Article Text

Abstract
Objective To analyse the prevalence, incidence and clinical relevance of pancreatic cysts detected as incidental finding in a population-based longitudinal study.
Design A total of 1077 participants (521 men, mean age 55.8±12.8 years) of 2333 participants from the population-based Study of Health in Pomerania (SHIP) underwent magnetic resonance cholangiopancreaticography (MRCP) at baseline (2008–2012). MRCP was analysed for pancreatic cysts with a diameter ≥2 mm. 676/1077 subjects received a 5-year follow-up (2014–2016). The prevalence and incidence of pancreatic cysts (weighted for study participation) were assessed in association to age, gender and suspected epidemiological risk factors. Mortality follow-up was performed in 2015 for all SHIP participants (mean follow-up period 5.9 years, range 3.2–7.5 years).
Results At baseline pancreatic cysts had a weighted prevalence of 49.1%, with an average number of 3.9 (95% CI 3.2 to 4.5) cysts per subject in the subgroup harbouring cysts. Cyst size ranged from 2 to 29 mm. Prevalence (p<0.001), number (p=0.001) and maximum size (p<0.001) increased significantly with age. The 5-year follow-up revealed a weighted incidence of 12.9% newly detected pancreatic cysts. 57.1% of the subjects initially harbouring pancreatic cysts showed an increase in number and/or maximum cyst size. Of all subjects undergoing MRCP, no participant died of pancreatic diseases within mortality follow-up.
Conclusion The prevalence of pancreatic cysts in the general population is unexpectedly high, and their number and size increase with age. Overall, no pancreatic cancer was observed in this collective during a 5-year follow-up. Nevertheless, prospective follow-up imaging showed minimal progress in more than 50%. Only about 6% of cysts and 2.5% of the study group initially presented with cysts of more than 1 cm and thus might be clinically meaningful.
- pancreatic cancer
- pancreas
- pancreatic epidemiology
- pancreatic tumors
- magnetic resonance imaging
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
Cystic pancreatic lesions are a frequent incidental finding in patients undergoing abdominal imaging; however, longitudinal studies are rare.
Mucinous cystic lesions harbour a considerable risk for malignant transformation.
Consensus guidelines on the management of cystic pancreatic lesions have never been evaluated in a population-based setting.
What are the new findings?
The prevalence of cystic pancreatic lesions in the general population on MRI corresponds to autopsy studies.
Prospective follow-up data in a population-based setting suggest that most pancreatic cysts are harmless incidental findings.
The true weighted incidence of pancreatic cysts above the size of 2 mm in the general population is 2.6% and dependent on age. Only 6% of cysts are detected with a size of more than 1 cm.
The risk of malignant transformation of an incidental pancreatic cyst in the general population is minimal as is the value of a pancreatic cyst as an indicator lesion for pancreatic cancer.
How might it impact on clinical practice in the foreseeable future?
Against the background of remaining controversies concerning the management of incidentally detected pancreatic cysts, a restrictive therapeutic and follow-up approach can be supported.
Screening of the general population for pancreatic cystic lesions to reduce the risk of malignant transformation and to reduce the burden of pancreatic cancer cannot be recommended.
Introduction
Cystic lesions of the pancreas are closed cavities containing liquid or semisolid material, which can either be neoplastic or non-neoplastic. Among the neoplastic cysts accounting for 10%–15% of all pancreatic cystic lesions,1 the serous type is seen as benign, whereas the mucinous form tends to have malignant potential.2 Reports indicate that common cystic tumours with a mucinous epithelial lining can harbour carcinoma in situ or invasive cancer in up to 60% of resected specimen depending on the size of the lesion, clinical symptoms caused by the lesion as well as signs of malignancy on imaging.3–6 However, the rate of malignancy is variable and precise risk assessment can only be given for an individual patient and should be based on current guideline recommendations.7–10 Most common are intraductal papillary mucinous neoplasms (IPMN), mucinous cystic neoplasms (MCN) and serous cystic neoplasms, while solid pseudopapillary neoplasms are a rarity. Together these four types represent 90% of premalignant pancreatic primarily cystic tumours.11 12 In contrast, non-neoplastic cysts, which constitute the majority of cysts, are mostly of inflammatory or dysontogenetic origin.
Pancreatic cysts represent a small yet increasingly detected entity of pancreatic abnormalities.2 Approximately 70% of pancreatic cystic lesions are discovered incidentally.13 14 A variety of diagnostic methods to detect cystic lesions and to clarify their nature, such as MRI with supplementary cholangiopancreaticography (MRCP), CT or endoscopic ultrasound (EUS) in combination with fine needle aspiration, exist. MRI is the preferred non-invasive imaging modality for assessing pancreatic pathologies because of its high soft tissue contrast. In addition, strong T2-weighted MRI like MRCP allows an improved detection of cystic lesions including septa, mural nodules and ductal communication.15 16 Overall, discrimination between different cyst types tends to be difficult, with an accuracy of cross-sectional imaging of 39.5%–46%.16 17 Final diagnosis can often only be made on the basis of follow-up examinations, histopathological processing after biopsy or postresection.
The prevalence of pancreatic cysts varies extremely with the mode of imaging used and among different studies. In an ultrasound study pancreatic cysts were only detected in 0.21% of the subjects.18 On CT scan, pancreatic cysts were found in 2.6%,19 whereas their prevalence detected by thick-slice MRI ranges from 13.5% to 19.6%.20–22 Autopsy studies, on the other hand, revealed a much higher number of pancreatic cysts up to 50% in an elderly population.18 23 24
Although in most cases pancreatic cysts are asymptomatic, their presence is a known independent predictor of pancreatic cancer.25 The discrimination between benign and premalignant or malignant pancreatic cysts proves to be of high importance for patients in order to avoid unnecessary procedures, such as radiological follow-up examinations or surgical resection. In this context, longitudinal studies are essential to improve diagnostic techniques for early diagnosis and to establish evidence-based management algorithms and understanding the clinical relevance of incidentally detected cystic pancreatic lesions.
Therefore, the purpose of this study was to assess the prevalence of incidentally detected pancreatic cysts in the healthy population in contrast to previous studies on patients, and to investigate their incidence and clinical outcome by assessing pancreatic mortality risk in a prospective longitudinal approach.
Materials and methods
Study population
Subjects were recruited from the Study of Health in Pomerania (SHIP). SHIP is a prospective, population-based cohort study in Northeast Germany with the objective to rate the prevalence and incidence of diseases, as well as to analyse associations between risk factors, subclinical disorders and manifest affliction.26 27 The baseline cohort SHIP-0, conducted between 1997 and 2001, comprised a representative sample of 4310 participants from a total population of 212 157 inhabitants.27 All participants from SHIP-0 were invited to a 5-year follow-up (SHIP-1) between 2002 and 2006. The underlying data of this study were derived from SHIP-2 (examination period 2008–2012), when whole-body MRI including MRCP was first offered as part of the investigational protocol. SHIP-2 is the 10-year follow-up of the SHIP cohort, in which 2333 of the initial 4310 subjects agreed to participate. From the SHIP-2 cohort, MRI and MRCP were accepted upon informed consent by 1275 subjects (response rate 54.7%). Analysis could be performed on 1077 subjects. In 165 cases MRI examination was prematurely terminated by the probands. Twenty-seven subjects had to be excluded because of missing data sets or correlation factors. In six participants MR images were of non-diagnostic quality. An overview of the study design is presented as flow chart in figure 1.
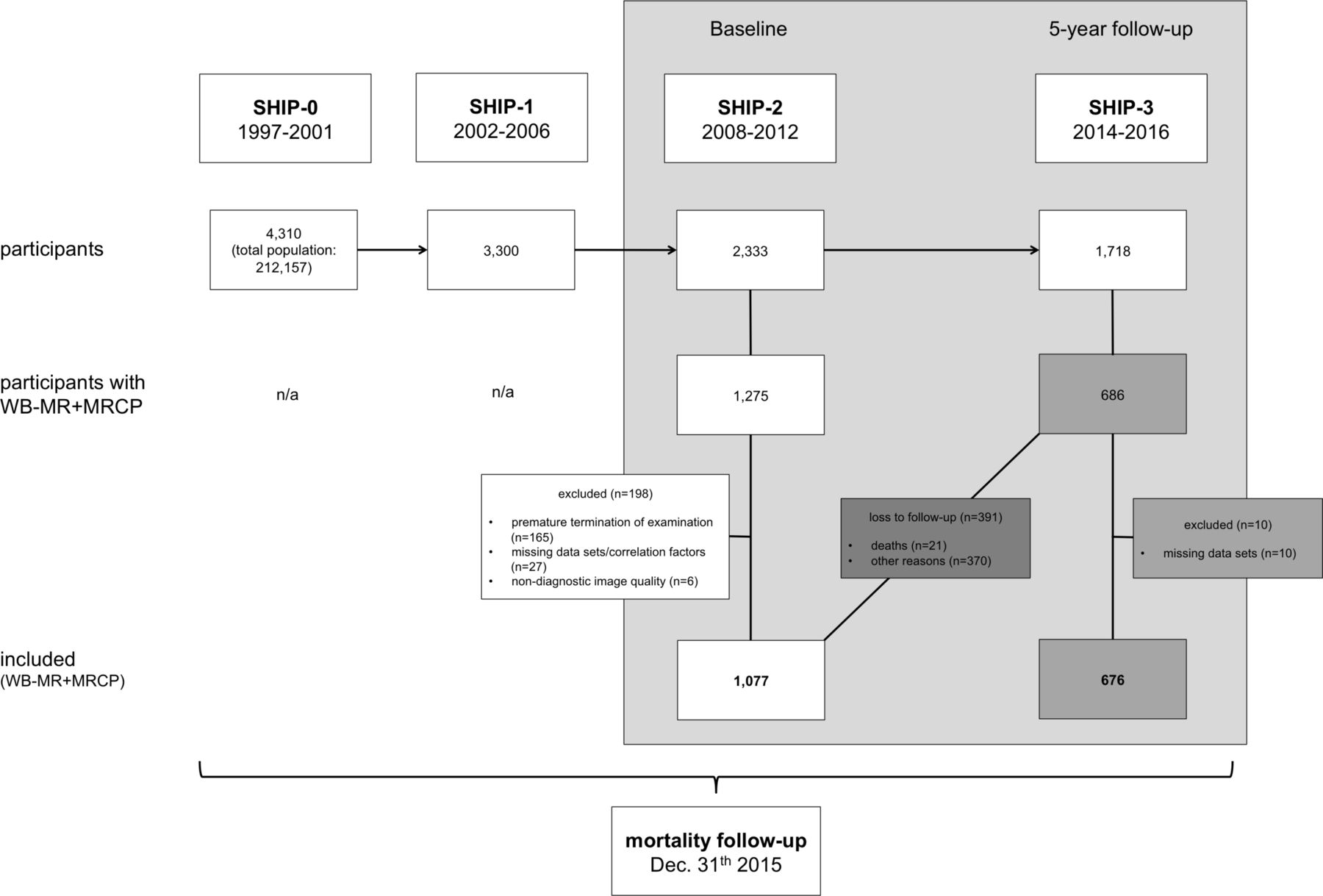
Study flow chart. MRCP, magnetic resonance cholangiopancreaticography; SHIP, Study of Health in Pomerania; WB-MR, whole-body magnetic resonance imaging.
The 5-year follow-up SHIP-3 started in 2014 and finished in March 2016. Out of 2333 possible participants from SHIP-2, 1718 subjects consented on a follow-up examination. From the 1077 subjects with previous MRI and MRCP, 686 agreed on follow-up examination (response rate 63.7%, mean follow-up period 4.8 years, range 2.7–7.5 years). From those, final analysis was performed on 676 volunteers; 10 participants were excluded because of missing data sets.
SHIP was approved by the institutional review board and written informed consent was secured from each participant. In addition, the associated project ‘Incidental Pancreatic Cysts in General Population’ was approved by the SHIP scientific advisory board (SHIP2012/69/D).
Mortality follow-up
Information on vital status of the whole SHIP cohort was collected at regular intervals from the time of study enrolment until 31 December 2015, and participants were censored at death or loss to follow-up. The local health authority provided death certificates, which were then coded by a certified nosologist according to the 10th revision of the International Classification of Disease. For the conducted substudy on pancreatic cysts, collected data were searched for the codes C25.0-9 (cancer of the pancreas) and K86.0-9 (other diseases of the pancreas). A mortality follow-up of all enclosed participants of SHIP was performed on 31 December 2015, including all volunteers recruited for MRI and MRCP (mean mortality follow-up period 5.9 years, range 3.2–7.5 years).
MRI
Whole-body MRI was performed using a 1.5 Tesla Magnetom Avanto (Siemens Healthcare, Erlangen, Germany) with a 280 mT/m gradient. The protocol has previously been described by Hegenscheid et al 28 and included a navigator-gated, strong T2-weighted, three-dimensional, turbo, spin-echo MRCP. The MRCP was acquired in a thin-slice technique and the postprocessing included an automated maximum-intensity projection reconstruction in coronal orientation. The following were the imaging parameters for MRCP: TR (resonance time)=~900 ms (adapted to navigator-triggered data), TE (echo time)=742 ms, bandwidth: 260 Hz/pixel, matrix: 384×384×44, slice thickness=1.5 mm.
Image analysis
Image analysis was performed using OsiriX V.4.6 (Bernex, Switzerland). One certified observer with 1 year of experience in abdominal radiology scrutinised the images of each participant for pancreatic cysts. For this purpose, the pancreatic duct was localised and strong T2-weighted hyperintense lesions with a diameter of 2 mm or more within the pancreas were assessed. In addition, observer 1 and a second observer with more than 12 years of experience in abdominal radiology re-evaluated a convenient sample of 72 MRI examinations to determine the interobserver and intraobserver reliability, accordingly. Remeasurements by observer 1 were undertaken after a period of 6 months.
For data analysis, cysts were categorised according to their number and diameter of the largest cyst during baseline and 5-year follow-up examination.
Clinical associations
All participants of the SHIP cohort answered standardised questions about their health status and lifestyle factors. Furthermore, blood samples were taken and analysed according to a preset protocol.26 From these data, information on body mass index (BMI), smoking status, serum lipase level, haemoglobin A1c (HbA1c), diabetes and alcohol consumption during the last 30 days of all participants were retrieved and used for correlation analysis.
These variables were selected, as they in our opinion constitute an influence on pancreatic diseases. Dependency of pancreatic cyst prevalence on gender was analysed, as the prevalence for specific cystic lesions of the pancreas, such as MCN, serous cyst adenomas or solid papillary neoplasia, is more prone in women, while IPMNs are equally distributed between gender. BMI, HbA1c and diabetes were investigated as metabolic syndrome might predispose to an attack of acute pancreatitis with residual cysts. Subclinical increase of lipase level is associated with blood group B, which also predisposes to chronic pancreatitis.29 Furthermore, smoking and alcohol are risk factors of chronic pancreatitis frequently associated with cyst occurrence.
Statistics
To evaluate the quality of our data, interobserver and intraobserver reliability was calculated by using kappa statistics. Hereby, a value below 0.20 defines disagreement, 0.20–0.40 poor agreement, 0.41–0.60 moderate agreement, 0.61–0.80 good agreement and over 0.80 excellent agreement.
All analyses were weighted for the whole study population in SHIP at baseline. For this we used two inverse probability weights multiplicatively. The first weight describes the dropout from baseline SHIP to SHIP-2, and the second weight describes the dropout from the core examinations to the MRI examinations in SHIP-2. To calculate these weights we used the predictions from logistic regression models with participation (yes/no) as outcome, and age, sex, BMI, HbA1c levels, diabetes, lipid levels, smoking status and income as explanatory variables.
First we present descriptive statistics of the sample by the presence of cystic lesions. Data are described as absolute numbers and percentages or as means and SD. The total number of pancreatic cysts in one person was counted and assigned into the following groups: 1–5, 6–10, 11–20 and >20. Furthermore, the diameter of the largest cyst in one subject, ranging from 2.00 to 5.00 mm, 5.01–10.00 mm, 10.01–20.00 mm and >20 mm, was assessed.
Prevalence of cyst occurrence, cyst number and cyst size were reported stratified by sex and the age groups <30, 30–39, 40–49, 50–59, 60–69, 70–79 and ≥80 years. Comparisons between the groups were calculated using χ2 test and Wilcoxon test. The associations between putative risk factors and cyst occurrence, number and size were assessed using age-adjusted and BMI-adjusted multivariable Poisson and linear regression models. Furthermore, we examined changes in the size and number of cyst size. An increase was defined as a rise in cyst size of at least 1 mm or in number of one additional cyst. Decrease was set as decline in cyst size of more than 1 mm or of one cyst less in number. Age and sex were associated with incident cyst occurrence by Poisson regression. In all analyses a p<0.05 was considered as statistically significant. All analyses were carried out by Stata V.14.2.
Results
MR images of 1077 subjects who received an MRCP examination were examined at baseline. Six hundred and seventy-six subjects received a 5-year follow-up. Gender distribution of included subjects in SHIP-2 was as follows: 521 men (48.4%) and 556 women (51.6%) with a mean age±SD of 55.8±12.8 years. Participants of the pancreatic substudy included in SHIP-3 encompassed 325 men and 351 women (figure 1).
Interobserver and intraobserver reliability
The interobserver agreement with regard to the presence of pancreatic cysts was excellent with kappa=0.9305 (SE 0.0832). Concerning the quantity and size of pancreatic cysts (>2 mm), the mean difference ±SD between both observers was found to be 0.04 (−1.66; 1.73) and −0.18 (−2.16; 1.81), respectively.
The intraobserver variability exhibited an excellent agreement of kappa=0.9442 (SE 0.0833) for the presence of cysts and a mean difference in cyst number of −0.01 (−1.24; 1.23) or size of −0.27 (−2.06; 1.55).
Pancreatic cysts at baseline
Among the 1077 probands screened at baseline examination, a total of 1681 cysts >2 mm were detected in 494 subjects. Characteristics of the study population overall and of the subgroups with/without pancreatic cysts at baseline are presented in table 1. Subjects with cystic lesions appeared to be older and presented with higher BMI and diagnosis of diabetes than those without.
Characteristics of the study population at baseline
The weighted prevalence of pancreatic cysts weighted for dropout of SHIP-2 and MRI examination was 49.1%. Of those 81.1% (n=416) showed a total cyst number of 1–5 (table 2). Only 13.0% (n=55) had 6–10 cysts, 3.8% (n=18) 11–20 and a minority of 2.2% (n=5) more than 20. When measuring the size of the largest cyst within one individual, 63.6% (n=335) of the 494 subjects carrying pancreatic cysts had cysts <5 mm, 30.6% (n=133) had cysts ranging between 5.01 and 10 mm, 5.1% (n=23) between 10.01 and 20.00 mm, and only 0.7% (n=3) >20 mm. The average number of cysts in the subgroup of participants harbouring cysts was 3.9 (95% CI 3.2 to 4.5), with a mean size of the largest cyst of 5.20 mm (95% CI 4.85 to 5.56 mm).
Occurrence and phenotype of pancreatic cysts at baseline
The presence, number and maximum size of cysts among the different age groups were analysed and are explicitly displayed in online supplementary table 1. The data collected showed a mounting cyst occurrence with increasing age (p<0.001). The highest prevalence was seen in subjects >80 years with 75.7%, whereas those between 30 and 39 years harboured cysts in only 17.1%. Subjects carrying incidental cysts were approximately 9 years older (mean age 60.5±11.6 years) than those without (mean age 51.7±12.3 years).
Supplementary file 1
In addition, a significant correlation could be seen between age and cyst count (p=0.001). Above 80 years, individuals exhibited a mean number of 7.6 (95% CI 2.7 to 12.4) cysts, and between 30 and 39 years a mean number of 1.4 cysts (95% CI 1.0 to 1.7).
Likewise, maximum cyst size increased with age (p<0.001). Subjects of 30–39 years had a mean diameter of the largest cyst of 4.29 mm (95% CI 1.92 to 6.65 mm), which increased up to 6.78 mm (95% CI 5.49 to 8.08 mm) in over 80-year-old probands. The association of prevalence, mean cyst number and mean maximum cyst size with age is depicted in figure 2.

Prevalence of pancreatic cyst occurrence, mean cyst count and mean size of the largest cyst according to age. Model-based prevalence estimates (A), mean cyst count (B) and mean size of the largest pancreatic cyst (C) increased significantly with age.
The prevalence of pancreatic cysts did not depend on gender (p=0.220), with 51.2% (260/556) detected in women and 46.8% (234/521) in men. Men displayed a mean cyst number of 3.8 (95% CI 3.2 to 4.4) and women of 3.9 (95% CI 2.8; 5.0). The mean cyst number (p=0.876) did not differ significantly with regard to sex. Likewise, the mean size of the largest cyst showed no gender-related significance, with 4.97 mm (95% CI 4.53 to 5.41 mm) in men and 5.40 mm (95% CI 4.86 to 5.95 mm) in women (p=0.223).
Concerning the BMI, a significant association was detected with regard to prevalence (p=0.013), but not concerning cyst number (p=0.874) or cyst size (p=0.983).
Furthermore, the prevalence of pancreatic cysts was analysed with regard to other potential risk factors. In this context, no correlation could be seen concerning smoking status, lipase level, HbA1c, diabetes or alcohol consumption during the last 30 days, and these had no impact on the development of pancreatic cysts. The risk ratio and p values of potential risk factors for the presence of pancreatic cysts unadjusted and adjusted for age and BMI are displayed in table 3. Unadjusted and adjusted values in relation to cyst number and cyst size are provided in online supplementary tables 2 and 3, where adjusted p values showed no significant association between any risk factor and cyst number or maximum size.
RR of potential risk factors for the presence of pancreatic cysts unadjusted and adjusted for age
Pancreatic cysts on follow-up
From the 676 participants with analysable diagnostic MRCP undergoing 5-year follow-up, 52.7% (n=345) showed pancreatic cysts on follow-up. Among the 367 subjects, who were cyst-free at baseline, 48 exhibited lesions on follow-up examination, revealing a weighted 5-year incidence of pancreatic cysts of 12.9% (2.6% per year). In 12 participants (1.6%) detected lesions of the preceding MRI had disappeared on the subsequent examination. No significant association was found between incidence of pancreatic cysts and age (p=0.203), gender (p=0.900) or BMI (p=0.633). Figure 3 gives an example of pancreatic cysts detected on MRI during baseline examination and their development on follow-up for one subject.

{kind=link}
{kind=link}
{kind=link}
Example of pancreatic cysts detected by MRI. Maximum intensity projection of magnetic resonance cholangiopancreaticography of the pancreas during baseline (A) and 5-year follow-up examination (B) shows increase in cyst number (exemplary white arrow) and size (exemplary red arrow).
Of those participants with pancreatic cysts at baseline and MRCP at follow-up, 172 (49.8%) showed an increase in maximum cyst size, whereas no change or a decrease occurred in 175 subjects (50.2%) (table 4). The total number of cysts increased in 128 participants (35.9%) during follow-up, but was stable or declined in 229 (64.2%). In summary, 1.3% (5/357) of the cases showed a decrease both in cyst size and frequency, 30.8% (114/357) displayed no change in cyst appearance, and 24.1% (87/357) showed an increase in number and diameter of the cystic lesion over time of follow-up.
Lesion change during 5-year follow-up
When looking at group categorisations enclosing all participants, subjects with no cysts at baseline showed a mean increase in cyst number of 0.2 (SD 0.65), and subjects with 1–5, 6–10, 11–20 and >20 cysts at baseline displayed an increase of 0.38 (SD 1.32), 0.32 (SD 1.65), 2.4 (SD 4.95) and 0.0, respectively, in follow-up examination. Stratified for those subjects with increase in cyst number, the mean increase was 1.54 (SD 1.09), 2.15 (SD 1.48), 2.29 (SD 1.11) and 4.80 (SD 6.38) for the subgroups none, 1–5, 6–10, 11–20 and >20, respectively.
The size of all pancreatic cysts between baseline and follow-up examination exhibited a mean increase of 0.45 mm (SD 1.29) in participants without cystic lesions at baseline, 0.39 mm (SD 1.61) in the group with 2.00–5.00 mm, 0.29 mm (SD 2.46) in the group with 5.01–10.00 mm, 1.17 mm (SD 2.58) in the group with 10.01–20.00 mm and 16.00 mm (SD 11.31) in the group with >20.00 mm measuring pancreatic cysts. Taking only those cysts with an increase in size during follow-up into account, a mean increase of 3.43 mm (SD 1.58, group without cysts at baseline), 1.51 mm (SD 1.23, group 2.00–5.00 mm), 2.15 mm (SD 1.81, group 5.01–10.00 mm), 2.63 mm (SD 1.55, group 10.01–20.00 mm) and 16.00 mm (SD 11.31, group >20.00 mm) was detected. A detailed analysis of cystic lesion change in the different subgroups is depicted in online supplementary tables 4 and 5.
Mortality follow-up
Of the 2333 participants of SHIP-2, three subjects died of pancreatic cancer within the period of mortality follow-up. Two of them did not consent to MRI; thus, an evaluation concerning an association between pancreatic cysts and tumour development could not be delineated. The third subject received an MRCP in the course of SHIP; however, at that time point neither signs of tumour nor cystic lesions could be detected. Apart from that, no deaths related to other pancreatic disorders were recorded within the study cohort.
Discussion
This study assessed the prevalence and incidence of pancreatic cysts detected as incidental finding on population-based MRI in order to analyse their progression and potential clinical relevance. Pancreatic cysts are common incidental findings with a prevalence of 49.1% and an incidence of 12.9% during 5-year follow-up according to our study. Analysis of subjects’ demographics showed a strong association between pancreatic cysts and subjects’ age. Based on data from death certificates on mortality follow-up, no death was attributed to pancreatic disease in subjects harbouring pancreatic cysts on previous imaging. However, two subjects within the study, who died of pancreatic cancer, declined to take part in the study MRI/MRCP examination. This as well as the small number of pancreatic ductal adenocarcinoma cases precludes a statement from our data on the role of cystic lesions as indicator lesions for pancreatic cancer. The expected age-adjusted 5-year pancreatic cancer prevalence in our cohort with respect to data from the German cancer registry was calculated with 3.7 cases, and thus our findings are within the expected range.
The incidental finding of pancreatic cysts has become a more and more pressing issue over the last years. On the one hand, advances in high-resolution, cross-sectional imaging technology and facilitated access make their detection more frequent.19 20 30–33 At the same time, management algorithms remain highly controversial in the absence of high-quality controlled studies, a recent example being the American Gastroenterological Association guidelines.22 Data for the prevalence of pancreatic cysts in asymptomatic patient cohorts range from as low as 0.21% up to 50% depending on the methods and means of detection.18 23 24 Compared with the literature,18–22 we found a high prevalence of pancreatic cysts of 49.1%—a frequency previously reported by autopsy studies.18 23 24 This result may be due to a better image quality of thin-slice MRI compared with other techniques such as CT or EUS, as well as the low cut-off value chosen for cyst detection of 2 mm in this study.
In SHIP we demonstrate both an increase in prevalence, number and mean size of pancreatic cysts with age, confirming several other studies.19 21 23 A correlation with gender, in accordance to Lee et al 21 and Zhang et al,20 could not be detected. Moreover, no association with risk factors for chronic pancreatitis, such as alcohol or nicotine abuse, was seen. However, cyst occurrence was related with BMI, a finding supported by a study by Mizuno et al,34 who found an association between pancreatic cysts and metabolic syndrome. The implication of that relation is still unclear and should be explored in more detail.
Although asymptomatic in most cases, pancreatic cysts do not necessarily have to be harmless. In a previous MRI study, 5.7% of the patients carrying pancreatic cysts showed concomitant malignant pancreatic tumours and 26.5% suffered from pancreatitis.20 Fernández-del Castillo et al 31 found in a retrospective study on patients that 3.5% of asymptomatic cysts <2 cm harbour malignant potential, and 26% of those >2 cm. The presence of pancreatic cysts is therefore seen as an independent predictor of pancreatic cancer.25 In our study cohort, 0.7% (n=3) of all persons carrying pancreatic cysts showed a cyst size above 2 cm, possibly posing them at higher risk of developing cancer.
The detection of pancreatic cancer in a curable stage proves to be difficult—at the time of diagnosis more than 80% of patients show metastasis, or the tumour is locally advanced and beyond resection,35 with a 5-year survival for all stages of 5%.36 In our study, none of the subjects harbouring cysts died during the observation period or developed pancreatic cancer on imaging during follow-up. Furthermore, the three subjects with a cyst >2 cm did not develop pancreatic cancer or other pancreas-related disease. Taken together, this suggests a rather low clinical relevance of incidentally found pancreatic cysts in a population-based setting. Population-based screening should thus not be recommended.
Early resection of pancreatic adenocarcinoma and its precursors might reduce mortality. However, because of the inherent risks of surgical treatment, the detection and evaluation of premalignant pancreatic cysts prove to be of high importance for patients in order to avoid unnecessary invasive treatment. Unfortunately, preoperative diagnostic accuracy in differentiating malignant from benign lesions remains challenging.37 Several societies provide opposing guidelines on the appropriate management of pancreatic cysts.7 22 38 39 Whereas in past years many recommended complete resection of all cysts, more recent guidelines suggest relaxing follow-up and refrain from surgical treatment, which is supported by our data. Similar problems exist concerning the optimal interval for follow-up examinations. Recommendations by consensus conferences envision a 6–12 months of follow-up.7 40 Other authors, however, suggest imaging at the earliest after 2 years in lesions <2 cm in size. Because of the relatively low overall likelihood of cyst progression, our data also support a longer interval of surveillance.
A well-known clinical dilemma in the treatment of pancreatic cysts is the difficulty to non-invasively clarify their nature. Thus a final diagnosis on cyst aetiology cannot be made from imaging in a population-based setting, as reported here. However, autopsy studies show that the prevalence of IPMN in cystic pancreatic lesions is approximately 20%, while normal epithelium can be detected in 47.5%.23 The prevalence of MCN of all cysts detected cannot be retrieved from the literature and autopsy reports would harbour a huge bias, as those lesions are usually operated on earlier in life. A rough estimate from the literature is given with 2% of all cystic lesions.41 Regarding these data we expect, although we cannot prove this, that a huge proportion of the small cystic lesions detected in our study are dysontogenetic, which are harmless and do not harbour malignant potential. In our view cysts below the size of 1 cm can be ignored once it is proven that they do not rapidly grow on the first follow-up. We would like to emphasise that by investigating probands from a population-based study, we merely detect incidental findings but not symptomatic disease.
This study has several limitations. First, the study design is observational. Second, definitive histology and cyst morphology of the detected pancreatic cysts remain unknown. The strong T2-weighted MRI protocol allowed only the detection of pancreatic cysts, but no sufficient morphological categorisation with regard to worrisome features such as noduli or contrast enhancement of the septae. Further studies on patient cohorts are, therefore, necessary to determine and evaluate malignant cyst criteria. The primary aim of our study was to observe cyst development in a longitudinal approach. Third, the data concerning follow-up encompass only two-thirds of the baseline study population. Here increases in cyst number and size are also frequent, so this might be a risk factor, although there is no definite proof since further follow-up is pending. The mid-term risk of pancreatic cysts, therefore, appears to be low, but long-term risk cannot be concluded from the presented data—following studies with a longer time interval might reveal some cancer risk. Furthermore, since the baseline examination ran from 2008 to 2012 and the last mortality follow-up was performed in 2015, the mortality follow-up period for some individuals was only 3 years. However, since the majority of participants were examined beforehand, we think that conclusions concerning malignant cyst progression can still be drawn. Fourth, our study only assessed pancreatic cysts by using MRI. Other imaging techniques may offer additional morphological features for cyst assessment. Likewise, the minimum cyst size for detection was set at 2 mm, making misinterpretation possible. Fifth, the decision on such a low cut-off value provided data on the true prevalence of pancreatic cysts, which appear to be harmless in most cases. Since the mean cyst size was 5.20 mm, only 26 cysts were larger than 1 cm and 3 larger than 2 cm, the conclusions of our study mainly apply to small cysts. Whether recommendation can be given from our data for incidentally detected cysts in clinical practice remains to be proven. Our data, which also hold information on larger cyst sizes, suggest such benevolent character; nevertheless, further studies are needed to support this thesis. Sixth, we could not correlate our findings for high risk stigmata or worrisome features as suggested by the Fukuoka consensus.7 However, regarding the very low number of cysts above the size of 2 cm, it is unlikely that those criteria would have altered our conclusion. Finally, the study population was derived from a population-based study, so that patients with pancreatic disease, history of pancreatic surgery or known predisposition of pancreatic cysts were not excluded as was done in other studies.19 42
In conclusion, this prospective study detected an unexpectedly high prevalence of small-sized pancreatic cysts in healthy persons, which increased with age and BMI, but displays no correlation with other risk factors. The follow-up data showed a progress in one-third, suggesting that the mid-term risk of pancreatic cysts is low, but relation of any long-term risk cannot be concluded from the presented data. Against the background of remaining controversies concerning the management of incidentally detected pancreatic cysts, our study supports a restrictive therapeutic and follow-up approach for incidentally detected small pancreatic cysts.
Supplementary file 2
Supplementary file 3
Supplementary file 4
Supplementary file 5
References
Footnotes
JM and J-PK contributed equally.
Contributors J-PK, M-LK and RB conceptualised and planned the study. HV coordinated the SHIP study. J-PK, JH, CP and RB analysed the MR images. TI conducted the statistical analysis. J-PK, M-LK, JM and ML participated in discussions, and provided critical scientific input and analysis suggestions. M-LK, J-PK and JM wrote the manuscript.
Funding This work was supported by the Deutsche Krebshilfe/ Mildred-Scheel-Stiftung (109102), the Federal Ministry of Education and Research (BMBF GANI-MED 03IS2061A and BMBF 0314107, 01ZZ9603, 01ZZ0103, 01ZZ0403, 03ZIK012) and the European Union (EU-FP-7: EPC-TM).
Competing interests None declared.
Patient consent Obtained.
Ethics approval Institutional Review Board, University Medicine Greifswald.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it published Online First. Errors in the spelling of the author list have been rectified.