
Abstract
The role of aspirin on the risk of cancers of the upper aerodigestive tract was investigated in the combined data of three Italian case–control studies, including 965 cases and 1779 hospital controls. The odds ratio was 0.33 for users of ⩾5 years, and 0.51 for ⩾5 years since first use.
Similar content being viewed by others

Main
Data on the role of aspirin on the risk of cancers of the upper aerodigestive tract are scanty, and mainly related to cancer of the oesophagus. In two rheumatoid arthritis cohorts from Finland (Isomäki et al, 1978) and Sweden (Gridley et al, 1993), no significant association between aspirin use and oesophageal cancer risk was observed (relative risk (RR)=0.94 and 1.3, respectively). In a large prospective study from the American Cancer Society, a significantly reduced risk of oesophageal cancer (RR=0.59) was reported in subjects who used aspirin ⩾16 times per month for at least 1 year, and the risk reduction was stronger among users for ⩾10 years (RR=0.54) (Thun et al, 1993). In the same study, a nonsignificant increased risk was observed for oral and pharyngeal cancer. In the cohort of the National Health and Nutrition Examination Survey, aspirin use was associated with a 90% decreased risk of developing oesophageal cancer, although the estimate was based on 15 cases only (Funkhouser and Sharp, 1995). A US population-based case–control study, including 221 squamous-cell oesophageal cancer and 293 adenocarcinoma cases, found a significant lower risk for current aspirin users (odds ratio (OR)=0.49 for squamous-cell and 0.37 for adenocarcinoma) (Farrow et al, 1998). In a British case–control study conducted on 159 women with squamous-cell oesophageal cancer, 10 cases vs 19 controls reported taking aspirin daily for at least 1 month (crude OR ⩾0.50) (Sharp et al, 2001). In a case–control study from Greece with 43 squamous-cell cancers and 56 adenocarcinomas of the oesophagus, the OR was nonsignificantly reduced for ever aspirin use (Garidou et al, 1996).
The potential role of aspirin use on cancers of the upper aerodigestive tract was further investigated using data from three case–control studies conducted in Italy.
Patients and methods
Three hospital-based case–control studies of cancer on the upper aerodigestive tract were conducted in Italy between 1992 and 2000 to examine alcohol, tobacco, diet, family history and other environmental factors, covering a total of 1362 cases and 3038 hospital controls (Franceschi et al, 1999; Bosetti et al, 2000; Talamini et al, 2002).
Controls were from the same hospitals as cases, admitted for a wide spectrum of acute, non-neoplastic conditions, not related to smoking, alcohol consumption or long-term modifications of diet; they were frequency-matched with cases by 5-year age groups, sex and study centre. To compensate for the rarity of laryngeal cancer in women, a control-to-case ratio of about 5 was chosen for women, as opposed to 2 for men. On average, 5% of cases and controls approached during their hospital stay refused to be interviewed (Franceschi et al, 1999; Bosetti et al, 2000; Talamini et al, 2002).
The interview-administered questionnaire included information on sociodemographic characteristics, anthropometric measures, lifestyle habits, including tobacco smoking and alcohol drinking, a validated food frequency section and personal and family medical history. The information on aspirin intake included indication, age at first use, frequency and duration of use. Regular use was defined as use for at least once a week for more than 6 months. To facilitate recall of use, a comprehensive list of major aspirin-containing preparations in Italy was supplied.
A total of 965 cases (850 men, 115 women) of the upper aerodigestive tract cancer (393 oral and pharyngeal, 225 oesophageal and 347 laryngeal cancer) and 1779 (1450 men, 329 women) controls with information on aspirin use were included in the present analysis.
ORs and the corresponding 95% confidence intervals (CI) were estimated using unconditional multiple logistic regression models (Breslow and Day, 1980), including terms for age, sex, study centre, years of education (<7, 7–11, ⩾12), alcohol (<14, 14–27, 28–55, ⩾56 drinks per week, plus a dummy variable for ex-drinkers) and tobacco consumption (never, ex-smoker, current smoker of <15, 15–24, ⩾25 cigarettes per day).
Results
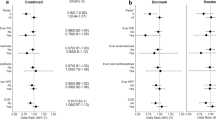
Table 1 gives the distribution of 965 upper aerodigestive cancer cases and 1779 controls according to selected measures of aspirin use. A total of 37 (3.8%) cases vs 87 (4.9%) controls reported regular aspirin use. Average frequency of use was 5.7 times per week among cases and 5.6 among controls; 32 cases and 78 controls took aspirin ⩾3 times per week, 27 cases and 57 controls every day. Indication of use was analgesia for 10 cases and 38 controls, whereas 27 cases and 49 controls took aspirin for cardiovascular prevention. The multivariate OR for regular use was 0.89 (95% CI 0.56–1.43). The OR decreased to 0.33 (95% CI 0.13–0.82) for users of ⩾5 years, and was 0.51 (95% CI 0.26–0.99) for ⩾5 years since first use.
A reduced risk with longer duration of aspirin use was observed for all sites considered: the ORs for ⩾5 years of use were 0.39 for oral and pharyngeal, 0.80 oesophageal and 0.09 laryngeal cancer. Similarly, the ORs for ⩾5 years since first use were 0.26, 0.66 and 0.55 for the three cancer sites, respectively.
Discussion
This study suggests that aspirin may have a beneficial effect on cancers of the upper aerodigestive tract. Although there is evidence of a possible protective effect of aspirin on oesophageal cancer (Bosetti et al, 2002), only scattered epidemiological data exist on its role on cancer of the oral cavity or larynx (Thun et al, 1993).
A significant reduced risk has been observed particularly for long-term use and in relation to a longer time since first use. These time–risk relations are similar to those described for colorectal cancer (Giovannucci et al, 1995, IARC, 1997; Thun et al, 2002), and therefore give plausibility to a causal association.
With reference to possible biological mechanisms, aspirin, as well as other nonsteroidal anti-inflammatory drugs (NSAID), acts on the arachidonic acid metabolism, blocking the synthesis of thromboxane, prostacyclin and prostaglandins, which in turn can influence cell proliferation, and hence cancer growth (Marnett, 1992; Marcus, 1995). A specific target of the protection against colorectal and other cancers by aspirin and other NSAID is the inhibition of cyclooxygenase-2, which is important for apoptosis, and therefore for control of the mechanisms of carcinogenesis (Featherstone, 1997; Hong and Sporn, 1997; Taketo, 1998a,1998b; Smith et al, 2000). The same mechanisms may be responsible for the favourable action of aspirin on oesophageal cancer and other cancers of the upper aerodigestive tract (Morgan and Vainio, 1998; Chan et al, 1999; Zimmermann et al, 1999; Li et al, 2000).
Limitations of our study should be considered that might have introduced a spurious association between aspirin use and the reduced risk of upper aerodigestive tract cancers. It is possible in fact that aspirin use has been affected by early symptoms of the conditions under study. The evidence of an association with longer use is, however, reassuring against this bias. Further, some of the diagnostic categories of the controls may be associated with increased aspirin use. However, the results were similar when cases were compared with each of the major diagnostic categories of controls, thus giving reassurance against potential selection biases. Another limitation of this study is that, although based on a large number of cases, it includes a relatively low number of regular aspirin users, reflecting the pattern of regular aspirin use in Italy. Among the strengths of the study are the similar catchment areas for cases and controls, the almost complete participation rate and the choice of hospitals controls, who are preferable to population ones with reference to reliability and validity of information on drug use, since cases and controls are similarly sensitised towards various aspects of their medical history (Kelly et al, 1990). Moreover, the risk estimates were adjusted for major risk factors for cancers of the upper aerodigestive cancer, that is, tobacco smoking and alcohol drinking, suggesting therefore that the inverse relation between long-term aspirin use and cancers of the upper aerodigestive tract is real.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Bosetti C, Gallus S, La Vecchia C (2002) Aspirin and cancer risk: an update to 2001. Eur J Cancer Prev 11: 535–542
Bosetti C, La Vecchia C, Talamini R, Simonato L, Zambon P, Negri E, Trichopoulos D, Lagiou P, Bardini R, Franceschi S (2000) Food groups and risk of squamous cell esophageal cancer in Northern Italy. Int J Cancer 87: 289–294
Breslow NE, Day NE (1980) Statistical Methods in Cancer Research. Vol. I, The Analysis of Case–Control Studies. IARC Sci Publs no. 32. Lyon: International Agency for Research on Cancer
Chan G, Boyle JO, Yang EK, Zhang F, Sacks PG, Shah JP, Edelstein D, Soslow RA, Koki AT, Woerner BM, Masferrer JL, Dannenberg AJ (1999) Cyclooxygenase-2 expression is up-regulated in squamous cell carcinoma of the head and neck. Cancer Res 59: 991–994
Farrow DC, Vaughan TL, Hansten PD, Stanford JL, Risch HA, Gammon MD, Chow W-H, Dubrow R, Ahsan H, Mayne ST, Schoenberg JB, West AB, Rotterdam H, Fraumeni Jr JF, Blot WJ (1998) Use of aspirin and other nonsteroidal anti-inflammatory drugs and risk of oesophageal and gastric cancer. Cancer Epidemiol Biomarkers Prev 7: 97–102
Featherstone C (1997) Aspirin for bowel cancer: an old friend finds a new role. Lancet 350: 418
Franceschi S, Levi F, Conti E, Talamini R, Negri E, Dal Maso L, Boyle P, Decarli A, La Vecchia C (1999) Energy intake and dietary pattern in cancer of the oral cavity and pharynx. Cancer Causes Control 10: 439–444
Funkhouser EM, Sharp GB (1995) Aspirin and reduced risk of oesophageal carcinoma. Cancer 76: 1116–1119
Garidou A, Tzonou A, Lipworth L, Signorello LB, Kalapothaki V, Trichopoulos D (1996) Life-style factors and medical conditions in relation to esophageal cancer by histologic type in a low-risk population. Int J Cancer 68: 295–299
Giovannucci E, Egan KM, Hunter DJ, Stampfer MJ, Colditz GA, Willett WC, Speizer FE (1995) Aspirin and the risk of colorectal cancer in women. N Engl J Med 333: 609–614
Gridley G, McLaughlin JK, Ekbom A, Klareskog L, Adami H-O, Hacker DG, Hoover R, Fraumeni Jr JF (1993) Incidence of cancer among patients with rheumatoid arthritis. J Natl Cancer Inst 85: 307–311
Hong WK, Sporn MB (1997) Recent advances in chemoprevention of cancer. Science 278: 1073–1077
IARC Handbooks of Cancer Prevention (1997) Non-Steroidal Anti-Inflammatory Drugs, Vol. 1. Lyon: International Agency for Research on Cancer
Isomäki HA, Hakulinen T, Joutsenlahti U (1978) Excess of lymphomas, leukemia, and myeloma in patients with rheumatoid arthritis. J Chron Dis 31: 691–696
Kelly JP, Rosenberg L, Kaufman DW, Shapiro S (1990) Reliability of personal interview data in a hospital-based case–control study. Am J Epidemiol 131: 79–90
Li M, Lotan R, Levin B, Tahara E, Lippman SM, Xu XC (2000) Aspirin induction of apoptosis in oesophageal cancer: a potential for chemoprevention. Cancer Epidemiol Biomarkers Prev 9: 545–549
Marcus AJ (1995) Aspirin as prophylaxis against colorectal cancer. N Engl J Med 333: 656–658
Marnett LJ (1992) Aspirin and the potential role of prostaglandins in colon cancer. Cancer Res 52: 5575–5589
Morgan G, Vainio H (1998) Barrett's oesophagus, oesophageal cancer and colon cancer: an explanation of the association and cancer chemopreventive potential of non-steroidal anti-inflammatory drugs. Eur J Cancer Prev 7: 195–199
Sharp L, Chilvers CED, Cheng KK, McKinney PA, Logan RFA, Cook-Mozaffari P, Ahmed A, Day NE (2001) Risk factors for squamous cell carcinoma of the oesophagus in women: a case–control study. Br J Cancer 85: 1667–1670
Smith ML, Hawcroft G, Hull MA (2000) The effect of non-steroidal anti-inflammatory drugs on human colorectal cancer cells: evidence of different mechanisms of action. Eur J Cancer 36: 664–674
Taketo MM (1998a) Cyclooxygenase-2 inhibitors in tumorigenesis (Part I). J Natl Cancer Inst 90: 1529–1536
Taketo MM (1998b) Cyclooxygenase-2 inhibitors in tumorigenesis (Part II). J Natl Cancer Inst 90: 1609–1620
Talamini R, Bosetti C, La Vecchia C, Dal Maso L, Levi F, Bidoli E, Negri E, Pasche C, Vaccarella S, Barzan L, Franceschi S (2002) Combined effect of tobacco and alcohol on laryngeal cancer risk: a case–control study. Cancer Causes Control 13: 951–964
Thun MJ, Henley SJ, Patrono C (2002) Nonsteroidal anti-inflammatory drugs as anticancer agents: mechanistic, pharmacologic, and clinical issues. J Natl Cancer Inst 94: 252–266
Thun MJ, Namboodiri MM, Calle EE, Flanders WD, Heath Jr CW (1993) Aspirin use and risk of fatal cancer. Cancer Res 53: 1322–1327
Zimmermann KC, Sarbia M, Weber AA, Borchard F, Gabbert HE, Schror K (1999) Cyclooxygenase-2 expression in human esophageal carcinoma. Cancer Res 159: 198–204
Acknowledgements
This work was conducted with the contribution of the Italian Association for Cancer Research, and the Italian League Against Cancer. We thank Mrs MP Bonifacino for her editorial assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Bosetti, C., Talamini, R., Franceschi, S. et al. Aspirin use and cancers of the upper aerodigestive tract. Br J Cancer 88, 672–674 (2003). https://doi.org/10.1038/sj.bjc.6600820
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6600820
Keywords
This article is cited by
-
Associations between aspirin use and the risk of cancers: a meta-analysis of observational studies
BMC Cancer (2018)
-
Aspirin and non-steroidal anti-inflammatory drug use and the risk of upper aerodigestive tract cancer
British Journal of Cancer (2014)
-
Non-steroidal anti-inflammatory drug and aspirin use and the risk of head and neck cancer
British Journal of Cancer (2013)
-
Non-steroidal anti-inflammatory drug and aspirin use and the risk of head and neck cancer: a systematic review
Cancer Causes & Control (2011)
-
Non-steroidal anti-inflammatory drugs and risk of gastric and oesophageal adenocarcinomas: results from a cohort study and a meta-analysis
British Journal of Cancer (2009)
