Article Text

Abstract
The prevalence of osteopenia in children with inflammatory bowel disease (IBD) is unknown. The effect of nutritional state, disease activity, and steroid therapy on bone mineral content (BMC) of whole body, lumbar spine, and left femoral neck measured by dual energyx ray absorptiometry in 32 children with IBD was assessed by comparison with 58 healthy local school children. Using the control data, a predicted BMC was calculated taking into account bone area, age, height, weight, and pubertal stage. The measured BMC in children with IBD was expressed as a percentage of this predicted value (% BMC). Mean (SD) % BMC was significantly reduced for the whole body and left femoral neck in the children with IBD (97.0 (4.5)% and 93.1 (12.0)% respectively, p<0.05). Of the children with IBD, 41% had a % BMC less than 1 SD below the mean for the whole body and 47% at the femoral neck. Reduction in % BMC was associated with steroid usage but not with the magnitude of steroid dose, disease activity, or biochemical markers of bone metabolism. In conclusion, osteopenia is relatively common in childhood IBD and may be partly related to the previous use of steroids.
- osteopenia
- inflammatory bowel disease
- bone mineral content
Statistics from Altmetric.com
Osteopenia is well recognised in adults with inflammatory bowel disease (IBD).1 The pathophysiology is unclear but is probably a combination of a number of inter-related factors. The inflammatory process itself, with the release of cytokines, may have a direct effect on bone mineralisation,2 and episodes of malabsorption and malnutrition along with periods of physical inactivity during acute relapse together may inhibit bone formation.3 IBD often necessitates treatment with relatively high doses of steroids for prolonged periods of time. Steroids are known to affect bone mineralisation by a direct inhibitory action on osteoblast activity, reduction of intestinal absorption of calcium, stimulation of parathyroid hormone release, and by adverse effects on growth hormone action.4 Steroids have also been shown to reduce gonadal hormone production.5 Future fracture risk is closely related to peak bone mass which is achieved soon after the end of puberty.6 Children with IBD have a frequently delayed and truncated pubertal growth spurt which may have adverse effects on the achievement of peak bone mass.7
Bone mineral status can be assessed by means of dual energyx ray absorptiometry (DXA). The case has been reported of a child who, soon after the diagnosis of Crohn’s disease, suffered several vertebral fractures secondary to severe osteopenia demonstrated on DXA scan.8 The incidence and wider prevalence of osteopenia in childhood IBD is not known. In the study reported here, bone mineral content (BMC) of the whole body, lumbar spine, and left femoral neck was measured by DXA in children with IBD and compared with that in a healthy local British control population. The effect of nutritional status, disease activity, and steroid therapy on the BMC of children with IBD was also assessed.
Subjects and methods
SUBJECTS
All children with IBD attending the gastroenterology clinic at the University Hospital of Wales participated in the study. Twenty one (10 boys) had Crohn’s disease and 11 (eight boys) ulcerative colitis. Fifty eight (29 male) healthy schoolchildren from the South Wales area were recruited as control subjects. This control group comprised 31 (17 male) siblings of children participating in another study in the department and 27 (12 male) relatives of staff within our department and volunteers from a local school. The control group was chosen to provide data from normal healthy children over as wide an age range as possible. No attempt was made to match the control children individually with the children with IBD because of the shorter stature in the latter. Informed consent was obtained from the parents and children. The study was approved by the South Glamorgan Health Authority research ethics committee.
METHODS
Auxology
Height was measured on a wall mounted Harpenden stadiometer (Holtain Ltd, Crymych, Dyfed) and weight on an Avery beam balance (Avery Ltd, Birmingham) by two trained observers. Body mass index was calculated from weight (kg)/height2 (m2). The measurements were expressed as SD scores using the 1990 growth standards for British children.9 10 Puberty was assessed by the method of Tanner. 11
Body composition
Body composition, as a marker of nutritional state, was assessed by skinfold thickness and DXA. Skinfold thickness was measured at the biceps, triceps, subscapular, and suprailiac sites and fat-free mass and percentage fat (% fat) calculated using the equations of Brook for prepubertal children,12 Durnin and Rahaman for children in puberty,13 and the equation of Siri.14
DXA measurements of fat-free mass and % fat were performed on a QDR 1000/W scanner (Hologic Inc, Waltham, MA, USA).15
Bone mineralisation
DXA measurements of BMC and bone area (BA) were taken for the whole skeleton, lumbar spine (L1–L4) and left femoral neck using the Hologic QDR 1000/W bone densitometer. Conventionally, bone mineralisation data have been expressed as an areal bone mineral density (BMD)—that is, BMC/BA; however, this fails to correct BMC for BA as both remain correlated with BMD. Furthermore BMD fails to remove the correlation of BMC with age, body size,16 and pubertal stage. Therefore predictive equations were produced for BMC based on the control population, using multiple regression analysis, with BMC as the dependent variable and BA, age, height, weight, pubertal stage, and gender as the independent variables. Independent variables were selected using a backward stepwise procedure such that all remaining variables in the final predictive formula for BMC were statistically significant (p<0.05). All continuous variables were converted to natural logarithms so as to linearise their relationship with BMC. The measured BMC was expressed as a percentage of the predicted value (% BMC), which allows comparison of values in subjects with a wide range of body size and age with the control population.
Biochemical measures of bone metabolism
Serum concentrations of calcium, phosphate, 25-hydroxycholecalciferol, and parathyroid hormone were measured as indices of calcium homoeostasis. The serum concentration of alkaline phosphatase was measured as a marker of bone formation, and fasting spot urine hydroxyproline/creatinine ratio was measured as a marker of bone resorption.
Disease activity
Disease activity was measured at the time of participation in the study and by retrospective case note analysis from clinic visits over the preceding year. Disease activity for Crohn’s disease was measured by a modified Harvey Bradshaw index.17 This index is based on five clinical variables (general well being, presence and severity of abdominal pain, number of liquid stools per day, presence of an abdominal mass, and the presence of complications), which produce a composite score between 0 and 20. Disease activity in ulcerative colitis was measured by the criteria of Truelove and Witts,18 which classifies activity in terms of clinical severity (mild, moderate, and severe). To allow for statistical comparisons with the group of children with Crohn’s disease, a numerical score was then applied to the severity classifications (mild, 2; moderate, 6; severe, 10).
Steroid usage
The duration and dosage of steroid treatment was recorded. The magnitude of steroid treatment was calculated using a modification of the method described by Motil et al.19 This is based on a composite score of daily dosage in mg/kg, duration of treatment, and mode (whether given continuously or intermittently) (table 1).
Calculation of steroid score
STATISTICAL ANALYSIS
Group means were compared using independent t tests, allowing mean differences and 95% confidence intervals to be calculated. The different steroid groups were compared using one way analysis of variance (ANOVA). Where the F ratio was significant (p<0.05) Tukey’s post hoc multiple comparison test was applied to compare individual groups with each other. The distribution of % BMC was tested for normality using the Kolmogorov-Smirnov test.
Results
AUXOLOGY AND BODY COMPOSITION
Although the control group was slightly younger, there was no significant difference between the ages of the patients and the controls (table 2). The children with IBD were significantly shorter and lighter than the controls (p<0.005), although there were no significant differences between patients and controls in any of the measures of body composition. However, as might be expected, girls had a higher % body fat than boys in both groups (p<0.001). The two groups were at similar stages of puberty (median stage 3).
Auxology and body composition measurements; values are mean (SD)
BONE MINERAL CONTENT
The mean % BMC for each site for the controls is close to 100%, which is to be expected since the predicted BMC is derived from the control population (table 3). % BMC was normally distributed at each site (Kolmogorov-Smirnov test, p>0.20), and the SD at each site then allowed definition of a normal reference range for interpretation of % BMC in the children with IBD (fig 1). % BMC was reduced for the whole body and the femoral neck in the patient group as a whole when compared with the controls (p<0.05) (table 3 and fig 1). When analysed separately the children with Crohn’s disease had significantly lower % BMC for the whole body and the femoral neck whereas those with ulcerative colitis did not have significantly reduced % BMC at any site. Of the children with IBD, 41% had a % BMC less than 1 SD below the mean for the whole body, 34% at the lumbar spine and 47% at the femoral neck.
Mean (SD) % BMC measurements

Distribution of % BMC of the whole body with age. Mean ± 2 SD based on control data.
RELATION TO BONE BIOCHEMISTRY
All biochemical investigations were within normal limits (table 4) and did not suggest the presence of abnormalities of calcium homoeostasis, bone formation, or bone resorption. There was no correlation between the biochemical markers of bone metabolism and % BMC at any site.
Biochemical measurements; values are mean (SD)
RELATION TO DISEASE ACTIVITY
The mean duration of IBD at the time of the study was 2.9 (range 0.3–10.3) years. The mean (SD) disease score at the time of participation in the study was 3.6 (1.8) and over the preceding year 5.1 (2.5). Other indicators of disease activity including erythrocyte sedimentation rate, platelet count, and haemoglobin concentration were within normal limits. There was no correlation between % BMC and disease activity at the time of the study or over the preceding year in patients with Crohn’s disease or ulcerative colitis whether analysed separately or together.
RELATION TO STEROID USAGE
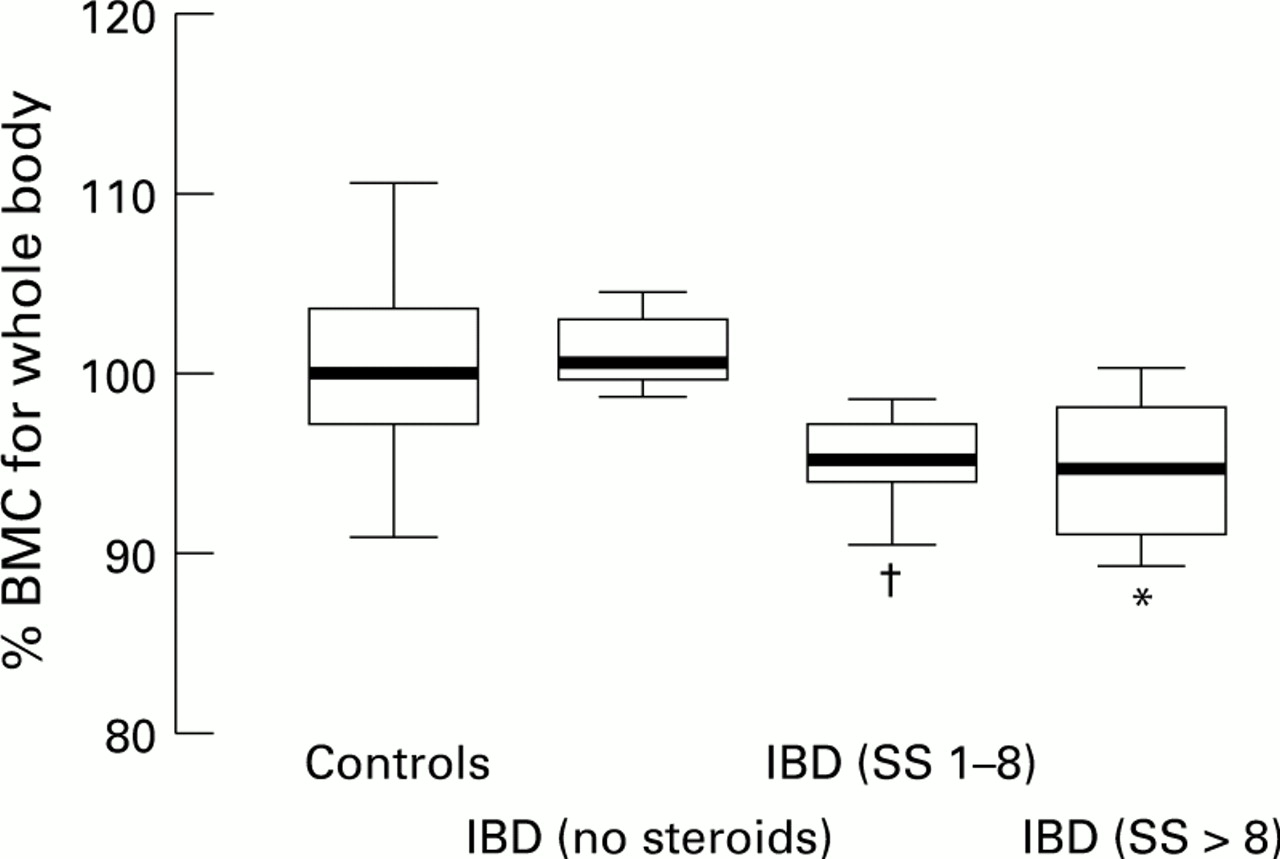
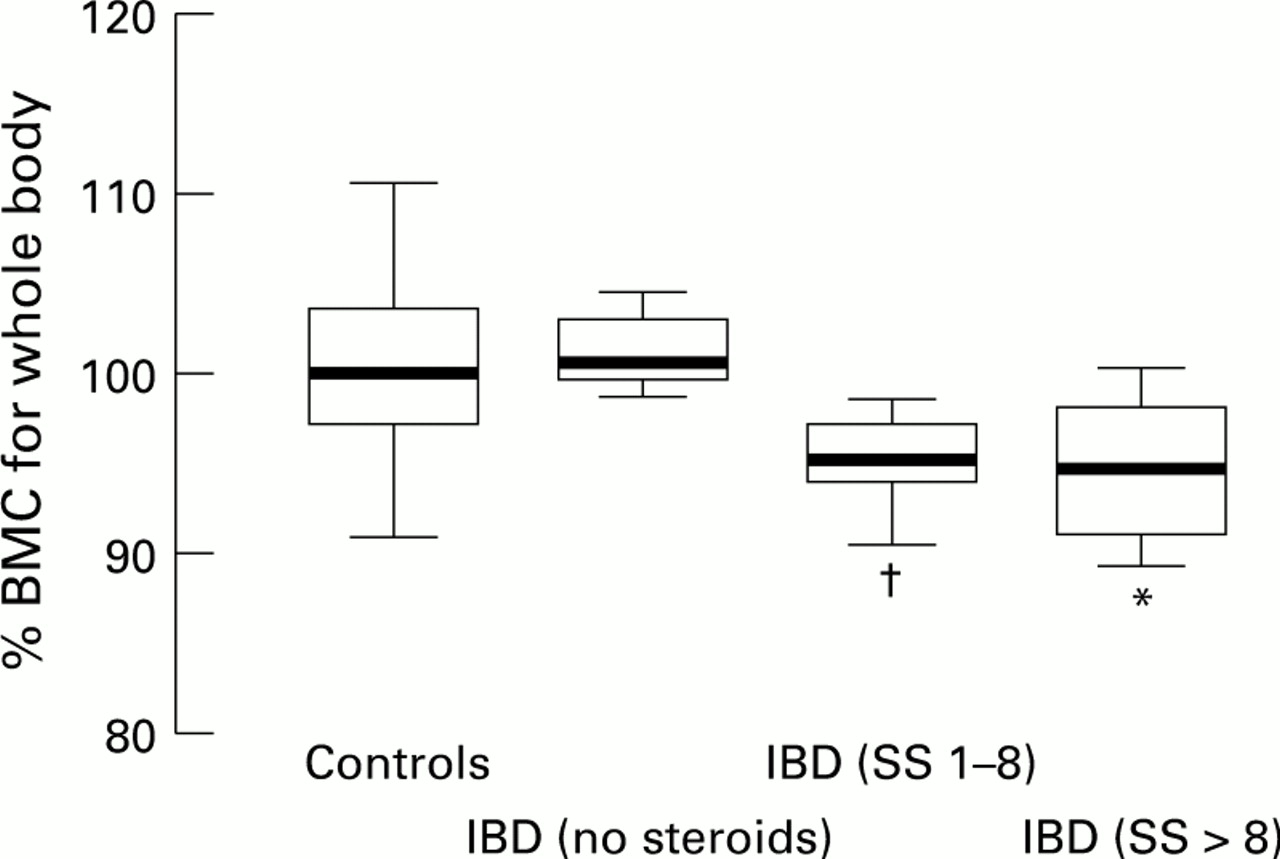
Six children with IBD had never been treated with steroids. Of those children who received steroid therapy, the mean (SD) duration of treatment was 1.2 (1.5) years. The mean (SD) steroid score was 6.3 (5.9). The mean (SD) percentage of time since diagnosis spent on steroids was 40.4 (38.3). Twenty children had discontinued steroid treatment before participating in the study and in these the mean (SD) time between discontinuation and participation was 1.3 (1.4) years. There was no correlation between the magnitude of steroid usage and % BMC nor between percentage time on or time since discontinuing steroids and % BMC. There was, however, a significant reduction in % BMC when the children who had received steroids were compared with those who had not and with the control group (ANOVA p<0.005) (fig2).
{kind=link}
{kind=link}
Effect of steroids on % BMC. SS = steroid score. *p<0.05 compared with controls and IBD (no steroids); †p<0.05 compared with controls (ANOVA and Tukey’s post hoc multiple comparison test).
Discussion
To our knowledge, this is the first published study of BMC in childhood IBD. The results indicate that children with IBD have reduced BMC when compared with healthy local control children, even after correction for their short stature and reduced body weight. This reduction in BMC was noted for the whole body and the femoral neck. We have assumed that a reduction of 1 SD from the mean might be expected to be a clinically important change, as this has been shown to increase fracture risk in adults.20 We calculated the power of our study to detect this magnitude of change as 99% for the children with IBD as a whole, 97% for those with Crohn’s disease, and 85% for those with ulcerative colitis. The reduction in % BMC was only statistically significant for the subjects with Crohn’s disease and not for those with ulcerative colitis. The mean reduction (95% confidence intervals) in % BMC for the whole body between the children with Crohn’s disease and the controls was 4.0 (1.6 to 6.3) and those with ulcerative colitis and the controls was 1.1 (−1.9 to 4.1). By comparison with an SD of 4.6 in the control population, this would indicate that some of the children with Crohn’s disease are likely to have a clinically important reduction in % BMC, whereas those with ulcerative colitis almost certainly do not, despite the small numbers in the study. At the lumbar spine the mean difference between the children with IBD and the controls was 3.8 (−0.9 to 8.4), indicating that no clinically important difference was detected, as well as there being no statistically significant difference.
The cause of the reduced BMC remains unclear. Studies in adults with IBD have produced conflicting results. In some, an association has been found between osteopenia and steroid usage.21 22 Other studies have suggested that reduced BMC is secondary to reduced bone formation23 24 or increased rates of bone loss.25 Low bone mineral density has been noted at diagnosis in Crohn’s disease,26 and growth failure in children with established IBD has been associated with increased disease activity18 19 and nutritional deficiencies.27
This study did not find an association between % BMC and disease activity. Disease activity is difficult to measure accurately, particularly retrospectively, and our assessment may not have been sensitive enough to detect an association. Also, the relatively small numbers in this study may not have been sufficient to reveal an association. In common with others,28 29 this study demonstrates that the reduction in BMC did not appear to be due to malabsorption of calcium or to metabolic bone disease. However, it is possible that important but transient differences in osteoblast or osteoclast activity may occur during the acute inflammatory process, which may lead to longer term effects on BMC but which were not detected by biochemical measurements undertaken in patients who in this study were mostly in remission from acute inflammatory episodes. The results of this study do not suggest a nutritional basis for the osteopenia, as all measures of body composition were normal.
The role of steroids in the reduction in BMC is unclear. Although children with IBD who received steroid treatment had a lower % BMC than those who did not and the control group, the difference in % BMC was not related to the magnitude of steroid use. Steroids are known to have a direct inhibitory effect on osteoblast activity and to have adverse effects on growth hormone action.4 It may be that the steroid effect is an all or none effect and therefore not related directly to dosage. Treatment with steroids may also act as a marker for other variables, such as worsening disease activity, which, in combination with steroid treatment, leads to a reduction in bone mineralisation. Studies of other chronic diseases in childhood have produced differing results. Reduced bone mineralisation has been documented in juvenile chronic arthritis and appears to be associated with disease activity rather than steroid usage,30whereas, after renal transplantation in chronic renal failure, steroid treatment has been implicated.31 Long term inhaled steroids in childhood asthma have not been shown to adversely affect bone mineral density,32 33 in contrast with studies in adults.34
The finding of osteopenia in children with IBD is important as it may predispose to osteopenia and osteoporosis in later adult life because of a failure to achieve adequate peak bone mass, which is one of the major determinants of future risk of fracture. A reduction in BMC of 1 SD below the mean has been shown in adults to increase future fracture risk by 50–100%.20 Assuming that similar relationships are relevant to the bones of growing children, this finding suggests that a number of children with IBD may be at substantial risk of fractures in later adult life.
We suggest that BMC should be monitored in all children with IBD and that if a significantly reduced BMC is observed, the use of steroids should be avoided if possible.
In conclusion, this study demonstrates that osteopenia occurs relatively frequently in children with IBD particularly those who have received steroids. This may be due to a number of interrelated factors and the underlying mechanism requires further evaluation.
Acknowledgments
We are grateful to Mr D Coleman, Mr J H Pearce, and Mrs RJ Pettit for assistance with the DXA measurements. J T W is supported by the local oncology charity, Llandough Aims to Treat Children with Cancer and Leukaemia with Hope (LATCH).