
Abstract
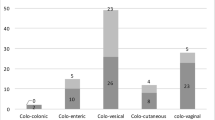
This study was undertaken to assess the appropriate management of patients with diverticulitis complicated by fistula formation. A retrospective chart review was conducted on patients with symptoms of a fistula who presented between 1975 to 1995. There were 42 patients (32 women, 76%; 10 men, 24%) who ranged in age from 46 to 89 years (mean 69.8±9.8). Six patients had multiple fistulas. The types of fistulas included colovesical (48%), colovaginal (44%), colocutaneous (4%), colotubal (2%), and coloenteric (2%). Operative procedures consisted of resection and primary anastomosis in 38 patients and a Hartmann's operation in one. Three patients were managed conservatively with antibiotics (two due to poor performance status, the third due to resolution of symptoms). There were no operative deaths. The postoperative course was uncomplicated in 69%, while 12 patients (31%) experienced 19 complications (40%). These consisted of urinary tract infection (9.5%), atelectasis (7.1%), prolonged ileus (4.8%), arrhythmias (4.8%) and renal failure, myocardial infarction, pseudomembranous colitis, peroneal nerve palsy, unexplained fever, pulmonary edema (2.4% each). There were no anastomotic leaks and no deaths. Hospital stay ranged from 6 to 31 days (mean 12.3±7.6). Fistulas due to diverticulitis were safely managed by resection and primary anastomosis without mortality and with acceptable morbidity in this series. Patients deemed to be poor operative risks can be managed with a course of nonoperative treatment.
Résumé
Cette étude a été entreprise afin de déterminer le traitement optimal des patients porteurs d'une diverticulite compliquée de fistule. Les dossiers des patients souffrant de fistule traités entre 1975 et 1995 ont été revus. Le collectif comporte 42 patients: 32 femmes (76%) et 10 hommes (24%) âgés de 46 à 89 ans (moyenne = 69,8 ans). Six patients ont des fistules multiples. Les fistules présentes sont colo-vésicales (48%), colo-vaginales (44%), colocutanées (4%), colo-tubaires (2%) et colo-entériques (2%). Le traitement chirurgical a consisté en une résection et une anastomose primaire chez 36 patients et une opération de Hartmann chez un sujet. Trois patients ont été traités de manière conservatrice avec des antibiotiques (2 en raison d'un mauvais état général, le troisième en raison d'une résolution de la symptomatologie). Aucune mortalité opératoire n'est à déplorer. La période post-opératoire a été sans complication chez 69% des patients alors que chez 12 patients (31%), on relève 19 complications (40%). Ces complications consistent en une infection urinaire (9,5%), une atélectase (1%), un iléus prolongé (4,8%), des arythmies (4,8%) et une insuffisance rénale, un infarctus du myocarde, une colite pseudo-membraneuse, une paralysie du nerf péronien, une fièvre inexpliquée, un oedème pulmonaire (2,4%) pour chacune de ces complications. Il n'y a aucune fuite anastomotique ni aucune mortalité. La durée des séjours va de 6 à 31 jours (moyenne 11,5 jours). Les fistules dues à la diverticulite peuvent être traitées de manière sûre par résection et anastomose primaire sans mortalité et avec une morbidité acceptable dans cette série. Les patients présentant de mauvais risques opératoires peuvent être traités de manière non opératoire.
Similar content being viewed by others


Author information
Authors and Affiliations
Additional information
Accepted: 21 November 1997
Rights and permissions
About this article
Cite this article
Vasilevsky, CA., Belliveau, P., Trudel, J. et al. Fistulas complicating diverticulitis. Int J Colorect Dis 13, 57–60 (1998). https://doi.org/10.1007/s003840050135
Issue Date:
DOI: https://doi.org/10.1007/s003840050135