Article Text

Abstract
Patients with functional gastrointestinal disorders may have visceral sensory dysfunction so that physiological stimuli induce their symptoms. The clinical significance of altered perception—that is, its relation to clinical symptoms—remains unclear. Data indicate that sensory dysfunction is associated with altered reflex activity. Hence evidence of combined sensory-reflex dysfunction as a common pathophysiological mechanism in various functional gastrointestinal disorders would suggest that they are different forms of the same process. Altered reflex activity and altered conscious perception of gastrointestinal stimuli may combine to differing degrees, and their interaction may produce clinical symptoms.
- visceral hypersensitivity
- visceral reflexes
- functional dyspepsia
- irritable bowel syndrome
- functional gastrointestinal disorders
- IBS, irritable bowel syndrome
Statistics from Altmetric.com
- visceral hypersensitivity
- visceral reflexes
- functional dyspepsia
- irritable bowel syndrome
- functional gastrointestinal disorders
SUMMARY
Experimental data collected over the past years suggest that patients with functional gastrointestinal disorders have visceral sensory dysfunction so that physiological stimuli induce their symptoms. Assessment of visceral sensitivity is still poorly developed but in analogy with somatosensory testing, differential stimulation by a combination of techniques may conceivably allow precise characterisation of sensory dysfunction. It has been well established that sensory dysfunction in patients with functional gastrointestinal disorders exclusively affects the visceral territory but the extent of the dysfunction in the different clinical syndromes remains controversial. Furthermore, the origin of visceral hyperalgesia has not yet been elucidated. Visceral afferent input is modulated by a variety of mechanisms operating between the gastrointestinal tract and the brain, and dysfunction of these regulatory mechanisms could distort gastrointestinal perception. The clinical significance of altered perception—that is, its relation to clinical symptoms—remains unclear. Some data indicate that the sensory dysfunction in these patients is associated with altered reflex activity, and both mechanisms may interact to produce the symptoms. Hence combined gastrointestinal sensory–reflex dysfunction seems to be a common pathophysiological mechanism in different functional gastrointestinal disorders, and these two effects may combine to differing degrees to produce specific clinical manifestations depending on the particular pathways that are affected. This working hypothesis would explain both the variety of clinical manifestations and the frequent overlap of gastrointestinal disorders.
INTRODUCTION
Patients with functional gastrointestinal disorders present with abdominal symptoms that have no organic cause demonstrable by conventional diagnostic tests. Because the underlying pathophysiology is unknown, the diagnosis of syndromes such as functional dyspepsia and irritable bowel syndrome (IBS) has traditionally been based entirely on clinical criteria.1
Functional gastrointestinal disorders were initially attributed to motor dysfunction. When the technology to study gastrointestinal motility became available, a variety of motor features were described in these patients. However, the way in which these motility patterns are related to symptoms remains unclear because the same features can also be observed in asymptomatic patients and healthy subjects. Thus by the late 1980s it had become apparent that the cause of most functional gastrointestinal disorders could not be explained solely on the basis of motility disturbances, at least not by those detected using standard manometric and electromyographic techniques. However, a series of contemporary studies suggested that patients with functional gastrointestinal disorders might have a sensory dysfunction which caused them to perceive normal physiological stimuli as gastrointestinal symptoms. These findings have triggered mounting interest in the field of visceral sensitivity, which until recently had only been explored superficially.2
INVESTIGATION OF VISCERAL SENSATION
As physiological stimuli to the gastrointestinal tract are normally not perceived, investigation of visceral sensitivity, at least in healthy humans, requires the induction of a test stimulus that activates afferent pathways and induces perception. The most commonly used stimulus is gastrointestinal distension, which is usually achieved by means of a distending device, a balloon or similar, mounted over an intraluminal tube. Distension can be produced either by manual inflation using a syringe or by means of more sophisticated methods such as the barostat, which applies fixed intraluminal pressures.3 Recent studies have shown that perception of gastrointestinal distension relies on stimulation of tension receptors. Interestingly, intraluminal volume and wall stretch do not appear to be involved in the process of distension.4 Hence the tensostat, which applies fixed levels of tension to the wall of the gastrointestinal tract, probably allows better standardisation of distending stimuli, regardless of the capacity or compliance of the organ being tested.
Gastrointestinal distension has been shown to induce symptoms which are similar to those reported by patients with functional gastrointestinal disorders; notably a sensation of abdominal pressure and fullness which are referred to the epigastrium and the paraumbilical region. The symptomatic response to distension is fairly homogeneous from the stomach down to the middle of the small bowel,5–8 suggesting that the response of the gastrointestinal tract to stimuli, and the discriminative value of symptoms in relation to the site of origin in the gastrointestinal tract, are both relatively poor. However, a small proportion of distensions in the stomach and proximal duodenum induce nausea. This is rarely induced by jejunal distension, which is frequently perceived as a colicky or stinging sensation.
Although the intensity of perception is stimulus related, the same type of sensations are induced by distensions that correspond to the threshold for perception as those associated with the threshold for discomfort. The inherent degree of sensitivity to stimuli along the gastrointestinal tract is also fairly uniform, but standardisation of distending stimuli in different segments of the gastrointestinal tract is nevertheless problematic.
Analogous to somatosensory testing, which involves a variety of stimulation techniques to activate specific pathways, stimuli other than distension have been tested in the gastrointestinal tract. Transmucosal electrical nerve stimulation has been applied to the intestinal tract using intraluminal electrodes mounted over a tube.5,6 Unlike distending stimuli which activate sensory pathways and induce perception by specific stimulation of mechanoreceptors on the gastrointestinal tract wall, transmucosal nerve stimulation induces a similar type of perception by non-specific stimulation of afferent pathways.
Thermal stimulation methods, involving both cold and warm stimuli, have been developed to test the sensitivity of visceral afferent fibres.9 Thermal stimulation of the gastrointestinal tract can be produced using intraluminal bags containing recirculating water at preset temperatures. It has been shown that the stomach and the intestines exhibit similar stimulus related thermal sensitivity but gastrointestinal thermosensitivity in humans, and specifically the identity of the afferents that are activated by warm and cold stimuli, remain under explored. Nevertheless, thermal stimuli still play a potentially useful role in conjunction with mechanical and electrical stimuli for the evaluation of gastrointestinal sensory dysfunction. Thus differential stimulation by a combination of techniques may conceivably help to define the sensory dysfunction in different subsets of patients with unexplained abdominal symptoms.
VISCERAL SENSATION IN FUNCTIONAL GASTROINTESTINAL DISORDERS
The sensory disorder associated with functional gastrointestinal disorders exclusively affects the viscera. Sensitivity,6,10 and the visceral responses to somatic pain, are normal as shown by the finding that somatic pain produced by cold stress induces gastric relaxation in patients with functional dyspepsia as well as in healthy subjects.11
The extent of gastrointestinal sensory dysfunction in patients with functional disorders remains controversial. Increased gastric but normal duodenal sensitivity has been shown in a specific subset of patients with functional dyspepsia, predominantly those complaining of postprandial bloating.10 In this study patients invariably stated that gastric distension, but not duodenal distension, reproduced customary symptoms whereas in healthy subjects both stimuli were perceived similarly (figs 1, 2). However, other studies have reported that patients with functional dyspepsia have an increased perception of intestinal distension.12 It has also been reported that patients with non-cardiac chest pain have a tendency to over interpret oesophageal stimuli as painful. These findings indicate that patients with functional dyspepsia form a heterogeneous population, and the different selection criteria that were used in these studies may explain these apparently conflicting results.
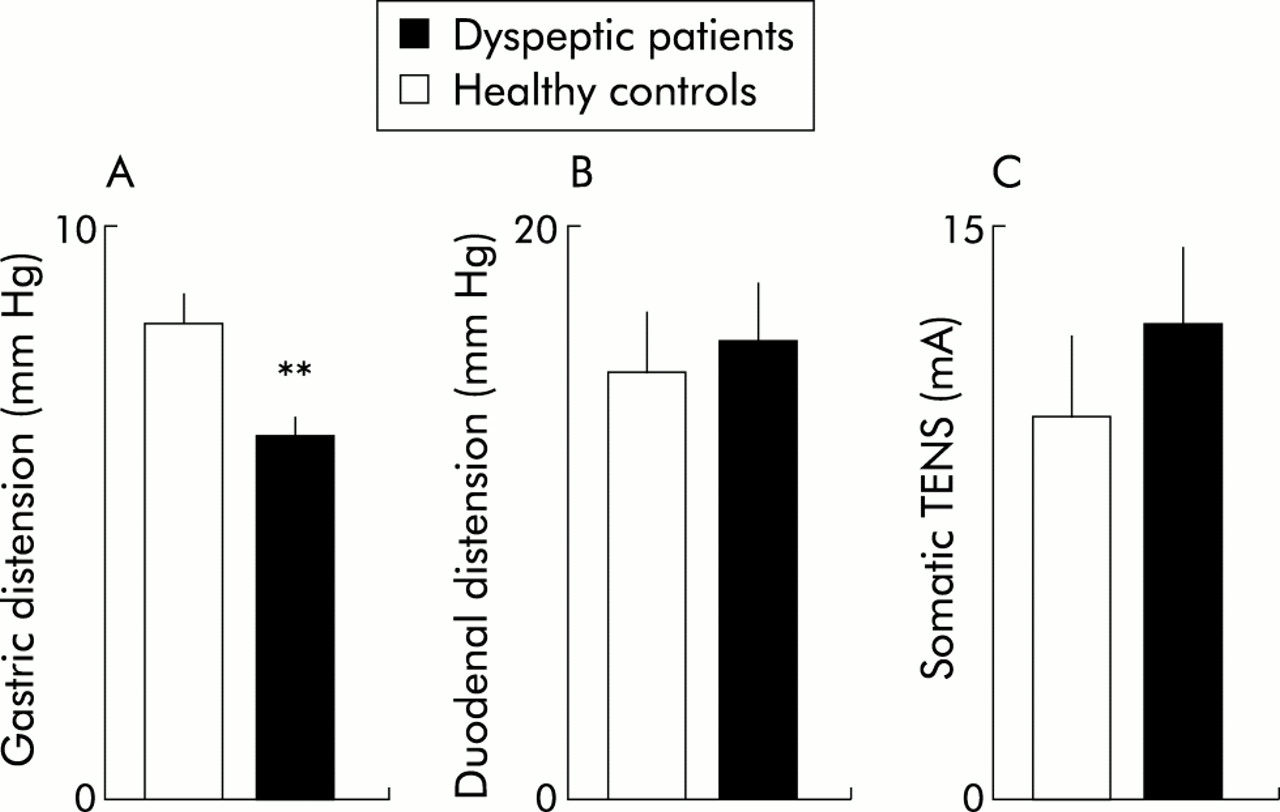
Visceral and somatic sensitivity in functional dyspepsia. The thresholds for discomfort to gastric distension (A), duodenal distension (B), and transcutaneous nerve stimulation (TENS) (C) applied on the hand are shown. Patients with dyspepsia experienced discomfort at significantly lower intragastric pressures than healthy controls (**p<0.01) but perception of both duodenal and somatic stimuli was normal. Reproduced with kind permission from Coffin and colleagues.10

{kind=link}
{kind=link}
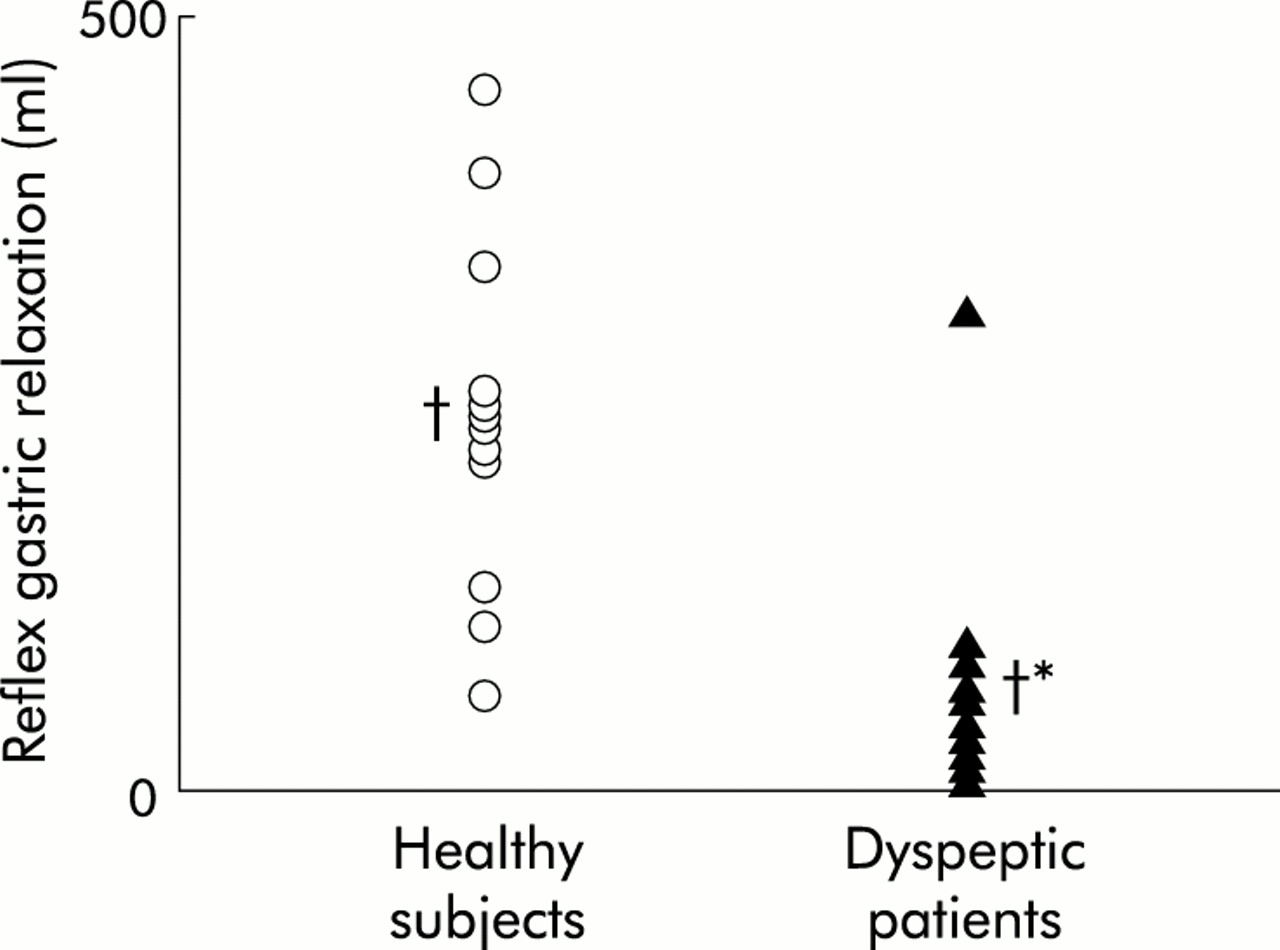
Enterogastric reflex induced by distension in functional dyspepsia. Individual gastric relaxatory responses to duodenal distension are shown (†mean values). The gastric relaxatory response was significantly smaller in dyspeptic patients than in healthy controls (*p<0.05). Impaired gastric relaxation after a meal in hypersensitive patients may produce dyspeptic symptoms. Reproduced with kind permission from Coffin and colleagues.10
Patients with IBS typically display hypersensitivity of the colon and rectum2,13 but more proximal regions of the gastrointestinal tract, such as the jejunum and even the oesophagus, may also be affected.6,14 Studies using mechanical stimuli or transmucosal nerve stimulation have shown that patients with IBS have a form of small bowel hypersensitivity that selectively affects mechanosensitive afferents, without disturbing normal perception of electrical stimulation.6 For instance, transmucosal electrical nerve stimulation in patients with IBS induces normal perception, even though electrical and mechanical stimuli produce similar sensations in most tests.6 These data suggest that small bowel hypersensitivity in IBS is related to selective alteration of mechanosensitive pathways but neither the cause nor the level of the afferent dysfunction has been established.
MODULATION OF VISCERAL SENSATION
Visceral afferent input is modulated by a variety of mechanisms operating between the gastrointestinal tract and the brain and conceivably, alteration of these mechanisms could result in distorted gastrointestinal sensation. The responses to gastrointestinal distension depend on muscular activity and compliance. Increased sensitivity to mechanical stimuli may arise from reduced compliance of the intestinal wall but a hypersensitivity mechanism cannot be ruled out because in most studies intestinal compliance was found to be normal.6,10,11
Visceral perception is also modified by the interaction of different stimuli. For instance, intestinal lipids increase the sensitivity of the intestine to mechanical stimuli, independently of any changes in intestinal compliance. Rather, sensitisation induced by lipids seems specifically related to mechanoreceptors because perception of transmucosal electrical stimulation which non-specifically activates afferents without relying on specific receptor activation, is not modified by intraluminal lipids. Cholecystokinin has been shown to sensitise mechanoreceptors and may play a role in this type of hypersensitive response.
The autonomic nervous system which regulates gastrointestinal function is thought to modulate visceral sensitivity. Increased sympathetic tone is known to increase the level of perception of gastrointestinal stimuli, without affecting reflex responses.15 Alteration of the sympathetic modulation of visceral sensitivity may therefore play a clinically relevant role in functional gastrointestinal disorders. Recent studies indicate that patients with IBS have increased sympathetic activity,16 and it is these patients who exhibit a similar type of sensory disturbance to that produced by sympathetic activity in that they manifest visceral hypersensitivity but have normal or even increased tolerance to somatic stimuli.6,13
Visceral perception is also known to be mediated at a cortical level and may therefore be influenced by cognitive mechanisms. Mental attention has been shown to increase perception to gastrointestinal stimuli,17 and there is evidence that psychological mechanisms play a role in modulating perception.18 These findings raise the possibility that patients with functional gastrointestinal disorders may pay more attention to gastrointestinal events than normal subjects.
VISCERAL REFLEXES IN FUNCTIONAL GASTROINTESTINAL DISORDERS
It has been shown that patients with functional gastrointestinal disorders may have altered visceral sensation but it is uncertain whether a sensory dysfunction per se explains the symptoms or whether they are associated with other types of dysfunction. Conventional techniques have failed to show significant gastrointestinal motor abnormality in these patients but more recent mechanistic studies have demonstrated the existence of specific reflex dysfunction.7,8,10 Normally, physiological stimuli induce both vagal and sympathetic reflexes that regulate the motor function of the gastrointestinal tract. Conceivably, reflex dysfunction may produce relevant motor abnormalities that are not detectable by conventional manometry.
Gastrointestinal reflexes in humans can be investigated in the laboratory by measuring the responses to distending stimuli. The barostat, which records changes in gastrointestinal tone, has proven particularly useful in this setting because brief inhibitory reflexes may be missed by recording intermittent phasic activity.7,8 In contrast with the uniformity of perception, the reflex responses to gastrointestinal distension are quite heterogeneous. Some researchers suggest that perception and reflex responses are dissociated and probably mediated by different mechanisms.7,8 From a pathophysiological standpoint this may be a very important finding because it infers that under certain conditions perception and reflex responses to gastrointestinal stimuli may be altered independently of one another. For example, patients with functional dyspepsia who have gastric hypersensitivity have also been shown to have impaired gastric reflexes.10 In these studies gastric relaxation in response to duodenal balloon distension, an enterogastric vagal reflex, was impaired in patients with functional dyspepsia who had normal duodenal sensitivity and compliance. Other studies indicate that the intestinal motor responses to distension (that is, the sympathetic intestino-intestinal reflex) may also be impaired in these patients.12
Although concomitant dysfunction of sensory and reflex pathways has not been explained satisfactorily, it is possible that both interact in a way that promotes the onset of symptoms. For instance, food ingestion normally induces relaxation of the proximal stomach to accommodate the meal without increasing intragastric pressure.19 The magnitude of the relaxation is regulated by nutrient dependent enterogastric reflexes, and as the relaxatory input decreases, the proximal stomach gently forces intragastric content into the antrum. In functional dyspepsia, gastric hyporeactivity to enterogastric reflexes would predictably result in defective accommodation of the proximal stomach with accompanying antral overload, thereby reducing fundal residence time and increasing antral filling.20 It can be further questioned whether, in the presence of marked postprandial antral distension, normal contractions may no longer occlude the lumen giving a false impression of antral hypomotility on manometric recordings. This situation is conceivable for corpus-antral function but unlikely in the prepyloric antral region. Impaired meal accommodation would tend to potentiate the hypersensitivity to distension because the stomach can only tolerate small volumes if not properly relaxed.3 Experimental data indicate that increased intragastric pressure after a meal, resulting from defective gastric accommodation, produces dyspeptic-type symptoms without disturbing gastric emptying.19 This condition resembles the experience of most patients with functional dyspepsia.21 Hence it is plausible that gastric hyporeflexia exacerbates the poor tolerance of patients with functional dyspepsia to intragastric volumes and thus contributes to the onset of clinical symptoms in the absence of major motor dysfunction.
Recent studies using a new methodology to evaluate intestinal gas dynamics further substantiate the role of combined sensory-reflex disturbances. These studies have shown that gas symptoms in patients with IBS and functional bloating are related either to impaired intestinal handling of gas leading to retention, to gastrointestinal hypersensitivity with poor gas tolerance, or both.22
CONCLUSIONS
Symptoms in patients with functional gastrointestinal disorders may be related to abnormal sensation but three key aspects of this putative relationship still remain obscure. Firstly, currently available methods fail to detect abnormal perception in all patients, suggesting that other factors may also be involved. Secondly, sensory dysfunction has not been characterised, even though potential mechanisms have been identified. Thirdly, abnormal gastrointestinal perception seems to be associated with reflex gastrointestinal dysfunction, and both could interact to produce symptoms.
Interestingly, evidence of sensory-reflex dysfunction as a common pathophysiological mechanism in various functional gastrointestinal disorders would suggest that they are different forms of the same process. Altered reflex activity and altered conscious perception of gastrointestinal stimuli may combine to differing degrees, and their interaction may produce clinical symptoms. The specific clinical syndromes would thus depend on the pathways affected.