Article Text

Abstract
Objectives Interventional endoscopic ultrasonography (EUS) procedures are gaining popularity and the most commonly performed procedures include EUS-guided drainage of pancreatic pseudocyst, EUS-guided biliary drainage, EUS-guided pancreatic duct drainage and EUS-guided celiac plexus ablation. The aim of this paper is to formulate a set of practice guidelines addressing various aspects of the above procedures.
Methods Formulation of the guidelines was based on the best scientific evidence available. The RAND/UCLA appropriateness methodology (RAM) was used. Panellists recruited comprised experts in surgery, interventional EUS, interventional radiology and oncology from 11 countries. Between June 2014 and October 2016, the panellists met in meetings to discuss and vote on the clinical scenarios for each of the interventional EUS procedures in question.
Results A total of 15 statements on EUS-guided drainage of pancreatic pseudocyst, 15 statements on EUS-guided biliary drainage, 12 statements on EUS-guided pancreatic duct drainage and 14 statements on EUS-guided celiac plexus ablation were formulated. The statements addressed the indications for the procedures, technical aspects, pre- and post-procedural management, management of complications, and competency and training in the procedures. All statements except one were found to be appropriate. Randomised studies to address clinical questions in a number of aspects of the procedures are urgently required.
Conclusions The current guidelines on interventional EUS procedures are the first published by an endoscopic society. These guidelines provide an in-depth review of the current evidence and standardise the management of the procedures.
- endoscopic ultrasonography
- pancreatic pseudocyst
- biliary endoscopy
- pancreatic disease
Statistics from Altmetric.com
Introduction
Interventional endoscopic ultrasonographic (EUS) procedures have undergone tremendous development over the past two decades. The types of procedures have expanded from drainage of pancreatic fluid collections to tumour ablations, gallbladder drainage and enteric anastomosis. With the aim of providing a road map to guide industry and investigators on how to facilitate implementation of therapeutic EUS into clinical practice, the EUS Working Group identified five interventions as high priority for research to increase their adoption in clinical practice in 2008. These procedures were celiac plexus neurolysis and block, drainage of pancreatic fluid collections, hepaticogastrostomy, choledochoduodenostomy and ablation of pancreatic-cystic neoplasm.1
Since then, large numbers of publications have addressed various aspects of EUS-guided interventional procedures. The procedural techniques have evolved and EUS-specific devices aimed at improving the ease and safety of performing the procedures have also emerged. In order to further promote the safe adoption of these techniques, a set of practice guidelines addressing these changes in the most commonly performed interventional EUS procedures is required. The guidelines should address the indications for the procedures, technical aspects, pre- and post-procedural management, management of complications and competency and training. The aim of the current paper is to formulate these guidelines in a scientific manner based on the best available evidence.
Methods
The procedures examined in the current guidelines were chosen by the Asian EUS group as they represent the most commonly performed interventional EUS procedures. They include EUS-guided drainage of pancreatic pseudocyst, EUS-guided biliary drainage (EUS-BD), EUS-guided pancreatic duct drainage (EUS-PD) and EUS-guided celiac plexus ablation. The Asian EUS group comprises expert endosonographers from 18 countries in Asia with a primary focus on education and research in EUS. Formulation of the guidelines was based on the best scientific evidence available. However, the panel acknowledges the fact that evidence may be lacking in certain areas of the concerned procedure. Thus, the RAND/UCLA (research and development) Corporation and UCLA (University of California-Los Angeles) appropriateness methodology (RAM) was used, as it could combine the best scientific evidence with the collective judgement of experts to formulate the statements. After completion of the statements, the guidelines were then sent to the advisors of the group for comments and feedback.
RAM is a method of group consensus developed in the 1980s by RAND and UCLA. It is a well-established method for creating guidelines for over 50 conditions and procedures.2 RAM enables the measurement of overuse or underuse of medical and surgical procedures and has been applied to the development of practice guidelines.3–8 In RAM, the concept of appropriateness refers to the relative weight of the benefits and harms of a medical or surgical intervention. An appropriate procedure is one in which ’the expected health benefit exceeds the expected negative consequences by a sufficiently wide margin that the procedure is worth doing, exclusive of cost'. The method was driven by the concern that the increasing complexity of medical care was resulting in some patients not undergoing procedures that they needed, and others undergoing procedures that they did not need. The rationale behind the method is that randomised clinical trials—the ‘gold standard’ for evidence-based medicine—often are either not available or cannot provide evidence at a level of detail sufficient to apply to the wide range of patients seen in everyday clinical practice. Nevertheless, physicians will still need to make decisions every day about when to apply them. Consequently, it was believed a method was needed that would combine the best available scientific evidence with the collective judgement of experts to yield a statement regarding the appropriateness of performing a procedure at the level of patient-specific symptoms, medical history and test results. Measurement of necessity was not performed for these guidelines.
The RAM process is shown in figure 1. The process involves: (1) performing a literature search to determine the evidence for processes of care; (2) creating clinical scenarios or statements for treatment options; (3) assembling an expert panel to grade the appropriateness of treatments; and (4) evaluating all appropriate processes for necessity.9 A leader was assigned to each of the interventional EUS procedures in question. A detailed literature review was conducted to synthesise the latest evidence of a broad range of peri-procedural processes involved in the interventional EUS procedure in question by the respective leaders.10 11 Electronic literature searches were conducted using PubMed, Medline and Embase from 1 January 1992 to 31 December 2016. Searches were performed under the following aspects to generate the statements: indications for the procedure, the optimal approach, pre-procedural evaluations and preparations, procedural considerations, adjunctive treatments, management of complications, competency and training. Articles were selected using MeSH headings and text words related to the interventional procedure. For pseudocyst drainage, the text words used were: pancreatic pseudocyst, pseudocyst drainage, cystogastrostomy, cystojejunostomy, transmural pseudocyst drainage, transpapillary pseudocyst drainage and percutaneous pseudocyst drainage; for biliary drainage, the following text words were used: EUS-guided biliary drainage, percutaneous biliary drainage, transluminal biliary drainage, choledochoduodenostomy and hepaticogastrostomy; for pancreatic duct drainage the text words used were: EUS-guided pancreatic duct drainage, pancreatic ducts and pancreatic duct intervention; and for celiac plexus ablations the following search terms were used: endoscopic ultrasound, celiac plexus block, celiac plexus neurolysis, chronic pancreatitis and pancreatic cancer. Only English language studies involving the concerned treatment approaches were included and comparative studies were preferred. Reference lists from eligible trials were also checked to locate missing publications. The titles of the articles and abstracts located were evaluated by the leader of the group and a member of the procedure. Where the article fulfilled the selection criterion, a copy of the full manuscript was obtained. Full manuscripts were then reviewed and a final decision was made about inclusion. Studies published only in abstract form, conference abstracts, symposium proceedings and case reports were not eligible for inclusion. Any disagreements were resolved by consensus. The same methodology was used for each interventional procedure in question for this manuscript and several reviews have also been published by the Asian EUS group.10–13

The RAM process.
Panellists on the voting panel were recruited through solicitation of nominations from the Asian EUS group which comprises experts in surgery, interventional EUS, interventional radiology and oncology from 11 Asian countries (table 1). Between June 2014 and October 2016 the panellists met in meetings to discuss and vote on the clinical scenarios for each of the interventional EUS procedures in question. For each statement, the panellists were asked to score the appropriateness of the management in each scenario. Appropriateness was scored from 1 (highly inappropriate) to 9 (highly appropriate). The data were analysed for areas of agreement and disagreement. Agreement was met when ≤4 panellists rated outside the 3-point region containing the median (ie, 1–3, 4–6, 7–9). Disagreement occurred when ≥4 panellists rated in each extreme 3-point region (ie, 1–3, 7–9). Discussions were focused on areas where there was disagreement. Statements were rewritten for clarification based on discussions and recommendations from the expert panel if there was disagreement. In statements where consensus could not be achieved, they were deleted from voting. All scenarios were re-voted for appropriateness by each panellist until agreement was obtained. In the final analysis, a procedure was classified as appropriate if the median rating was 7–9, with agreement; inappropriate if the median rating was 1–3, with agreement; and uncertain if the median rating was 4–6, with agreement. The level of agreement was indeterminate when it failed to satisfy either of these criteria. When there was agreement that the scenario was appropriate, it was then scored for necessity in the same manner. The final level of agreement reflects the median appropriateness scores and the dispersion of the scoring (reflected by the mean absolute deviations from the median). For pseudocyst drainage and pancreatic duct drainage, four rounds of revisions of the statements were required to reach an agreement for each procedure; for celiac plexus ablations, five rounds of revisions were required; and biliary drainage required seven rounds of statement revisions. The statements of each of the interventional EUS procedures are presented here. For each of the statements, the evidence supporting them was graded according to the approach as suggested by the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) Working Group.14 The quality of evidence was rated high when we were very confident that the true effect lies close to that of the estimate of the effect; it was rated moderate if we were moderately confident of the effect estimate; it was rated low if our confidence estimate was limited and very low if we had very little confidence in the effect estimate.
Expert Panel members, specialty and hospital affiliation
Results
Consensus statements on the optimal management of EUS-guided pancreatic pseudocyst drainage
Consensus statements on the optimal management of EUS-guided pancreatic pseudocyst drainage are shown in table 2.
Consensus statements on the optimal management of endoscopic ultrasonography (EUS)-guided pancreatic pseudocyst drainage
Indications for the procedure
Statement 1
Acute pseudocysts should be drained if they persist for more than 4–6 weeks, have a mature wall and are ≥6 cm in size, causing symptoms or complications.
Statement is Appropriate (9.0)
Evidence level: Moderate
Supporting evidence and comments
Acute pseudocysts can occur in 6.3–35.5% of patients with acute pancreatitis.15–19 60% of acute pseudocysts that are <6 cm would resolve spontaneously and do not need treatment. Those ≥6 cm are associated with a higher risk of developing complications and more frequently require interventions.20 21 Time should be allowed for maturation of the cyst wall for drainage and this usually takes 4–6 weeks. Further delay in drainage beyond 8 weeks may increase the risk of developing complications.21 The presence of symptoms or an enlarging pseudocyst is correlated with the need for intervention. Complications from the pseudocyst can occur and include haemorrhage, infection, rupture, obstruction of the gastrointestinal tract and bile duct, and warrant intervention.22
Optimal approach for drainage
Statement 2
EUS-guided drainage is the optimal drainage approach in uncomplicated pseudocysts that are located adjacent to the stomach or duodenum.
Statement is Appropriate (9.0)
Evidence level: High
Supporting evidence and comments
Pancreatic pseudocysts can be drained by endoscopic, percutaneous and surgical approaches.10 23–33 Endoscopic approaches can be further divided into oesophagogastroduodenscopy (OGD)-guided or EUS-guided drainage. In a systematic review comparing the outcomes of various approaches, it was noted that surgical drainage appeared to reduce mortality and the adverse events rate compared with the percutaneous approach, while the EUS approach reduced hospital stay, cost and improved quality of life compared with surgery (table 3). EUS- and OGD-guided drainage were both feasible for pseudocyst drainage, but the success rate of the EUS approach was better for non-bulging cysts and the approach conferred additional safety benefits. The use of EUS improves the precision of drainage by allowing visualisation of extraluminal structures and intervening blood vessels. Results from two randomised trials and two retrospective studies are available. The studies employed EUS in different stages of the procedures.27–29 34 The EUS-guided approach was associated with significantly higher success rates in two studies.27 29 Differences in adverse events were not significant, but clinically significant bleeding was reported in one study resulting in one death and another requiring endoscopic haemostasis and blood transfusion.29
Studies comparing the outcomes of various approaches for pseudocyst drainage
Thus, EUS-guided drainage appeared to be advantageous in drainage of pancreatic pseudocysts located adjacent to the stomach or duodenum. In patients with unfavourable anatomy, surgical cystojejunostomy or percutaneous drainage could be considered. Similar findings were noted in another Cochrane review.23
Pre-drainage evaluation
Statement 3
Pre-drainage evaluation includes contrast-enhanced computed tomography (CECT) or magnetic resonance cholangiopancreatography (MRCP) and occasionally prior EUS to decide on the best approach for drainage.
Statement is Appropriate (9.0)
Evidence level: Moderate
Supporting evidence and comments
A pseudocyst usually develops posterior to the stomach, duodenum or towards the paracolic gutter. However, it can also form at atypical locations including the mediastinum, intrahepatic, intra/perisplenic, perirenal and pelvic areas.35–37 Hence, a CECT or MRCP is essential in delineating the anatomy. When available, MRI is preferred over CECT for depicting the presence of any solid debris within the pancreatic fluid collection.38 In addition, the use of EUS may sometimes be needed to assess the feasibility of endoscopic drainage and to assess the presence of intervening vessels.
Statement 4
Multidisciplinary involvement including an endoscopist, interventional radiologist and surgeons is required in complicated cases to decide on the best approach to drainage.
Statement is Appropriate (9.0)
Evidence level: Low
Supporting evidence and comments
EUS-guided drainage of pseudocysts offers high technical and clinical success rates. However, some situations may be challenging to the endoscopist and a multidisciplinary meeting would be useful to decide on the best approach for drainage. These include pseudocysts that are recurrent, at atypical locations, infected or bleeding. For pseudocysts that are not adjacent to the stomach or duodenum, surgical cystoenterostomy should be the subsequent choice of procedure.10 This could be done by laparoscopic or open means. Surgical resection may be indicated in patients with a bleeding pseudocyst or a recurrent pseudocyst due to disconnected duct syndrome. Laparoscopic cholecystectomy could be performed at the same operation. Percutaneous drainage may be indicated in ruptured pseudocysts or moribund patients who could not undergo endoscopic or surgical drainage.
Pre-procedural preparations
Statement 5
Prophylactic antibiotics are recommended and should be continued post-procedurally.
Statement is Appropriate (8.0)
Evidence level: Low
Supporting evidence and comments
There are no randomised controlled studies addressing the use of prophylactic antibiotics prior to pseudocyst drainage. There are also no data on whether antibiotics should be continued after the procedure and how long they should be continued. However, by draining the pseudocyst into the stomach, the endoscopist is converting a clean system to a clean-contaminated environment. Furthermore, given the low cost of antibiotics and infection being the most common complication after the procedure, provision of antibiotics before the procedure should be recommended. Available studies on the use of antibiotics mainly investigated their role in preventing infection of pancreatic necrosis and used different antibiotic regimes.39–45 These studies used high-dose second/third-generation cephalosporins or imipenem group antibiotics. A similar regime should be adopted as prophylactic antibiotics for pseudocyst drainage. Pseudocyst fluid should also be aspirated at the time of puncture to guide subsequent therapy if infection ensues. The Committee also agreed that antibiotics should be continued after the procedure, but the exact duration is uncertain. However, a period of 3–5 days after the procedure is common practice.
Procedural considerations
Statement 6
The use of fluoroscopy is recommended during EUS-guided pseudocyst drainage.
Statement is Appropriate (9.0)
Evidence level: Low
Supporting evidence and comments
EUS-guided pseudocyst drainage is a multi-step procedure involving puncturing of the cyst, track dilation and stent insertion. The use of fluoroscopy is essential for monitoring the position of the guidewire during looping within the pseudocyst and also stent placement. Although two studies have demonstrated the feasibility of performing the procedure under EUS guidance only, the Committee believes that the use of X-rays can provide another dimension of visual assessment during the procedure and improve safety without incurring additional risks.46 47
Statement 7
One or two plastic double pigtail stents should be inserted to maintain the patency of the cystogastrostomy after EUS-guided drainage.
Statement is Appropriate (8.0)
Evidence level: Moderate
Supporting evidence and comments
Until recently, plastic double pigtail stents were the standard stents used for pseudocyst drainage. These stents are cheap, safe and easily accessible.48 Technical and clinical success rates of over 90% have been reported.24 26 29 However, no randomised studies have addressed the optimal number of plastic stents that should be inserted. In a retrospective study, no difference in treatment success was found with respect to the size of stents (7 Fr vs 10 Fr: 87.7% vs 90.5%; P=0.766) or the number of stents (1 vs >1 stent: 88.9% vs 88.6%, P=0.999).49 On multiple logistic regression analysis, the stent size and number were also not predictors of the number of interventions required for treatment success. Thus, the endoscopist needs to exercise judgement on the likelihood of stent occlusion from cyst contents and decide if one or multiple stents is required.
Statement 8
The use of metallic stents for pancreatic pseudocyst drainage outside a clinical trial is not recommended.
Statement is Appropriate (7.0)
Evidence level: Moderate
Supporting evidence and comments
The use of self-expanding metal stents (SEMS) for pseudocyst drainage is increasingly reported.50–62 Metal stents may offer several potential advantages to drainage of pseudocysts, including improved drainage with a larger diameter stent, reduced risk of stent obstruction, direct endoscopic access to the collection, reduced number of instrumental changes and possibly reduced procedural time. The types of SEMS can be divided into straight tubular stents or EUS-specific double-flanged stents. The double-flanged stents can be further divided into lumen apposing (LAMS) and non-lumen apposing stents.63 EUS-specific stents possess design characteristics with EUS-guided deployment in mind. The stents are short, large diameter and bi-flanged to provide some anti-migratory properties. A further distinction on whether these stents are LAMS based on the strength of the lumen apposing force generated by the flanges was made. In theory, stents with a higher lumen apposing force can hold two non-adhering lumens together better and reduce the chance of leakage or stent migration. However, as described in a study below, such high lumen apposing force may also be a potential cause for adverse events. Hence, whether LAMS are more beneficial than non-LAMS is still controversial. Furthermore, there is no accepted definition on what properties LAMS should possess.
There are currently no randomised data on how metal stents compare with plastic stents for pseudocyst drainage. A distinction between the outcomes of SEMS for pseudocysts and walled-off pancreatic necrosis (WOPN) should also be made. In a systematic review, no differences in technical and clinical success were noted.48 Studies that used tubular SEMS reported an adverse events rate of 0–44.4%.50–54 The types of adverse events encountered included bleeding, infection and stent migration. On the other hand, the reported adverse events rates of double-flanged stents in pancreatic pseudocysts ranged from 6.7% to 11.1%.55–61 In a recent report of an ongoing randomised trial assessing the role of LAMS for WOPN, serious adverse events including delayed bleeding, buried stent syndrome and biliary stricture were observed in up 50% of the recruited patients.62 Hence, there is currently no place for the use of metal stents for pseudocyst drainage. In addition, any benefits arising from the use of SEMS will need to be balanced against the increased cost of the device, as a recent publication concluded that the use of LAMS is more expensive than plastic stents without significant differences in outcomes.
Statement 9
The risk of pseudocyst recurrence may be increased in patients with pancreatic ductal disruption.
Statement is Appropriate (9.0)
Evidence level: Moderate
Supporting evidence and comments
The development of pancreatic fluid collections is related to the disruption of the pancreatic duct with extravasation of pancreatic juice. The presence of main pancreatic duct disruptions was more often seen in patients with pancreatic necrosis and the finding was associated with a longer hospital stay.64 65 Pancreatic duct disruptions can be classified into complete or partial. A partial duct disruption is present when part of the duct wall is still in continuity and is signified when the main pancreatic duct is opacified upstream from the disruption site during endoscopic retrograde cholangiopancreatography (ERCP). Complete disruption is signified as an abrupt cut-off and/or extravasation of injected contrast medium without filling of the upstream pancreatic duct during ERCP.66
In one study, complete disruption was more frequently associated with >50% necrosis and full-thickness glandular necrosis compared with partial disruption.66 The success rate of endoscopic transpapillary pancreatic stenting across the stricture site was also lower in complete disruption (20% vs 92%, P=0.01). Patients with complete main pancreatic duct disruption also showed a higher rate of pancreatic fluid collection recurrence (71% vs 17%, P=0.003) and required surgery more often (43% vs 6%, P=0.027).
Adjunctive treatments
Statement 10
The insertion of a pancreatic ductal stent is suggested in patients with partially disrupted pancreatic ducts.
Statement is Appropriate (8.0)
Evidence level: Moderate
Supporting evidence and comments
The use of pancreatic duct stenting as a treatment for persistent pancreatic duct leak was reported in several studies.66–76 Most of the studies consisted of a small number of patients and the success rate in achieving permanent resolution of the leak was 50–88%. A distinction between partial and complete pancreatic duct disruptions was made in five studies.66 69–71 73 In two studies, a stent that bridged the disruption correlated with a successful outcome.69 70 The success rate of placing a pancreatic stent was significantly lower in patients with complete disruption compared with partial disruption (20% vs 92%, P=0.001).66
Statement 11
The use of nasocystic catheters is recommended in large or infected pseudocysts.
Statement is Appropriate (8.0)
Evidence level: High
Supporting evidence and comments
The use of a nasocystic catheter in conjunction with transmural stenting was reported in four studies, three in pseudocysts and one in walled off pancreatic necrosis.77–81 The nasocystic catheter is used to provide continuous irrigation and drainage of the cyst cavity in an aim to prevent or treat infection. The size of the catheter was 5–7 Fr. The volume of irrigation used was highly variable. One study used 50 mL of normal saline three times daily, another study irrigated 100 mL/hour of normal saline solution for 48–72 hours, and the volume was not specified in two studies. In the only randomised study that included pseudocysts of 10 cm or larger, the infection rates, hospital stay and resolution time of the pseudocyst were significantly lower with the use of nasocystic catheters.80 In the study on WOPN, the use of nasocystic catheters was associated with a lower risk of stent occlusion. Thus, the use of nasocystic catheters is suggested in large or infected pseudocysts.
Management of complications
Statement 12
Centres performing the procedure should have multidisciplinary support including interventional radiologist, surgeons and anaesthesiologist to prevent and manage complications.
Statement is Appropriate (9.0)
Evidence level: Low
Supporting evidence and comments
EUS-guided pseudocyst drainage is a relatively safe procedure with a risk of adverse events ranging from 0% to 34%.10 82 Most patients can be discharged within 1–2 days after the procedure. Nevertheless, severe life-threatening conditions can occur in patients who develop bleeding, infection or perforation. Bleeding can occur during creation of a transmural track or as a result of stent erosion.29 61 62 82 The condition has been reported with the use of plastic stents and SEMS. Prompt treatment by interventional radiology with angiographic embolisation is often required.83 Infection is usually due to an obstructed stent and requires endoscopic stent exchange. Perforation can occur when the transmural track is lost, and the condition is traditionally managed by surgery. However, recent advances in endoscopic accessories have allowed most perforations to be managed endoscopically by clipping or suturing.84 85 Thus, institutions performing the procedure should have facilities to manage these conditions.
Competency and training
Statement 13
Skills in EUS-guided pseudocyst drainage are best acquired through observation, followed by hands-on training in the porcine model and then performance of the procedure in patients.
Statement is Appropriate (7.0)
Evidence level: Moderate
Supporting evidence and comments
Data from the Asian EUS group workshops have shown that a dedicated training programme improves knowledge and skills in EUS.86 Observation of the procedure should best be in high-volume centres experienced in interventional EUS. Hands-on training should begin in the porcine model and trainees should familiarise themselves with the steps of the procedure and instruments that they are using.87 When proficiency is obtained in models, trainees should then perform the procedure under the supervision of an experienced endoscopist.
Statement 14
ERCP skills are beneficial to the endoscopist learning EUS-guided pseudocyst drainage and should be incorporated into the training programme.
Statement is Appropriate (9.0)
Evidence level: Low
Supporting evidence and comments
There is limited literature addressing this issue. However, since many of the instruments and techniques used in the procedure were borrowed from ERCP, the panel believes that proficiency in ERCP skills, although not essential, would be beneficial to endoscopists learning EUS-guided pseudocyst drainage.88
Statement 15
Performance of 5–10 supervised procedures is required to gain competency in EUS-guided pseudocyst drainage.
Statement is Appropriate (7.0)
Evidence level: Low
Supporting evidence and comments
The literature is also scarce in addressing this issue. Two studies have examined the impact on outcomes with increasing experience of the procedure.89 90 In one study it was observed that resolution rates and days to resolution were significantly improved after the first 20 procedures89 while, in another study, the procedural time was found to be significantly shorter after the first 25 procedures without differences in technical success, clinical success and adverse events rates.90 However, the Committee acknowledges that both of these studies were reported during the early development of the technique. The technique was still in evolution and endoscopists were performing the procedure without supervision. Hence, using current standards of performing the procedure and assuming that the endoscopist is competent in ERCP, a lower number of procedures would be required to attain competency. It was thus agreed that performance of 5–10 procedures under supervision is the minimum requirement to obtain competency. However, the learning curve of each trainee is different and each should be assessed individually to assess for their competency.
Consensus statements on the optimal management of EUS-guided biliary drainage (EUS-BD)
Consensus statements on the optimal management of EUS-guided biliary drainage (EUS-BD) are shown in table 4.
Consensus statements on the optimal management of endoscopic ultrasonography-guided biliary drainage (EUS-BD)
Indications for the procedure
Statement 1
EUS-BD is recommended as the procedure of choice for biliary drainage in patients with failed ERCP if expertise is available.
Statement is Appropriate (8.0)
Evidence level: High
Supporting evidence and comments
EUS-BD has emerged as an acceptable alternative in patients with obstructive jaundice and failed ERCP (table 5).91 Two meta-analyses have demonstrated EUS-BD to have high technical success in excess of 90% with adverse event rates in the range of 17–23%.92 93 A randomised study has shown EUS-BD to be superior to percutaneous transhepatic biliary drainage (PTBD) in expert hands in terms of adverse events and re-intervention rate.94 Procedure-related adverse events were 8.8% in the EUS-BD group compared with 31.2% in the PTBD group (P=0.022), while the mean frequency of unscheduled re-intervention was 0.34 in the EUS-BD group and 0.93 in the PTBD group (P=0.02). EUS-BD (choledochoduodenostomy) has also been compared with surgical hepaticojejunostomy in a small randomised trial.95 Technical and clinical success was comparable between the two groups. However, the procedural time of EUS-BD was significantly shorter (P=0.027), while no difference was observed in adverse events rates (P=0.651) and quality of life scores.
Randomised studies comparing EUS-guided biliary drainage (EUS-BD) versus percutaneous transhepatic biliary drainage and surgical bypass
Statement 2
EUS-BD is an alternative procedure to obtain biliary drainage in patients with altered postoperative anatomy or duodenal stenosis precluding ERCP if expertise is available.
Statement is Appropriate (8.0)
Evidence level: Moderate
Supporting evidence and comments
Approaching the papilla may be difficult or impossible in patients with duodenal stenosis or surgically altered anatomy with endoscopy. The success rate of ERCP in these situations is dependent on reaching the papilla, which may not be possible in up to 40% of patients.96 EUS-BD is a good alternative in such situations as the bile duct can be accessed from the proximal stomach. Available literature shows a high success rate of EUS-BD in patients with altered anatomy. However, prospective comparative studies with ERCP are lacking. A retrospective study comparing the approaches showed that EUS-BD was associated with better success rates, reduced procedural times but higher adverse events rates.97
Optimal approach for drainage
Statement 3
In patients with distal common bile duct obstruction, the transduodenal and transhepatic approaches for EUS-BD are used.
Statement is Appropriate (8.0)
Evidence level: Moderate
Supporting evidence and comments
A number of EUS-BD procedures are available. The same procedure may be named differently depending on the literature and a standardised nomenclature was not available.98 99 The Asian EUS group has recently suggested a nomenclature for EUS-guided biliary interventions (figure 2). The procedures include access procedures (rendezvous technique) and direct drainage procedures. Prior to EUS-BD, the endoscopist should have an algorithm on whether EUS-BD is used for access or drainage, or both. When performing EUS-guided rendezvous ERCP, EUS is only used in the initial part of the procedure for bile duct access and introduction of a guidewire through the papilla. The echoendoscope is then changed to a duodenoscope for retrieval of the guidewire to complete the procedure with ERCP.

Nomenclature for endoscopic ultrasonography (EUS)-guided biliary interventions.
In terms of access, the bile duct can be accessed by the transduodenal and transhepatic routes. Both approaches have been found to be effective provided that the ducts are adequately dilated. There is lack of clarity about the preferred route when both routes are feasible for puncture. Current data are conflicting, with some reports showing the transduodenal route to be safer while others show no difference.97 100
Direct drainage procedures can be transpapillary (antegrade stenting) or transluminal (choledochoduodenostomy (CDS) and hepaticogastrostomy (HGS)). For CDS, a fistula track is first created between the common bile duct and the first part of the duodenum for insertion of a stent. For HGS, a fistula is first created between the left intrahepatic duct and the stomach followed by insertion of a stent. There are also reports of stents placed between the right intrahepatic duct and duodenum, but the procedure is more technically demanding.101 In a small randomised study comparing 25 patients who received HGS and 24 who received CDS, the clinical success of HGS was higher (91% vs 77%) and the adverse events were also slightly higher (20% vs 12.5%), although neither outcome reached statistical significance.102
Thus, in patients with distal common bile duct obstruction, both procedures could be performed. The choice of the procedure is not clear, but depends on a combination of factors including technical expertise, stent patency, risk of adverse events and anatomical factors including presence of dilated bile duct or biliary radicals, duodenal stenosis and altered anatomy.
Statement 4
A transhepatic approach to EUS-BD is recommended for hilar blocks.
Statement is Appropriate (8.0)
Evidence level: Low
Supporting evidence and comments
Transduodenal stent placement in a patient with hilar obstruction is likely to be more challenging than transhepatic stent placement. The transhepatic approach is preferred, and drainage could be obtained with antegrade stenting or HGS. The risk of cholangitis increases when contrast is injected into undrained ducts and care should be taken to avoid excessive contrast injection.103 104
Pre-drainage evaluation
Statement 5
MRCP or CECT is recommended in patients with suspected hilar obstruction prior to the EUS-BD procedure.
Statement is Appropriate (9.0)
Evidence level: Very Low
Supporting evidence and comments
MRCP provides a roadmap for stent placement by delineation of the type of hilar obstruction and other relevant bile duct anatomy. Inadvertent contrast injection and/or manipulation in a non-dilated or non-drainable segment could result in cholangitis. Thus, it is considered prudent to obtain MRCP prior to intervention in patients with hilar obstruction. There are no data regarding the utility of a roadmap in EUS-BD, but it appears logical based on data available for ERCP.105 In patients with distal common bile duct obstruction, an ultrasound or CECT could be performed as initial investigations prior to EUS-BD.
Pre-procedural preparations
Statement 6
Antibiotic prophylaxis is recommended before the EUS-BD procedure.
Statement is Appropriate (9.0)
Evidence level: Moderate
Supporting evidence and comments
There are no studies demonstrating the efficacy of prophylactic antibiotics in patients undergoing EUS-BD. However, the procedure is similar to other biliary interventions like ERCP and PTBD with contrast injection and manipulation done in an obstructed biliary system, resulting in introducing and/or disseminating bacteria. The use of antibiotics was shown to prevent cholangitis, septicaemia, bacteraemia and pancreatitis in ERCP, particularly for obstructed systems.106 Thus, prophylactic antibiotics should be used in a similar manner. Antibiotics that cover biliary flora such as enteric gram-negative organisms and enterococci should be used (second-generation cephalosporin or quinolone).
Procedural considerations
Statement 7
A 19-gauge EUS-FNA needle is recommended for duct puncture.
Statement is Appropriate (8.0)
Evidence level: Moderate
Supporting evidence and comments
A 19-gauge fine needle aspiration (FNA) needle allows passage of a 0.035 inch or 0.025 inch guidewire. Smaller size needles can be used but thinner wires will be required (0.018 inch or 0.021 inch). A 19-gauge needle allows efficient wire manipulations, but may be difficult to manoeuvre in angulated positions like the duodenum. The use of ‘flexible’ nitinol needles may improve the manoeuvrability in such positions.107
Statement 8
A 0.035 inch or 0.025 inch guidewire with floppy tip should be used to negotiate the bile duct.
Statement is Appropriate (9.0)
Evidence level: Low
Supporting evidence and comments
Both types of wires appear to be equally effective for EUS-BD and they are the most common types of wires used for EUS-BD. The use of thinner wires is possible, but the wires are easy to kink and are not stable for tract dilation and stenting and should be used with caution. A 450 cm wire is commonly used, although some studies have used a shorter 240 cm glide wire to allow faster exchange of accessories.108
Statement 9
Catheters, balloons or cystotomes are recommended for tract dilation. Tract dilation with a precut papillotome is not recommended.
Statement is Appropriate (8.0)
Evidence level: Low
Supporting evidence and comments
There are some data suggesting a higher complication rate when a precut papillotome is used for dilation.109 A 6 Fr cystotome is favoured as it is fast and efficient. 5 Fr stiff catheters and 4 mm biliary dilating balloons may be used if a cystotome is not available in some countries. Recently, one-step systems have become available and obviate the need for dilation as the cautery at the tip of the delivery catheter works as a dilator or cautery.110–112 These novel one-step systems avoid the need for repeated instrumental changes and reduced procedural times.
Statement 10
Fully or partially covered metal stents are recommended for transluminal stenting. Uncovered metal stents can be used for antegrade transpapillary stenting.
Statement is Appropriate (8.0)
Evidence level: Low
Supporting evidence and comments
Covered stents are preferred for transluminal procedures to prevent bile leak. Uncovered stents may be used for transpapillary procedures. LAMS are short dumbbell-shaped fully covered metallic stents with wide flanges to allow anchoring.63 There are limited data available for the use of LAMS except in EUS-guided CDS.111
Statement 11
The use of metal stents is recommended over plastic stents for EUS-BD to reduce the risk of bile leak.
Statement is Appropriate (8.0)
Evidence level: Low
Supporting evidence and comments
There are some data to suggest that bile leak is more common following plastic stent placement. In a large retrospective study, adverse events were significantly higher with plastic stents (42.8% vs 13%, P=0.01). In another study the incidence of cholangitis was significantly higher in the plastic stent group (11% vs 3%, P=0.02).100 113
Management of complications
Statement 12
Multidisciplinary support including interventional radiologist, surgeons and anaesthesiologist to prevent and manage complications is recommended in centres performing EUS-BD.
Statement is Appropriate (9.0)
Evidence level: Very Low
Supporting evidence and comments
EUS-BD may give rise to severe adverse events like perforations, bile leaks and bleeding.114 It is advisable that surgical and interventional radiology support be available in centres performing EUS-BD.
Competency and training
Statement 13
Training of EUS-BD should be done at expert centres with facilities and expertise in EUS, ERCP and PTBD.
Statement is Appropriate (9.0)
Evidence level: Very Low
Supporting evidence and comments
EUS-BD is an advanced endoscopic technique that shares similar skills and accessories with ERCP and PTBD. Currently, EUS-BD is being used as a salvage procedure after failed ERCP. Facilities for PTBD should be available in the event of failed EUS-BD. The three procedures complement each other and training centres should have expertise in all these procedures.
Statement 14
Training in EUS-BD should only commence in those endoscopists experienced in EUS-FNA, wire manipulation techniques and biliary stent placement.
Statement is Appropriate (9.0)
Evidence level: Low
Supporting evidence and comments
There are no formal training programmes for EUS-BD at most centres. The number of patients undergoing EUS-BD is small even at advanced centres. There are no data on the experience an endoscopist is required to attain before training in EUS-BD should be commenced. However, it appears logical to impart training to candidates who are well versed with components of the EUS-BD procedure including FNA, wire manipulation and biliary stent placement.
Statement 15
Pig or ex vivo models are suitable for hands-on training on EUS-BD and should be incorporated into the training programme for EUS-BD.
Statement is Appropriate (8.0)
Evidence level: Low
Supporting evidence and comments
Pig models can be created by endoscopic ligation of the ampulla of Vater, resulting in dilation of the biliary system.115 The process is cumbersome and unpredictable in terms of the degree of biliary dilation obtainable. Ex vivo pig models are easier to create and may be suitable for training of biliary and gallbladder drainage. Three-dimensional (3D) printed models have been described. They appear to be useful but need more modifications. Finding the appropriate material for 3D printing is challenging.116
Consensus statements on the optimal management of EUS-guided pancreatic duct drainage
Consensus statements on the optimal management of EUS-guided pancreatic duct (EUS-PD) drainage are shown in table 6.
Consensus statements on the optimal management of endoscopic ultrasonography-guided pancreatic duct (EUS-PD) drainage
Indications for the procedure
Statement 1
EUS-PD is recommended in patients with pancreatic duct obstruction after failed ERCP.
Statement is Appropriate (8.0)
Evidence level: Moderate
Statement 2
EUS-PD is recommended in patients with pancreatic duct obstruction and surgically altered anatomy or duodenal stenosis where ERCP is not possible.
Statement is Appropriate (9.0)
Evidence level: Moderate
Supporting evidence and comments (statements 1 and 2)
While EUS and percutaneous approaches are alternatives to surgical biliary drainage after failed ERCP, EUS-PD is the only option for non-surgical pancreatic duct drainage after failed endoscopic retrograde pancreatography (ERP).11 117 118 Outcomes in over 200 patients who received EUS-PD showed a pooled technical success rate of 76.6% and adverse events of 18.9%.118 In patients where the papilla can be reached by the duodenoscope, pancreatic duct drainage should be attempted by ERP first. In patients with surgically altered anatomy, ERP with balloon enteroscopy could be performed. In patients with altered anatomy, however, the success rate of reaching the blind end of the roux limb is dependent on the length of the roux limb and ranges between 33% and 88%.119 120 Thus, the EUS approach provides an important alternative in these patients. In a recent study comparing EUS-PD with enteroscopy-assisted ERP, EUS-PD was associated with significantly higher technical and clinical success rates (92.5% vs 20%, P<0.001%; and 87.5% vs 23.5%, P<0.001, respectively).121 However, there were also significantly more mild to moderate adverse events in the EUS-PD group (35% vs 2.9%, P<0.001) without significant differences in procedural times and hospital stay.
On the other hand, it was also noted that newer short-type single or double balloon enteroscopes have become available.122 123 Results from two large-scale studies showed that the success rate in reaching the blind end of the duodenum was 92.6–97% and the treatment success was 81.8–100%, while adverse event rates were 5% in both studies. Thus, the success in reaching the blind end of the roux limb was significantly increased with the newer enteroscopes and studies comparing the outcomes of the EUS approach with the newer devices would be required to assess the advantages and disadvantages of both procedures.
Optimal approach for drainage
Statement 3
EUS-PD could be achieved by the rendezvous technique, pancreatico-gastrostomy and antegrade stenting.
Statement is Appropriate (8.0)
Evidence level: Moderate
Supporting evidence and comments
Similar to EUS-BD, EUS-PD could be divided into access procedure (rendezvous technique) and direct drainage procedures.11 117 124–128 Direct drainage procedures can be transpapillary (antegrade stenting) or transluminal (pancreaticogastrostomy or pancreaticoduodenostomy). For the rendezvous technique, EUS is employed in the initial part of the procedure for pancreatic duct access and guidewire introduction. ERCP is then performed for guidewire retrieval and completion of the procedure. For the transluminal technique, a fistula is first created between the stomach or the duodenum with the pancreatic duct followed by stent insertion. In antegrade stenting, a guidewire is passed across the papilla after pancreatic duct puncture. The tract is then dilated for insertion of a stent across the papilla from the stomach.
Statement 4
The transgastric approach should be used as the initial approach for EUS-PD.
Statement is Appropriate (8.0)
Evidence level: Low
Supporting evidence and comments
The pancreatic duct could be punctured from several routes including the transgastric, transduodenal or transjejunal approach in surgically altered patients. The most common approach is the transgastric approach, followed by transduodenal or transjejunal.118 129 There are no data to suggest which approach is superior; however, the transgastric approach provides the endoscopist with the greatest flexibility on which part of the pancreas to puncture. The site of puncture also affects the direction the guidewire passes, which in turn affects stent placement.
Statement 5
Appropriate imaging including MRCP or CECT is recommended in patients with obstruction of the main pancreatic duct prior to EUS-PD.
Statement is Appropriate (9.0)
Evidence level: Very low
Supporting evidence and comments
Pre-procedural planning is an important element to successful pancreatic duct drainage by the EUS approach. In order to understand the anatomy in each patient, MRCP or CECT should be performed prior to the procedure. The optimal approach is selected by choosing the location with the shortest distance between the bowel lumen and the pancreatic duct, an absence of interposed vasculature, and maximal stability with an angle to allow tract dilation and device deployment. Since the point where ductal puncture is most convenient may not necessarily be the best to facilitate subsequent guidewire insertion and stent placement, pre-procedural imaging and planning is important to the success of the procedure.
Pre-procedural preparations
Statement 6
Antibiotic prophylaxis is recommended before the EUS-PD procedure.
Statement is Appropriate (8.0)
Evidence level: Very Low
Supporting evidence and comments
There are no studies demonstrating the efficacy of prophylactic antibiotics in patients undergoing EUS-PD. However, EUS-PD is similar to other endoscopic pancreaticobiliary interventions and may result in introduction and/or dissemination of bacteria. Thus, prophylactic antibiotics should be used in a similar manner. Antibiotics that cover biliary flora such as enteric gram-negative organisms and enterococci should be used (second-generation cephalosporin or quinolone).
Procedural considerations
Statement 7
Following pancreatic duct puncture with a 19-gauge needle, a 0.035 inch or 0.025 inch guidewire with floppy tip is recommended to be used to negotiate the pancreatic duct and the papilla.
Statement is Appropriate (9.0)
Evidence level: Very low
Supporting evidence and comments
A 19-gauge needle is frequently used to puncture the pancreatic duct.11 117 118 128 129 After puncture, a guidewire is inserted through the 19-gauge needle and to enter the pancreatic duct. The guidewire used should have enough stability for subsequent insertion of dilator and stent. The use of 0.035 inch and 0.025 inch guidewires with a hydrophilic tip may reduce the risk of kinking and buckling when negotiating tight strictures or stenosis. When the pancreatic duct can only be punctured with a 22-gauge needle, then a 0.018 inch or 0.021 inch guidewire is required. These wires kink easily and are not stable for tract dilation and stenting, so they should be used with caution.
Statement 8
Catheters, dilators, cystotomes or balloons are recommended for track dilation.
Statement is Appropriate (9.0)
Evidence level: Very Low
Supporting evidence and comments
Dilation of the needle tract is required prior to stent insertion.11 117 118 128 129 The size of dilation depends on the diameter of the stent. The needle tract can be dilated with catheters and balloons used in ERCP. However, insertion of these instruments may be impossible in a calcified pancreas or when an acute angulation exists between the needle tract and the pancreatic duct. In this situation, electrocautery may be used to dilate the tract. However, the use of cautery can sometimes lead to pancreatitis, pancreatic leak, bleeding or perforation. Therefore, it is important to use cautery sparingly and adjust the direction of the electrocautery to the axis of the tract.117 118 129 The use of coaxial electrocautery may be preferable to a precut papillotome as the direction of cutting is along the axis of the tract, but no studies have compared the devices in EUS-PD.
Statement 9
Plastic stents without intervening side holes between the ends of the stent are recommended for EUS-PD.
Statement is Appropriate (8.0)
Evidence level: Low
Supporting evidence and comments
7 Fr straight plastic stents without intervening side holes between the ends of the stent are most commonly used, although stents of other sizes could also be employed.129 130 Straight stents may have more pushability than pigtail stents. However, stent migration was shown to occur more frequently compared with double pigtail plastic stents in one study (9% vs 23%, P=0.62).131 Recently, fully covered SEMS with antimigratory properties for EUS-PD have been reported. A technical and clinical success rate of 100% has been reported in 25 patients with significant reduction in pain scores after placement.132 However, the long-term outcomes of metal stents for EUS-PD will need further evaluation.
Management of complications
Statement 10
Multidisciplinary support including interventional radiologist, surgeons and anaesthesiologist are recommended in centres performing the procedure to prevent and manage complications as complication rates of EUS-PD are higher than ERCP.
Statement is Appropriate (9.0)
Evidence level: Low
Supporting evidence and comments
EUS-PD is a technically demanding procedure. A pooled technical success rate among 222 patients was 76.6% and adverse events rates were 18.9%. Adverse events included pancreatitis, perforation, bleeding, peripancreatic pseudocyst/abscess formation, abdominal pain, pneumoperitoneum, pseudoaneurysm and shearing of guidewire coating.118 133 Prompt management of these adverse events is best done in a multidisciplinary manner. Furthermore, centres should be equipped with options to drain the pancreatic duct with advanced ERCP techniques or surgery in the event of failed EUS-PD.
Competency and training
Statement 11
EUS-PD should be done at expert centres with facilities and expertise in interventional EUS and advanced ERCP.
Statement is Appropriate (9.0)
Evidence level: Very Low
Supporting evidence and comments
As mentioned above, EUS-PD is a technically demanding procedure with a low margin for error even when performed in expert centres. Although not supported by any study, the group believes that centres performing EUS-PD should have abundant experience in interventional EUS and advanced ERCP in order to manage failures and adverse events promptly.
Statement 12
EUS-PD should be performed by experienced endoscopists in EUS and EUS-FNA, wire manipulation techniques and stent placement.
Statement is Appropriate (9.0)
Evidence level: Very Low
Supporting evidence and comments
The group believes that EUS-PD is one of the most difficult types of EUS drainage procedures. Endoscopists performing the procedure should have abundant experience in advanced EUS techniques and stent placement. In addition, abundant experience in other EUS-guided drainage procedures may improve the success rate and reduce the risk of adverse events.
Consensus statements on the optimal management of EUS-guided celiac plexus ablation (neurolysis and gangliolysis)
Consensus statements on the optimal management of EUS-guided celiac plexus ablation (neurolysis and gangliolysis) (EUS-CPN and -CGN) are shown in table 7.
Consensus statements on the optimal management of endoscopic ultrasonography-guided celiac plexus ablation (neurolysis and gangliolysis) (EUS-CPN and -CGN)
Indications for the procedure
Statement 1
EUS-guided celiac plexus neurolysis (CPN) is recommended in patients suffering from pain due to unresectable upper abdominal cancer, particularly for pancreatic cancer.
Statement is Appropriate (8.0)
Evidence level: High
Supporting evidence and comments
The celiac plexus is responsible for transmitting pain sensation originating from the upper abdominal organs including the pancreas, liver, gallbladder, stomach and ascending and transverse colons. CPN disrupts the transmission of pain signals from afferent nerves to the spinal cord by injecting a neurolytic agent into the celiac plexus. Therefore, EUS-CPN can be used for the treatment of pain arising from the upper abdominal cancers. Among them, pancreatic cancer is the most common indication as more than 80% of patients in the advanced stages of pancreatic cancer experience pain, and pain control is a major challenge in the management of these patients.134
CPN has been shown to reduce pain scores and opioid consumption in patients with unresectable pancreatic cancers.135–137 Furthermore, CPN causes fewer adverse events than opioids. However, performing CPN in addition to pancreaticoduodenectomy did not result in a further reduction of pain, suggesting that the procedure should not be used in surgical candidates.138
Statement 2
EUS-guided CPN for treatment of pain arising from chronic pancreatitis is not recommended.
Statement is Appropriate (7.0)
Evidence level: Moderate
Supporting evidence and comments
The efficacy of EUS-CPN is relatively low for patients with pain arising from chronic pancreatitis. In a meta-analysis, EUS-CPN for pain in pancreatic cancer (n=283) was compared with that for chronic pancreatitis (n=376).139 The pooled proportion of patients with relief of pain was 80.12% in pancreatic cancer and 59.45% in chronic pancreatitis. In another meta-analysis of 11 relevant studies, EUS-CPN was effective in alleviating pain in 72.54% of patients with pancreatic cancer and 51.46% of patients with chronic pancreatitis.140 Similar findings were reported in a more recent meta-analysis.141 Thus, the role of EUS-CPN in chronic pancreatitis is still controversial due to the limited efficacy. If a trial of the procedure is planned, then a temporary block of the plexus using bupivacaine should be performed to observe for any effect in achieving pain relief.
Optimal approach for ablation
Statement 3
The EUS-guided approach is recommended over percutaneous image-guided techniques for celiac plexus ablation.
Statement is Appropriate (9.0)
Evidence level: Moderate
Supporting evidence and comments
The EUS-guided approach is performed under the guidance of precise real-time imaging. In addition, assessment with colour Doppler ultrasonography allows avoidance of injury to interposing blood vessels. Therefore, the approach is safer, more accurate and convenient than percutaneous image-guided approaches including radiographic, fluoroscopic, CT or transcutaneous ultrasonographic guidance. Only one study has compared the effectiveness of EUS-guided celiac plexus block (EU-CPB) with that of CT-guided CPB for chronic pancreatitis.142 The results showed that EUS-guided CPB provided more persistent pain relief than CT-guided CPB. However, only 10 patients were included for EUS-guided CPB and eight patients for CT-guided CPB. Nevertheless, given that the results of EUS-CPN are widely published and the procedure is continued to be practiced in many countries, the panel believes that the efficacy of the EUS and percutaneous approach should be at least comparable.
Pre-procedural preparations
Statement 4
Prophylactic antibiotics are suggested to be given when bupivacaine with steroids are used for EUS-CPB.
Statement is Appropriate (7.0)
Evidence level: Low
Supporting evidence and comments
In general, prophylactic antibiotics are not given before and after EUS-CPN. However, serious infectious complications such as peripancreatic abscess and retroperitoneal abscess are occasionally reported after injection of steroid in EUS-CPB in the setting of chronic pancreatitis.139 143–145 Therefore, prophylactic antibiotics are recommended before EUS-CPB when steroids are used.146 Antibiotics that cover enteric gram-negative organisms and enterococci should be used (second-generation cephalosporin or quinolone).
Procedural considerations
Statement 5
10–20 mL of absolute ethanol is recommended for EUS-CPN and the volume may be reduced in EUS-guided celiac ganglia neurolysis (CGN).
Statement is Appropriate (8.0)
Evidence level: High
Supporting evidence and comments
Absolute ethanol is injected into the region until an echogenic cloud is seen to spread sufficiently under EUS. A total amount of 10–20 mL of ethanol is usually used in the EUS-CPN. In contrast, 1–2 mL of ethanol is usually used to inject the ganglion in EUS-CGN until it becomes hyperechoic and difficult to visualise. A randomised study showed that the total amount of injected ethanol was significantly lower in EUS-CGN than in EUS-CPN.147
Statement 6
Phenol may be used instead of alcohol for EUS-guided CPN in patients with alcohol intolerance due to aldehyde dehydrogenase deficiency, but the comparative efficacy and safety of the two agents is uncertain.
Statement is Appropriate (8.0)
Evidence level: Low
Supporting evidence and comments
Alcohol intolerance can be confirmed by an alcohol patch test which tests an individual for aldehyde dehydrogenase deficiency.148 Only one study has investigated the effectiveness of phenol instead of ethanol.149 In this study, phenol was used for six patients with alcohol intolerance and the effectiveness was compared with that of 16 patients without alcohol intolerance who received an ethanol injection. There was no significant difference in the positive response rate on day 7 and the rate of complications between the two groups. Further studies are required to evaluate the efficacy and safety of phenol.
Statement 7
In order to perform EUS-CGN, the celiac ganglia can be identified between the aorta and the left adrenal gland in most patients. Otherwise, they may be located cephalad to the origin of the celiac axis in others.
Statement is Appropriate (8.0)
Evidence Level: Moderate
Supporting evidence and comments
The celiac ganglia are most frequently seen to the left of the celiac artery, between the aorta and the left adrenal gland, at the level between the celiac artery and the left renal artery. They are also visualised cephalad to the celiac artery in some cases. They usually appear as hypoechoic nodular structures linked by hypoechoic threads residing in the periphery of this region.147 150
Efficacy of treatment
Statement 8
Early EUS-CPN at the time of EUS-guided fine needle aspiration is recommended as it reduces pain and may moderate opioid consumption compared with best medical therapy.
Statement is Appropriate (7.5)
Evidence Level: High
Supporting evidence and comments
A study compared pain reduction and narcotic use after early EUS-CPN at the time of EUS with that of conventional pain management.151 They concluded that early EUS-CPN could reduce pain and may moderate morphine consumption in patients with painful inoperable pancreatic cancers.
Statement 9
When the ganglion cannot be identified, EUS-CPN is performed by single or bilateral injections but evidence is contradictory on which approach is superior.
Statement is Appropriate (8.5)
Evidence Level: High
Supporting evidence and comments
EUS-CPN is conventionally done with two approaches.152–154 The classic approach, known as the central technique, involves injection of the agent at the base of the celiac artery. The second approach, the bilateral technique, involves injecting the agent on both sides of the celiac artery. With improvements in ultrasound imaging technology, the celiac ganglion an now be visualised with EUS.155 The ganglion can be directly punctured for delivery of neurolytic agents resulting in celiac ganglion neurolysis (CGN). In addition, a modified technique for broad distribution of the agent was also reported.156 It involves injection around the superior mesenteric artery and celiac artery using a thin needle resulting in broad plexus neurolysis. A meta-analysis that included eight studies compared the treatment efficacy between unilateral and bilateral techniques. The rate of pain relief was significantly higher with bilateral injections compared with unilateral injections in patients with pancreatic cancer (84.54% vs 45.99%).139 In another cohort study, the short-term safety and efficacy of central and bilateral EUS-CPN/EUS-CPB in 160 patients was assessed (71 treated centrally, 89 treated bilaterally).152 The mean reduction in pain score was significantly higher in patients treated with bilateral injections (70.4% vs 45.9%). A positive response (>50% reduction in pain score) was also significantly more frequent in the bilaterally treated group (77.5% vs 50.7%). In addition, the only predictor of a positive response was the use of the bilateral procedure. These results suggested that the bilateral procedure was more effective than the central procedure. However, a randomised trial later showed no difference in pain relief between the central and bilateral techniques (central 69% vs bilateral 81%; P=0.340).153 In addition, another retrospective study also showed similar pain reduction between the central and bilateral procedures.154 Thus, it is still controversial whether the bilateral approach is superior to the unilateral approach for relieving pain.
Statement 10
EUS-guided CGN is recommended over single or bilateral injections around the celiac artery for improved pain relief.
Statement is Appropriate (8.0)
Evidence Level: High
Supporting evidence and comments
The initial report of EUS-CGN showed a high response rate in a small group of patients.155 A retrospective comparative study then reported their data of EUS-CPN versus CGN.157 In the study, EUS-CGN was performed when the celiac ganglia were visible by EUS, otherwise bilateral EUS-CPN was performed. Multivariate analysis showed that patients with visible celiac ganglia were 15 times more likely to respond (OR 15.7; P=0.001). Subsequently, a multicentre randomised controlled trial was conducted to compare the efficacies of central EUS-CPN and EUS-CGN. The positive response rate was significantly higher in the EUS-CGN group (73.5% vs 45.5%). The complete response rate was also significantly higher in the EUS-CGN group (50.0% vs 18.2%).
Statement 11
Celiac broad plexus neurolysis may be associated with improved efficacy but routine use is not recommended.
Statement is Appropriate (7.5)
Evidence Level: Moderate
Supporting evidence and comments
A retrospective cohort study examined predictive factors for pain relief after EUS-CPN.158 Multivariate analysis revealed that direct invasion of the celiac plexus (OR 4.82, P=0.0387) and distribution of ethanol only on the left side of the celiac artery (OR 8.67, P=0.0224) were significant factors for a negative response to EUS-CPN. A study then assessed the effect of broad distribution of the neurolytic agent.156 In their retrospective study, they compared the effectiveness of standard EUS-CPN and EUS-guided broad plexus neurolysis (EUS-BPN). EUS-BPN involves injection along the celiac artery, superior mesenteric artery and inferior mesenteric artery using a thin 25-gauge needle. As a result, ethanol was distributed more widely and better pain relief was obtained in EUS-BPN than in EUS-CPN. These studies suggest that broad distribution of the injected ethanol was an important factor to predict the good response to EUS-CPN. However, the results of this study require further confirmation by other studies and it is uncertain whether such wide distribution of alcohol would result in any detrimental effects.
Management of complications
Statement 12
The complications of EUS-CPN and CGN are generally minor and do not need specific treatment.
Statement is Appropriate (8.0)
Evidence Level: Low
Supporting evidence and comments
Common reported adverse events of EUS-CPN include transient diarrhoea (0–23.4%), transient pain exacerbation (0–36%), transient hypotension (0–33%) and inebriation (0–12.5%).139 140 142–144 147 149 151–167 In most cases these events are mild and do not need specific treatment. In a randomised study of central EUS-CPN and EUS-CGN, the overall adverse events rates were similar between the two groups.147
Statement 13
Repeated injections for chronic pancreatitis should be avoided to prevent development of major complications.
Statement is Appropriate (8.0)
Evidence Level: Low
Supporting evidence and comments
Severe adverse events such as retroperitoneal bleeding, abscess and ischaemia rarely occur after EUS-CPN or EUS-CPB.144 145 152 168–175 Most of these events, especially infectious ones, were reported in the setting of chronic pancreatitis. Retroperitoneal bleeding occurred in two cases who underwent the bilateral technique.152 168 Ischaemic events were lethal in three cases.172 174 175 These vascular injuries and ischaemic events are probably due to injecting alcohol into an inappropriate site or an excessive number of sessions of EUS-CPN.
Competency and training
Statement 14
Training in EUS-guided celiac plexus ablation is recommended in endoscopists experienced in EUS and EUS-FNA.
Statement is Appropriate (9.0)
Evidence Level: Very Low
Supporting evidence and comments
EUS-CPN and CGN are relatively simple procedures. However, serious adverse events occasionally occur. Before and during the needle puncture, the target regions should be clearly visualised in a stable position. The needle tip should be visualised at all times during the puncture to avoid injury of vessels and other organs. Endoscopists who are competent in EUS-FNA would be able to perform the procedure provided that target regions are visualised.
Discussion
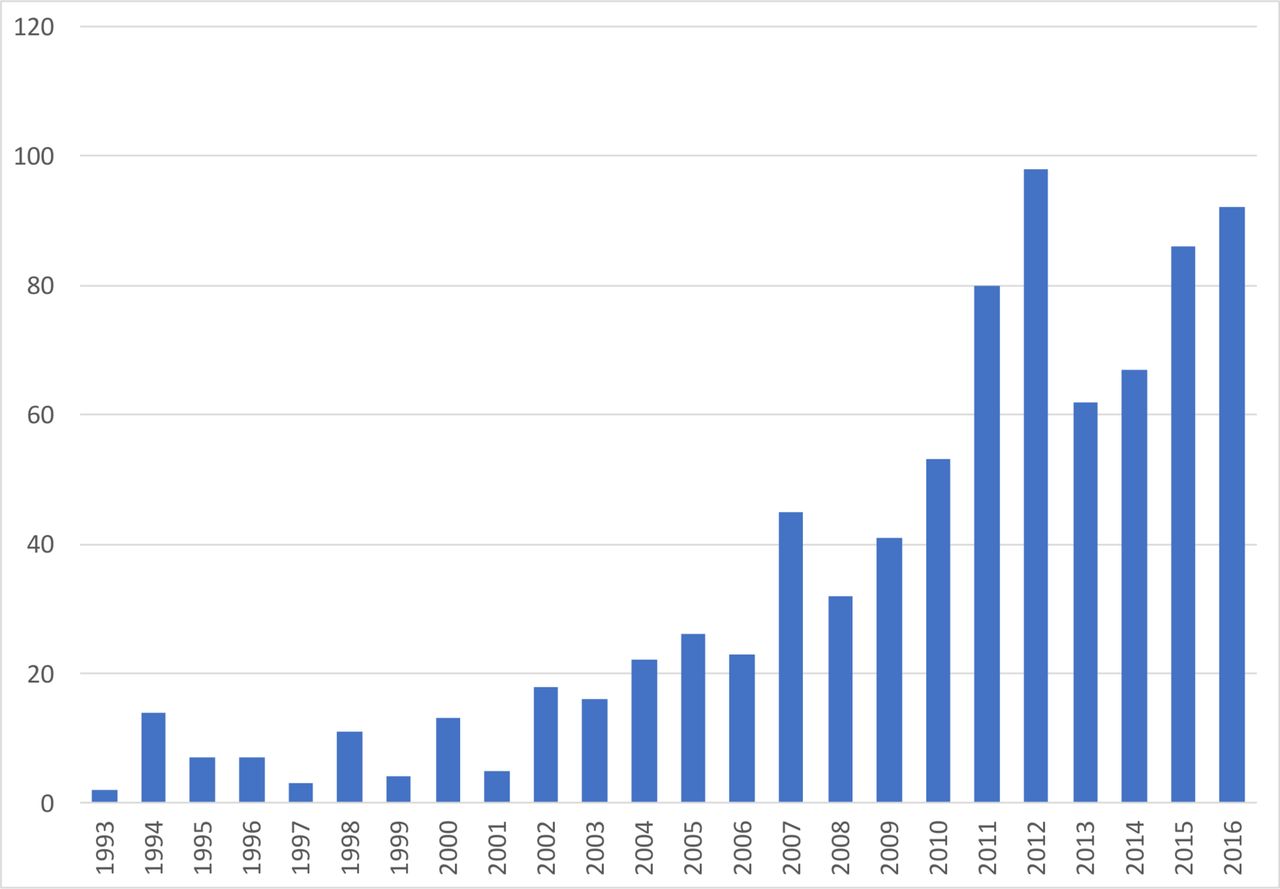
EUS-guided drainage of a pancreatic pseudocyst was first reported in 1992.176 Since then, interventional EUS has undergone exponential growth throughout the past 20 years. Using the term ‘interventional EUS’ as a search criterion on PubMed, the number of publications each year has grown enormously (figure 3). Furthermore, new therapeutic procedures are reported every few years. The types of EUS interventional procedures have grown from those initially described by the EUS Working Group to now include gallbladder drainage, gastrointestinal anastomosis, portal vein interventions and tumour ablations.177–185
{kind=link}
{kind=link}
{kind=link}
Number of publications on interventional endoscopic ultrasonography (EUS) each year
The current set of guidelines is the first published by an endoscopic society. Prior to formulation of the guidelines, the panel acknowledges the fact that evidence may be lacking in certain areas of the procedure. Thus, the RAM process was adopted to help formulate the guidelines. The rationale behind RAM is that randomised clinical trials are often not available or cannot provide evidence at a level of detail sufficient to apply to the wide range of patients seen in everyday clinical practice. Nevertheless, physicians will still need to make decisions every day about when to apply them. Thus, a method that could combine the best available scientific evidence with the collective judgement of experts to yield a statement regarding the appropriateness of performing a procedure at the level of patient-specific symptoms, medical history and test results is required. The strength of the instrument is that RAM has been shown to produce criteria that have excellent face, construct and predictive ability.186 187 Furthermore, studies comparing RAM results with subsequent randomised controlled trials have found excellent correlation.7
The current guidelines were developed on the four commonly performed therapeutic EUS procedures. An additional strength of the guidelines is that they focused on the technical aspects of the procedures and also addressed management issues before and after the intervention. Furthermore, competency and training issues were also discussed. All but one of the statements were found to be appropriate and necessary. This means that the expected benefits on following the guidelines exceeds the harms sufficiently that the service must be offered to the patient. Thus, the panel believes that the guidelines would be applicable to all those practising or learning interventional EUS procedures around the world. In addition, the guidelines could help standardise the elements involved with the procedures as wide variations in practice have been observed, and establishment of a consensus for safe practices is required.88
There are a number of limitations to the current guidelines. First, these EUS procedures are still in evolution and the devices used are not uniformly available across all countries. Hence, they should be adopted after consideration of device availability, institutional practices and endoscopist preferences. Second, the guidelines did not address outcome indicators of the procedures. The panel believes that this aspect should be addressed in future updates of the guidelines. When the procedures become more standardised, outcomes could be benchmarked across centres. In addition, since the learning curve in a few of the procedures is not established, concrete suggestions on the minimal number of procedures required to be performed in order to attain competency could not be provided. Lastly, the expert panel consisted mostly of interventional endosonographers and it is established that panels made up of members from the same discipline may rate more indications as appropriate than do panels composed of multiple specialties.
The current guidelines also identified a number of areas where randomised studies are urgently required to address the clinical questions. The use of EUS-specific metal stents in pseudocyst drainage needs to be justified due to its higher cost. The procedural characteristics of different EUS-BD procedures need to be better determined to understand which approach is the safest while providing the longest stent patency. Randomised studies comparing EUS-PD versus ERCP in surgical altered anatomy are required to understand which is the best approach in these challenging situations. Newer celiac plexus ablation techniques need to be evaluated in a multicentre setting to confirm the efficacy published in smaller studies.
The only other set of published guidelines on interventional EUS was provided by the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) in 2016. Interventional EUS was included as part of the set of guidelines under interventional ultrasound. Eight statements on EUS drainage of pancreatic fluid collections, six statements on EUS-BD and PD and eight statements on EUS-CPN were provided. Compared with the current guidelines, the guidelines published by EFSUMB were lacking in providing clear indications to the procedure, appraisal of the technical aspects, management of complications and competency and training f the procedures. These deficiencies would limit the practical applicability in clinical practice.
In conclusion, the current guidelines on interventional EUS procedures are the first published by an endoscopic society. They provide an in-depth review of the current evidence and standardise the management of the procedures.
References
Footnotes
Contributors AYBT: Concept and design, voting member, data collection and analysis, drafting of the manuscript. VD: Concept and design, voting member, drafting of the manuscript. MK: Concept and design, voting member, drafting of the manuscript. IY: Concept and design, voting member, drafting of the manuscript. ZDJ: Voting member, critical review of the manuscript. DWS: Voting member, critical review of the manuscript. MA: Voting member, critical review of the manuscript. TLA: Voting member, critical review of the manuscript. KH : Voting member, critical review of the manuscript. IH: Voting member, critical review of the manuscript. TI: Voting member, critical review of the manuscript. SL: Voting member, critical review of the manuscript. KM: Voting member, critical review of the manuscript. NP: Voting member, review of the manuscript. RP: Voting member, critical review of the manuscript. RST: Voting member, critical review of the manuscript. H-PW: Voting member, critical review of the manuscript. AMY: Voting member, critical review of the manuscript. RH: Critical review of the manuscript. SV: Critical review of the manuscript. KY: Voting member, critical review of the manuscript. LKYH: Critical review of the manuscript, final approval of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.