Article Text

Abstract
Background This is a consensus developed by a group of expert endoscopists aiming to standardise the preparation, process and endoscopic procedural steps for diagnosis of early upper gastrointestinal (GI) cancers.
Method The Delphi method was used to develop consensus statements through identification of clinical questions on diagnostic endoscopy. Three consensus meetings were conducted to consolidate the statements and voting. We conducted a systematic literature search on evidence for each statement. The statements were presented in the second consensus meeting and revised according to comments. The final voting was conducted at the third consensus meeting on the level of evidence and agreement.
Results Risk stratification should be conducted before endoscopy and high risk endoscopic findings should raise an index of suspicion. The presence of premalignant mucosal changes should be documented and use of sedation is recommended to enhance detection of superficial upper GI neoplasms. The use of antispasmodics and mucolytics enhanced visualisation of the upper GI tract, and systematic endoscopic mapping should be conducted to improve detection. Sufficient examination time and structured training on diagnosis improves detection. Image enhanced endoscopy in addition to white light imaging improves detection of superficial upper GI cancer. Magnifying endoscopy with narrow-band imaging is recommended for characterisation of upper GI superficial neoplasms. Endoscopic characterisation can avoid unnecessary biopsy.
Conclusion This consensus provides guidance for the performance of endoscopic diagnosis and characterisation for early gastric and oesophageal neoplasia based on the evidence. This will enhance the quality of endoscopic diagnosis and improve detection of early upper GI cancers.
- endoscopy
- gastric neoplasia
- oesophageal cancer
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Upper gastrointestinal (GI) cancers are common cause of cancer death worldwide. The prognosis of upper GI cancers is closely related to the stage of the disease. Generally, the 5 year survival rate for patients with early upper GI cancers exceeds 85%. Patients with early stage upper GI cancers are usually asymptomatic. Endoscopic recognition can be difficult and is a major challenge to clinicians. Currently, there is no global consensus on the use of diagnostic upper endoscopy to recognise and characterise early GI cancers, especially from Asia where upper GI cancers are highly prevalent (approximately three quarters of the worldwide prevalence).1 2 In this paper, , we develop an Asian consensus regarding the preparation and application of image enhanced endoscopy (IEE) for the diagnosis of early upper GI cancers.
Methodology
A professional group was formed by leading Asian endoscopists as a non-government organisation to improve endoscopic diagnosis of early GI cancers through a structured educational programme in Asia. The group organised three meetings to develop a consensus on diagnostic endoscopy for GI neoplasia. The Delphi method was used to develop the consensus statements. The panel of experts was divided into two groups, focusing on upper and lower GI endoscopy, respectively. The upper GI statements are reported here.
First consensus meeting (22–24 January 2016)
The first face to face meeting focused on the drafting of consensus statements on standards of diagnostic upper GI endoscopy in the following areas:
Standard preparation for diagnostic endoscopy
Endoscopic recognition of early GI neoplasia
Endoscopic characterisation of early GI neoplasia.
Initial draft statements were formulated, discussed and agreed by the panel of experts. Each member was assigned to search for evidence for or against the respective statement and to prepare for discussion and voting in the following consensus meetings. The literature search for each statement was conducted on publications in English from scientific databases, including AMED, BIOSIS previews, EBM reviews, Embase, Ovid MEDLINE and Cochrane Trials and systematic reviews.
PICO method for establishment of statements
The PICO method (Problem/Population; Intervention; Comparison; Outcome) was employed to identify the appropriate intervention and standards for the conduct of diagnostic endoscopy, focusing on the detection and characterisation of early GI neoplasia as a clinical outcome. All statements were established following the PICO worksheet (figure 1) (see online supplementary 1).
Supplemental material

PICO (Problem/Population; Intervention; Comparison; Outcome) worksheet and search strategy.
Second consensus meeting (June 2016)
After the search for evidence in respect of each statement, a second face to face meeting was conducted to refine the statements and to vote on them. Appropriate time was provided to members to refine each statement through discussion. After the meeting, a period of 5 months was allocated for the further collection of comments through a closed group internet platform.
Third consensus meeting (November 2016)
All the experts in the panel joined the third consensus face to face meeting and completed anonymous voting on all the statements.
Delphi method for voting
The expert panel formulated statements in two separate rounds of voting and opinion collection. After each round, facilitators provided a summary of the experts’ opinions from the previous round for refinement. The voting was based on a review of the literature on a Likert scale which ranged from 1 to 5 (1=accept completely, 2=accept with some reservation, 3=accept with major reservation, 4=reject with reservation, 5=reject completely). All votes were cast anonymously by means of a wireless polling system. Consensus was achieved when >80% of members indicated that they accepted the statement completely or accepted it with some reservation. If consensus was not reached, panel members discussed the statement again with a view to its modification. Discussion was followed by a second round of voting. If consensus was still not reached, the statement was discussed and modified for a third time and a final round of voting was conducted. Each statement was graded on the level of evidence in its support and the strength of the recommendation it received (tables 1, 2 and 3).
Quality of evidence summarised for each of the statements will be graded according to the classification below
Classification of recommendation
A list of statements
Consensus statements
Statement 1.1: Risk stratification regarding UGI cancers should be performed before diagnostic oesophagogastroduodenoscopy (OGD)
Level of evidence: III
Level of recommendation: B
Level of acceptance: 100%
Identification of high-risk patients should alert the endoscopist to observe mucosa with greater care with more liberal application of IEE. There should be a lower threshold to biopsy suspicious lesions.3 There are individuals at higher risk of UGI cancer. Risk stratification performed before diagnostic oesophagogastroduodenoscopy (OGD) may improve cancer detection (table 4).
Factors for risk stratification for esophageal and gastric cancer before and during endoscopy
Oesophageal squamous cell carcinoma (SCC)
Oesophageal cancer is often diagnosed in patients aged ≥50 years old. Smokers have a fivefold greater risk than non-smokers.4 Alcohol consumption is a consistent risk factor for oesophageal SCC, and risk increases with the amount of alcohol consumed. About 40% of East Asians experience ‘facial flushing’ after drinking alcohol, due to an aldehyde dehydrogenase 2 (ALDH2) deficiency.5 6 This is associated with a significant increased risk of oesophageal SCC compared with a fully active ALDH2 metaboliser for light, moderate and heavy alcohol drinking (ORs of 6.11, 53.86 and 77.10, respectively).7 Past history and/or concomitant SCC in the head and neck region or another part of the oesophagus increase the likelihood of oesophageal SCC.8 9
Oesophageal adenocarcinoma
The incidence of oesophageal adenocarcinoma is eight times higher in Caucasian men than in women.10 The risk of developing oesophageal adenocarcinoma is about twofold higher among smokers.11 12 Currently there is no conclusive association of obesity with adenocarcinoma.
Gastric adenocarcinoma
The incidence of gastric cancer increases among patients aged ≥50, with men having a twofold higher incidence. Worldwide, gastric cancer is more common in individuals with an East Asian, South and East European or Central and South American ethnic background.1 2 The occurrence of gastric cancer is 1.5–10.1 times higher in the siblings or offspring of gastric cancer patients.13 Several inherited cancer predisposition syndromes, including hereditary diffuse gastric cancer, familial adenomatous polyposis and Lynch syndrome, should be managed by experts in genetic testing and counselling.
Chronic Helicobacter pylori infection of the gastric mucosa causes inflammation followed by atrophy and intestinal metaplasia (IM), leading to dysplasia and cancer.14 Gastric cancer develops in about 1% of individuals with H. pylori infection, and >95% of patients with gastric cancer have active or past H. pylori infection.15 Thus, past or current H. pylori infection, especially when combined with the presence of mucosal atrophy and/or IM, is a substantial risk factor.16 In patients with a history of endoscopic resection of early gastric cancer (EGC), metachronous gastric cancer develops frequently, with a cumulative 5 year incidence of 7–15%. H. pylori eradication reduces the risk of the development of metachronous gastric cancer, but never eliminates it.17 18
Statement 1.2: Presence of endoscopic high-risk findings for UGI cancers should raise the index of suspicion of the endoscopists
Level of evidence: III
Level of recommendation: B
Level of acceptance: 100%
In addition to clinical information, important endoscopic findings are also associated with a significant risk of upper GI cancers. Therefore, endoscopists should be alerted to such findings during OGD (table 4).
Oesophageal SCC
Oesophageal melanosis is associated with oesophageal (OR 6.5, 95% CI 2.9 to 15) and oropharyngo-laryngeal (OR 15, 95% CI 4.1 to 53) SCC19 (figure 2A). Iodine chromoendoscopy visualises precancerous dysplastic lesions in the oesophageal mucosa as Lugol-voiding lesions (LVLs, figure 2B). Patients with numerous (>10 in an endoscopic image) LVLs (≥5 mm) have concomitant oesophageal SCC (OR 21, 95% CI 11 to 43),20 and subsequent development of metachronous oesophageal SCC after endoscopic resection (2 year cumulative incidence of 24.7%; RR 7.4, 95% CI 2.6 to 22).21 22

Melanosis is commonly seen in the soft oral palate (A, white arrows) as well as in the oesophagus, indicating risk of presence of squamous cell carcinoma (SCC) in the oropharynx, larynx and oesophagus. (B) Multiple Lugol-voiding lesions in the background oesophageal mucosa predict subsequent development of metachronous oesophageal SCC after endoscopic resection of a primary lesion. (C) A case of intramucosal adenocarcinoma in the oesophago-gastric junction (OGJ). A reddish irregular mucosa presented at the 1 o’clock position of the OGJ. (D) Magnifying the narrow band image (NBI) (white box in C) identified an area with irregular microvessels and a demarcation line at the distal side of the lesion, suggesting the lesion was neoplastic.
Oesophageal adenocarcinoma
A longer segment of columnar mucosa in Barrett’s oesophagus is associated with a higher risk for high grade dysplasia (HGD) and adenocarcinoma.23–25 Some studies have reported that Barrett’s neoplasia, especially in the short segment Barrett’s oesophagus, developed more frequently in the area between 1 and 5 o’clock, which warrants careful endoscopic examination26–28 (figure 2C,D).
Gastric adenocarcinoma
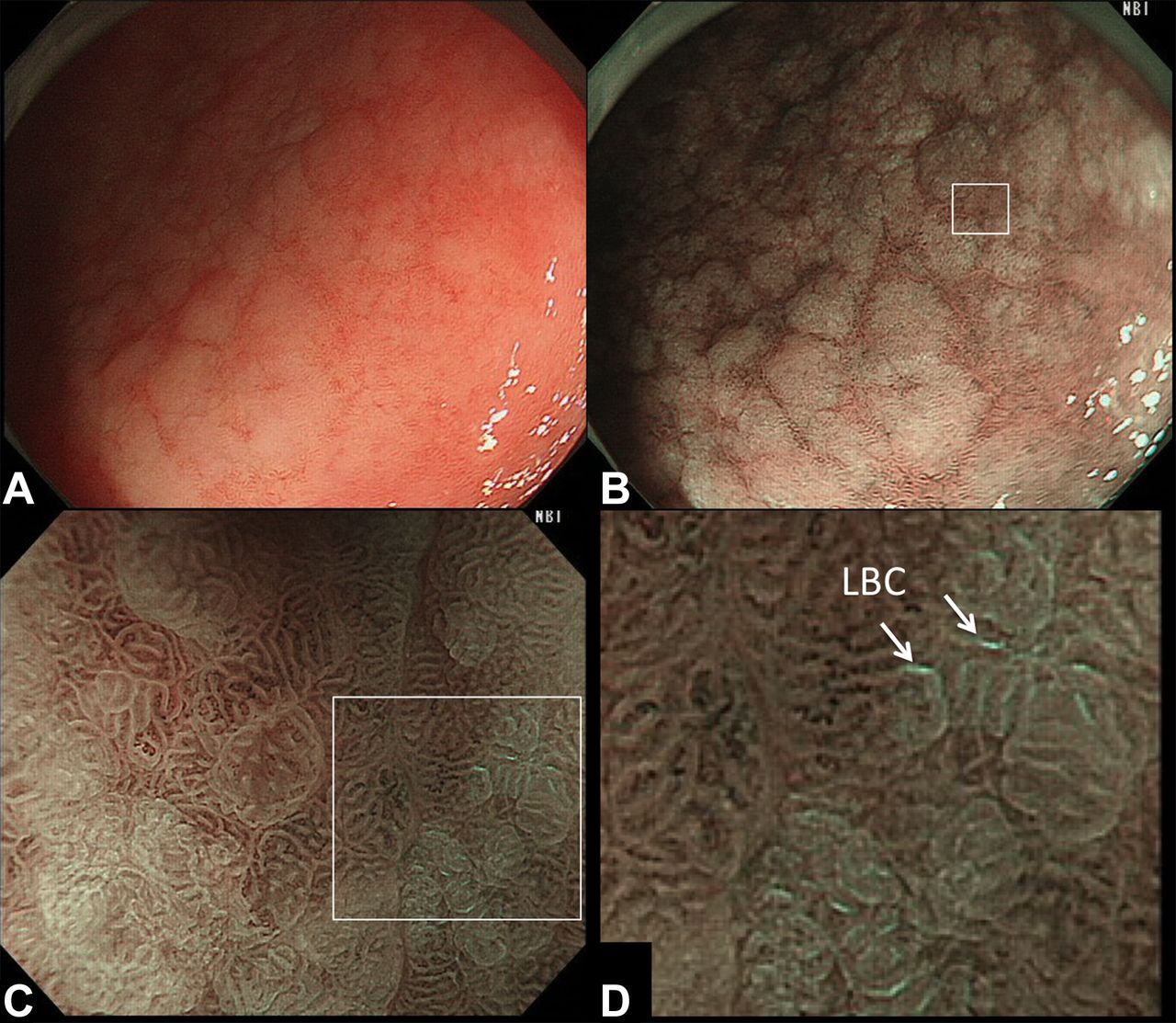
Kimura and Takemoto characterised the endoscopic findings of atrophic mucosa in the corpus as areas with increased visibility of vessels, pale colour or low height29 (figure 3A,B). This characterisation marks an important distinction between atrophy and normal mucosa, where fundic glands are diminished or lost by chronic H. pylori infection, from non-atrophic fundic mucosa.30 31 The extent of endoscopic gastric mucosal atrophy correlates with the risk of gastric cancer.16 Gastric IM is a well-known precancerous condition (figure 4A,B).14 32 The extent of the IM is usually graded by systematic biopsies,33 but narrow band imaging (NBI), a recently-developed IEE technology, visualises gastric IM with high degrees of accuracy (sensitivity of 89% and specificity of 93% with the light blue crest sign, figure 4C,D).34 In contrast, endoscopic findings of regular arrangement of collecting venules (figure 3C,D)35 and fundic gland polyp36 are indicative of H. pylori naïve patients, suggesting a very low risk of gastric cancer. Endoscopic findings could be a good adjunct or even an alternative to the histological assessment of gastric cancer risk by multiple biopsies.37 38

Patient with Helicobacter pylori-associated chronic atrophic gastritis. (A) In a white light image, atrophic mucosa with whitish colour and increased vessel visibility were seen in the lessor curvature of the corpus. (B) An auto-fluorescence image (AFI) showed the atrophic mucosa including the intestinal metaplasia as a greenish area. (C) Patient with neither H. pylori infection nor atrophic gastritis. The corpus mucosa looked homogeneously reddish and gastric folds were well preserved in whole circumference. (D) In the close view, regularly arranged collecting venules were seen.

Patient with gastric intestinal metaplasia. (A) White light image showed slightly elevated whitish patches in the antrum. (B) A narrow band image (NBI) enhanced the presence of the whitish patches. (C and D) By magnifying the NBI image (white box in B), the light blue crest (LBC—which is defined as a fine blue-white line of light on the surface of the epithelium—is seen at the intestinal metaplasia.
Statement 2: Presence or absence of premalignant mucosal changes during OGD should be documented
Level of evidence: III
Level of recommendation: C
Acceptance: 100%
As endoscopic diagnosis of premalignant conditions is associated with risks of upper GI neoplasia, the expert panel recommended documenting these findings. This information will assist clinicians managing their patients to recommend a surveillance programme for those at high risk. The ESGE guideline on the management of precancerous conditions and lesions in the stomach recommended surveillance endoscopy for patients with extensive atrophy and/or intestinal metaplasia at 3-year intervals.3
Statement 3.1: Use of sedation is recommended to enhance the detection rate of superficial neoplasm of the oesophagus and stomach
Level of evidence: III
Level of recommendation: C
Level of acceptance: 80%
No studies have directly assessed the role of sedation on the endoscopic detection rate of superficial upper GI neoplasia.39 40 A systematic review has investigated the effect of sedation on the performance of endoscopy in 3918 patients from 16 studies.41 One of the large placebo-controlled randomised controlled trials (RCTs) showed that midazolam and meperidine resulted in significantly better patient cooperation (79% vs 19%), satisfaction (79% vs 47%), and willingness to repeat the procedure (81% vs 65%). A meta-analysis of two other RCTs confirmed that sedation resulted in significantly better patient satisfaction (RR 2.29, 95% CI 1.16 to4.53).
Although there was no direct evidence to support the use of sedation to enhance the detection of early upper GI neoplasm, the consensus panel recommended the use of sedation as it improved patient acceptance and tolerance for surveillance OGD.
Statement 3.2: Use of an antispasmodic agent is recommended to enhance the detection rate of superficial neoplasm during OGD and IEE
Level of evidence: III
Level of recommendation: C
Level of acceptance: 80%
Two types ofantispasmodic agents are commonly used for OGD: hyoscine/glucagon injection, and topical spray of peppermint oil/L-menthol. No RCTs have been conducted on the use of hyoscine/glucagon for OGD. Intravenous hyoscine and glucagon is not widely used for diagnostic endoscopy because of its potential side effects and its cost. Topical peppermint oil was found to have an antispasmodic effect on the stomach comparable to that of hyoscine.42 43 For L-menthol, the active extracts from peppermint oil, Hiki et al reported a dose-dependent effect in suppressing gastric peristalsis and a positive correlation with the endoscopist’s ease of observation.44–46 None of the studies evaluated visual clarity, diagnostic yield or the detection rate of mucosal pathology.
Most experts commented that there was no evidence in the literature to support the use of antispasmodic agents in enhancing the detection of superficial upper GI neoplasia, but their use was recommended as there would be an indirect effect on the visual clarity of mucosal examination.
Statement 3.3: Use of mucolytic and/or defoaming agents is recommended for the improvement of visual clarity of OGD and IEE
Level of evidence: I
Level of recommendation: A
Level of acceptance: 100%
Three mucolytic/defoaming agents (N-acetylcysteine, pronase and simethicone) have been investigated in RCTs either as single or combination regimens.47–50 The use of simethicone (either alone or in combination) allows significantly better visual clarity under upper endoscopy.47–49 The addition of N-acetylcysteine did not increase mucosal visibility if simethicone was given beforehand.49 51 Two systematic reviews and meta-analyses yielded contradictory results regarding the addition of pronase to simethicone to improve mucosal clarity.51 52 One recent RCT found that pronase significantly improved visibility in the proximal stomach and endoscopists’ satisfaction compared with control (P=0.014 and P=0.034, respectively).53 While the diagnostic performance of NBI endoscopy to detect IM did not differ in either group, the negative predictive value of NBI endoscopy showed a significant improvement over that of white light endoscopy (WLE) only in the pronase group (P=0.013). The consensus panel found that the current evidence supported the use of simethicone for improving visibility during OGD as one RCT had shown that pronase improved the negative prediction rate of IEE.
Statement 4: Systematic endoscopic mapping of the entire oesophagus and stomach may improve the detection rate of UGI superficial neoplasm
Level of evidence: III
Level of recommendation: C
Level of acceptance: 100%
The rate of missing an upper GI cancer during OGD was 2.3–13.9% in the West, and >20% with regard to gastric cancer in Asia.54 55 A meta-analysis showed that 11.3% of upper GI cancers were missed during OGD performed up to 36 months before diagnosis.56 There are some locations of the upper GI tract where risks of missing cancer are high during OGD.26 28 57 Endoscopic photo-mapping during OGD may decrease the possibility of missing lesions at these high-risk areas. Yao et al proposed a systematic screening protocol for the stomach (SSS).58 In this protocol, a total of 22 endoscopic photos from three to four quadrants at specific locations in the stomach would be taken either in a clockwise or counter-clockwise manner. A study from China reported that training in the diagnosis of EGC, which included a systematic inspection protocol that required at least 20 photographic images to be taken, improved the EGC detection rate from 0.2% to 2.3%.59
In summary, there was no well-designed study that directly evaluated the effect of systematic photo-mapping for OGD on improving the detection rate of superficial upper GI neoplasia. However, the panel agreed that systematic observation of the upper GI tract would improve the detection of superficial neoplasia by avoiding blind spots.
Statement 5: Sufficient examination time is recommended to increase detection rate of upper GI superficial neoplasm
Level of evidence: II
Level of recommendation: B
Level of acceptance: 89%
Examination time remains one of the most subjective operator dependent aspects of diagnostic endoscopy.60 Ideally, the longer the examination time, the better the detection rate of significant pathologies during endoscopy. However, time is limited in clinical practice and lengthening procedures will likely result in a higher requirement for sedation and reduced patient tolerability. It will also have significant resource implications for endoscopy centres.
A multicentre prospective study revealed that lengthening (>1 min/cm) the Barrett’s inspection procedure resulted in a higher detection rate of HGD and adenocarcinoma (P=0.001).61 In a single-centre retrospective trial in Singapore, endoscopists who spent a mean OGD time of longer than 7 min were twice as likely to detect high-risk lesions (OR 2.50, 95% CI 1.52 to 4.12) and three times as likely to detect neoplastic lesions (OR 3.42, 95% CI 1.25 to 10.38) than their counterparts who conducted shorter examinations.62 A similar Japanese study indicated that moderate (5–7 min) and slow (>7 min) endoscopists for OGD identified about twice as many neoplastic lesions (OR 1.90, 95% CI 1.06 to 3.40, and 1.89, 95% CI 0.98 to 3.64, respectively) than quicker (<5 min) endoscopists.63 Park et al retrospectively analysed the data of 111 962 patients who underwent OGD in a health-screening programme and found that slow endoscopists were more likely to detect gastric adenoma or carcinoma.64
An adequate examination time plays an important role in enhancing the detection rate of early upper GI neoplasia. This will also serve as an important quality indicator for OGD among endoscopy centres. A systematic endoscopic observation of the upper GI tract, including the taking of a standard minimum number of photos, should take a procedural time of 8 min.54
Statement 6: Structured training improves the detection rate of upper GI superficial neoplasm
Level of evidence: II-3
Level of recommendation: C
Level of acceptance: 97%
The diagnosis of early GI neoplasia is a two-step process which requires endoscopists to identify the suspicious lesion and differentiate its pathology. Training in endoscopic diagnosis should not merely seek to improve technical skills, but should also include a cognitive- and knowledge-based protocol.
A prospective RCT showed in-classroom teaching on NBI diagnosis for Barrett’s neoplasm yielded a higher percentage of high-confidence answers to diagnosis than self-directed web learning, but there was no difference in overall accuracy between the two learning groups. The authors concluded that self-directed web learning may be adequate because it can be accessed and repeated at any time.65 A multicentre prospective study showed that a web-based video learning programme for NBI diagnosis of precancerous gastric lesions produced an improvement in global accuracy, specificity for gastric IM and sensitivity for dysplasia.66 Mabe et al demonstrated a significant improvement in test scores for magnifying NBI diagnosis of EGC after an educational lecture on vessel plus surface (VS) classification.67 Yao et al developed an e-learning programme on the detection of EGC in WLE68 and investigated its usefulness in an RCT that enrolled 332 endoscopists from 35 countries around the world.69 The improvement of test scores in the e-learning group was significantly higher than in the non-e-learning group. Although most studies indicated an improvement in test results for e-learning, one observational study suggested the effectiveness of a voluntary training programme in increasing the detection rate of EGC in a ‘real-world’ clinical setting.70
Structured training improves the knowledge and recognition skills of endoscopists in the diagnosis of early upper GI cancers. This in turn should improve the effectiveness of endoscopic detection and characterisation of the disease in clinical practice.
Statement 7.1: IEE in addition to WLI improves the detection rate for oesophageal superficial neoplasm
Level of evidence: I
Level of recommendation: A
Level of acceptance: 100%
There are two main types of IEE: dye-based IEE (chromoendoscopy) and equipment-based IEE, which includes techniques such as NBI, flexible spectral imaging colour enhancement (FICE), blue laser/light imaging (BLI), i-SCAN and optical enhancement i-SCAN.71 Iodine chromoendoscopy enhances the detection of superficial oesophageal SCC as an iodine-unstained area, especially when it cannot be observed in WLE.7 72 Iodine chromoendoscopy increases sensitivity for dysplastic/cancerous lesions to 96% compared with only 62% with WLE. A multicentre prospective RCT demonstrated that NBI detected superficial oesophageal SCC more frequently than WLI (97% v 55%, P<0.001) (figure 6).73 In a multicentre RCT comparing high definition WLE with NBI for the detection of Barrett’s neoplasm, NBI detected more dysplastic areas (30% vs 21%, P=0.01) than WLE.74 A meta-analysis concluded that IEE increased the diagnostic yield for detection of dysplasia or cancer by 34% (95% CI 20% to 56%; P<0.0001).75 IEE improves the detection rate of both superficial oesophageal SCC and Barrett’s oesophagus associated dysplasia.

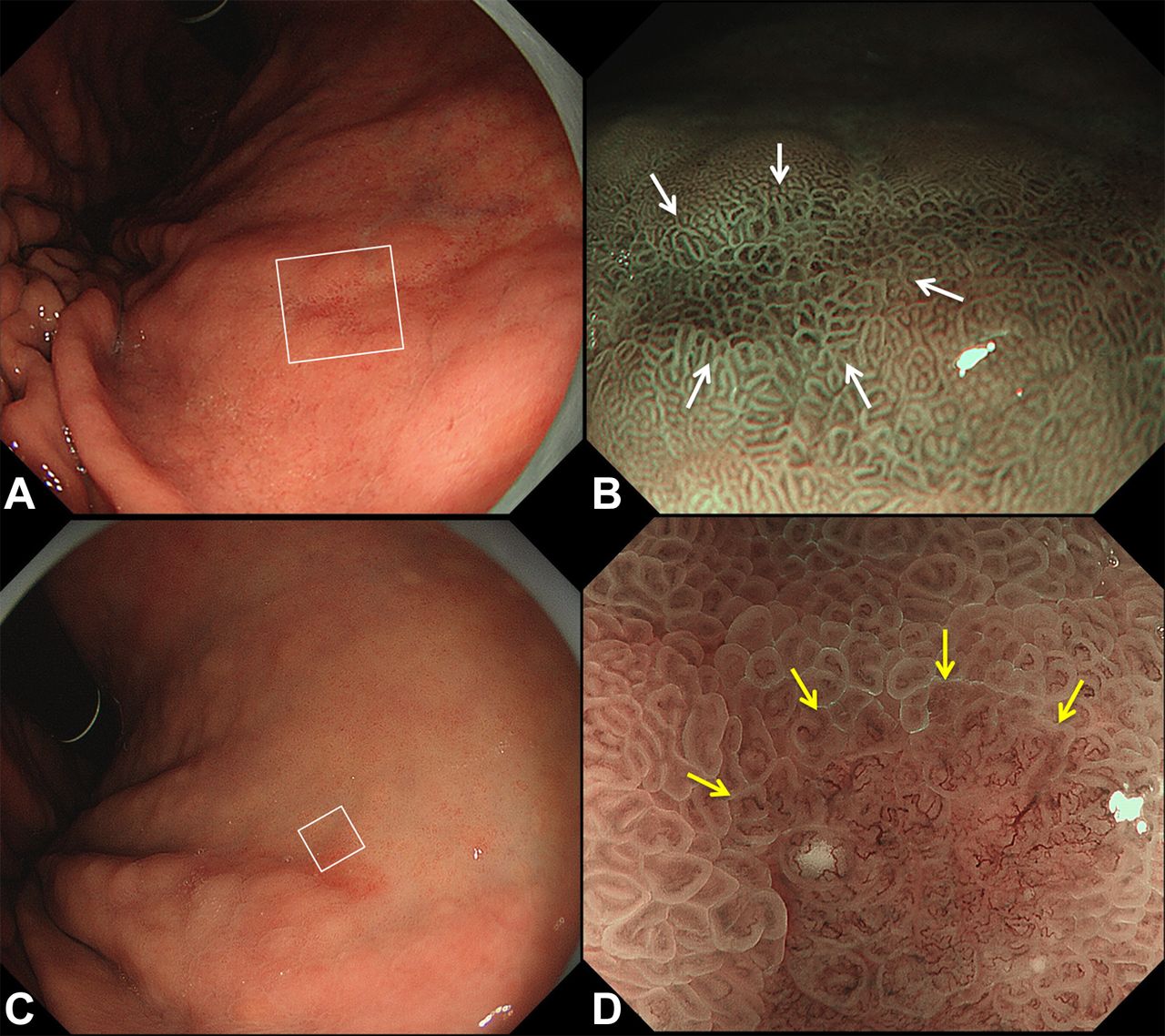
A case of Helicobacter pylori associated chronic atrophic gastritis. (A) A small depressed lesion was found in the gastric corpus. (B) In a magnifying narrow band image (NBI) (white box in A), the lesion was demarcated but there were regular microsurface and regular microvessels within the demarcation line (white arrows). (C) A case of small early gastric cancer. A small reddish area was seen in the gastric corpus. (D) In a magnifying NBI image (white box in C), the lesion was demarcated (yellow arrows) and there were irregular microvessels within the demarcation line.
Statement 7.2: IEE in addition to WLI improves the detection rate of gastric premalignant mucosal changes such as gastric intestinal metaplasia and atrophy
Level of evidence: I
Level of recommendation: A
Level of acceptance: 93%
A multicentre RCT reported that detection of gastric IM was significantly higher using NBI compared with WLE (17.7% vs 7.7%, P<0.001, figure 5).76 Another single centre RCT showed that NBI significantly increased the detection of IM and gastric atrophy.77 Endoscopic trimodal imaging using auto-fluorescence imaging (AFI) followed by NBI also increased the detection rate of IM (figure 3B).78 These RCTs supported the initial results from a number of prospective non-randomised tandem studies.79 80 In the case of gastric neoplasm, two non-randomised prospective crossover studies suggested that trimodal imaging can increase the detection rate of gastric neoplasm over WLE alone.81 82 A retrospective study reported that trimodal imaging significantly reduced the frequency of missed synchronous gastric lesions when compared with WLI (2.3% vs 9.3%, P<0.01).83 Accordingly, there is robust evidence that IEE increased the detection rate of premalignant gastric pathologies.

Patient with superficial oesophageal squamous cell carcinoma. (A) White light image did not show obvious mucosal changes. (B) In a narrow band image, slightly brownish areas were seen from 9 to 12 o’clock site. (C) Magnifying observation in the brownish area revealed irregular microvessels. The irregular microvessels maintained a loop structure and they were observed as ‘brownish dots’. (D) Iodine chromoendoscopy clearly visualised the lesion as a non-staining area.
Statement 8: IEE in addition to WLI is useful for the delineation of UGI superficial neoplasia
Level of evidence: II-2
Level of recommendation: B
Level of acceptance: 97%
Dye-based IEE without magnification in addition to WLI for the characterisation of superficial oesophageal neoplasm
Oesophageal HGD and carcinoma appear as non-stained areas with a pinkish colour with iodine-based chromoendoscopy.84 One observational study indicated that iodine chromoendoscopy improved lesion delineation in 88% of cases involving oesophageal HGD or SCC.85 Expert endoscopists proposed that iodine chromoendoscopy is indispensable for the accurate delineation of oesophageal SCCs, enabling the borders of the lesion to be accurately established before endoscopic treatment.86 87 Recent ESGE guidelines also supported the use of iodine chromoendoscopy especially during performance of endoscopic submucosal dissection (ESD) to delineate tumour margins.88
Dye-based IEE without magnification in addition to WLI may be useful for the characterisation of early gastric neoplasm
Chromoendoscopy with indigo carmine contrasts the surface topography of the gastric mucosa, provides better recognition of morphological characteristics and improves lesion characterisation and delineation. Accurate morphological characterisation may facilitate targeted biopsy as well as margin delineation for endoscopic resection.
Indigo carmine can be used separately or in combination with acetic acid.89–92 A meta-analysis showed that any chromoendoscopy including indigo carmine was superior to WLE for diagnosis of EGC in terms of sensitivity and specificity, and that the addition of acetic acid further improved diagnostic accuracy.93 Several observational studies have indicated the usefulness of combining indigo carmine with acetic acid for delineation of EGC. A recent multicentre RCT showed that the diagnostic performance of indigo carmine chromoendoscopy was similar to that of magnifying NBI for delineating EGC.94
The performance of chromoendoscopy requires the preparation of dye, but it does not require the use of specialised and expensive equipment. Moreover, the preparatory time for chromoendoscopy should be reasonable. Hence the consensus panel recommended the use of chromoendoscopy for characterisation and delineation of EGC.
Equipment-based IEE without magnification for the characterisation of superficial oesophageal neoplasm
When non-magnifying NBI was compared with iodine chromoendoscopy for the detection of oesophageal SCC, NBI demonstrated higher accuracy (77% vs 68%, P=0.03) and specificity (75.2% vs 64%, P=0.01).95 In the opinion of the expert panel, IEE can achieve better delineation of the tumour extent for superficial oesophageal neoplasia. However, further well-designed studies will be needed to quantify its efficacy.
Equipment-based IEE without magnification for the characterisation of early gastric neoplasm
New-generation IEEs (second-generation NBI and BLI) provide brighter endoscopic images that enable an overview to be gained of the entire gastric mucosa. Pimentel-Nunes et al proposed diagnostic criteria to characterise gastric premalignant lesions including chronic gastritis, IM and carcinoma using non-magnifying NBI,96 and these criteria were validated in a multicentre prospective cohort study.37 One observational study indicated that diagnostic accuracy for differentiating adenocarcinoma from benign gastric lesions was significantly higher in non-magnification NBI than in WLE (92.3% vs 61.5%).97 At present, the consensus panel recommended the use of equipment-based IEE without magnification for characterisation and delineation of EGC as evidenced by the accuracy of IEE without magnification demonstrated in prospective cohort studies.96 97
Statement 9: Magnifying endoscopy with NBI is recommended for better characterisation of upper GI superficial neoplasm
Level of evidence: I
Level of recommendation: A
Level of acceptance: 100%
Oesophageal SCC
A multicentre RCT showed the superiority of magnifying NBI for the diagnosis of superficial oesophageal SCC compared with conventional WLE with accuracy similar to histological diagnosis on biopsy (figure 5c).73 98
Oesophageal adenocarcinoma
Two systematic reviews indicated that magnifying NBI had high diagnostic precision for HGD in Barrett’s oesophagus, based on an irregular microsurface and/or an irregular microvascular pattern.99 100
Gastric adenocarcinoma
A multicentre RCT demonstrated that a combination of WLE and magnifying NBI for small depressed type EGC achieved sensitivity of 95.0%, specificity of 96.8% and accuracy of 96.6%. These results were significantly better than those achieved with WLE or magnifying NBI alone (figure 6).101 102 A multicentre prospective cohort study using VS classification confirmed the excellent diagnostic performance of magnifying NBI for the diagnosis of EGC, with accuracy, sensitivity and specificity of 98.1%, 85.7% and 99.4%, respectively.103 In VS classification, the presence and absence of (1) a demarcation line and (2) an irregular microvessel pattern and/or irregular surface pattern were evaluated. Three meta-analyses support the efficacy of magnifying endoscopy for diagnosis of EGC.104–106 Based on these results, experts recommended the algorithm ‘magnifying endoscopy simple diagnostic algorithm for early gastric cancer (MESDA-G)’ to enhance the detection and characterisation of early gastric cancers (figure 7).107

Magnifying endoscopy simple diagnostic algorithm for early gastric cancer (MESDA-G). A suspicious lesion is assessed for the presence or absence of a demarcation line and/or irregular colour or surface in white light endoscopy. First, the lesion is evaluated for a demarcation line. If it is not present we can confidently make a diagnosis of ‘non-cancer’. When the lesion has a demarcation line, the presence (or absence) of an irregular microstructure and/or microvessel patterns are essential to make a diagnosis of cancer (or non-cancer). IMSP; irregular microsurface pattern; IMVP, irregular microvessel pattern.
Statement 10: Endoscopic characterisation with IEE avoids unnecessary biopsies for upper GI superficial lesions
Level of evidence: I
Level of recommendation: B
Level of acceptance: 97%
Biopsy from a suspicious lesion is necessary to prove it is a neoplasm that requires treatment. However, it is possible to avoid biopsy if endoscopic diagnosis provides a high rate of accuracy for benign lesion diagnosis as well as a high rate of negative predictive value of malignant change.
Oesophageal SCC
A prospective cohort study revealed that NBI and probe-based confocal laser endomicroscopy (pCLE) both provided excellent diagnostic accuracy and reduced the number of biopsies needed to be taken for diagnosis in iodine non-stained areas representing the presence of early oesophageal SCC.108
Oesophageal adenocarcinoma
Sharma et al conducted a multicentre RCT that compared high definition WLE using four quadrant biopsies every 2 cm, together with targeted biopsies from visible lesions (Seattle protocol) with NBI for detection of IM and Barrett’s neoplasia.74 The study showed that both WLI and NBI detected 104/113 (92%) patients with IM, but NBI required fewer biopsies per patient (3.6 vs 7.6, P<0.0001).74 The recent meta-analysis concluded that NBI was useful for the diagnosis of dysplasia in Barrett’s oesophagus, with sensitivity at 91% and specificity at 95%.109 This fulfils the Preservation and Incorporation of Valuable Endoscopic Innovations (PIVI) criteria.110 However, it should be noted that the latest guideline in 2016 by the American College of Gastroenterology recommended that at least eight biopsies should be taken in patients with Barrett’s oesophagus.111
Gastric adenocarcinoma
A prospective cohort study showed that the use of magnifying NBI could reduce the number of biopsies required for the detection of EGC103 (figure 8).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Strategy of biopsy for screening gastroscopy with magnifying narrow band imaging (NBI). The entire gastric mucosa is screened with white light endoscopy for a suspicious lesion. When the lesion is a pale colour, a biopsy is performed from the lesion. When the lesion looks reddish, it is evaluated with magnifying NBI for the presence and absence of a demarcation line and/or an irregular microsurface/microvessel pattern. If the diagnosis cannot be made with high confidence, the biopsy is recommended. If the diagnosis is made with high confidence, especially if it is benign, a biopsy could be avoided. C-WLI, conventional white light endoscopy; M-NBI, magnifying narrow band imaging.
Discussion
Upper GI cancers are difficult to recognise at the early stage. Chadwick et al studied a cohort of 2727 patients who had gastric cancer and reported that 8.3% had received an upper endoscopy 3 to 36 months before diagnosis.112 There are multiple reasons for missing early upper GI cancers during endoscopy. Most of these early cancers are only represented by subtle changes in microstructural and microvascular patterns, and the inability to recognise these changes during endoscopy could be related to inadequate training, limited use of IEE, and an insufficiently systematic approach involving incomplete examination and inadequate preparation of the mucosa to enhance recognition. The current consensus on diagnostic upper GI endoscopy aims to unify clinical practice, as well as improve the quality and standards in diagnostic endoscopy.
Recently, the British Society of Gastroenterology (BSG) and the Association of Upper Gastrointestinal Surgeons of Great Britain and Ireland (AUGIS) published a position statement on quality standards in upper GI endoscopy.113 These statements were developed according to the patient management pathway, including pre-procedure, procedure, disease specific and post-procedure management issues. This quality standards position statement differs from our current Asian consensus, in that the Asian consensus focused on endoscopic diagnosis of early GI neoplasia while the quality standards position statement was established from a general approach to the performance of diagnostic endoscopy. As far as improvements in diagnostic endoscopy are concerned, the two statements are complementary. The BSG statement is aimed at ensuring a systematic approach to diagnosis and requires photographic documentation at relevant anatomical landmarks and recognised lesions, adequate mucosal visualisation, and inspection time during a diagnostic OGD to be recorded for surveillance procedures. This Asian consensus will standardise the procedure and approach to the recognition and characterisation of early upper GI neoplasia.
The Western endoscopy societies have issued practice guidelines for endoscopic management of premalignant and malignant condition/lesions in the oesophagus114 115 and the stomach.116 Most guidelines recommend use of WLE and/or random biopsies to make a diagnosis of those premalignant lesions, but they do not include endoscopic practice for detection and characterisation of early upper GI cancers using IEE. The management of precancerous conditions and lesions in the stomach (MAPS) guideline3 suggested use of NBI with/without magnifying endoscopy, but it was not strongly endorsed because of limited evidence at that time. Accumulated recent evidence on IEE was reflected in this consensus. Because this consensus was drafted from Asian experts, the consensus may be more applicable among Asian countries, especially where the incidence of gastric cancer and squamous oesophageal cancer is moderate to high. However, when the expert panel developed the consensus, differences among Asian countries or between East and West were not considered. We believe that this consensus will lead to an improvement in diagnostic endoscopy by standardising the procedures, preparation and training around the world.
References
Footnotes
Contributors PWYC is responsible for overall coordination and planning of the consensus meetings, drafting and critical appraisal of statement 6, writing and editing of the manuscript. NU is responsible for drafting and critical appraisal of statement 1 as well as writing and editing of the manuscript. RS is responsible for drafting and critical appraisal of statement 1 and the manuscript, as well as participation as an expert in the consensus meeting. TG is responsible for drafting and critical appraisal of statement 2 and the manuscript, as well as participation as an expert in the consensus meeting. EKWN is responsible for drafting and critical appraisal of statement 3 and the manuscript, as well as participation as an expert in the consensus meeting. KY is responsible for drafting and critical appraisal of statement 9 and the manuscript, as well as participation as an expert in the consensus meeting. TLA is responsible for drafting and critical appraisal of statement 7 and the manuscript, as well as participation as an expert in the consensus meeting. SHH is responsible for drafting and critical appraisal of statement 5 and the manuscript, as well as participation as an expert in the consensus meeting. DK is responsible for drafting and critical appraisal of statement 8 and the manuscript, as well as participation as an expert in the consensus meeting. FY is responsible for drafting and critical appraisal of statement 4 and the manuscript, as well as participation as an expert in the consensus meeting. RP is responsible for drafting and critical appraisal of statement 10 and the manuscript, as well as participation as an expert in the consensus meeting. KG is responsible for drafting and critical appraisal of statement 8 and the manuscript, as well as participation as an expert in the consensus meeting. JYWL, HT, HI is responsible for drafting and critical appraisal of the manuscript, as well as participation as an expert in the consensus meeting.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests The consensus meeting is supported by a non-government organisation named Asian Novel Bio-Imaging and Intervention Group (ANBIG) which focused on training and education of endoscopic diagnosis and management of early gastrointestinal cancers in Asia. All the authors are members of ANBIG. The manuscript underwent editorial review by a professional academic English editor.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.