortality patterns of CRC in 2012
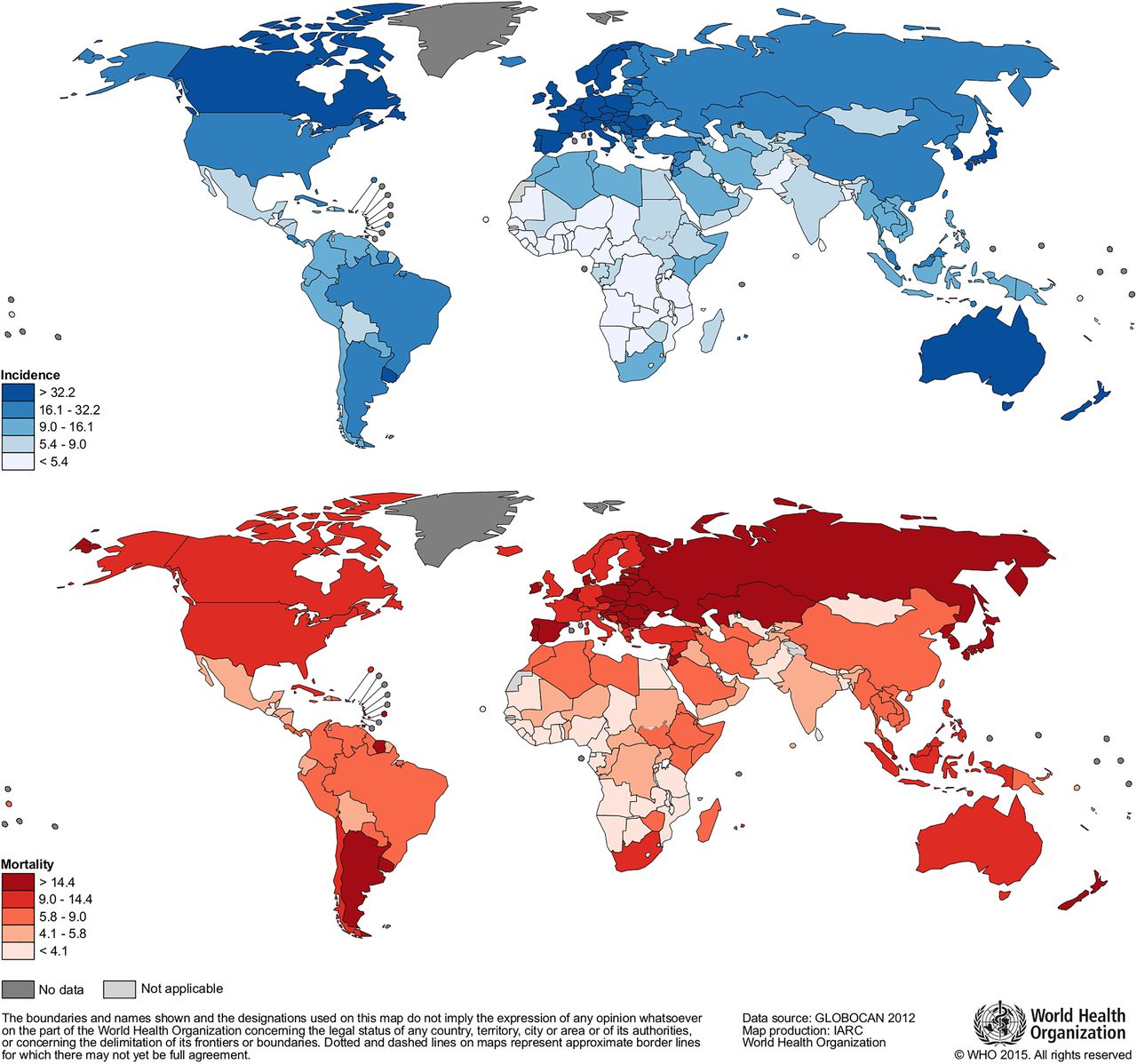
In 2012, the estimated incidence rates in males varied from <5 (per 100 000) in several African countries to over 40 in certain countries in Europe, Northern America and Oceania (figure 1). The highest rates in males were observed in Slovakia (61.6), Hungary (58.9) and the Republic of Korea (58.7), while the lowest were seen in sub-Saharan Africa, in The Gambia and Mozambique (both 1.5 per 100 000). Geographical patterns were very similar between the sexes, although rates in females tended to be lower (25% less) than their male counterparts (data not shown, see ref. 1). Gradients in incidence were observed with increasing levels of HDI: incidence rates in countries with a very high HDI were six times greater than countries with a low HDI (figure 2A). Geographical patterns of CRC mortality rates generally followed those of incidence, although the highest rates observed tended to be in countries with high rather than very high HDI in Central and Eastern Europe and Latin America (figure 1). As with incidence, mortality showed a distinct gradient across HDI levels (figure 2B), while comparisons of incidence-to-mortality revealed higher case fatalities among countries indexed with lower levels of HDI.

Worldwide colorectal cancer incidence and mortality rates (age adjusted according to the world standard population, per 100 000) in males in 2012 (GLOBOCAN 20121).

Correlation between age-standardised colorectal cancer incidence (left panel) and mortality rates (right panel) and human development index (HDI) in both sexes combined (GLOBOCAN 20121).
Trends in incidence and mortality from CRC
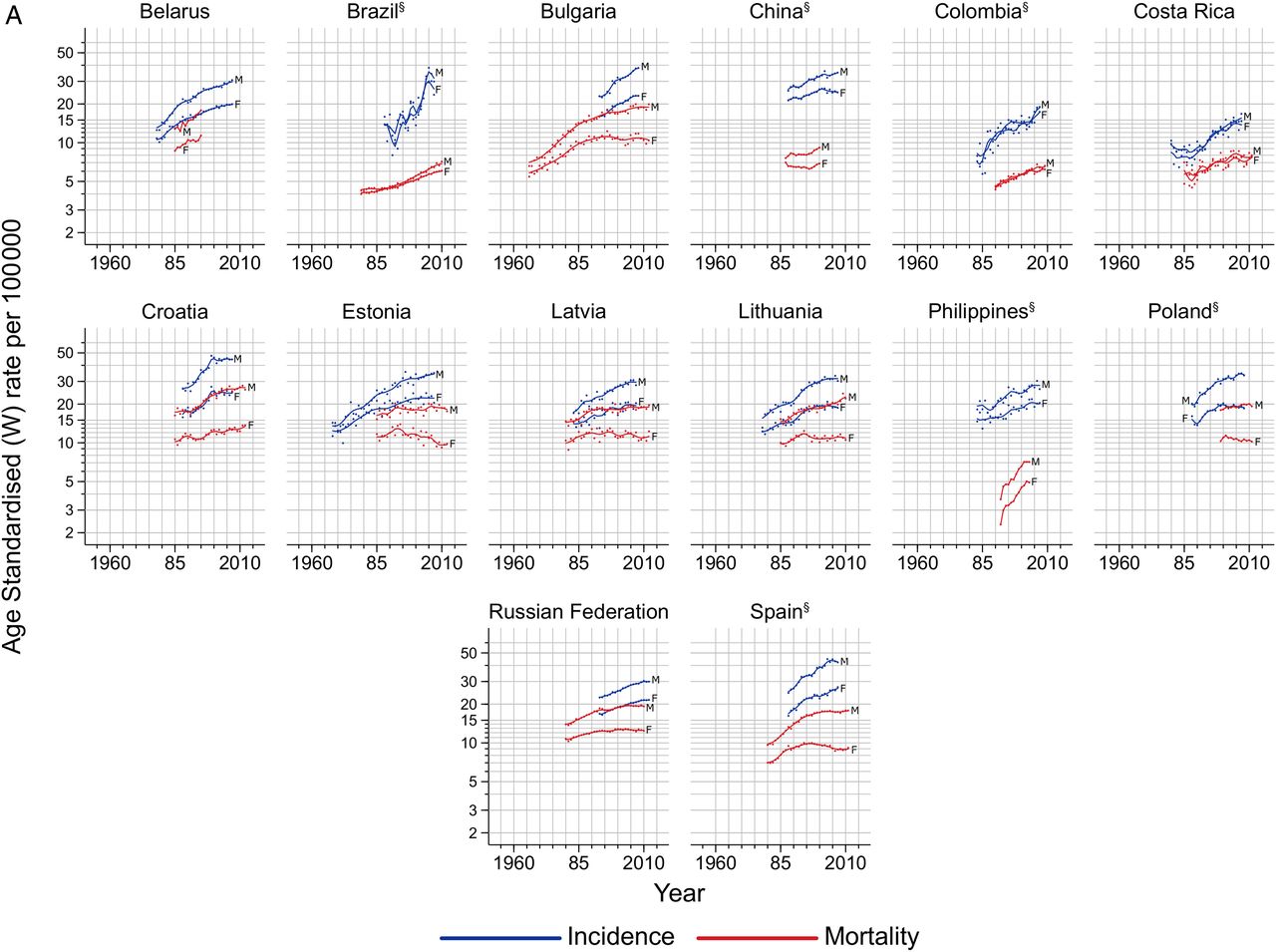
Based on temporal characteristics of incidence and mortality (in males), three different groups of countries were identified (table 1): those with increasing or stable incidence and mortality (group 1, n=14 countries), those with increasing incidence and decreasing mortality (group 2, n=14 countries) and those with decreasing incidence and mortality (group 3, n=9 countries). The results are presented according to these three categories.
Trends in colorectal cancer incidence and mortality: three groups of temporal pattern
Group 1: increasing incidence and mortality
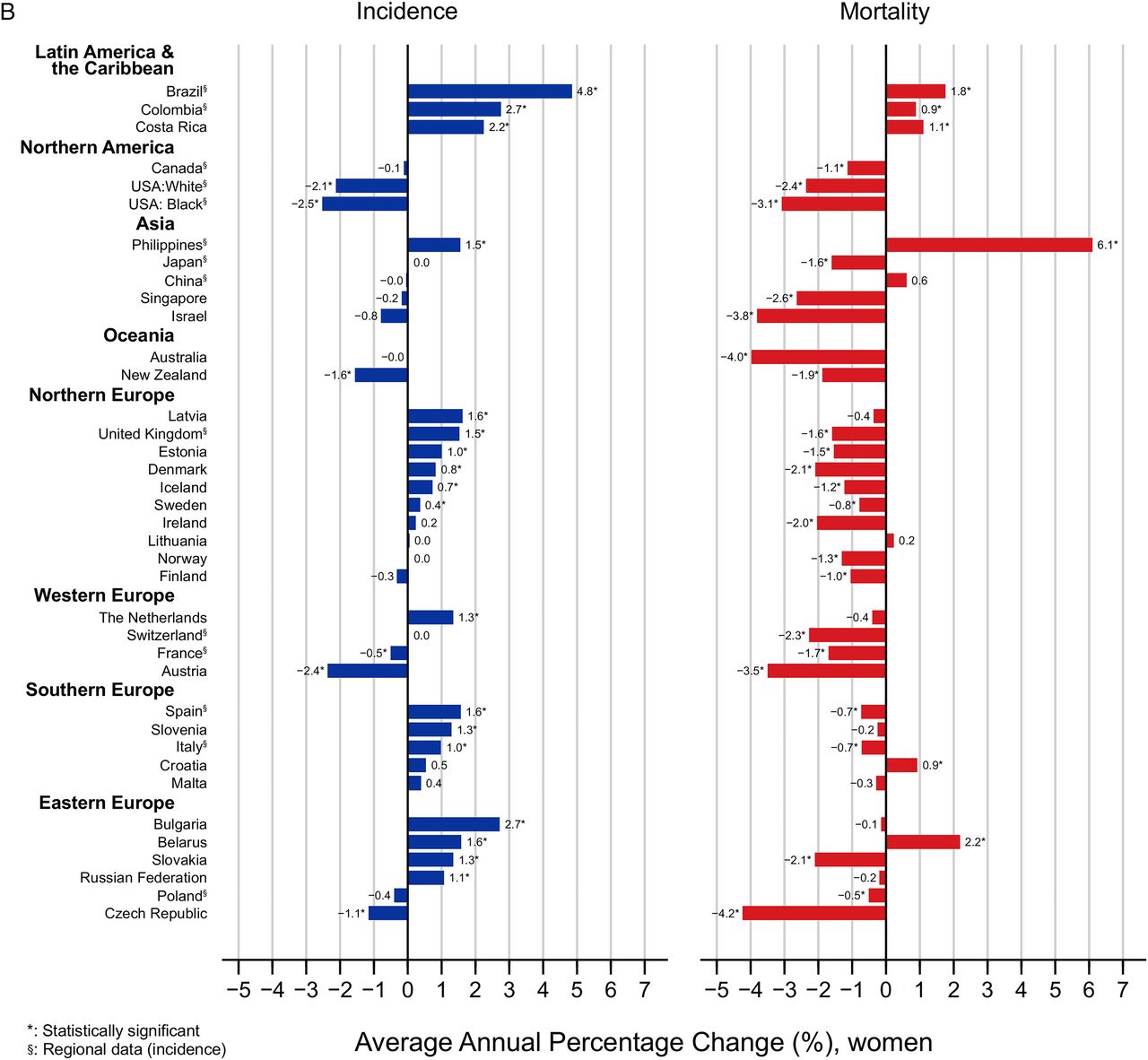
Increases in both incidence and mortality over the most recent 10-year period were seen in this group, comprising several Eastern European countries, and also in populations in Latin America and Asia (see figures 3A and 4A/B; online supplementary annex tables S2 and S3). In males, the largest increases in incidence were seen in Brazil (AAPC 7.2, 95% CI −7.5 to 24.2), Costa Rica (3.6, 95% CI 3.1 to 4.2) and Bulgaria (3.6, 95% CI 3.1 to 4.2), while mortality rates rose most rapidly in the Philippines (5.7, 95% CI 4.7 to 6.7) and Belarus (3.4, 95% CI 2.5 to 4.3). Incidence uniformly rose in all countries within this group, while mortality rates appeared to level off in Bulgaria, Russia, Croatia, Spain, Latvia and Estonia. Trends in females were similar to those in males, although both incidence and mortality were generally lower except in Latin American countries (Brazil, Costa Rica and Colombia), where rates in males and females were quite similar.
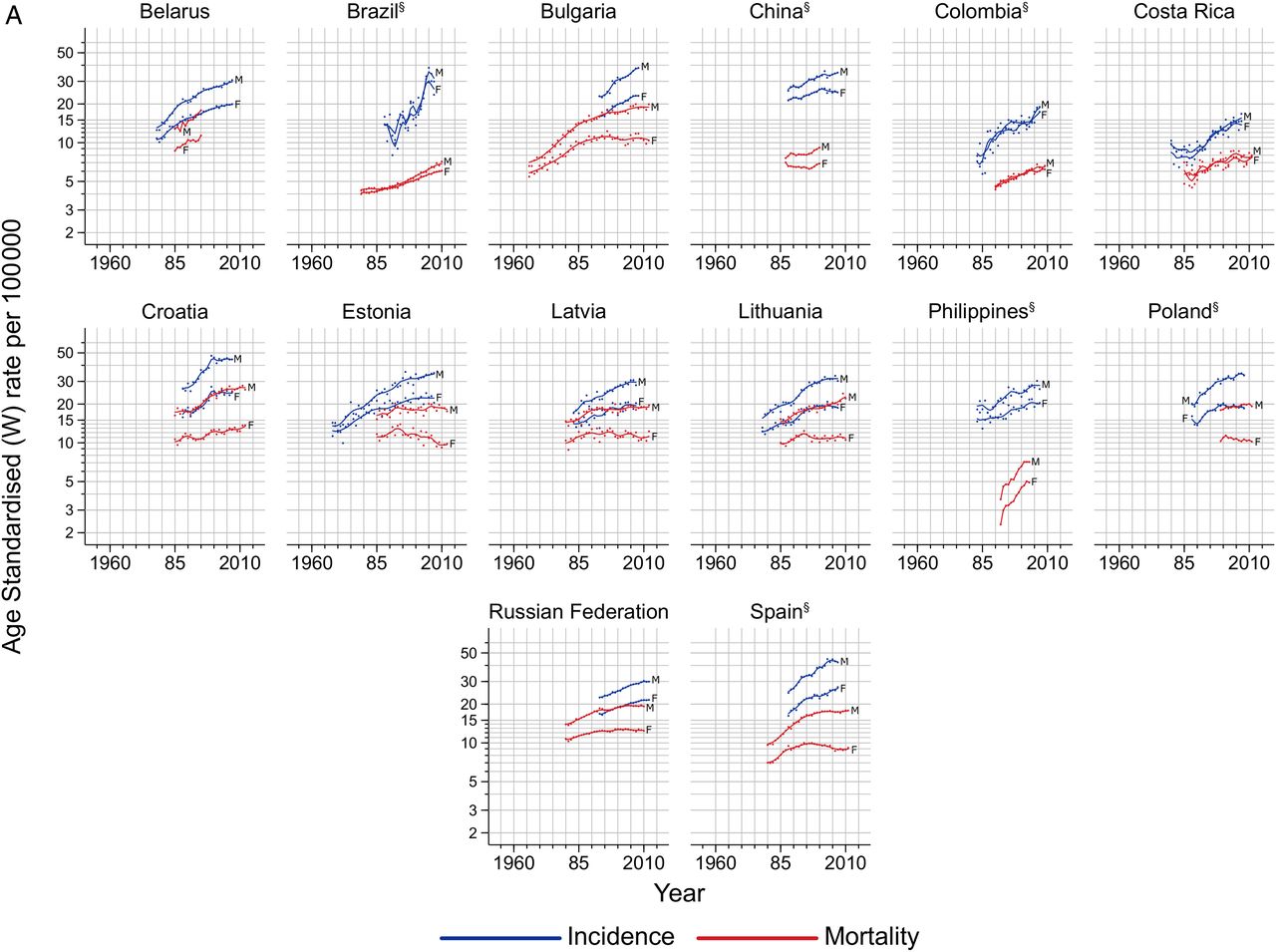
(A) Trends in colorectal cancer incidence and mortality in males (M) and females (F) by country (group 1: increasing or stable incidence and mortality). §Regional data. (B) Trends in colorectal cancer incidence and mortality in males (M) and females (F) by country (group 2: increasing incidence and decreasing mortality). §Regional data. (C) Trends in colorectal cancer incidence and mortality in males (M) and females (F) by country (group 3: decreasing incidence and mortality). §Regional data.

Continued

Continued

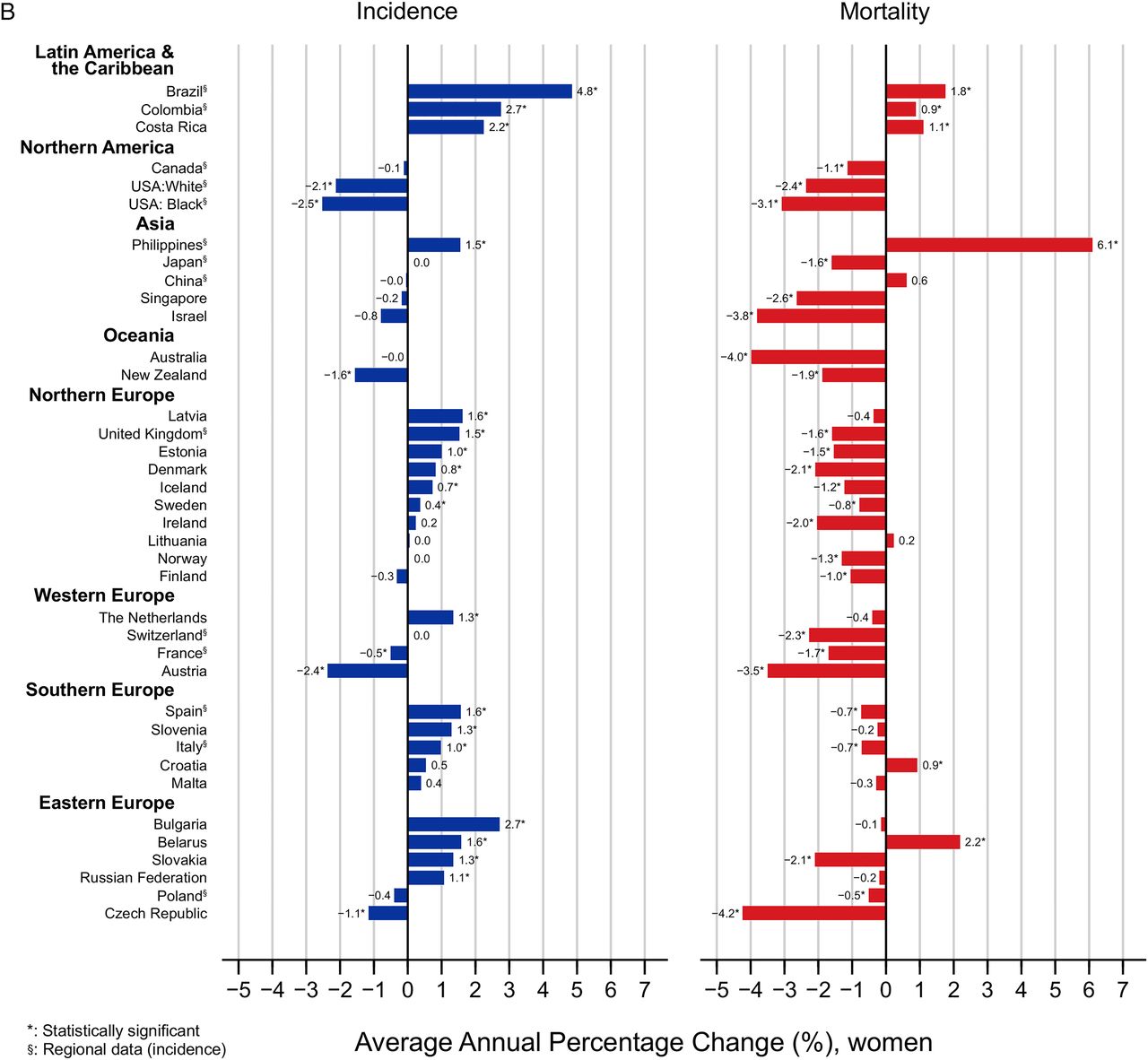
(A) Average annual percentage change (AAPC) of colorectal cancer incidence and mortality in the most recent period (10 years), males. (B) AAPC of colorectal cancer incidence and mortality in the most recent period (10 years), females.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Continued
Group 2: increasing incidence and decreasing mortality
In this group, incidence rates continued to increase while mortality rates decline, an observation seen in several European countries, and also in Canada and Singapore (see figures 3B and 4A/B; online supplementary annex tables S2 and S3). The rate of increase in incidence in males was marked in Southern European countries including Slovenia (2.7, 95% CI 0.5 to 5.0), Malta (1.7, 95% CI 0.5 to 2.9) and Italy (1.7, 95% CI 1.5 to 1.9), while stable or slight rises in trends were observed in Northern European countries and in Canada. Although mortality rates decreased most remarkably in Ireland (−2.1, 95% CI −2.9 to −1.3) and Denmark (−1.9, 95% CI −2.3 to −1.6), the corresponding incidence rates remained constant during the most recent 10-year period. As declining mortality rates were also observed in the UK (−2.0, 95% CI −2.2 to −1.8), these were, however, paralleled by a significant average increase of 1.3% per year in incidence. Trends were similar in both sexes.
Group 3: decreasing incidence and mortality
Decreases in both CRC incidence and mortality in this group were restricted to the highest HDI countries such as Australia, Iceland, New Zealand and Japan (see figures 3C and 4A/B; online supplementary annex tables S2 and S3). While the magnitude of declining incidence in males were marked among US Whites (AAPC −3.0, 95% CI −3.3 to −2.7) and Blacks (−2.2, 95% CI −3.3 to −1.0), mortality declines were greatest (−4.6% per annum) in the Czech Republic. Again, patterns were similar for males and females.
Discussion
This paper provides a comprehensive overview of the patterns and trends in the overall CRC incidence and mortality worldwide. CRC incidence and mortality rates varied widely, with distinct gradients across HDI levels. We identified three patterns of CRC incidence and mortality trends: (1) increases in both incidence and mortality in the most recent decade, as observed in rapidly transitioning countries (eg, medium and high HDI countries including those in the Baltics, as well as Russia, China and Brazil), (2) increases in incidence, with concomitant decreases in mortality, as seen in very high HDI countries including Canada, UK, Denmark and Singapore and (3) decreases in both incidence and mortality, as observed in a number of the highest HDI-indexed countries including the USA, Japan and France.
The mortality declines observed in latter two groups affect both sexes and have been previously reported in North America (the USA and Canada5 ,18), Oceania (Australia and New Zealand), most European countries (other than Croatia, Romania, Latvia, Estonia and Russia) and Asia (Japan).2 These can partly be linked to improving survival through the adoption of best practices in cancer treatment and management for CRC.19 ,20 Removal of polyps and early detection efforts,21–24 including the adoption of colonoscopy, flexible sigmoidoscopy, CT colonography, faecal immunochemistry testing and faecal occult blood testing, may be responsible for the rest of the observed trends. The introduction of screening tests may initially increase CRC incidence rates due to the detection of undiagnosed disease but has been shown to reduce incidence longer term due to the removal of precancerous polyps during colonoscopy.24 This may be particularly pertinent in explaining the uniformly decreasing mortality trends in the USA, Israel and Japan, countries where organised screening and early detection programmes have been established since the 1990s.25 However, the extent to which screening interventions are responsible for the recent reduction in incidence rates in these countries, relative to a reduction in risk via a changing prevalence and distribution of the key risk factors, is difficult to clarify at present. Other high-income countries have introduced organised screening practices very recently; it is however unlikely that screening has materially influenced recent incidence trends in these countries.
The presence of birth cohort effects implies the importance of changing risk in successive generations in contributing to the recent plateau or declines in incidence observed in certain very high HDI countries without long-standing organised screening programmes, most notably Australia, New Zealand and several European countries.26 Certainly, changes in the prevalence of lifestyle-related factors linked to the extent of ‘westernisation’ are likely to be, in part, responsible for the global variation in CRC incidence as well as the observed increasing incidence trends in countries in transition in groups (1) and (2). These modifiable risk factors include alcohol consumption,27–29 poor diet (low consumption of fruits and vegetables, and high consumption of red/processed meats),30–36 obesity,37 ,38 physical inactivity39 ,40 and smoking.41–43 Despite higher relative risks, family history of CRC44 and IBD45 accounts for only a small proportion of the observed variation of CRC burden globally given their lower prevalence. Established protective factors that could partly explain stabilising of incidence rates in high-income countries include the regular use of aspirin,46 ,47 the use of oestrogens after menopause48 and possibly vitamin D intake.49
Dietary patterns and the overall composition of diet have shifted dramatically over the past half-century, with distinct differences within world regions and individual countries. In Japan, for example, cereal consumption decreased sharply and vegetable consumption remained almost stable since the 1950s until 1990.50 In contrast, meat and fat intake increased sharply from the mid-1950s until the early-1970s to mid-1970s. The slow increase until the last decade has been met with marked concomitant increases in both colon cancer incidence and mortality during the years 1990–2000.51 The rapid transition in income and economic growth in low-income and middle-income countries has shifted dietary patterns towards an increased intake of fat, sugar and animal-source foods.52 Changes in the food environment including access to cheaper ‘junk’ food were also paralleled by reductions in physical activity and increases in sedentary behaviour, fuelled by both increases in overweight and obesity and changes in the built environment.53
Increases in mortality have been reported in several countries in Latin America, the Caribbean and Asia,54 ,55 and these may reflect limited health infrastructure and poorer access to early detection and treatment.56 Survival from CRC depends heavily on the stage at diagnosis,57–59 and the unfavourable distribution of advanced cancers in low-income and middle-income countries may explain the higher M:I ratios as well as increases in mortality in these countries. For colon cancer, typically the tumour and corresponding lymph vessels are removed during surgery and adjuvant chemotherapy is administered to patients at high risk of relapse.60 As for rectal cancer, complete removal of the mesorectum is the standard surgical procedure that has been shown to increase survival and substantially decrease the risk of recurrence.60 ,61 In addition, typically a combination of (neo)adjuvant chemotherapy and radiotherapy is administered, whereby the recommended regimen depends heavily on the tumour type and stage at diagnosis. Yet, in low-income settings such as sub-Saharan Africa, surgery is often the only available treatment option and adjunctive therapy often not available.62 Among all patients with cancer receiving radiotherapy in low-income and middle-income countries only 1.3% and 3.1% received radiotherapy for cancers of the colon and rectum, respectively, while the ‘optimum’ proportion should have been 14% and 61%, respectively.58 Furthermore, delays in diagnosis, referral and treatment and also cultural beliefs and financial constraints, for example, in rural areas of Latin America, may explain part of the higher mortality in this region.62 ,63
This study has a number of strengths and limitations. We have aimed to provide a comprehensive analysis of geographical variations of both CRC incidence and mortality in 2012 by sex and the corresponding trends in both indicators in 37 countries. Attention should be drawn to lack of availability of recorded (registry) incidence and mortality data (particularly in low-income and middle-income countries) in deriving national incidence and mortality estimates in 184 countries as part of our GLOBOCAN compilation; only one-third and one-fifth of the world's countries presently report high-quality incidence and mortality data, respectively. For the trends analyses, we used CI5 data of high comparability, completeness and validity to assess trends in incidence. In using national mortality, we used only data with at least WHO-defined medium levels of completeness and coverage.
The intention was to provide a global snapshot of the scale and profile of CRC today, using high-quality data wherever possible. This study serves as a pointer to show how the disease burden is likely to develop in low-income countries in the longer term and highlights the pressing need for cancer control action to halt the rising mortality rates in many low-income and middle-income countries. While the scope of this study necessitates a general approach, the main weakness stems from a lack of granularity in the analyses. We have not included here a separate assessment of colon and rectal cancer, nor did we examine variations in distal (left-sided) cancers of the rectosigmoid junction and proximal (right-sided) cancers of the descending and sigmoid colon, despite many studies reporting a rising proportion of the latter tumours. The inclusion of birth cohort analyses would also have led to a more robust assessment of the recent direction of trends enabling the generation of hypotheses linked to the changing prevalence of causative factors in successive cohorts and the impact of early-stage factors and early-in-life experiences, and their further study will increase our understanding of the aetiology of this cancer.
Diverse global CRC patterns and trends point towards widening disparities and an increasing burden in countries in transition. Generally, CRC incidence and mortality rates correlate with the adoption of a western lifestyle; while they are still rising rapidly in many low-income and middle-income countries linked to ongoing societal and economic development, in highly developed countries, rates are stabilising or decreasing. Decreases in incidence (also seen in recent birth cohorts) in high HDI and high-risk countries are likely driven by changes in lifestyle and dietary patterns over the past decades, which might translate into further future rate declines as these cohorts age. Early detection and screening might have led to short-term increases in incidence, but such interventions will eventually contribute to mortality reductions through the increased detection of early-stage tumours.
The fact that CRC has replaced infection-related cancers as the second most common cancer in several middle-income countries (particularly among women) highlights the major challenge of CRC control in countries undergoing significant socioeconomic transition, and the importance of continued efforts to monitor trends in CRC incidence, mortality and survival worldwide. Without targeted resource-dependent actions based on this evidence, the number of patients with CRC will continue to increase in future decades beyond those already projected as a result of population ageing and population growth. Improvements in treatment options and accessibility, including tertiary care, are vital in low-income and middle-income countries that face an increasing burden of CRC. In light of the limited capacity for health service provision and associated costs, however, there remains an overwhelming need to prioritise and integrate primary prevention and early detection measures into existing healthcare plans.64
Acknowledgments
The authors gratefully acknowledge all cancer registries and their staff who have contributed in sharing their data needed for this study. This work was undertaken during the tenure of a Postdoctoral Fellowship to Dr Mónica S. Sierra from The International Agency for Research on Cancer, partially supported by the European Commission FP7 Marie Curie Actions—People—Co-funding of regional, national and international programmes (COFUND).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
- Data supplement 3 - Online table 3
Press release
Files in this Data Supplement:
Footnotes
Contributors Study concept and design: MA, ML, MSS and FB. Analysis and interpretation of data: all authors. Drafting the manuscript: MA, MSS and FB. Critical revision of the manuscript for important intellectual content: all authors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.