Article Text

Abstract
Background: Measurement of faecal elastase (FE1) is used widely to screen for pancreatic exocrine insufficiency (PI). FE1 does not allow differentiation of primary from secondary PI.
Aims: To investigate the relation between duodenal morphology and FE1 in children with secondary PI resulting from primary gastrointestinal diseases.
Methods: A group of 51 children underwent small intestinal biopsy and FE1 measurement. Villus to crypt ratio (VCR) and inflammation within the lamina propria of duodenal mucosal biopsy specimens were scored and compared with FE1 values.
Results: In 51 children from nine diagnostic categories, a highly significant correlation between FE1 and both duodenal morphology and inflammation was found.
Conclusion: Small bowel enteropathy is associated with low FE1 concentrations, indicative of secondary exocrine pancreatic insufficiency.
- faecal elastase
- duodenum
- enteropathy
- inflammation
- CCK, cholecystokinin
- FE1, faecal elastase
- GI, gastrointestinal
- PI, pancreatic exocrine insufficiency
- PZ, pancreozymin
- PVA, partial villous atrophy
- VCR, villus to crypt ratio
Statistics from Altmetric.com
- CCK, cholecystokinin
- FE1, faecal elastase
- GI, gastrointestinal
- PI, pancreatic exocrine insufficiency
- PZ, pancreozymin
- PVA, partial villous atrophy
- VCR, villus to crypt ratio
Measurement of faecal elastase 1 (FE1) concentration is a simple, non-invasive, and widely available test, which allows clinicians to estimate pancreatic exocrine function. It has been shown to be a useful screening test for severe primary pancreatic insufficiency, in conditions such as cystic fibrosis or Shwachman's syndrome.1–5 Reduced FE1 concentrations are found in some individuals with coeliac disease.6–8 A variety of enteropathic processes other then coeliac disease are associated with reduced excretion of faecal elastase. We have therefore studied the relation between duodenal morphology, duodenal inflammation, and FE1.
PATIENTS AND METHODS
Patients
Retrospective analysis was undertaken of all children between March 1997 and February 2000, who had undergone (1) small intestinal biopsy and (2) FE1 measurement within a month of each other at Great Ormond Street Hospital.
Faecal elastase 1
FE1 concentrations were measured using an enzyme linked immunosorbent assay (ELISA) kit, which uses two monoclonal antibodies against two distinct epitopes of human pancreatic FE1 (Schebo Tech, GmbH, Wettenberg, Germany). The assay is linear between 15 and 400 μg elastase per g faecal weight with a lower detection limit of 15 μg/g. Results were expressed as μg/g of stool and nominally scored as indicative of normal pancreatic exocrine function (>200 μg/g), moderate pancreatic exocrine insufficiency (100–200 μg/g), or severe pancreatic exocrine insufficiency (<100 μg/g).1,4 Excessive stool water may be associated with falsely low faecal elastase results and liquid stool samples were therefore discarded.9,10
Secretin–cholecystokinin (CCK) test
In a small number of children, with a faecal elastase less than 200 μg/g, the secretin–CCK test, a direct test of pancreatic exocrine function,11 was performed. For this a tube was placed under fluoroscopy in the third part of the duodenum. Duodenal juice was aspirated over a 15 minute period and collected in plastic tubes on ice. Further samples were collected during consecutive 15 minute periods following injection of intravenous secretin (2 IU/kg), and subsequently intravenous CCK (2 IU/kg), which stimulate pancreatic ductal and acinar secretion respectively. Duodenal juice volume, pH, bicarbonate, lipase, and trypsin concentrations were determined in the laboratory.11
Duodenal histology
Histological sections of duodenal mucosa stained with haematoxylin and eosin (H&E) were examined by light microscopy in a double blind fashion by an experienced paediatric histopathologist and a paediatric gastroenterologist. The morphology was assessed by measuring villus to crypt ratio (VCR) and scored in the following manner: 0 = flat mucosa, 1 = severe partial villous atrophy (PVA) (1:1 VCR), 2 = moderate PVA (1.5:1 VCR), 3 = mild PVA (2–2.5:1 VCR), 4 = normal VCR. Inflammation within the lamina propria of the biopsy specimens was scored (3 = no inflammation present, 2 = mild infiltrate of plasma cells, 1 = notable infiltrate).
Statistical analysis
Statistical analysis was performed using t test and regression analysis.
RESULTS
A total of 51 patients (24 boys, 27 girls; aged 27 days to 12 years) fulfilled the study entry criteria. FE1 was measured 60 times in 51 patients within a month of duodenal biopsy, nine patients having undergone both investigations a second time during a subsequent investigative episode. The intravenous secretin–CCK stimulation test had been undertaken in six of 51 patients during this same period.
The patients fell into nine diagnostic categories based on clinical and histopathological criteria: autoimmune enteropathy, indeterminate enteropathy, post-infectious enteropathy, tufting enteropathy, food sensitive enteropathy, food allergy without enteropathy, short gut syndrome with enteropathy, idiopathic inflammatory bowel disease (Crohn's disease), and failure to thrive without gastrointestinal (GI) cause. Figure 1 shows stool elastase concentrations for each of the diagnostic groups.

FE1 concentrations in different diagnostic groups. 1 = autoimmune enteropathy; 2 = idiopathic inflammatory bowel disease, 3 = indeterminate enteropathy, 4 = food sensitive enteropathy, 5 = food allergy without enteropathy, 6 = post-infectious enteropathy, 7 = tufting enteropathy, 8 = short gut syndrome, 9 = failure to thrive without GI cause. FE1 concentrations: ≤15–100 = severe exocrine pancreatic insufficiency; 101–200 = moderate; ≥200 = normal. Range ≤15 to ≥400.
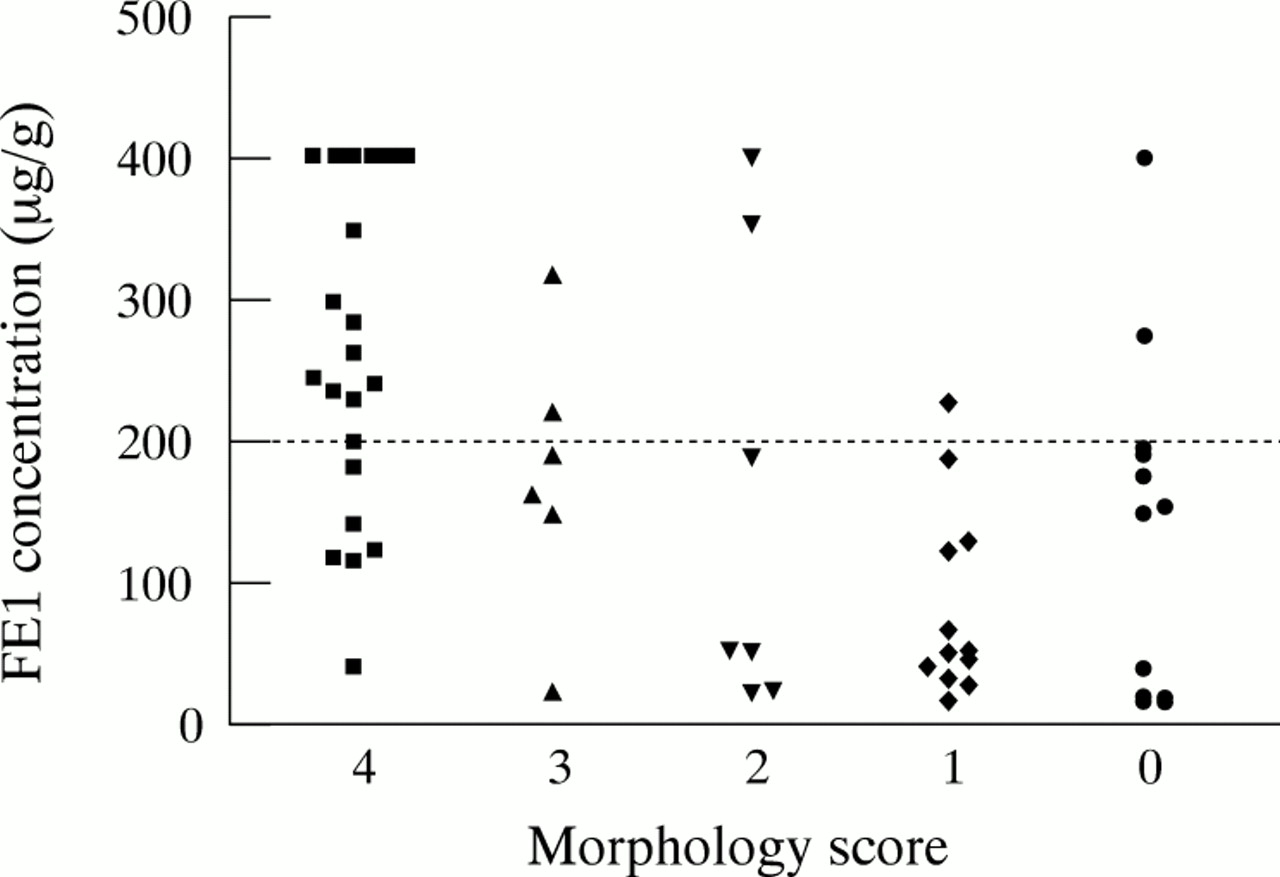
When mucosal morphology was compared with concentrations of FE1, using linear regression analysis, a highly significant correlation was shown between faecal elastase and duodenal morphology (t ratio 4.55; p ≤ 0.0001; fig 2, table 1). Twenty six estimations were compatible with normal exocrine pancreatic function (>200 μg/g), 17 with moderate (100–200 μg/g), and 17 with severe (<100 μg/g) pancreatic insufficiency. Of the 26 normal results, 19 (73.1%) were matched with normal duodenal mucosal biopsy specimens and seven (26.9%) with enteropathies. Of the 17 (28.4%) stool elastase concentrations between 100 and 200 μg/g, six (35.3%) had normal histology and 11 (64.7%) enteropathies. Of the 17 (28.4%) stool elastase concentrations below 100 μg/g, only one (5.9%) had normal mucosa and 16 (94.1%) had enteropathies. In patients with normal small bowel morphometry and low FE1, we found inflammation to be present in 6/7 (85.7%), compared with 4/19 (21.1%) of patients with normal morphology and normal FE1. Table 1 summarises these results according to clinical diagnosis.
Comparison of faecal elastase 1 concentration with duodenal morphology

Comparison of FE1 concentration with duodenal morphology. 4 = normal VCR, 3 = 2–2.5:1 VCR (mild PVA), 2 = 1.5:1 VCR (moderate PVA), 1 = 1:1 VCR (severe PVA), 0 = flat mucosa.
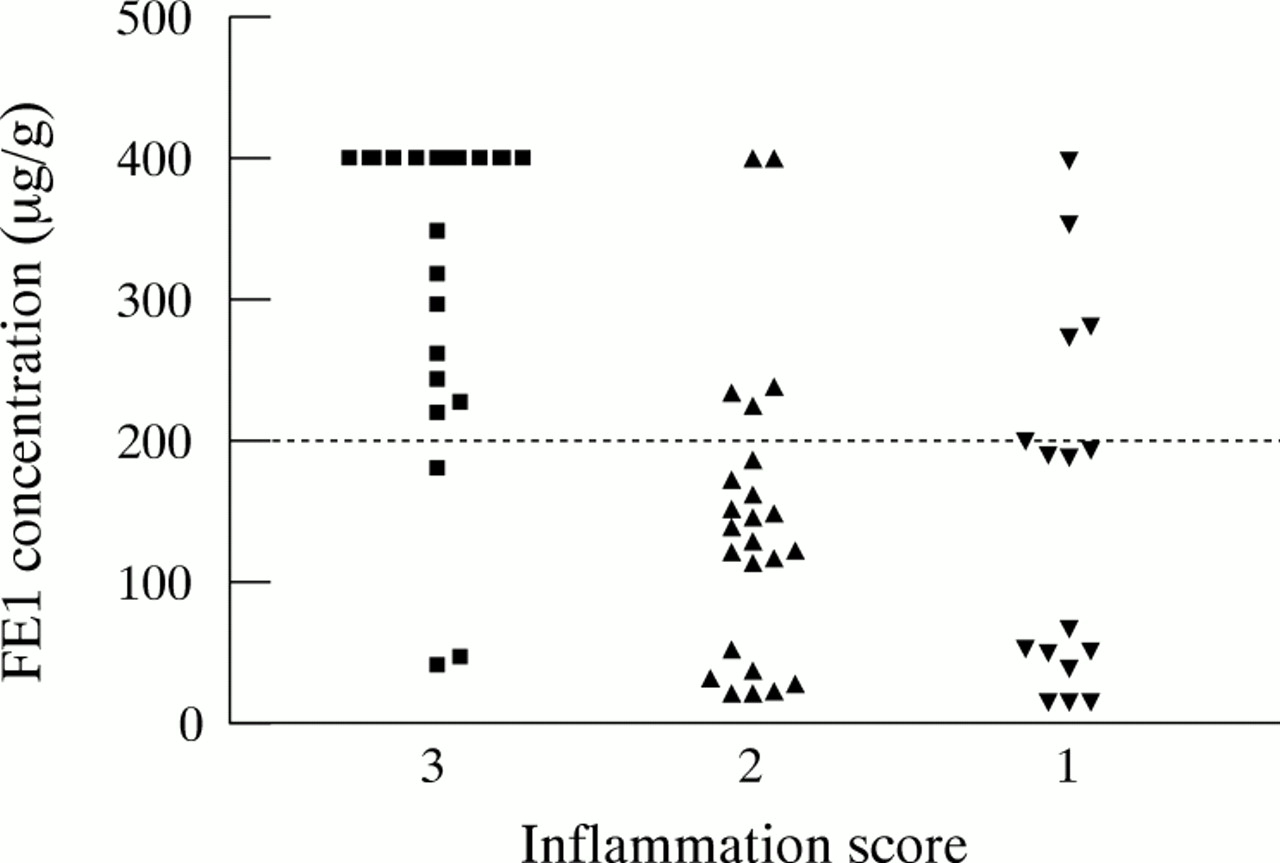
Inflammation was found to correlate with concentrations of FE1 (fig 3, table 2). Linear regression analysis showed the association to be statistically significant with a t ratio of 4.10 (p = 0.0001). Of the 26 normal FE1 results, 17 (65.4%) patients had no inflammation. Of 34 low FE1 results 31 (91.2%) had evidence of mucosal inflammation within the duodenum. Only 3/60 (5%) with low FE1 results had no evidence of small intestinal inflammation within this selected group of patients. Of 17 patients with no inflammation and normal FE1, 16 (94.1%) had normal small intestinal morphometry.
Comparison of faecal elastase 1 concentration with duodenal inflammation

{kind=link}
{kind=link}
{kind=link}
Comparison of FE1 concentration with duodenal inflammation. 3 = normal mucosa, 2 = moderate infiltrate, 1 = severe infiltrate.
Results of direct secretin–CCK stimulated pancreatic secretion revealed post-stimulation trypsin/lipase levels in the normal range for six patients, showing that their pancreas could respond normally to physiological humoral stimuli.
DISCUSSION
The exocrine pancreas secretes digestive enzymes (acinar tissue) and bicarbonate (ductal tissue). The secretory process is driven by neurohumoral events dependent on the presence of food within the duodenal lumen. Nutrient sensing is undertaken both by vagal afferent nerves and by mucosal enteroendocrine cells. Enteroendocrine cells secrete cholecystokinin in response to intraduodenal lipid/proteins, which stimulates pancreatic acinar secretion of zygmogens.
Many methods are available to measure either directly or indirectly pancreatic exocrine function. Direct methods are labour intensive and invasive. They are best undertaken in centres in which there is a regular clinical need for the investigation so that staff and laboratory alike are competent in carrying out the investigation. Indirect methods include measurement of pancreatic digestive activity (PABA test, 13C triglyceride breath test12) or measurement of pancreatic enzymes in the stool (faecal chymotrypsin and elastase). Most suffer shortcomings relating to the complexity of the test and/or poor sensitivity/specificity. In recent years faecal elastase determination has become a popular screening investigation for pancreatic exocrine insufficiency because it is simple, cheap, reliable, and widely available. Elastase 1 is produced by the acinar cell of the pancreas and is not degraded during intestinal transit. Hence stool content of FE1 reflects its secretion by the pancreas. FE1 is enriched about fivefold in faeces compared to duodenal juice as a result of faecal dehydration.13,14 The FE1 assay is not affected by temperature15,16 or pancreatic replacement therapy,1 with low individual inter-day, inter-assay, and intra-assay variations.3,15,17 During the first month of life faecal elastase concentrations increase to a plateau of >400 μg/g,17 rendering the assay well suited to the paediatric age range. The assay is reported to have a high sensitivity and specificity in diagnosing severe primary pancreatic exocrine insufficiency1,4,18 (93–100% sensitivity, 83–100% specificity5,15,17,19,20) when values of <200 μg/g are used to indicate pancreatic insufficiency. Patients with small bowel mucosal damage, in association with coeliac disease, have also been found to have low FE1 concentrations,6–8 which increase to normality21 with the restoration of the mucosa integrity on a gluten free diet.7 Our study in children with reduced stool elastase and normal CCK–PZ tests provides evidence that the secretory capacity of the pancreas is normal in individuals with enteropathy. Thus the most likely mechanism of functional PI is a reduction in pancreatic stimulation with impaired secretion of secretin or CCK by the inflamed intestine.7 There remains a possibility of reduced pancreatic exocrine synthesis as a result of long standing malnutrition or primary pancreatic impairment.8 Low values of FE115 and other pancreatic enzymes12 have been noted in other primary GI mucosal diseases and regarded as either false positive results22–24 or just been discarded.
This study clearly shows that small intestinal enteropathy of various origins is associated with reduced excretion of faecal elastase. The presence of inflammation within the duodenal mucosa has a profound negative effect on the exocrine pancreatic function. The link between mucosal inflammation and impaired pancreatic exocrine function impairment remains poorly understood, although it seems reasonable to propose that the enteroendocrine or neuroendocrine drive of the pancreas by the duodenum is perturbed in some way.
Conclusion
This study supports the notion that small bowel mucosal integrity is necessary for normal control of exocrine pancreatic secretion. It highlights the need for gastrointestinal mucosal biopsy in individuals with reduced FE1 concentrations in whom causes of primary pancreatic insufficiency (principally cystic fibrosis and Shwachman's syndrome) have been excluded.
REFERENCES
Footnotes
-
Research at the Institute of Child Health and Great Ormond Street Hospital for Children NHS Trust benefits from R&D funding received from the NHS Executive.