Article Text

Abstract
The purpose of this study was to determine whetherHelicobacter pylori infection can contribute to growth deficit, especially in pubescent children who need large amounts of iron for growth. A structured questionnaire was sent to the parents of 532 healthy children aged 10 to 15 years (mean 12.9) to obtain demographic information on the parents and the environment. Of the 532 questionnaires sent out, 375 (70.5%; 170 girls and 205 boys) were returned. After collecting blood samples from participants, haemoglobin, serum iron, total iron binding capacity, serum ferritin, and serum IgG antibodies to H pylori were measured. The effects of risk factors such as H pylori infection, iron deficiency anaemia, sex, socioeconomic status, type of house, and crowding index on growth were analysed using multiple regression analysis. Of 63 H pyloripositive children, 18 (28.6%) were below the 25th centile values for height, compared with 63 of 312 (20.2%) H pylori negative children. The prevalence rate ofH pylori infection was 15.5% (53 of 343) in children without iron deficiency anaemia and 31.3% (10 of 32) in those affected. The relative risk of short stature was 2.2 (95% confidence interval (CI), 1.0 to 4.8) for iron deficiency anaemia, and 1.4 (95% CI, 0.8 to 2.4) for H pylori infection. The mean height was significantly lower in the group having bothH pylori infection and iron deficiency anaemia. Therefore, H pylori infection accompanied by iron deficiency anaemia, rather thanH pylori infection per se, might delay pubertal growth.
- Helicobacter pylori
- iron deficiency anaemia
- growth deficit
- adolescents
Statistics from Altmetric.com
Helicobacter pylori is known to be an aetiological agent of chronic gastritis and peptic ulcer disease. It is acquired early in life in the developing countries and most of the population is infected by the age of 10 years.1 Once acquired, the infection lasts several decades in most cases, with a very low rate of spontaneous eradication.2 There have been some interesting reports published, which have highlighted rather unusual manifestations of H pylori infection in children—protein losing enteropathy,3 diarrhoea and malnutrition,4 and iron deficiency anaemia.5
Several studies have investigated the effects of H pylori infection on children's growth. A French study showed that H pylori was found in over half of the children being examined because of their short stature.6Another European study revealed that H pylori infection was associated with the subnormal growth of older girls only, at around the time of puberty.7 A recent study in Italy found that a reduction in height seen in older children aged 8.5 to 14 years was related to H pyloriinfection.8 In this study, they suggest thatH pylori might be one of the environmental factors capable of affecting growth. The mechanism of this association has not been elucidated.
Recently, we conducted a double blinded, placebo controlled trial in older children with iron deficiency anaemia and a coexistingH pylori infection.9 We found that H pylori infection can contribute to iron deficiency anaemia, and that infection should be suspected when the iron deficiency anaemia is refractory to iron administration. We also proposed that treatment for iron deficiency anaemia coexistent with H pylori infection should includeH pylori eradication. Iron requirements in adolescents are high, and much iron is needed to supply the high requirements for growth.10 Iron deficiency during this crucial period results in a reduction of longitudinal growth and weight gain.11 12
The purpose of our study was to determine whether H pylori infection can contribute to growth deficit, especially around the time of puberty, when children need large amounts of iron for growth.
Methods
SUBJECTS
We recruited 532 healthy children (285 boys and 247 girls) aged 10 to 15 years from the Pucheon anaemia study, which was launched in October 1996. The aim of the study was to investigate the prevalence of anaemia and the iron status of school children in Pucheon, a city near Seoul, Korea. The criteria for enrollment included: no history of severe diseases, no recent use of drugs such as antibiotics or antacids, and no use of remedies containing iron. Parents of subjects were informed about the study by letter. Of the 532 questionnaires sent out, 375 (70.5%; 205 boys and 170 girls) were returned.
QUESTIONNAIRE
A structured questionnaire was sent to the children's parents, with the help of school teachers, to obtain parental information on: occupation; educational level; and environmental information, such as the type of house, number of rooms in the house, and number of persons living in the house. Informed consent was obtained from every parent before children were enrolled in our study.
LABORATORY ASSAYS
Blood samples of participants were obtained by venepuncture. After collecting the blood samples, various haematological studies were performed, which included the measurement of haemoglobin, serum iron, total iron binding capacity, and serum ferritin. Serum IgG antibodies to H pylori were also measured. The haemoglobin concentration was measured using a Coulter S-PLUS IV (Coulter Electronics, Miami, Florida, USA). Serum was separated and stored at −20°C for analysis of iron deficiency. Serum iron and total iron binding capacity were determined spectrophotometrically (Hitachi, Tokyo, Japan). Transferrin saturation was calculated by dividing the concentration of serum iron by the total iron binding capacity. The serum ferritin assay was performed using a radioimmunoassay kit (Ferritin-Iron II; Ramco Laboratories, Houston, Texas, USA). Serum IgG antibodies to H pylori were measured using an enzyme linked immunosorbent assay (ELISA), the GAP test IgG kit (Bio-Rad Laboratories, Hercules, California, USA).
METHODS OF ANALYSIS
Iron deficiency anaemia was defined as a low serum ferritin concentration (< 12 ng/ml), low transferrin saturation (< 15%), and a low haemoglobin concentration (< 120 g/l).13 Helicobacter pylori infection was defined as a positive ELISA result. Centile values of height and weight were obtained by using standard Korean children's height and weight charts. We used the 25th centile values for height or weight as the threshold values for subnormal growth. To identify risk factors affecting growth, we sorted the subjects into four groups, based on the presence or absence of H pylori infection and iron deficiency anaemia, and which were defined as follows: (1) subjects having both iron deficiency anaemia and H pylori infection (IDA+/Hp+; n = 10); (2) subjects having iron deficiency anaemia only (IDA+/Hp−; n = 22); (3) subjects havingH pylori infection only (IDA−/Hp+; n = 53); and (4) subjects having neither iron deficiency anaemia norH pylori infection (IDA−/Hp−, n = 290). The means and 95% confidence intervals (CI) of height and weight distributions were calculated, and statistical adjustment was made for age differences; the four groups were then compared. The statistical interaction between H pyloriinfection and iron deficiency anaemia was also examined.
Sex, socioeconomic class, and household crowding were included as variables because it is known that they can affect the prevalence rate of H pylori infection and iron deficiency anaemia. Categorisation of socioeconomic class was based on the parents' occupation and education by applying the Hollingshead index14 (table 1). Five educational levels and five occupational categories were used to identify socioeconomic classes. A score of 0 was given to the lowest level of education and occupation and a score of 4 was given to the highest. Four socioeconomic classes were identified ranging from lowest (I) to highest (IV) on the basis of the sum of scores. Household crowding was shown by a crowding index: the number of persons living in the house divided by the number of rooms.
Educational and occupational levels of both parents used in forming the Hollingshead index of socioeconomic class
STATISTICAL ANALYSES
The χ2 test and the Mantel-Haenszel χ2test were used to assess the association between the independent factors related to the prevalence of H pylori infection and growth. The effects of risk factors such asH pylori infection, iron deficiency anaemia, sex, socioeconomic status, type of house, and crowding index on growth were analysed by multiple logistic regression modelling. These models enabled the assessment of the relative importance ofH pylori infection and iron deficiency anaemia while controlling for the other risk factors.
We used ANOVA to calculate and compare the mean and 95% CI values for the height and weight distributions after adjustment for age. The interactive effect of H pylori infection coupled with iron deficiency anaemia on growth was analysed by using the interaction term of H pylori infection and iron deficiency anaemia. Unless stated otherwise, a p value ⩽ 0.05 was taken to be significant. All statistical analyses were performed using SAS statistics software (version 6.12).
Results
The ages of participants ranged from 10 to 15 years (mean, 12.9 years). No differences were found in the demographic or physiological variables or the prevalences of H pyloriinfection and iron deficiency anaemia between those who did and those who did not respond to the questionnaire.
Sixty three of 375 children (16.8%) were infected withH pylori. Iron deficiency anaemia was found in 8.5%. Table 2 summarises the effects of independent variables on height and weight by univariate analyses. We found that 18 of 63 (28.6%) of H pylori positive children were below the 25th centile values for height, compared with 63 of 312 (20.2%) of H pylori negative children. However, this difference was not significant (p = 0.14). Significant differences in height and weight were found between those children with and without iron deficiency anaemia (p = 0.006 and 0.007, respectively).
The effects of independent variables on growth by univariate analyses
The prevalence rate of H pylori infection was 15.5% (53 of 343) in children without iron deficiency anaemia and 31.3% (10 of 32) in those affected (p = 0.022). The presence of iron deficiency anaemia was found to be significant by univariate analysis, but no such relation was found between H pylori infection and growth. Helicobacter pylori infection was also included in the multiple logistic regression model because there is a known relation betweenH pylori infection and iron deficiency anaemia. Table 3 shows the relative risks for height and weight in relation to H pylori infection and iron deficiency anaemia. In the logistic regression model, the relative risk of height below the 25th centile values was 2.2 (95% CI, 1.0 to 4.8) for the iron deficiency anaemia group, and 1.4 (95% CI, 0.8 to 2.4) for the H pylori infected group. The relative risk of weight below the 25th centile values was 2.1 (95% CI, 1.0 to 4.6) for iron deficiency anaemia, and 0.7 (95% CI, 0.4 to 1.3) for H pylori infection.
The results of logistic regression analysis of variables that are significant in the univariate analysis and their association with height and weight
Table 4 shows the means of the heights and weights obtained after adjustment for age in the four groups (IDA+/Hp+, IDA+/Hp−, IDA−/Hp+, and IDA−/Hp−). The mean height of subjects decreased significantly in the group having both H pylori infection and iron deficiency anaemia (p = 0.0104; fig1). No significant interaction was found between H pylori infection and iron deficiency anaemia in terms of growth (p = 0.2247).
Adjusted means (95% confidence intervals) of height and weight for age

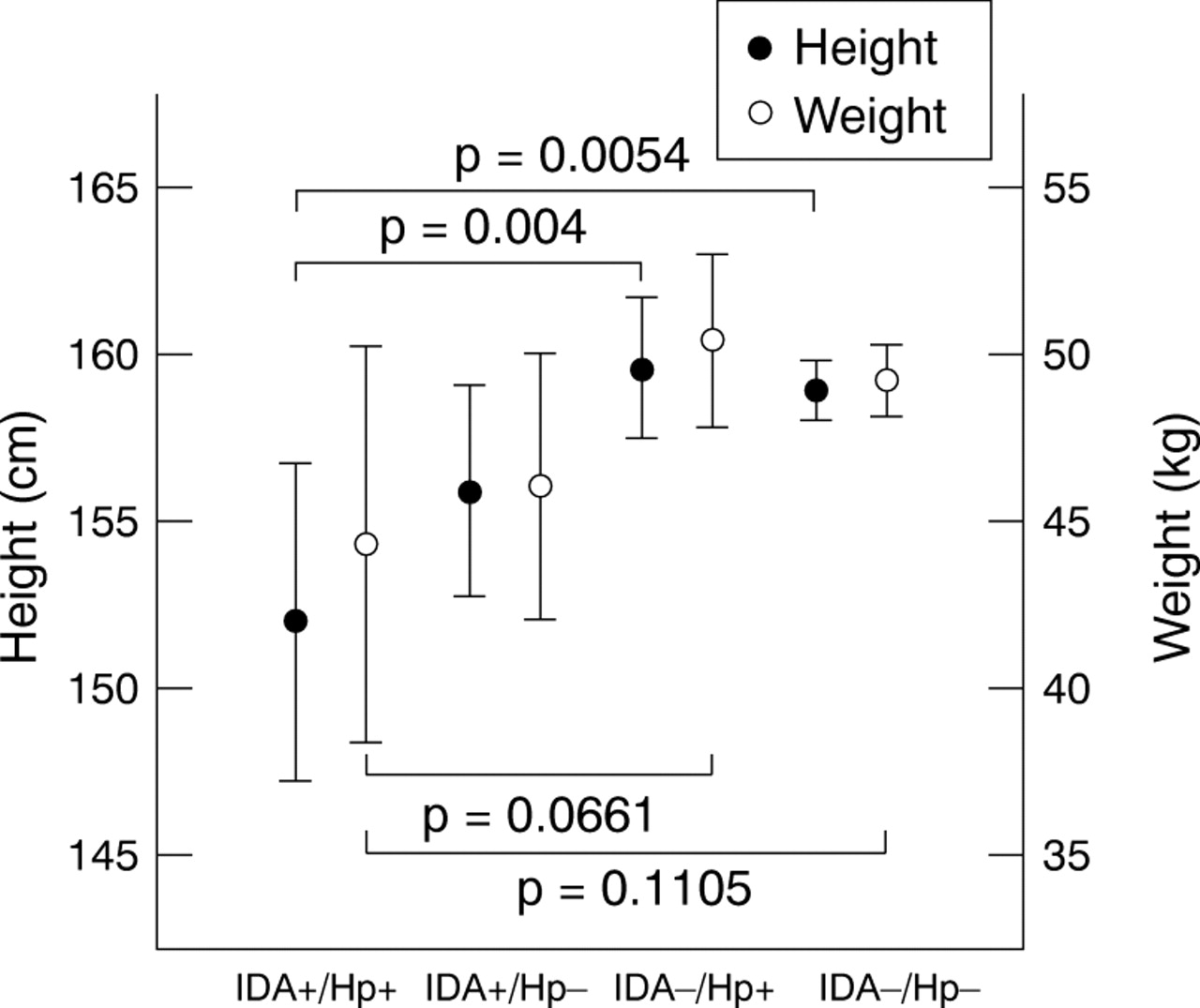{kind=link}
Comparison of the means of height and weight among the four groups. IDA+/Hp+, subjects with both iron deficiency anaemia and Helicobacter pylori infection (n = 10); IDA+/Hp−, subjects with iron deficiency anaemia only (n = 22); IDA−/Hp+, subjects with H pylori infection only (n = 53); and IDA−/Hp−, subjects with neither iron deficiency anaemia nor H pylori infection (n = 290). Ranges are 95% confidence intervals. The means of height and weight decreased in the group with both H pylori infection and iron deficiency anaemia (p = 0.0104 for height and 0.1252 for weight).
Discussion
Our data show that although H pyloriinfection seemed to affect growth when the population was analysed solely on the basis of infection, this is a result of the association between H pylori infection and iron deficiency anaemia. It is unlikely that H pylori infection alone is directly associated with the reduced growth of children, as some other studies have suggested.7 8 Perri et alproposed four mechanisms by which H pylori infection might lead to short stature.8First, that it could cause dyspeptic symptoms. Second, that the infection could result in a low energy intake and malnutrition. Third, that a long standing infection induces low grade chronic gastric inflammation and the release of cytokines that could affect growth. Finally, that H pylori might be associated with poor socioeconomic background, malnutrition, and exposure to other chronic diseases, which could affect growth. However, our findings reveal that H pylori infection coupled with coexisting iron deficiency anaemia is associated with subnormal growth at puberty, which is particularly associated with height.
The diagnosis of H pylori infection was assessed only by means of specific serum IgG antibodies. This is based on our experience of various tests used to diagnoseH pylori infection in Korean children.15 In our study, serological examination using the GAP test IgG kit showed a sensitivity of 94.9% and a specificity of 92.4% in Korean children. Hence, we used this test for the diagnosis of H pylori infection, although our case was somewhat weakened by the fact that H pylori was identified by serology only.
In our recent study, we found that H pyloriinfection contributed to iron deficiency anaemia, and that infection should be suspected when iron deficiency anaemia is refractory to iron administration.9 Treatment of H pylori infection was associated with a more rapid response to oral iron treatment than the use of iron alone, and it led to an enhanced iron absorption even in those who did not receive oral iron supplementation. We hypothesised that iron deficiency anaemia coupled with H pylori infection occurs most frequently in rapidly growing pubescent children. Adolescents are particularly susceptible to iron deficiency because of the high amounts of iron needed to sustain their growth, dietary deficiency, and menstrual blood loss in girls.10 Infection withH pylori might affect iron absorption metabolism in the stomach and exacerbate the iron deficit in children whose iron is supplied marginally, with anaemia ensuing promptly. Therefore, when adolescents have iron deficiency anaemia, it is recommended that they should be evaluated for H pylori infection. If they are found to have both, the iron deficiency anaemia should be treated by the eradication ofH pylori along with iron supplementation. It is hypothesised that when children who have been suffering from chronicH pylori infection are affected with iron deficiency anaemia, especially during adolescence, their growth can be affected. Although the mechanisms by which H pylori infection might lead to iron deficiency anaemia are still unclear, a recent study ruled out gastrointestinal bleeding or iron malabsorption and suggested that H pylorigastritis could act as a sequestering focus for iron.16
We found H pylori infection in 53 of 343 (15.5%) children without iron deficiency anaemia and in 10 of 32 (31.3%) affected children (p = 0.022). Of 63 H pylori positive children, 18 (28.6%) were below the 25th centile values for height, compared with 63 of 312 (20.2%)H pylori negative children. Although this difference seemed to suggest that H pyloriinfection could affect growth, it was not significant. After conducting logistic regression analysis, iron deficiency anaemia was still significantly associated with subnormal growth. The data from the analysis showed that iron deficiency anaemia had a significant effect on subnormal growth, rather than H pyloriinfection, which contradicts previous reports.7 8
When the subjects were divided into four groups, a significant decrease in the mean height of subjects in the group with bothH pylori infection and iron deficiency anaemia was found. The data for boys and girls were analysed separately but no significant difference could be found, although it seems probable that such differences exist, particularly in terms of the height and weight of boys (table 4). We believe that this difference was not significant because the number in the IDA+/Hp+ group was too small for accurate analysis: three boys and seven girls.
We looked for an interaction between H pylori infection and iron deficiency anaemia but failed to identify any such interaction that influenced growth. In spite of the lack of an interaction, growth delay was identified in the group havingH pylori infection accompanied by iron deficiency anaemia, and our study shows that iron deficiency anaemia is an independent risk factor. In addition, there is evidence thatH pylori infection contributes to iron deficiency anaemia.9 Therefore, we believe that bothH pylori infection and iron deficiency anaemia might contribute to subnormal growth.
We conclude that H pylori infection accompanied by iron deficiency anaemia, rather thanH pylori infection per se, might delay pubertal growth. When older children with reduced pubertal growth are found to be infected with H pylori, iron deficiency anaemia can be considered to be a cause of the growth deficit. Likewise, when they are found to be affected with iron deficiency anaemia, they should be evaluated for H pylori infection. If iron deficiency anaemia related toH pylori infection is causally associated with growth delay in adolescents, eradication of H pylori along with iron supplementation might be helpful in the treatment of children with pubertal growth delay andH pylori infection.
Acknowledgments
We thank MY Seo and MY Kim for their valuable contribution to this work.