Article Text

Abstract
The gut-derived incretin hormone, glucagon-like peptide 1 (GLP-1) lowers postprandial blood glucose levels by stimulating insulin and inhibiting glucagon secretion. Two novel antihyperglycaemic drug classes augment these effects; GLP-1 receptor agonists and inhibitors of the GLP-1 degrading enzyme dipeptidyl peptidase 4. These so called GLP-1 based or incretin based drugs are increasingly used to treat type 2 diabetes, because of a low risk of hypoglycaemia and favourable effect on body weight, blood pressure and lipid profiles. Besides glucose control, GLP-1 functions as an enterogastrone, causing a wide range of GI responses. Studies have shown that endogenous GLP-1 and its derived therapies slow down digestion by affecting the stomach, intestines, exocrine pancreas, gallbladder and liver. Understanding the GI actions of GLP-1 based therapies is clinically relevant; because GI side effects are common and need to be recognised, and because these drugs may be used to treat GI disease.
- GUT HORMONES
- GLUCAGEN-LIKE PEPTIDES
- GASTROINTESTINAL PHYSIOLOGY
Statistics from Altmetric.com
Introduction
The incretin hormone glucagon-like peptide 1 (GLP-1) is secreted by the gut in response to nutrient ingestion. It enhances insulin secretion by the pancreatic islet cells and inhibits glucagon secretion, thereby lowering postprandial blood glucose levels.1 Two novel drug classes were developed to augment these responses and target hyperglycaemia in type 2 diabetes (T2DM): GLP-1 receptor agonists (GLP-1RAs) and inhibitors of the GLP-1 degrading enzyme, dipeptidyl peptidase 4 inhibitors (DPP-4Is) (table 1). Based on their pharmacokinetic profiles, GLP-1RAs are classified into short-acting and long-acting agents. At present, these GLP-1 (or incretin) based drugs are widely used as second-line treatment for T2DM, after metformin has failed.2
Overview of the registered GLP-1 receptor agonists and DPP-4 inhibitors
Apart from contributing to the enteroinsular axis, GLP-1 is involved in several other processes. Thus, GLP-1 based therapies have extrapancreatic effects including early satiety, weight loss, increased insulin sensitivity, blood pressure lowering and improved lipid profiles.3 These actions have been extensively advocated, because of potential cardiovascular benefits. Less attention has been given to the GI effects of GLP-1 and associated therapies. By delaying a range of digestive processes, these responses contribute to glucose lowering.4 Endogenous GLP-1 reduces proximal GI motility, whereas pharmacological concentrations influence the physiology of the stomach, intestines, exocrine pancreas, gallbladder and liver.
Understanding the GI effects of these drugs is of clinical importance. First, GLP-1 based drugs may be employed to treat GI disorders, as emerging evidence indicates that they are beneficial in, for instance, non-alcoholic fatty liver disease (NAFLD), IBS and short bowel syndrome. Second, they often cause GI complaints, mostly nausea, constipation and diarrhoea. With their increasing prescription rate, such side effects will be frequently encountered and need to be recognised. Finally, concerns have been raised that GLP-1 based therapies may induce pancreatitis and pancreatic cancer.
In order to understand the GI implications of GLP-1 based therapies, it is necessary to return to the physiological basis. This review will provide insight in the underlying mechanisms of GLP-1 and GLP-1 based therapies and discusses the potential beneficial and adverse effects of these new drugs on each GI organ system.
GLP-1 physiology
As the name suggests, GLP-1 is homologous to glucagon, sharing the precursor proglucagon. Alternate splicing leads to glucagon production in the pancreatic α-cells and GLP-1 in the enteroendocrine L cells.5 L cells are present throughout the intestine, but predominantly in the distal ileum. These cells are triggered to secrete GLP-1 by the presence of nutrients (mostly glucose and fat), as well as by bile acids (figure 1).6–8 Already minutes after a meal, plasma GLP-1 levels start to rise, peaking after 2 h. Since GLP-1 secretion starts prior to the arrival of nutrients to the ileum, a feed-forward loop must be present. This indirect mechanism seems to involve neuronal pathways. For instance, blockage of the acetylcholine receptor of L cells by atropine inhibits this early GLP-1 secretion in humans.9

GLP-1 life cycle. Legend: GLP-1 is secreted from intestinal L cells after direct stimulation of luminal receptors or indirect stimulation through neuronal pathways. As soon as GLP-1 is released in the portal circulation, degradation by DPP-4 occurs. When GLP-1 reaches the liver, 25% of the originally secreted GLP-1 is left. Further degradation occurs in the liver and arterial system, and only 15% reaches peripheral organs. Here, GLP-1 stimulates the GLP-1 receptor. GLP-1 additionally affects target organs through indirect stimulation of the vagal nerve in the portal vein. DPP-4, dipeptidyl peptidase 4; GLP-1, glucagon-like peptide 1; GLP-1R; glucagon-like peptide 1 receptor.
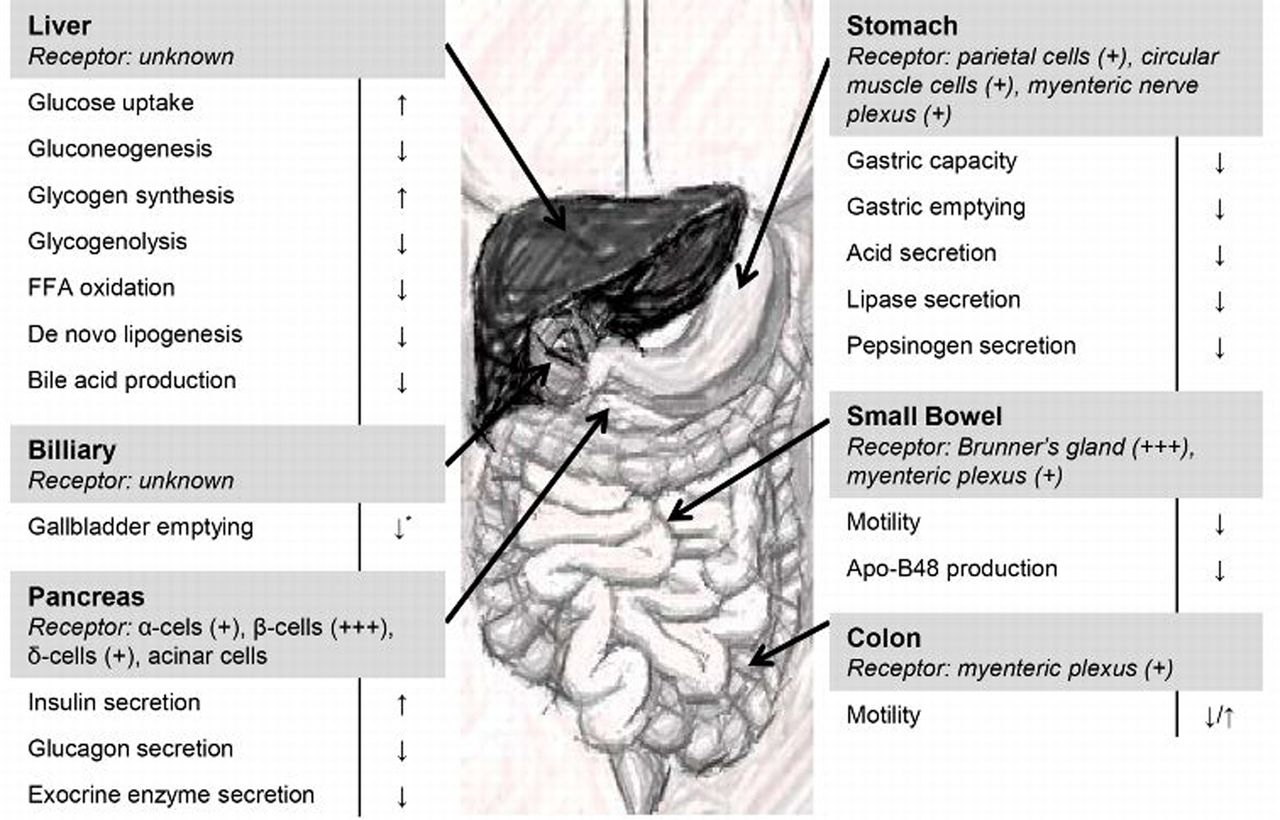
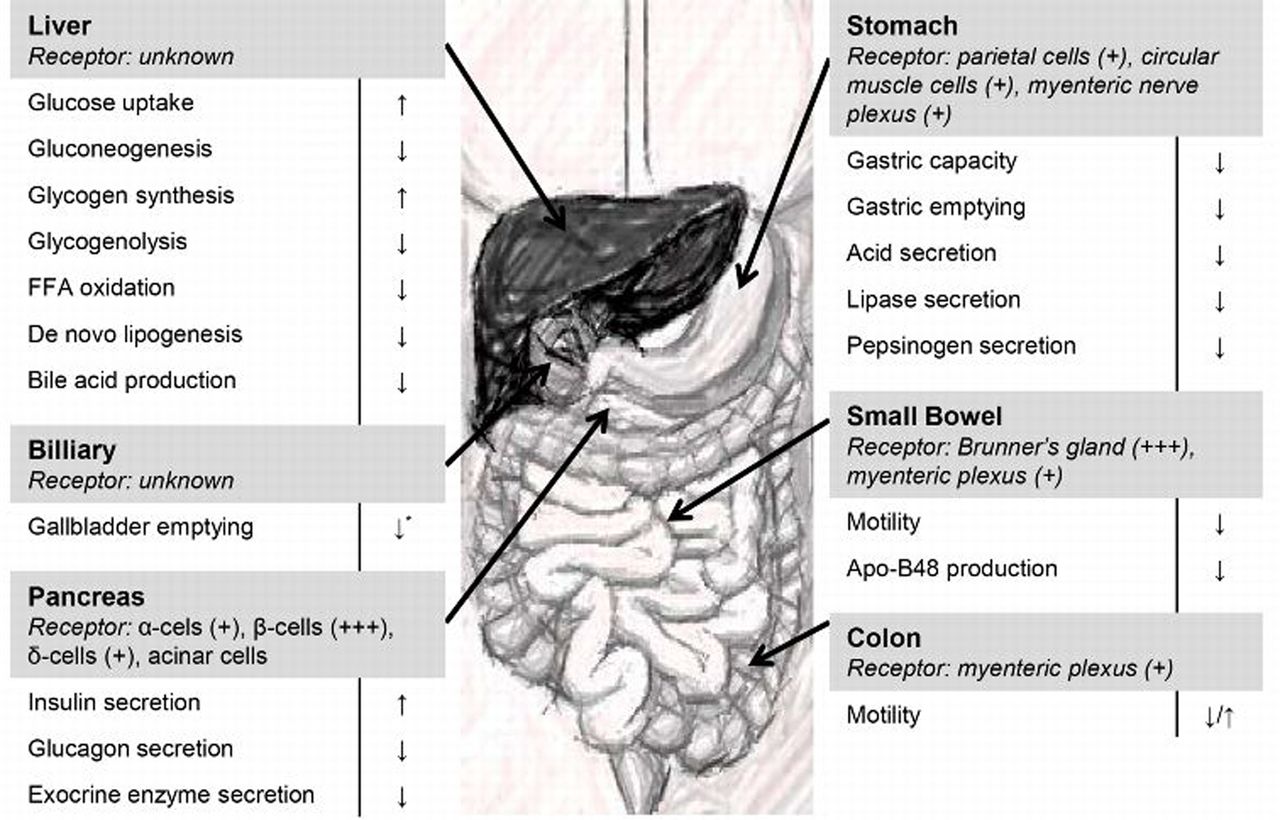
The actions of GLP-1 are thought to be effectuated by the GLP-1 receptor (GLP-1R), which is present in numerous organs (figure 2).10 ,11 However, when this receptor is antagonised by exendin (9–39), some effects still pertain, suggesting involvement of additional receptors.12 After meals, GLP-1 levels quickly return to baseline. Rapid degradation by dipeptidyl peptidase 4 (DPP-4) and renal clearance of GLP-1 and its metabolites result in a half-life of 1–2 min.13 ,14 Only 10–15% of the endogenous GLP-1 enters the circulation (figure 1).15 Given this low systemic concentration, indirect receptor stimulation through the vagal nerve was postulated. Indeed, in animals and humans, vagal blocking diminished the effects of GLP-1.16 ,17
{kind=link}
{kind=link}
The effects of GLP-1 on different GI organ systems. Legend: Receptor concentrations are graded from (+) to (+++) and were determined using validated immunohistochemistry or autoradiography methods.10 ,11 *effects have only been demonstrated for GLP-1RA, effects of GLP-1 peptide unstudied. Apo-B48, apolipoprotein B48; FFA, free fatty acid; GLP-1, glucagon-like peptide 1.
Incretin and enterogastrone
Endogenous GLP-1 stimulates pancreatic insulin secretion in a glucose-dependent manner. As such, it is involved in the so called ‘incretin effect’, meaning higher insulin release after oral glucose intake, than after intravenous glucose administration. Its potency is demonstrated by blockage of the GLP-1R, which results in a 50–70% decrease in insulin secretion after oral glucose intake.18–20 In addition, GLP-1 may also serve as an enterogastrone, a hormonal mediator of the ileal brake phenomenon.21 This mechanism guards the distal intestine from caloric overload, by reducing GI transit, gastric acid secretion, pancreatic exocrine excretion and gallbladder emptying.22 Several studies using the GLP-1 receptor antagonist exendin (9–39) revealed an inhibitory role of GLP-1 on proximal GI motility.20 ,23–25 Some even suggest that the role of GLP-1 as enterogastrone outweighs its role as incretin in glucose homoeostasis.26 ,27
GLP-1 based medication
GLP-1 based drugs mimic and exceed the effects of endogenous GLP-1 on metabolism and digestion, causing additional changes in intestinal mucosal proliferation, gallbladder motility, and hepatic glucose and lipid production (figure 2).28 Two types of GLP-1 based therapies are in use: incretin mimetics; GLP-1RAs that bind to the GLP-1 receptor and mimic the action of GLP-1, and incretin enhancers; DPP-4Is that prolong endogenously produced GLP-1 activity, and the activity of other hormones that are degraded by DPP-4 (table 2).
Other peptides degraded by DPP-4 and their actions, stimulated during DPP-4 inhibition
For both antihyperglycaemic drug classes, several agents have been approved for the treatment of T2DM. The first available GLP-1RA, exenatide, was based on a peptide extracted from saliva of the gila monster (Heloderma suspectum). Subsequently, synthetic forms, more homologous to human GLP-1, were developed. The crucial difference between endogenous GLP-1 and GLP-1RAs is the susceptibility for degradation by DPP-4. GLP-1RAs are resistant to degradation, leading to prolonged half-lives of 2–160 h. Combined with a high dose administration, this results in 6–10 times supranatural serum levels.29 Based on their half-lives, GLP-1RAs are classified as short-acting agents (exenatide twice daily and lixisenatide) and long-acting agents (albiglutide, dulaglutide, exenatide once weekly and liraglutide). GLP-1RAs are administered subcutaneously, ranging from twice daily to once weekly, but other routes are being investigated.30
DPP-4Is are taken orally, once or twice daily, while once-weekly formulations are currently being developed.31 They inhibit degradation by 80–97%, with half-lives of 2–40 h and maintain GLP-1 at postprandial levels.29 However, DPP-4 degrades GLP-1, and several other hormones, including glucose-dependent insulinotropic peptide, glucagon-like peptide 2 (GLP-2) and peptide YY (PYY) (table 2). Hence, DPP-4Is have a wider range of actions than GLP-1RAs. Because some of these actions neutralise each other, GI effects are more pronounced with GLP-1RAs than DPP-4Is.
GI effects of GLP-1 based therapies
Stomach and duodenum
GLP-1 and GLP-1RAs decrease gastric emptying in healthy volunteers and patients with diabetes.32 In a variety of studies, GLP-1 prolongs the lag time, inhibits propulsion waves, stimulates pyloric tone and doubles time to empty 50% of gastric contents.32–37 It also decreases gastric acid and lipase secretion by 67% and 36%, respectively.38 ,39 The underlying mechanisms for these responses are unclear. Direct stimulation of GI smooth muscle cells by GLP-1 did not change gastric tone in rats.40 After vagal blocking, the GLP-1 effect on gastric motility was lost.16 ,17 ,25 Combined, these data suggest vagal mediation.
While short-acting agents retain their gastric inhibitory effects after prolonged treatment, these effects wane significantly with long-acting GLP-1RAs, already after 2 weeks.41–43 Tachyphylaxis, due to sustained receptor exposure by long-acting agents, has been postulated to cause this phenomenon. However, this theory is mostly based on small studies in healthy volunteers.44 ,45
In contrast to GLP-1RAs, DPP-4Is have little to no effect on gastric motility.24 ,32 ,46 ,47 An explanation for this discrepancy remains elusive. Some have speculated that the DPP-4I-induced rise in GLP-1 to postprandial levels is not high enough to cause gastric inhibition,48 but GLP-1 infusion up to similar levels did reduce gastric emptying.49 An alternative hypothesis is that DPP-4Is simultaneously affect other peptides that counteract the inhibitory effect of GLP-1. For example, degradation of PYY (1–36) to the more potent gastric inhibitor PYY (3–36) is prevented by DPP-4 inhibition.50
Clinical implications
Glucose control
A complex interaction exists between glycaemia and gastric motility.51 Higher glucose levels delay, whereas lower levels stimulate gastric emptying.52–54 As a result, the inhibitory effect of GLP-1 on gastric emptying is more pronounced during hyperglycaemia and reduced during hypoglycaemia.52 ,53 Conversely, gastric emptying rate is accountable for approximately 35% of the postprandial glucose excursions.55 ,56 Consequently, inhibition of gastric emptying by GLP-1 and short-acting GLP-1RAs reduces postprandial glucose levels.34 ,57 The significance of this effect was demonstrated in a study where co-infusion of the prokinetic erythromycin blunted the inhibiting effect of GLP-1 infusion on postprandial glucose excursions.58
Weight loss
While DPP-4Is are weight-neutral, GLP-1RAs (short-acting and long-acting) induce weight loss in a dose-dependent manner.59 Recently, a high-dose preparation of the long-acting GLP-1RA liraglutide (3.0 mg) has been approved for weight reduction.60 Mechanisms underlying this weight loss are still incompletely understood. A GLP-1RA-mediated reduction in gastric emptying was postulated to be responsible for decreased appetite. However, the waning effect of tachyphylaxis and reduced fasting appetite suggest other, additional mechanisms.61 Likely, central neurological mechanisms are involved. Preclinical data show that GLP-1 reduces homeostatic and reward-associated food intake and, in humans, GLP-1 affects brain areas related to feeding and satiety.62 Yet, in a recent study, liraglutide reduced central nervous activation initially, but no longer after 12 weeks of treatment, while self-reported hunger scores remained suppressed.63 Unfortunately, effects on gastric emptying were not measured in this study.
Functional dyspepsia
Functional dyspepsia is characterised by delayed gastric emptying, decreased gastric accommodation and increased visceral sensitivity.64 In theory, the inhibitory effects of GLP-1RAs on motility could worsen dyspeptic symptoms (tables 3 and 4). On the other hand, their increase in gastric accommodation and decrease in visceral perception may relieve symptoms.36 ,65 Unfortunately, no clinical studies have been performed regarding the effects of GLP-1RAs in this patient group.
Potential GI therapeutic indications for glucagon-like peptide 1 based therapies
Side effects of GLP-1 based therapies
Dumping syndrome
In case of dumping, the gastric inhibitory effects of GLP-1 may slow down transit and thus reduce the hyperosmolar fluid challenge to the proximal intestine, which causes dumping symptoms (nausea, dizziness and fatigue after meals66). Inhibitory effects on small bowel transit (see below) may contribute, and may additionally reduce abdominal pain and diarrhoea. Recently, a case series demonstrated beneficial effects of liraglutide in seven patients with dumping syndrome after a gastric bypass.67 Whether symptoms improved because of reduced gastric emptying or an earlier insulin peak is unclear. Further studies are needed to establish the effects of GLP-1 based therapies in this specific patient population.
Gastroparesis
The magnitude by which GLP-1RAs decrease gastric emptying depends on baseline gastric motility.68 When gastric emptying is already delayed, GLP-1 seems to have little inhibitory effect and the glucose-lowering effect appears reduced.68 Thus, in patients with gastroparesis, a common complication of T2DM,69 GLP-1RAs may be less effective. Moreover, GLP-1RAs may aggravate symptoms of nausea, vomiting, abdominal pain, early satiety and bloating in patients with (signs of) gastroparesis. Manufacturers currently advise not to use GLP-1RAs in such patients, but evidence is limited and more studies are urgently needed.
Upper GI side effects
Nausea and vomiting are common side effects of GLP-1RAs, which are minimised by a dose-escalating initiation.70 They occur in at least 25% of patients and, although often short-lasting, are a major cause for drug discontinuation.71 After 6 months of treatment, nausea remains present in 3% with long-acting and 9% with short-acting GLP-1RAs.42 ,71 These numbers were mostly acquired by self-reporting, but even when a validated questionnaire was used, liraglutide significantly increased ‘indigestion’ scores, compared with placebo.72 It has long been suggested that these effects are caused by inhibition of gastric emptying. This would explain the absence of nausea with DPP-4Is, and the abating effect with long-acting GLP-1RAs, because of tachyphylaxis. However, nausea also occurs in fasting patients73 and its presence is not closely correlated to gastric emptying inhibition.34 Recent animal studies suggest that central neurological nausea circuits are involved, but human evidence is still lacking.74 Also, why these side effects are common after subcutaneous injection and rare after intravenous administration is still unresolved.75
Another frequent complaint with GLP-1RAs is (nocturnal) gastro-oesophageal reflux.72 This seems surprising, since GLP-1 reduces gastric pressure and acid secretion.36 ,76 Perhaps, GLP-1(RA)s also reduce gastro-oesophageal sphincter pressure, but this has not been investigated yet.
Small and large intestines
GLP-1(RA) infusion evidently decreases small bowel activity, as observed by a reduction in migratory motor complexes in the fasting state and a reduction in postprandial spiking activity.32 ,77 ,78 The colonic effects of GLP-1 are less clear.32 GLP-1 seems to inhibit colonic motility, as was shown by reduced circular contractions in full thickness muscular colon strips.79 ,80 Notably, a reduction in glycaemia tends to increase intestinal motility, thus the direct inhibitory effect of GLP-1 and GLP-1RAs are likely to be underestimated in these studies.81 Similar to the gastric responses, the intestinal effects appear to be indirect and are probably mediated through neuronal involvement.40 ,79 ,82 ,83
Exogenous GLP-1 affects intestinal motility, and morphology and absorption. GLP-1RAs and DPP-4Is decrease intestinal absorption of triglycerides and lower plasma levels of apolipoprotein B48 and triglycerides.68 ,84–87 In healthy rodents, mucosal mass and intestinal length increased after 12 weeks of treatment with a GLP-1RA, but not with a DPP-4I.88 However, in an animal model of experimental colitis, DPP-4I did restore mucosal damage.89 Thus, GLP-1RAs and DPP-4Is seem to have proliferative effects on intestinal epithelial cells. This combination of decreased motility and absorption further inhibits glucose absorption.68 ,78
Clinical implications
Irritable bowel syndrome
Though contraintuitive, patients with constipation-predominant IBS (c-IBS) may benefit from GLP-1 effects (tables 3 and 4). In these patients, symptoms seem to be caused by abnormal contractions of the circular colonic muscles, which are reduced by GLP-1.79 Indeed, a placebo-controlled trial showed that the GLP-1RA ROSE-010 improved scintigraphically measured colonic transit time in patients with c-IBS.80 Furthermore, high-dose GLP-1 infusion reduced migratory motor complexes and intestinal motility in patients with IBS.77 Data from animal studies suggests that GLP-1RAs also decreases visceral sensitivity.90 In a double-blind randomised prospective trial in humans, pain relief, assessed with a visual analogue score, was higher with ROSE-010, as compared with placebo.91 Since T2DM and IBS frequently coincide, GLP-1RAs might be of double benefit to these patients.92
Short bowel syndrome
Malabsorption is a frequent problem in short bowel syndrome, obviously caused by the reduced intestinal absorbent surface. Loss of the terminal ileum also eradicates the ileal brake mechanism, further compromising digestion. Infusion of GLP-1 peptide significantly reduced diarrhoea and faecal excretions in patients with short bowel, as compared with placebo.93 Similar findings were observed in five cases for the short-acting GLP-1RA exenatide twice daily.94 Although not studied, long-acting GLP-1RAs are probably not as effective, since they have little effect on gastric emptying. A cause of potential concern is the inhibiting effect of GLP-1RAs on appetite, since patients with short bowel syndrome need adequate energy and electrolyte intake.93
Effects of DPP-4Is have not been studied in this population, yet other non-GLP-1-substrates of DPP-4 seem to benefit the clinical condition and quality of life of this patient group. For example, GLP-2 improves intestinal absorption and the nutritional status in patients with short bowel syndrome.95 Recently, the GLP-2RA teduglutide was approved for the treatment of short bowel syndrome.96 Combined infusion of GLP-1 and GLP-2 led to greater effects on intestinal absorption, compared with infusion of either peptide alone, suggesting that DPP-4 inhibition may be highly effective in these patients.93
Mucosal healing in mucositis and IBD
The proliferative effect of GLP-1RAs and DPP-4Is on intestinal mucosa provides possibilities for treatment of chemotherapy-induced mucositis. In animal studies, pharmacological levels of exogenous GLP-1 ameliorated 5-fluorouracil-induced mucositis.97 Although DPP-4Is have no effect on healthy mucosa, the DPP-4I anagliptin restored mucosal damage in an animal model of experimental colitis.89 Also, DPP-4 inhibition increases levels of active GLP-2 and stromal-derived factor-1α, both of which are involved in mucosal healing.88 ,97 These animal studies evidently call for further investigation.
Currently, there are no data confirming that GLP-1 based therapies ameliorate IBD. However, administration of GLP-1RAs or DPP-4Is reduced systemic inflammatory parameters.98 ,99 In addition, GLP-1RAs lower inflammatory activity in psoriasis.100 This combination of mucosal healing and alleviation of systemic inflammation may bare new possibilities for treatment of IBD.
Intestinal side effects: constipation and diarrhoea
Many patients experience constipation or, in contrast, diarrhoea, while using GLP-1 based drugs.72 ,101 Constipation may be caused by a decrease in colonic muscle contractions.79 An explanation for diarrhoea is lacking. In one study, patients experienced osmotic diarrhoea, 8 h after administration of GLP-1.102 Potentially, the intestinal effects of GLP-1 reduce absorption, thereby leading to increased osmosis. Reduced pancreatic exocrine excretion may also play a role, causing malabsorption (see below).103 ,104
Colon carcinoma
Although cell proliferation is beneficial for mucosal healing, it may also induce dysplasia. In mice with familial adenomatous polyposis, GLP-1 and GLP-1RAs increased polyp numbers and size.105 After bariatric surgery, which increases GLP-1 levels, the incidence of colorectal cancer is elevated.106 Consequently, GLP-1 based therapies should be used with caution in subjects at risk for colorectal cancer, until further studies become available.
Exocrine pancreas
Intravenous infusion of GLP-1 reduces pancreatic exocrine function in preclinical and human studies.103 ,104 ,107 In pigs, GLP-1 reduced bicarbonate secretion.107 Administration to healthy volunteers led to an immediate decrease in pancreatic trypsin and lipase secretion of over 40%.103 ,104 Underlying mechanisms are incompletely understood. Direct stimulation of acinar cells by GLP-1 did not affect pancreatic amylase secretion in vitro.108 Again, indirect mediators are likely, possibly through vagal nerve activation or through the pancreas-stimulating hormones secretin and cholecystokinin (CCK).39 ,107 Also, the (GLP-1 induced) gastric effects decrease duodenal acidity, which is a major stimulus for secretin/CCK secretion. Thus, inhibition of exocrine secretion may be partly mediated by gastric responses.103 To date, the influence of GLP-1 based drugs on exocrine pancreatic function remains unstudied.
Clinical implications
Pancreatitis and pancreatic carcinoma
Soon after their introduction, GLP-1 based drugs were linked to development of pancreatitis and pancreatic cancer109 (tables 3 and 4). In patients with T2DM using GLP-1 based drugs, a subtle and asymptomatic increase in plasma lipase and amylase levels was observed,110 ,111 suggesting subclinical inflammation or pancreatic duct obstruction. Findings from animal studies are conflicting. A handful of studies showed that GLP-1RAs induce pancreatic inflammation, cellular proliferation and intraepithelial neoplasia (PanIN).112–114 One study found an association between the DPP-4I sitagliptin and pancreatitis, ductal cell replication and metaplasia in a rat model of diabetes.115 However, the majority of animal studies did not find any effect of GLP-1RAs or DPP-4Is on pancreatic physiology, even with a 240 times increased dose.116–122 Notably, some studies even suggested that GLP-1RAs decreases inflammation and malignant degeneration.114 ,123–125
Few human histological studies are available. In a study in pancreatic donors, including 12 patients with diabetes without GLP-1 based therapy, 7 using sitagliptin and 1 exenatide, GLP-1 based therapy was associated with α-cell hyperplasia and PanIN lesions.126 However, re-analyses showed that the treatment and control groups in this study were severely mismatched, which probably induced confounding.127 ,128 A recent study has demonstrated the absence of the GLP-1R on human pancreatic ductal cells,10 which contradicts the hypothesis that GLP-1R activation leads to ductal cell proliferation.113
Clinical data are available from pharmacovigilance studies, database studies and randomised clinical trials (RCTs). Pharmacovigilance studies have shown associations between GLP-1RAs and DPP-4Is and acute pancreatitis and pancreatic carcinoma.109 However, since these studies depend on spontaneous reporting by clinicians, they become notably unreliable when a certain side effect receives media attention, as happened in this case. Additionally, they lack information on confounders. Indeed, patients with T2DM often have concomitant risk factors for pancreatitis, including obesity, long-standing disease and use of comedication. Importantly, these factors are likely to be more present in patients with an indication for GLP-1 based therapy.
In contrast, healthcare databases are able to correct for potential confounding. These did not show a relation between GLP-1 based therapies and pancreatic adverse events,129–134 except for a single study. In this case, a combined analysis of exenatide and sitagliptin was performed.135 When each drug was analysed separately, however, no association with pancreatitis was found. Four recent large-scale RCTs, axagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus - Thrombolysis in Myocardial Infarction (SAVOR-TIMI 53) (saxagliptin), Examination of Cardiovascular Outcomes with Alogliptin versus Standard of Care in PAtients with Type 2 Diabetes Mellitus and Acute Coronary Syndrome (EXAMINE) (alogliptin), Trial to Evaluate Cardiovascular Outcomes After Treatment with Sitagliptin (TECOS) (sitagliptin) and Evaluation of Lixisenatide in Acute Coronary Syndrome (ELIXA) (lixisenatide), which investigated the cardiovascular safety of DPP-4Is and GLP-1RAs, did not identify an increased risk of pancreatitis or pancreatic cancer.136–139 Notably, a trend towards an increased incidence of acute pancreatitis with sitagliptin was seen (0.3% vs 0.2% with placebo, p value 0.066).138 However, these trials did not have sufficient power and follow-up to investigate rare side effects. A meta-analysis did not find any association with acute pancreatitis, although the most recent studies were not included and an update is needed.140
Recently, the regulatory authorities have reviewed all available preclinical and clinical evidence, and found no causal association between GLP-1 based therapies and pancreatic adverse events.141 Yet, all studies combined, evidence is still scarce and the follow-up time of current studies may be too short for the development of pancreatic cancer. Thus final conclusions cannot be made. Until further data become available, it is highly recommended not to use these agents in patients with a (family) history of pancreatic disease.
Liver and biliary system
GLP-1 induces several metabolic changes in the liver, adding to lower glucose and lipid levels. Independent from insulin and glucagon, GLP-1 stimulates hepatic glycogen storage, while suppressing gluconeogenesis.142 ,143 It increases mitochondrial degradation of fatty acids and inhibits triglyceride production.144 ,145 In addition, GLP-1 influences bile metabolism.87 It lowers bile acid production and increases excretion, thereby lowering the bile acid exposure of hepatocytes.146 In vitro, GLP-1 and the GLP-1RA exendin-4 increase cholangiocyte proliferation and reduce apoptosis.147 Moreover, a single dose of exenatide decreased CCK-induced gallbladder contractions in healthy humans.28 Combined, these biliary effects may potentially prevent secondary biliary cirrhosis in patients with cholangiopathies.
Clinical implications
Non-alcoholic fatty liver disease
GLP-1 based therapies seem to be beneficial in NAFLD and non-alcoholic steatohepatitis (NASH) (tables 3 and 4). In several animal models, GLP-1 based therapies decreased steatosis and hepatic damage.148 Evidence in humans is less conclusive. Studies showed a reduction in transaminase levels and spectroscopy-measured steatosis, after treatment with GLP-1RAs or DPP-4Is in patients with T2DM and ultrasonography-proven or biopsy-proven NAFLD.149–152 Likewise, on histology, 1 year of treatment with sitagliptin improved NASH severity.153 However, none of these trials had an adequate control group, precluding definite conclusions. Three recent RCTs are of interest. In patients with T2DM, insulin glargine reduced MRI-measured hepatic fat, while liraglutide had no effect.154 Sitagliptin reduced steatosis significantly more than sulfonylurea derivates.155 In patients with biopsy-confirmed NASH (with or without diabetes), 48 weeks of liraglutide treatment was associated with histological resolution of steatohepatitis.156
The mechanisms underlying the effects of GLP-1 based therapies on NAFLD remain speculative. Steatosis is induced by obesity and insulin resistance, while inflammatory cytokines, bacterial endotoxins, mitochondrial dysfunction and/or endoplasmic reticulum stress further lead towards steatohepatitis.157 ,158 As GLP-1RAs and DPP-4Is increase hepatic insulin sensitivity, this may explain the beneficial effect on NAFLD.159–162 GLP-1-induced improvement of hepatic triglyceride handling probably also plays a role. Furthermore, GLP-1RAs and DPP-4Is reduce hepatocyte endoplasmic reticulum stress163 ,164 and inflammatory cytokines,164 ,165 both involved in NASH development.
Cholelithiasis
High-dose liraglutide treatment has been related to increased occurrence of cholelithiasis and cholecystitis in studies, investigating this drug as weight-reducing agent.166 The underlying mechanism remains unclear, but may involve altered bile acid production and excretion, decreased gallbladder emptying or liraglutide-induced weight loss.
Conclusions and future perspectives
The GLP-1 based drugs, GLP-1RAs and DPP-4Is, are increasingly used to treat T2DM. Apart from their insulinotropic effects, their GI effects provide therapeutic possibilities for a wide scale of GI diseases, including functional dyspepsia, dumping syndrome, IBS, IBD, short bowel syndrome, NAFLD/NASH and cholestatic disorders. Since digestive disorders frequently coincide with T2DM, GLP-1 based drugs may have added benefits in these patient groups.
The recent registration of liraglutide for weight loss confirms the safety of these agents in normoglycaemic subjects, and creates possibilities for a more general application in GI disease. However, evidence is still mechanistic in nature, and not solid enough to direct clinical care. To gain approval for such indications, more studies are needed, which will take time. While results from ongoing studies on NAFLD are eagerly awaited (clinicaltrials.gov: NCT01237119, NCT02147925 and NCT01744236), large-scale RCTs with adequate control groups are needed to establish safety and efficacy for other applications.
On the other hand, GLP-1 based therapies frequently cause GI side effects, such as nausea, constipation and diarrhoea, which need to be recognised. Such side effects may limit the use of these drugs in patients with pre-existing GI symptoms, which are common; in a self-reported study, nausea, heartburn, early satiety, diarrhoea and constipation were all more prevalent in patients with diabetes than in controls.167 Also, reports of serious adverse events (ie, acute pancreatitis, pancreatic cancer) need to be acknowledged. Although an increased risk was never proven, these issues need to be clarified, before GLP-1 based therapies can be advocated for treatment of GI disorders.
Finally, to enhance patient comfort, respiratory and oral administration routes of GLP-1RAs are currently being developed. Whether these agents will exert similar metabolic and GI effects needs to be investigated. Hypothetically, oral GLP-1RA could reach high portal levels, and thus be extra beneficial for NAFLD. Inhalation of (very) short-acting GLP-1RA could strongly and briefly reduce gastric emptying, and thus be beneficial for dumping syndrome.
In conclusion, understanding the GI actions of GLP-1 based therapies is clinically relevant for diabetologists and gastroenterologists, because GI side effects are common and need to be recognised, and because these drugs may potentially be applied to treat GI disease.
References
Footnotes
Contributors MMS, LT, MHAM and DHvR researched the literature and (re)wrote the article. All authors (MMS, LT, MHAM, MHHK, DLC and DHvR) made a substantial contribution to the discussion of the content, and reviewed and edited the manuscript before submission.
Competing interests Through MHHK, the VU University Medical Center received research grants from Boehringer-Ingelheim, Novo Nordisk and Sanofi. The other authors declared no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.