Article Text

Abstract
The genetics of isolated colonic Crohn's disease place it approximately midway between Crohn's disease with small intestinal involvement and UC, making a case for considering it as a separate condition. We have therefore systematically reviewed its epidemiology, pathophysiology and treatment. Key findings include a higher incidence in females (65%) and older average age at presentation than Crohn's disease at other sites, a mucosa-associated microbiota between that found in ileal Crohn's disease and UC, no response to mesalazine, but possibly better response to antitumour necrosis factor than Crohn's disease at other sites. Diagnostic distinction from UC is often difficult and also needs to exclude other conditions including ischaemic colitis, segmental colitis associated with diverticular disease and tuberculosis. Future studies, particularly clinical trials, but also historical cohorts, should assess isolated colonic Crohn's disease separately.
- CROHN'S COLITIS
Statistics from Altmetric.com
Introduction
Diagnosis of Crohn's disease is often contentious when ileal involvement is lacking. This has a long history. Colitis with skip lesions and rectal sparing was considered in 19301 as ‘regional migratory ulcerative colitis’. Crohn's classic 1932 paper did not include cases with colonic involvement,2 although non-tuberculous granulomatous involvement of ileum and colon had been reported in 19233 and later by others.4 ,5 From the 1930s to the 1950s, colitis without rectal or terminal ileal involvement was usually designated ‘regional’ or ‘segmental’ colitis.6
The British surgeon Wells first used ‘Crohn's disease of the colon’ when describing cases of granulomatous regional colitis in 1952.7 Initially, this was not widely accepted and Kirsner (1960) continued to refer to cases with submucosal granulomata and skip lesions as UC.8 Identification of Crohn's disease of the colon separately from UC was strongly reinforced by Lockhart-Mummery and Morson,9 who described 25 cases with features including non-bloody diarrhoea, anal fistulae, rectal sparing, skip lesions and strictures. Histopathology showed submucosal giant cell granulomata, fibrous thickening and regional lymph node enlargement. This paper caused a ‘paradigm shift’ that has led practice since. It was reinforced the following year when Cornes and Stecher10 reported 45 patients with isolated colonic Crohn's disease, with fistulation in nearly two-thirds, and skip lesions in 20%.
Later evidence that colonic Crohn's disease, unlike UC, might be improved by faecal diversion,11 ,12 treatable by segmental resection13 and associated with poor outcomes after ileal pouch-anal anastomosis,14 seemed to confirm even more securely its position as a form of Crohn's disease and distinct from UC.
Distinction of colonic Crohn's disease from UC may be difficult though. The term ‘indeterminate colitis’ was introduced to describe cases, ‘10%–20%’, where, after colectomy and examination of the resected colon, a clear diagnosis is not possible.15 The term was often incorrectly applied to patients without colectomy until ‘IBD unclassified’ (IBD-U) was recommended for such cases.16
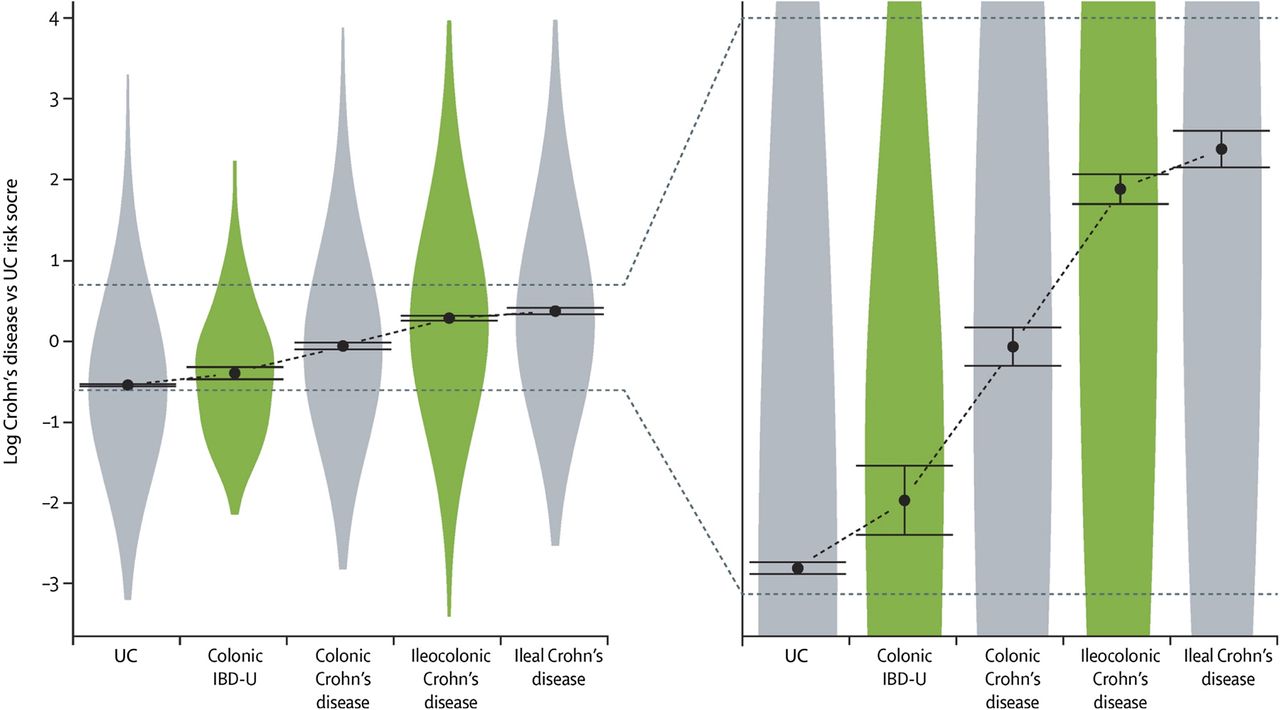
The scene is now changing again—extensive data show that isolated colonic Crohn's disease is genetically separable from Crohn's disease involving the small intestine.17 When the ratio of Crohn's disease-associated to UC-associated genes is compared with disease phenotype, isolated colonic Crohn's disease lies approximately midway between ileal Crohn's and UC. IBD-U, although statistically separable from UC overlaps it considerably and ileocolonic Crohn's disease similarly overlaps ileal Crohn's disease (figure 1). This finding led to recommendation that Crohn's disease with ileal involvement (ileal and ileocolonic), isolated colonic Crohn's disease and UC should be considered as three separate conditions.

Comparison between Crohn's disease genetic risk score and UC genetic risk score for different locations of Crohn's disease, UC and IBD unclassified (from Cleynen et al,17 with permission). This shows that isolated colonic Crohn's lies approximately equidistant genetically between ileal Crohn's disease and UC. IBD-U, IBD unclassified.
It is therefore time to review the epidemiology, genetics, serology, microbiology, and response to treatment of isolated colonic Crohn's disease and to reconsider whether this ‘evidence’ favours isolated colonic Crohn's disease as a variant of Crohn's disease, as a variant of UC or as a separate condition.
Methods
The medical literature was searched using National Library of Medicine/PubMed on 1 December 2015 using the terms ‘colonic and Crohn's’ ‘Crohn's and colitis’ ‘epidemiology and Crohn's’. We conducted additional searches for ‘smoking and Crohn's disease’ and ‘oral contraception and Crohn's’. Later (1 June 2016), additional searches for ‘Crohn's’ and each of the therapies covered were performed. After removal of duplicates and screening of abstracts for relevance, 840 were selected for further review (see online supplementary figures 1 and 2). While the literature search was fully systematic, the subject of this review is necessarily much broader than that of a conventional systematic review. We have only included full publications in English language and have not attempted to judge quality of the data. For epidemiological studies, we included all reports that (a) contained data on at least 100 patients with Crohn's disease and (b) included separate data for isolated colonic Crohn's disease (Montreal classification L2). Where published studies had overlapping patient base and time period, we used only the more completely described data set to avoid duplication. For other aspects of the review (genetics, serological testing, response to therapies and association with environmental factors), we included all studies that identified isolated colonic Crohn's disease separately. For therapeutic studies, we have separately identified data that have been obtained from randomised clinical trials and those that have been obtained from cohort studies. It should be noted that whereas pure ileal Crohn's and pure colonic Crohn's should be readily distinguished by a comprehensive diagnostic assessment including ileal intubation, incomplete assessment could mislabel ileocolonic as colonic. This should be taken into account particularly with respect to older studies, but we have taken care to ensure that all data included here regarding isolated colonic disease relate to patients thought at the time of publication not to have ileal disease. Statistical analysis was performed using StatsDirect V.3.0.171 (StatsDirect, UK).
Supplementary figure
Supplementary figure
Pathology, differential diagnosis and disease course: defining the condition
The histological features of isolated colonic Crohn's disease were first defined by Lockhart-Mummery and Morson.9 They labelled patients with this diagnosis because “they had the same characteristic pathology in the large intestinal lesions as that described by Hadfield18 for the disease as it affects the small intestine”. Gross appearances of the colon following colectomy include less sharp demarcation of ulceration than typically seen in UC and with areas of intact intervening mucosa. In some cases, very marked fibrous thickening with associated stricturing was present. Fibrosis and oedema sometimes extended into the pericolic fat and enlargement of regional lymph nodes was marked. Warren later split the macroscopic features into three patterns: isolated rectal disease; stricturing colonic disease and diffuse colitis—usually with rectal sparing, and noted that approximately 75% develop perianal pathology during their disease course.19
Microscopic features described by Morson included discontinuous inflammation and ulceration, which could extend into the submucosa or deeper into the wall as the basis of fistula formation, plus focal crypt irregularity. Non-caseating epithelioid granulomas were present in the majority, distributed through all layers of the bowel wall as well as regional lymph nodes. Other features included submucosal lymphangiectasia and neuromatous hyperplasia.20 It has subsequently been noted that the earliest lesions—aphthous ulcers—which usually overlie lymphoid follicles, are preceded by a ‘red ring’ sign on colonoscopy, biopsy of which reveals a lymphoid follicle surrounded by reactive hypervascularisation.21
Histopathology alone is diagnostic only in the minority—in a series of 103 cases of Crohn's colitis, diagnosis was determined by microscopy alone in 28%, by distribution (rectal sparing and/or discontinuity) alone in 22% and by combination of the two in 50%.22 Particularly discriminatory features suggesting Crohn's colitis rather than UC include granulomata, submucosal inflammation and relative preservation of goblet cells.23 ,24 At an international workshop, expert pathologists ‘correctly’ identified only 64% of cases with Crohn's colitis and 74% with UC25 leading the European consensus on histopathology of IBD (2013) to note that “accurate discrimination between the two diseases (Crohn's colitis and ulcerative colitis) is not yet optimal among expert gastrointestinal pathologists”. Given that inflammatory disease pathogenesis is multifactorial, an alternative interpretation would be that there is a continuous phenotypic spectrum that runs through from ‘typical’ UC, through IBD-U to ‘typical’ Crohn's colitis.
Early studies reported an additional incidence peak of Crohn's disease in the elderly resulting from cases particularly affecting the sigmoid colon.26 Following the later clarification of segmental colitis associated with diverticular disease (SCAD), this seems probably attributable to SCAD. SCAD can be indistinguishable histologically from IBD and includes a ‘Crohn's-like’ variant with granulomata.27 This reflects emphasis often placed on the diagnostic specificity of the granuloma. However, granulomas are only found in colonoscopic biopsies at diagnosis in about 66% of adults with colonic Crohn's disease, falling to 18% at follow-up.28 Moreover, granulomas, particularly in association with crypts, can be found in UC.29 Other forms of colitis that may need to be considered in the differential diagnosis include ischaemic colitis (see earlier) and infections including amoebiasis and tuberculosis, but it is beyond the scope of this review to consider these further.
Localisation of disease to the colon remains fairly constant over time. The largest published data set by far is the 16 902 Crohn's disease cohort, including 2933 with isolated colonic disease, in the recent genotype/phenotype association study.17 This confirmed previous reports of low rates of progression to ileocolonic disease (5%–14% over 7–10 years).30–32 Although luminal narrowing is common, stricturing (B2 disease) as defined in the Vienna/Montreal classifications requires the presence of prestenotic dilatation or obstructive signs or symptoms and this very rarely occurs, for example, 0/45 cases in a Belgian series,33 whereas penetrating disease (B3) as defined by the Vienna classification (ie, including peri-anal fistulae) occurred in 23% in the same series, less frequently than in patients with ileal disease (46%; p=0.0003) or ileocolonic (28.6%; not significant (NS)). The much larger genotype/phenotype association study confirmed that cumulative probability of progression to B2 and B3 combined over 10 years was substantially lower in colonic disease—23%, than in ileocolonic disease—62%, or ileal disease—68%.17 The risk of surgery (discussed later) was also much lower at 10 years (22%) than for ileocolonic (42%) or ileal disease (62%). A recent meta-analysis showed that colon cancer risk in isolated colonic Crohn's disease is similar to UC of equivalent extent with a pooled standardised incidence ratio (SIR) of 1.7; 95% CI 0.9 to 2.6 (population-based data) compared with SIR 1.8; 95% CI 1.2 to 2.4 for UC but rising to SIR 18.2; 95% CI 7.8 to 35.8 for extensive colonic Crohn's disease in a referral centre population compared with SIR 21.6; 95% CI 15.0 to 31.0 for extensive UC.34
Epidemiology
Changes over time
Studies reporting sequential data from a single centre or region show interesting time trends. Studies from the UK35 ,36 and Sweden37 reported a marked increase in isolated colonic Crohn's as a proportion of total Crohn's from 1970 to 1990 (figure 2A), whereas later studies, particularly from France38 have shown a downward trend since 1990. When looked at across all geographical areas (table 1), although there is no obvious difference in proportion of isolated colonic disease between countries or regions, there is a similar time trend with increase in isolated colonic disease between 1960 and 1990, peaking at an average of about one-third of all Crohn's disease cases, and decreasing since (p=0.02 by polynomial regression, figure 2B).
Studies of CD age and sex distribution and proportion of total, where isolated colonic CD separately identified (in approximate median date order)

{kind=link}
{kind=link}
(A) Isolated colonic Crohn's disease (CD) as percentage of all CD by year in studies reporting sequential data from the same centres or geographical areas. (B) Isolated colonic Crohn's disease as percentage of all Crohn's disease by year in all studies.
Sex variation
We found eight studies that stated the sex distribution of patients with isolated colonic Crohn's disease. In all but one, the female preponderance was equal or greater to that reported from the same study for total Crohn's disease (table 1)—isolated colonic Crohn's disease averaging 65.1% female, compared with Crohn's disease excluding isolated colonic 55.3% female (p=0.027 by paired t-test).
Age at diagnosis
Age at diagnosis of isolated colonic Crohn's disease (in seven studies; table 1), has a median between 28 and 45, around 10 years older than generally reported for all Crohn's—for example, median 25 years in the 16 902 patients studied by Cleynen et al.17 Older age of isolated colonic versus other sites of Crohn's disease was also confirmed by the IBDchip European Project.72 The preponderance of isolated colonic disease among children with very early onset Crohn's disease is discussed later.
Smoking
Cigarette smoking is associated with increased risk for development and progression of Crohn's disease but reduced risk for UC. Smoking is more strongly associated with risk for ileal and ileocolonic Crohn's disease than for isolated colonic disease (table 2). Only one study (of nine)79 reported a higher rate of smoking among patients with isolated colonic Crohn's disease. If the South African data83 that reported exceptionally high rates (73%) across all groups are excluded, the other studies report rates for smoking among patients with isolated colonic disease that averaged 37.8% compared with 49.8% (p=0.008 by paired t-test) for other Crohn's disease sites. This smoking rate is probably slightly higher than for the general population—approximately 30% European adults were smokers in 2008 (WHO).84
Studies of smoking in CD where isolated colonic disease was separately identified
Smoking worsens prognosis of Crohn's disease overall and cessation of smoking improves it.85 ,86 This has been studied less in isolated colonic disease but the conclusion is similar. The largest study80 included 688 patients with Crohn's colitis, 978 with UC and 118 with ‘indeterminate’ colitis. Sixty-one per cent of patients with UC or indeterminate colitis had stopped smoking before disease onset compared with only 12% in isolated colonic Crohn's disease. In women but not men with isolated colonic disease, the risk of needing immunosuppression was increased among smokers (10-year cumulative risk 48% in non-smokers vs 58% in smokers, p<0.01). An earlier study74 showed that smokers with Crohn's colitis relapsed approximately 50% more often (p=0.028) and with more pain (p<0.007) than non-smokers.
Thus, smoking at best has a neutral effect on isolated colonic Crohn's disease but more likely is harmful.
Oral contraception
Meta-analysis of 14 studies, with adjustment for smoking, showed a relative risk of 1.51 (95% CI 1.17 to 1.96, p=0.002) for Crohn's disease among women currently taking oral contraception.87 The relative risk for UC was also increased at 1.53 (95% CI 1.21–1.94, p=0.001). Six of the seven studies that reported risk associated with oral contraception separately for isolated colonic disease found a significant association (table 3) with relatively high OR (2.63), risk ratios (3.6 and 3.23) or HR (4.13). The sole exception89 only included eight cases with isolated colonic Crohn's disease and showed no overall association between oral contraception and risk for Crohn's disease. Excluding the latter study,89 five of the other six studies show higher risks among oral contraceptive users for isolated colonic Crohn's than for other sites.
Studies of oral contraceptive usage in CD where isolated colonic disease was separately identified
Oestrogen-associated ischaemic colitis as a confounder
An early study from Birmingham50 reported patients with apparent oral contraceptive-associated colonic Crohn's disease who had non-granulomatous colitis with rectal sparing.
Ischaemic colitis is a rare but recognised complication of oral contraception that might cause diagnostic confusion.95–97 Most cases have a short duration with typical features of ischaemic colitis including abdominal pain, and rectal bleeding. Colonoscopy shows mucosal friability but no linear ulceration and the proximal colon and rectum are typically normal. Such cases should be readily distinguishable from colonic Crohn's disease, but Tedesco et al98 reported five cases of oral contraceptive-associated colitis with features that overlapped more with colonic Crohn's disease than with ischaemic colitis. Moreover, colonic ‘thumbprinting’, a characteristic feature of ischaemic colitis has been reported in Crohn's disease.99 It is unclear whether diagnostic overlap with milder cases of oral contraceptive-associated ischaemic colitis contributes to the female preponderance of isolated colonic Crohn's disease. If it does then the change to lower oestrogen dosing in later versions of the contraceptive pill might be a plausible explanation for the apparent fall off in cases in recent decades.100 Clinicians should be aware of the possible associations between oral contraception and IBD or ischaemic colitis and advise patients accordingly—such advice should usually include at least a temporary cessation of oral contraception to assess impact on the colitis.
Genetics
The strongest genetic association with IBD is the link between NOD2/CARD15 and Crohn's disease. Meta-analysis of 42 studies showed that this association was stronger for Crohn's disease with small bowel involvement than for those without (OR 2.53; 95% CI 2.01 to 3.16).101 Subsequent study of 1528 patients with Crohn's disease from 8 centres (in 7 European countries) (IBDchip) confirmed the association of NOD2/CARD15 with ileal involvement and also showed that interleukin-23 receptor polymorphisms were more strongly associated with isolated colonic Crohn's (OR 2.20; 95% CI 1.17 to 4.57).72
The most consistent genetic link with UC is with the rare major histocompatibility complex/human leucocyte antigen (HLA) class II allele HLA-DRB*0103. This occurs in <2% in European and white North American populations and is absent in the Japanese. It is strongly associated with colonic Crohn's disease, where it is present at up to 32% frequency with ORs for isolated colonic disease of 5.1 to 18.5 compared with Crohn's disease at other sites.102
The largest study to compare genetic associations with Crohn's disease phenotype included 19 713 patients from 49 centres across 16 countries in Europe, North America and Australasia.17 This confirmed that the strongest association with isolated colonic Crohn's disease was HLA-DRB1*01:03 (p=1.47×10−23, ileal vs colonic OR 0.32, 95% CI 0.29 to 0.41; ileocolonic vs colonic OR 0.47, 95% CI 0.39 to 0.57). The only other loci that were significant across all analyses in this study were NOD2 (16q12), again associated with increased risk for ileal involvement (OR ileocolonic vs colonic 1.61 to 1.59, and 1.89 for the three NOD2 polymorphisms tested) and also macrophage stimulating 1 that encodes a protein which induces macrophage phagocytosis polymorphisms which were more weakly associated with ileal involvement (OR 1.07 to 1.10 according to polymorphism and whether comparing ileal or ileocolonic with colonic disease). When overall genetic risk scores for Crohn's disease and UC were computed as a ratio and compared with phenotype, isolated colonic Crohn's disease was found to be approximately ‘balanced’ in respect of Crohn's disease versus UC genetic risk factors (figure 1). It was found though that even the combination of smoking status with the strongest genetic predictors could only explain 6.8% of the variance for disease location.
Isolated colonic Crohn's disease in childhood and single gene disorders
Among children with very early onset Crohn's disease, there is a marked preponderance of cases with isolated colonic disease, for example, 76.5% before age 5103 and 42% before age 8.104 Among younger cases, there is a strong male preponderance, for example, 1.6:1 across all Crohn's disease presenting <5103 and some of this is accounted for by X linked single gene disorders. The first such condition to be identified was X linked chronic granulomatous disease. Chronic granulomatous disease is associated with defects in neutrophil function leading to skin lesions and in around 40% with a form of IBD that is indistinguishable from Crohn's disease, typically with predominant colorectal and perianal involvement.105 It is due to mutations in one of four nicotinamide adenine dinucleotide phosphate (NADPH) oxidase complex component genes of which the most common (CYBB) located on the X chromosome accounts for about 65% cases.
Rapid developments in DNA sequencing have allowed identification of over 50 further single gene disorders that present as IBD, typically as colonic disease and with presentation before age 6, defined as very early onset IBD (VEO-IBD).106 VEO-IBD cases account for 4%–10% of paediatric IBD.107 One of the most common single gene variants is in the coding region of X linked inhibitor of apoptosis protein that accounts for about 4% of male patients with paediatric onset Crohn's disease.108
Serology including antimicrobial and antineutrophil antibodies
Antimicrobial antibodies such as anti-Saccharomyces cerevisiae (ASCA) and antibodies to outer membrane protein (ompC) are found less often and/or at lower titre in isolated colonic Crohn's than in other Crohn's phenotypes.109 Meta-analyses confirm this particularly for ASCA.110–112 Average sensitivity of ASCA for isolated colonic Crohn's disease diagnosis is 31% but with a wide range (8%–59%) and an average 14% positivity rate in UC (table 4). The clinical utility of ompC antibodies has been less studied, but reported positivity/sensitivity in isolated colonic Crohn's disease is substantially lower than that for ASCA.
Serological test results in isolated colonic CD and UC
Antineutrophil antibodies, particularly an atypical perinuclear antibody (pANCA), are present in around 55% of patients with UC112 and 23% of patients with isolated colonic Crohn's disease (table 4). This compares with pANCA positivity of around 11% in Crohn's disease overall and 3% in non-IBD controls.112
A combination of positive ASCA and negative pANCA is more discriminatory, for example, positivity rate in isolated colonic Crohn's disease of 52% compared with 9% in UC,120 but is still insufficiently predictive for routine clinical use.123
Thus, the frequency in isolated colonic Crohn's disease of both ASCA and pANCA antibodies lies somewhere in between that found in Crohn's disease with ileal involvement (more likely ASCA+, and pANCA−) and that found in UC (more likely ASCA− and pANCA+).
Microbiota
The faecal microbiota in active IBD is commonly dysbiotic with reduced bacterial diversity.124 ,125 This could be secondary to inflammation yet still significant in maintaining chronicity. The large study of pretreatment Crohn's disease by Gevers et al showed only a mild dysbiosis in the faecal microbiota and much greater separation of Crohn's disease from healthy controls when the mucosa-associated microbiota was studied.126 Ileal and rectal mucosal samples typically showed a reduction in Firmicutes such as Faecalibacterium prausnitzii and an increase in Proteobacteria such as Escherichia coli as well as in Veillonella, Haemophilus and Fusibacteria. This confirmed many previous studies showing an increase in mucosa-associated E. coli in Crohn's disease as well as several showing a reduction in F. prausnitzii.127–130
The faecal and mucosa-associated microbiota in isolated colonic Crohn's disease is generally closer to that of healthy controls than is found in patients with ileal or ileocolonic Crohn's disease (table 5). Thus, Baumgart et al127 found that an increase in ileal mucosa-associated E. coli and reduction in ileal F. prausnitzii was only present in patients with Crohn's disease who had ileal involvement and not in those with isolated colonic disease. Similarly, a study of twins with/without Crohn's disease showed that faecal microbial diversity was only reduced and Proteobacteria increased in patients with ileal involvement and not in patients with isolated colonic disease.128 A previous report by the same group also showed a reduction in F. prausnitzii in patients with Crohn's disease with ileal involvement but not in isolated colonic disease.129 Both the twin study by Willing et al129 and the large study in children126 and adolescents132 did however show differences between the mucosa-associated microbiota in isolated colonic Crohn's disease and UC. 16sRNA pyrosequencing of mucosal samples131 confirms the increase in E. coli and reduced F. prausnitzii in Crohn's disease with ileal involvement with milder changes in isolated colonic disease, although the latter did show some reduction in F. prausnitzii compared with healthy controls. This study also confirmed that the mucosa-associated microbiota is consistent at different sites from ileum to rectum in the same individual.
Studies of mucosal microbiota in CD where isolated colonic disease was separately identified
In conclusion, mucosa-associated microbiota changes in Crohn's disease are more marked than faecal changes. The microbiota in isolated colonic Crohn's disease shows changes that tend to be less marked and less consistent than those found in Crohn's disease with ileal involvement.
Response to treatment
Mesalazine
Systematic reviews show no convincing benefit of oral mesalazine (5-aminosalicyclic acid) over placebo either in induction of remission or in maintenance of medically induced remission in Crohn's disease as a whole,133–137 although it may have a modest benefit in maintaining surgically induced remission.137 Sulfasalazine (sulfapyridine linked via azo bond to 5-aminosalicylate) has possible modest efficacy in induction of remission.133 ,134
Among trials that have reported data separately for isolated colonic Crohn's disease, only one trial studied the effect of oral mesalazine in remission induction138 and four studied its effect in maintenance of medically induced remission139–142 (table 6). In none of these was mesalazine significantly more effective than placebo but in two studies,139 ,140 there was a weak signal suggesting a better response in ileal disease. A single trial of olsalazine showed worse results than for placebo, probably because of drug-related diarrhoea.146 Sulfasalazine was no better than placebo in two trials of maintenance,143 ,144 but there was a weak signal of efficacy in remission induction in two trials144 ,145 and these only studied 17 and 27 patients with isolated colonic disease, respectively (including placebo). Apart from case reports, there have been no published studies of rectal mesalazine in isolated colonic Crohn's disease.
Trials of 5-ASA preparations where data presented separately for isolated colonic CD
It can be reasonably concluded that mesalazine and olsalazine do not have efficacy in isolated colonic Crohn's disease. Sulfasalazine possibly has some efficacy in remission induction.
Antibiotics
Systematic reviews suggest a beneficial effect for antibiotics in the induction of remission for Crohn's disease, although these have included diverse antibiotics and small trials.147–149 The largest study to date is for rifaximin.150 Three doses were tested: 400, 800, 1200 mg or placebo twice daily for 12 weeks with good efficacy overall but no dose response. Among patients with isolated colonic disease, higher remission rates (51%) were found for rifaximin (pooled doses) than for placebo (37%) and efficacy was better in this group than for other disease sites (table 7).
Trials of antibiotics where data provided separately for patients with isolated colonic CD
Metronidazole has also shown better efficacy in isolated colonic Crohn's disease but based on very small numbers (Blichfeldt et al:151 n=6 crossover; Sutherland et al:152 8 active and 4 placebo). In a study of 134 patients randomly assigned to ciprofloxacin and metronidazole, both 500 mg twice daily, or placebo in combination with budesonide 9 mg daily,153 a trend was seen towards benefit in patients with colonic involvement compared with those without, but separate data were not reported for patients with isolated colonic disease. A large randomised trial of long duration (up to 2 years) antibiotic therapy (clarithromycin, rifabutin and clofazimine) targeted against Mycobacterium avium paratuberculosis in patients also receiving tapered prednisolone showed short-term efficacy with 66% active in remission at 16 weeks compared with 50% placebo (p=0.02) and 39% relapsed by 12 months compared with 56% placebo (p=0.054).154 No differential response was seen according to disease location, but data were not presented separately for patients with isolated colonic disease.
Thus, rifaximin and metronidazole show some evidence of efficacy in patients with isolated colonic Crohn's disease and antibiotics tend to perform better in this group of patients than in Crohn's disease at other sites but based on very small data sets. Further trials are clearly needed.
Corticosteroids
Given the widespread use of corticosteroids in Crohn's disease, the quality of evidence for their efficacy is surprisingly poor. There have only been two placebo-controlled trials of standard glucocorticosteroids.144 ,145 Each of these included only eight steroid-treated patients with isolated colonic disease (table 8) with one trial144 showing no benefit and the other145 showing efficacy. There has never been a trial to assess dose-responsiveness to conventional corticosteroids in Crohn's disease, so optimal dosage is unknown. More data are available for budesonide but trials have focused predominantly on patients with ileal or ileocolonic disease, so data in isolated colonic disease are again very sparse. The data from one comparison with mesalazine155 support efficacy in isolated colonic Crohn's disease, possibly with a weaker effect than conventional corticosteroids,156 but reduced corticosteroid side effects.
Trials of oral corticosteroids where data provided separately for isolated colonic CD
Antitumour necrosis factor
None of the randomised trials of infliximab157 ,158 or adalimumab159–162 reported subgroup analyses of outcomes based on disease location. In a randomised, placebo controlled trial of certolizumab pegol, patients with colonic (OR 2.39, 95% CI 0.99 to 5.75, p=0.052) and ileocolonic disease (OR 2.07, 95% CI 1.01 to 4.28, p=0.048) were more likely to achieve remission at week 6 compared with ileal disease (OR 0.42, 95% CI 0.18 to 0.99, p=0.048)163 (table 9).
Randomised controlled trials (RCTs) and cohort studies of biological therapy in Crohn's disease where data were provided separately for patients with isolated colonic disease
Several cohort studies have assessed colonic disease location as a predictor of response to antitumour necrosis factor (TNF) agents, four with infliximab and one with adalimumab. Three cohort studies assessing induction therapy with infliximab164–166 all showed better response rates in isolated colonic disease than for disease at other sites. Paradoxically, cohort studies of infliximab maintenance in children167 and of adalimumab maintenance in adults168 both showed higher risk of lost response or dose escalation in isolated colonic disease. Overall, the evidence supports good efficacy for anti-TNF therapy in induction of remission in isolated colonic Crohn's disease, but possibly with a higher subsequent rate of loss of response.
Vedolizumab
In the combined induction and maintenance study of vedolizumab, there was no significant difference in efficacy in isolated colonic disease compared with other locations169 (table 9).
Enteral nutrition
Exclusive enteral nutrition is effective as primary therapy in patients with active Crohn's disease170 ,171 and partial enteral nutrition has shown efficacy in maintenance of remission.172 In UC, total parenteral nutrition and bowel rest are ineffective173 and comparison of enteral with parenteral nutrition showed no difference in efficacy,174 implying no efficacy for enteral nutrition either. Whether enteral nutrition is effective as primary therapy in isolated colonic Crohn's disease is controversial. Relatively few studies provide separate data on patients with isolated colonic Crohn's disease (table 10). Five of the six studies are in children. Two studies176 ,177 report poorer results in children with isolated colonic disease compared with those with small intestinal involvement. Numbers are small though (19 cases of isolated colonic disease across the 2 trials) and the other studies (including 72 cases of isolated colonic disease across 4 trials) found no significant difference in remission rates for those with isolated colonic disease compared with other sites. Further trials of exclusive enteral nutrition are needed in patients with isolated colonic disease.
Results of exclusive enteral nutrition as primary therapy in CD where data provided separately for isolated colonic CD
Surgery
Faecal diversion
Colonic Crohn's disease commonly responds to ‘bowel rest’ induced by a defunctioning ileostomy, whereas UC does not.11 ,12 Instillation of unfiltered ileostomy contents into the defunctioned colon induced relapse, whereas instillation of content that had passed through a 0.22 micron pore diameter filter did not, implying a role for bacteria in pathogenesis.181 Defunctioning ileostomy is less commonly performed for the treatment of uncomplicated colonic Crohn's disease since it was shown that at least 50% relapsed after continuity was restored.182
Resection
The cumulative risk of surgery for isolated colonic Crohn's disease is reported to be 22%–33% 10 years after diagnosis compared with around 75%–90% for ileal disease.17 ,66 Partial resection, either right hemicolectomy for proximal disease or a segmental resection for more distal disease has been shown to be successful therapy for colonic Crohn's disease13 ,183 as is colectomy with ileorectal anastomosis for more extensive disease if the rectum is uninvolved.184 ,185 Approximately 75% of patients with ileorectal anastomosis will still have a functioning anastomosis after 10 years and about two-thirds of those treated by segmental resection will not have required a further resection.185 Recurrence rates are similar after either procedure.186 This contrasts with left-sided UC, where the tempting option of left hemicolectomy with right-sided colo-anal anastomosis consistently fails, usually with rapid recurrence of colitis in the retained colon.187 It should be noted though that segmental resection for colon cancer complicating colonic Crohn's disease has been associated with high (39%) risk for metachronous colon cancer188 suggesting that panproctocolectomy might be a safer option for such patients.
Ileo-anal pouch reconstruction
Crohn's disease has generally been considered a contraindication for restorative ileo-anal pouch surgery and even in selected patients pouch failure of 57% has been reported from the UK.189 Others have suggested that it may be successful in very carefully selected patients. Thus, a series of 3707 patients with ileal-pouch anal anastomosis from the Cleveland Clinic included 150 with Crohn's disease, of whom 32 had a preoperative diagnosis, the remainder diagnosed by postoperative histopathology or on follow-up. Among 59 patients with Crohn's disease reaching 10-year follow-up, pouch survival was 80%.190 Forty-nine of 132 patients (37%) needing pouch excision had a histological diagnosis of Crohn's disease. Considering that a preoperative diagnosis of Crohn's disease was only present in <1% of patients receiving pouch-anal anastomosis, these data do not make a strong case for this procedure in patients with a definite diagnosis of colonic Crohn's disease.
Conclusion
Current data suggest that the genetics, microbiota, serology and smoking association of isolated colonic Crohn's disease lie between those of ileo/ileocolonic Crohn's disease and UC and make a strong case for this phenotype being considered separately (table 11). Genetic data in particular show good separation from ileal/ileocolonic Crohn's disease and the low rate of progression from isolated colonic to ileocolonic disease helps to justify this distinction. There is a disappointing paucity of good quality therapeutic data but the lack of response to mesalazine, whose target cell is the surface epithelium, suggests a different pathophysiology to UC and there are important differences from UC in surgical outcomes, including a good response to segmental resection in selected cases and a generally poor response to pouch reconstruction. Taken together, this implies a compelling need for isolated colonic Crohn's disease to be identified separately from ileal/ileocolonic disease and from UC. This is particularly important when future therapeutic trials are designed and when cohort studies are reported.
A summary of the distinguishing features of the three IBDs: ileal/ileocolonic CD, isolated colonic CD, UC
References
Footnotes
Contributors JMR initiated the review. JMR and SS performed the literature searches and together wrote the first draft. AE advised on the analysis and presentation of epidemiology data. All authors contributed to the writing of the manuscript and approved the final version of the manuscript.
Competing interests SS has received speaker fee from MSD, Actavis, AbbVie, Dr Falk Pharmaceuticals, Shire and received educational grant from MSD, AbbVie, Actavis and is an advisory board member for AbbVie, Dr Falk Pharmaceuticals, Janssen and Vifor Pharmaceuticals. JMR is or has been a member of advisory boards for Atlantic, Pharmacosmos, Procter and Gamble, Vifor and Dr Falk Pharmaceuticals, has received speaking honoraria from Abbott, Dr Falk Pharmaceuticals, Ferring, GlaxoSmithKline, Merck, Procter and Gamble, Schering Plough, Shire and Wyeth and with the University of Liverpool and Provexis UK, holds a patent for use of a soluble fibre preparation as maintenance therapy for Crohn's disease plus a patent pending for its use in antibiotic-associated diarrhoea.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All relevant data are included in the article.