
Abstract
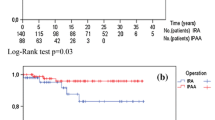
Increasing numbers of polyposis registries have led to more young patients being diagnosed with familial adenomatous polyposis (FAP). To provide guidelines for selecting the appropriate surgical procedure in teenagers (10–19 years), we compared the results of colectomy and ileo-rectal anastomosis (IRA, n=17 patients) to the results of resrorative proctocolectomy and ileal pouch-anal anastomosis (IPAA, n=7 patients). Charts were reviewed to obtain data on the operative technique, blood loss and transfusions, hospital stay (including the time for ileostomy closure), and early (within 30 days of surgery) and late complications. Functional results (bowel movements per 24h, use of antidiarrheal drugs, seepage, and fecal incontinence) and quality of life were evaluated prospectively with a questionnaire and physical examination. The median follow-up time was 49 months (range, 6 to 95 months) after IRA, and 36 months after IPAA (range, 4 to 87 months). Although restorative proctocolectomy and IPAA, is a longer (5.75 vs 3.1 hours), more bloody (500 vs 300 mL blood loss), and more complex operation with a longer hospital stay (12 vs 7 days) than IRA (P=0.008, P=0.006, P=0.02, respectively), no significant difference (P>0.05) was found between groups concerning the complication rate or quality of life. For teenagers with FAP and rectal carpeting, large rectal adenomas, curable cancer in the upper two-thirds of the rectum, or who are unavailable for follow-up, we recommend a restorative proctocolectomy and IPAA. For the other patients, the decision whether to perform IRA or restorative proctocolectomy with IPAA depends on the patient's desire and the surgeon's skill.
Résumé
La multiplication des registres de polypose a permis de diagnostiquer un nombre croissant de sujets jeunes proteurs d'une polypose adénomateuse familiale (FAP). Afin d'établir des recommandations dans la sélection du traitement chirurgical approprié chez des adolescents (10–19 ans), nous avons comparé les résultats de la colectomie et de l'anastomose iliéo-rectale (IRA, n=17 patients) aux résultats de procto-colectomie avec rétablissement de la continuité par l'intermédiaire d'une poche iléoanale (IPAA, n=7 patients). Les dossiers ont été revus afin d'obtenir des données sur la technique opératoire, les pertes sanguines et les transfusions, la durée de séjours hospitaliers (incluant la période nécessaire pour la fermeture de l'iléostomie), ainsi que les complications précoces (à moins de 30 jours de l'opération) et les complications tardives. Les résultats fonctionnels (nombre de selles par 24 h, usage de médications anti-diarrhéïques, fuites et incontinence fécale) et la qualité de la vie ont été évalués prospectivement à l'aide d'un questionnaire et de consultations de contrôle. Le suivi moyen a été de 49 mois (de 6 à 95 mois) après l'IRA et de 36 mois après l'IPAA (de 4 à 87 mois). Bien que la colo-poctectomie avec rétablissement de la continuité par IPAA soit plus longue (5,75-heures vs 3,1) plus sanglante (500 ml pertes sanguines vs 300 ml) et plus complexe avec un séjour hospitalier plus long (12 jours vs 7 jours) que l'IRA (P=0.008, P=0.006 et P=0.002), nous n'avons pas observé de différence P>0.05 entre les deux groupes en ce qui concerne le taux de complecations et la qualité de vie. Nous recommandons une colo-proctectomie avec rétablissement de la continuité par une IPAA chez des adolescents porteurs d'une polypose adénomateuse familiale et de tapis d'adénome du rectum présentant des cancers curables des deux tiers supérieurs du rectum chez lesquels le follow-up ne pourra que difficilement être assuré. Dans les autres cas, la décision de réaliser une IRA ou une procto-colectomie avec IPAA dépend des souhaits du patient et de l'expérience du chirurgien.
Similar content being viewed by others

References
Jagelman DG (1986) Choice of operation in familial adenomatous polyposis. Ann Chir Gynaecol 75:71–74
Sarre RG, Jagelman DG, Beck GJ, McGannon E, Fazio VW, Weakley FL, Lavery IC (1987) Colectomy with ileorectal anastomosis for familial adenomatous polyposis: the risk of rectal cancer. Surgery 101:20–26
Slors JFM, Jager FCA, Trum JW, Taat CW, Brummelkamp WH (1989) Long-term follow-up after colectomy and ileorectal anastomosis in familial adenomatous polyposis coli. Is there still a place for the procedure? Hepatogastroenterol 36:109–112
De Cosse JJ, Bulow A, Neale K, Jarvinen H, Alm T, Hultcrantz R, Moesgaard F, Costello C (1992) Rectal cancer risk in patients treated for familial adenomatous polyposis. Br J Surg 79:1372–1375
Wexner SD, Wong WD, Rothenberger DA (1990) The ileoanal reservoir. Am J Surg 159:178–183
Tjandra JJ, Fazio VW (1993) The ileal pouch-indications for its use and results in clinical practice. Curr Pract Surg 5:22–28
Madden MV, Neale KF, Nicholls RJ, Landgrebe JC, Chapman PD, Bussey HJR, Thompson JPS (1991) Comparison of morbidity and function after colectomy with ileorectal anastomosis or restorative proctocolectomy for familial adenomatous polyposis. Br J Surg 78:789–792
Jagelman DG (1991) Ileorectal anastomosis-familial adenomatous polyposis. Hepato-Gastroenterol 38:535–537
Bess MA, Adson MA, Adson LR, Moertel CG (1980) Rectal cancer following colectomy for polyposis. Arch Surg 115:460–467
Bussey HJR (1975) Family studies, histopathology, differential diagnosis and results of treatment. In: Bussey HJR (ed) Familial polyposis coli. The John Hopkins University Press, Baltimore, pp 1–75
O'Connell PR, Pemberton JH, Weiland LH, Beart RW, Dozois R, Wolffe BG, Telander RL (1987) Does rectal mucosa regenerate after ileoanal anastomosis? Dis Colon Rectum 30:1–5
Motta JC, Ricketts RR (1992) The J-pouch Swenson procedure for ulcerative colitis and familial polyposis. Am Surg 58:613–617
Perrault J, Telander RL, Zinsmeister AR, Kaufman B (1988) The endorectal pull-through procedure in children and young adults: a follow-up study. J Pediatr Gastroenterol Nutr 7:89–94
Wesson DE (1988) Early results with the J-pouch procedure in children. Can J Surg 31:182–184
Odgwe L, Sherman PM, Filler R, Shandling B, Wesson D (1987) Straight ileoanal anastomosis and ileal pouch-anal anastomosis in the surgical management of idiopathic ulcerative colitis and familial polyposis coli in children: follow-up and comparative analysis. J Pediatr Gastroenterol Nutr 6:426–429
Fonkalsrud EW, Loar N (1992) Long-term results after colectomy and endorectal ileal pullthrough procedure in children. Ann Surg 215:57–62
Winslet MC, Barsoum G, Pringle W, Fox K, Keighley MR (1991) Loop ileostomy after IPAA-is it necessary? Dis Colon Rectum 34:267–270
Nugent KR, Phillips RKS (1992) Rectal cancer risk in older patients with familial adenomatous polyposis: a cause for concern. Br J Surg 79:1204–1206
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Ziv, Y., Church, J.M., Oakley, J.R. et al. Surgery for the teenager with familial adenomatous polyposis: ileo-rectal anastomosis or restorative proctocolectomy?. Int J Colorect Dis 10, 6–9 (1995). https://doi.org/10.1007/BF00337577
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF00337577