
Abstract
Background
Barrett’s esophagus is a well-known acquired condition resulting from gastroesophageal reflux disease (GERD). However, it is still unknown whether Barrett’s esophagus develops gradually over time in patients with GERD. To address this issue, we investigated the change in the prevalence and length of short-segment Barrett’s esophagus (SSBE) over time.
Methods
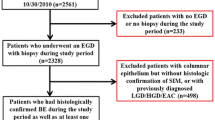
From January 2005 to March 2007, we enrolled 5338 patients who received upper gastrointestinal endoscopy. Prevalence and length of endoscopically identified SSBE were evaluated within groups divided on the basis of 10-year age intervals. The factors possibly influencing SSBE length such as symptoms, antacid use, and endoscopic findings were also evaluated. Additionally, the length change in 236 patients with histologically confirmed Barrett’s esophagus was evaluated over a 2-year follow-up.
Results
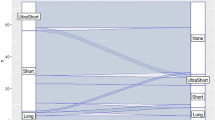
Of the 5338 enrolled patients, 1997 had SSBE. The prevalence of endoscopically identified SSBE was significantly higher and its length was significantly longer in elderly patients. Multiple regression analysis showed that age, presence of reflux esophagitis, reflux symptoms, and hiatal hernia were positively correlated with SSBE length. Analysis of the 2-year follow-up study of histologically confirmed SSBE revealed significant extension of Barrett’s length in 28.0% of 236 patients. Presence of reflux symptoms and hiatal hernia were identified as positive predictors and proton pump inhibitor administration as a negative predictor of SSBE elongation.
Conclusions
Positive predictors for the extension of SSBE were presence of hiatal hernia and reflux symptoms, but not age.
Similar content being viewed by others

References
Cameron AJ, Zinsmeister AR, Ballard DJ, Carney JA. Prevalence of columnar-lined (Barrett’s) esophagus. Comparison of population-based clinical and autopsy findings. Gastroenterology 1990;99:918–922.
Pera M, Cameron AJ, Trastek VF, Carpenter HA, Zinsmeister AR. Increasing incidence of adenocarcinoma of the esophagus and esophagogastric junction. Gastroenterology 1993;104:510–513.
Fass R, Ofman JJ. Gastroesophageal reflux disease-should we adopt a new conceptual framework? Am J Gastroenterol 2002;97:1901–1909.
Cameron AJ, Lomboy CT. Barrett’s esophagus: age, prevalence, and extent of columnar epithelium. Gastroenterology 1992;103:1241–1245.
Fass R, Hell RW, Garewal HS, Martinez P, Pulliam G, Wendel C, et al. Correlation of oesophageal acid exposure with Barrett’s oesophagus length. Gut 2001;48:310–313.
Tharalson EF, Martinez SD, Garewal HS, Sampliner RE, Cui H, Pulliam G, et al. Relationship between rate of change in acid exposure along the esophagus and length of Barrett’s epithelium. Am J Gastroenterol 2002;97:851–856.
Peters FT, Ganesh S, Kuipers EJ, Sluiter WJ, Klinkenberg-Knol EC, Lamers CB, et al. Endoscopic regression of Barrett’s oesophagus during omeprazole treatment; a randomised double blind study. Gut 1999;45:489–494.
Malesci A, Savarino V, Zentilin P, Belicchi M, Mela GS, Lapertosa G, et al. Partial regression of Barrett’s esophagus by longterm therapy with high-dose omeprazole. Gastrointest Endosc 1996;44:700–705.
Schell TG. Acid suppression and adenocarcinoma of the esophagus: cause or cure? Am J Gastroenterol 2004;99:1884–1886.
El-Serag HB, Aguirre TV, Davis S, Kuebeler M, Bhattacharyya A, Sampliner RE. Proton pump inhibitors are associated with reduced incidence of dysplasia in Barrett’s esophagus. Am J Gastroenterol 2004;99:1877–1883.
Hillman LC, Chiragakis L, Shadbolt B, Kaye GL, Clarke AC. Proton-pump inhibitor therapy and the development of dysplasia in patients with Barrett’s oesophagus. Med J Aust 2004;180:387–391.
Sharma P, Sampliner RE, Camargo E. Normalization of esophageal pH with high-dose proton pump inhibitor therapy does not result in regression of Barrett’s esophagus. Am J Gastroenterol 1997;92:582–585.
Weston AP, Badr AS, Hassanein RS. Prospective multivariate analysis of factors predictive of complete regression of Barrett’s esophagus. Am J Gastroenterol 1999;94:3420–3426.
Sharma P. Barrett esophagus: will effective treatment prevent the risk of progression to esophageal adenocarcinoma? Am J Med 2004;117Suppl 5A:79S–85S.
Carlsson R, Dent J, Bolling-Sternevald E, Johnsson F, Junghard O, Lauritsen K, et al. The usefulness of a structured questionnaire in the assessment of symptomatic gastroesophageal reflux disease. Scand J Gastroenterol 1998;33:1023–1029.
Armstrong D. Review article: towards consistency in the endoscopic diagnosis of Barrett’s oesophagus and columnar metaplasia. Aliment Pharmacol Ther 2004;20Suppl 5:40–47.
Sharma P, Dent J, Armstrong D, Bergman JJ, Gossner L, Hoshihara Y, et al. The development and validation of an endoscopic grading system for Barrett’s esophagus: the Prague C & M criteria. Gastroenterology 2006;131:1392–1399.
Lundell LR, Dent J, Bennett JR, Blum AL, Armstrong D, Galmiche JP, et al. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification. Gut 1999;45:172–180.
Amano K, Adachi K, Katsube T, Watanabe M, Kinoshita Y. Role of hiatus hernia and gastric mucosal atrophy in the development of reflux esophagitis in the elderly. J Gastroenterol Hepatol 2001;16:132–136.
Kimura K, Takemoto T. An endoscopic recognition of the atrophic border and its significance in chronic gastritis. Endoscopy 1969;3:87–97.
Asayama M, Shibata M, Kondo Y, Tauchi M, Yanagawa T, Sato S, et al. Retrospective cohort study of chronological change of short-segment Barrett’s esophagus. Dig Endosc 2005;17:28–31.
Gopal DV, Lieberman DA, Magaret N, Fennerty MB, Sampliner RE, Garewal HS, et al. Risk factors for dysplasia in patients with Barrett’s esophagus: results from a multicenter consortium. Dig Dis Sci 2003;48:1537–1541.
Schnell TG, Sontag SJ, Chejfec G. Adenocarcinoma arising in tongues or short segments of Barrett’s esophagus. Dig Dis Sci 1992;37:137–143.
Drewitz DJ, Sampliner RE, Garewal HS. The incidence of adenocarcinoma in Barrett’s esophagus: a prospective study of 170 patients followed 4.8 years. Am J Gastroenterol 1997;92:212–215.
Sharma P, Morales TG, Bhattacharyya A, Garewal HS, Sampliner RE. Dysplasia in short-segment Barrett’s esophagus: a prospective 3-year follow-up. Am J Gastroenterol 1997;92:2012–2016.
Hirota WK, Loughney TM, Lazas DJ, Maydonovitch CL, Rholl V, Wong RK. Specialized intestinal metaplasia, dysplasia, and cancer of the esophagus and esophagogastric junction: prevalence and clinical data. Gastroenterology 1999;116:277–285.
Amano Y, Kushiyama Y, Ishihara S, et al. Barrett’s esophagus with predominant intestinal metaplasia correlates with superficial COX-2 expression, increased proliferation and reduced apoptosis: changes that are partially reversed by NSAIDs usage. Aliment Pharmacol Ther 2004;20:793–802.
Amano Y, Kushiyama Y, Yuki T, Yuki T, Takahashi Y, Chinuki D, et al. Prevalence of and risk factors for Barrett’s esophagus with intestinal predominant mucin phenotype. Scand J Gastroenterol 2006;41:873–879.
Dickman R, Green C, Chey WD, Jones MP, Eisen GM, Ramirez F, et al. Clinical predictors of Barrett’s esophagus length. Gastrointest Endosc 2005;62:675–681.
Avidan B, Sonnenberg A, Schnell TG, Sontag SJ. Hiatal hernia and acid reflux frequency predict presence and length of Barrett’s esophagus. Dig Dis Sci 2002;47:256–264.
Wakelin DE, Al-Mutawa T, Wendel C, Green C, Garewal HS, Fass R. A predictive model for length of Barrett’s esophagus with hiatal hernia length and duration of esophageal acid exposure. Gastrointest Endosc 2003;58:350–355.
Conio M, Filiberti R, Blanchi S, Ferraris R, Marchi S, Ravelli P, et al. Risk factors for Barrett’s esophagus: a case control study. Int J Cancer 2002;97:225–229.
Gerson LB, Shetler K, Triadafilopoulos G. Prevalence of Barrett’s esophagus in asymptomatic individuals. Gastroenterology 2002;123:461–467.
Voutilainen M, Färkkilä M, Juhola M, Nuorva K, Mauranen K, Mäntynen T, et al. Specialized columnar epithelium of the esophagogastric junction: prevalence and associations. The Central Finland Endoscopy Study Group. Am J Gastroenterol 1999;94:913–918.
Wilkinson SP, Biddlestone L, Gore S, Shepherd NA. Regression of columnar-lined (Barrett’s) oesophagus with omeprazole 40 mg daily: results of 5 years of continuous therapy. Aliment Pharmacol Ther 1999;13:1205–1209.
Ouatu-Lascar R, Fitzgerald RC, Triadafilopoulos G. Differentiation and proliferation in Barrett’s esophagus and the effects of acid suppression. Gastroenterology 1999;117:327–335.
Amano Y, Chinuki D, Yuki T, Takahashi Y, Ishimura N, Kazumori H, et al. Efficacy of proton pump inhibitors for cellular proliferation and apoptosis in Barrett’s oesophagus with different mucin phenotypes. Aliment Pharmacol Ther 2006;24Suppl 4:41–48.
Horwhat JD, Baroni D, Maydonovitch C, Osgard E, Ormseth E, Rueda-Pedraza E, et al. Normalization of intestinal metaplasia in the esophagus and esophagogastric junction: incidence and clinical data. Am J Gastroenterol 2007;102:497–506.
Overholt BF. Acid suppression and reepithelialization after ablation of Barrett’s esophagus. Dig Dis 2000–2001;18:232–239.
Biddlestone LR, Barham CP, Wilkinson SP, Barr H, Shepherd NA. The histopathology of treated Barrett’s esophagus: squamous reepithelialization after acid suppression and laser and photodynamic therapy. Am J Surg Pathol 1998;22:239–245.
Amano Y, Kushiyama Y, Yuki T, Takahashi Y, Chinuki D, Ishimura N, et al. Predictors for squamous re-epithelialization of Barrett’s esophagus after endoscopic biopsy. J Gastroenterol Hepatol 2007:22;901–907.
Neumann CS, Iqbal TH, Cooper BT. Long term continuous omeprazole treatment of patients with Barrett’s oesophagus. Aliment Pharmacol Ther 1995;9:451–454.
Katsube T, Adachi K, Furuta K, Miki M, Fujisawa T, Azumi T, et al. Difference in localization of esophageal mucosal breaks among grades of esophagitis. J Gastroenterol Hepatol 2006;21:1656–1659.
Edebo A, Vieth M, Tam W, Bruno M, van Berkel AM, Stolte M, et al. Circumferential and axial distribution of esophageal mucosal damage in reflux disease. Dis Esophagus 2007;20:232–238.
Moriyama N, Amano Y, Okita K, Mishima Y, Ishihara S, Kinoshita Y. Localization of early stage dysplastic Barrett’s lesion in patients with short segment Barrett’s esophagus. Am J Gastroenterol 2006;101:2666–2667.
Dekel R, Wakelin DE, Wendel C, Green C, Sampliner RE, Garewal HS, et al. Progression or regression of Barrett’s esophagus—is it all in the eye of the beholder? Am J Gastroenterol 2003;98:2612–2615.
Egger K, Meining A, Werner M, Höfler H, Classen M, Rösch T. Endoscopic measurement of Barrett’s esophagus length is unreliable—a prospective comparative biopsy study. Z Gastroenterol 2004;42:499–504.
Guda NM, Partington S, Vakil N. Inter- and intra-observer variability in the measurement of length at endoscopy: implications for the measurement of Barrett’s esophagus. Gastrointest Endosc 2004;59:655–658.
El-Serag HB, Garewel H, Kuebeler M, Sampliner RE. Is the length of newly diagnosed Barrett’s esophagus decreasing? The experience of a VA Health Care System. Clin Gastroenterol Hepatol 2004;2:296–300.
Amano Y, Kinoshita Y. Barrett’s esophagus: perspectives on its diagnosis and management in Asian populations. Gastroenterol Hepatol 2008;4:45–53.
Amano Y, Ishimura N, Furuta K, Takahashi Y, Chinuki D, Mishima Y, et al. Which landmark results in a more consistent diagnosis of Barrett’s esophagus, the gastric folds or the palisade vessels? Gastrointest Endosc 2006;64:206–211.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Okita, K., Amano, Y., Takahashi, Y. et al. Barrett’s esophagus in Japanese patients: its prevalence, form, and elongation. J Gastroenterol 43, 928–934 (2008). https://doi.org/10.1007/s00535-008-2261-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-008-2261-y