Article Text

Abstract
Visceral hypersensitivity is widely regarded as the reason for the development of functional gastrointestinal disorders, including functional dyspepsia and irritable bowel syndrome. The principles and techniques involved in testing the hypothesis that visceral sensitivity is important are discussed, together with the controversies in the assumptions, methods, and interpretations of the data acquired to date.
- visceral sensation
- barostat
- tensostat
- tension
- stretch
- receptors
- functional gastrointestinal disorders
- ACC, anterior cingulate cortex
- IBS, irritable bowel syndrome
- MRI, magnetic resonance imaging
- SPECT, single photon emission computed tomography
- VAS, visual analogue scale
Statistics from Altmetric.com
- ACC, anterior cingulate cortex
- IBS, irritable bowel syndrome
- MRI, magnetic resonance imaging
- SPECT, single photon emission computed tomography
- VAS, visual analogue scale
SUMMARY
Although visceral hypersensitivity is widely regarded as important in functional gastrointestinal disorders, the optimal methods for its assessment are unclear. This paper reviews some of the principles and techniques involved in testing the hypothesis that visceral sensitivity is important, namely: barostat; different distension paradigms; tensostat; and impedance. The role of wall tension is discussed as it relates to activation of tension or volume receptors. Measurement of wall properties such as compliance and accommodation, and novel simple methods, such as a nutrient drink test, may bring these assessments to the clinical management of patients.
INTRODUCTION
Visceral hypersensitivity is widely regarded as the reason for the development of functional gastrointestinal disorders, including functional dyspepsia and irritable bowel syndrome (IBS).1 Although the field has advanced considerably in the past decade, the goal of this article is to discuss controversies in the assumptions, methods, and interpretations of the data acquired to date, and to explore areas requiring more thorough study. As there is insufficient research to provide comprehensive or broad perspectives, data from several regions of the gastrointestinal tract will be examined.
DEFINITIONS OF VISCERAL SENSATION PARAMETERS
Prior to discussing the pros and cons of measurements of parameters considered in describing sensation, a few definitions are essential.
Accommodation
Accommodation is the relaxation of the stomach in the early postprandial period. Using the barostat, wall tone is assessed as the relative change (that is, not an absolute measurement) of stomach volume under constant pressure. However, the volume of accommodation can also be measured with novel imaging methods such as single photon emission tomography (SPECT), magnetic resonance imaging (MRI), or three dimensional ultrasonography.
Compliance
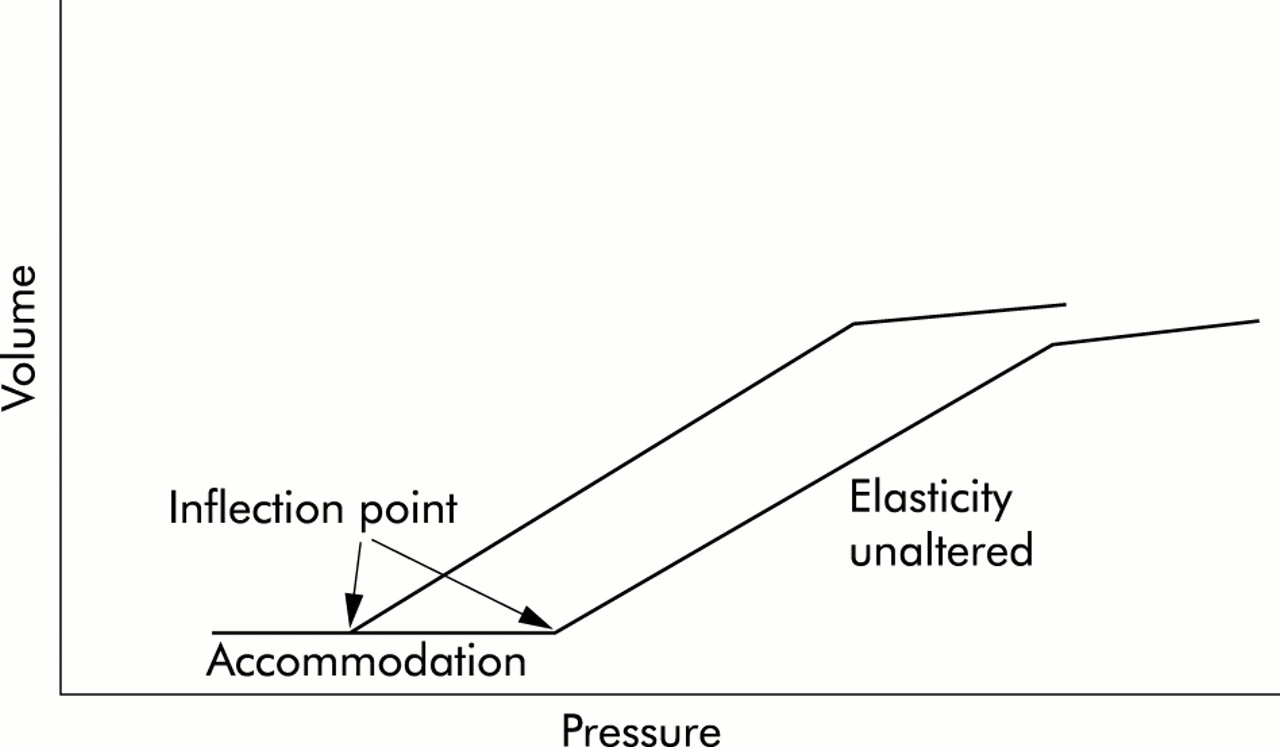
Compliance is the volume response (y axis) to an imposed pressure (x axis). As shown in fig 1, there is a sigmoid relationship with initial reflex relaxation (change in wall tension without volume change), followed by a linear section that reflects partly the elasticity of the viscus wall, and a final plateau phase. Compliance is inversely related to elastance. Wall compliance is measured by means of isobaric stepwise (ramp) distension (for example, with a barostat). The nature of the balloon (latex or polyethylene) and the method of inflation influence the results.2–6
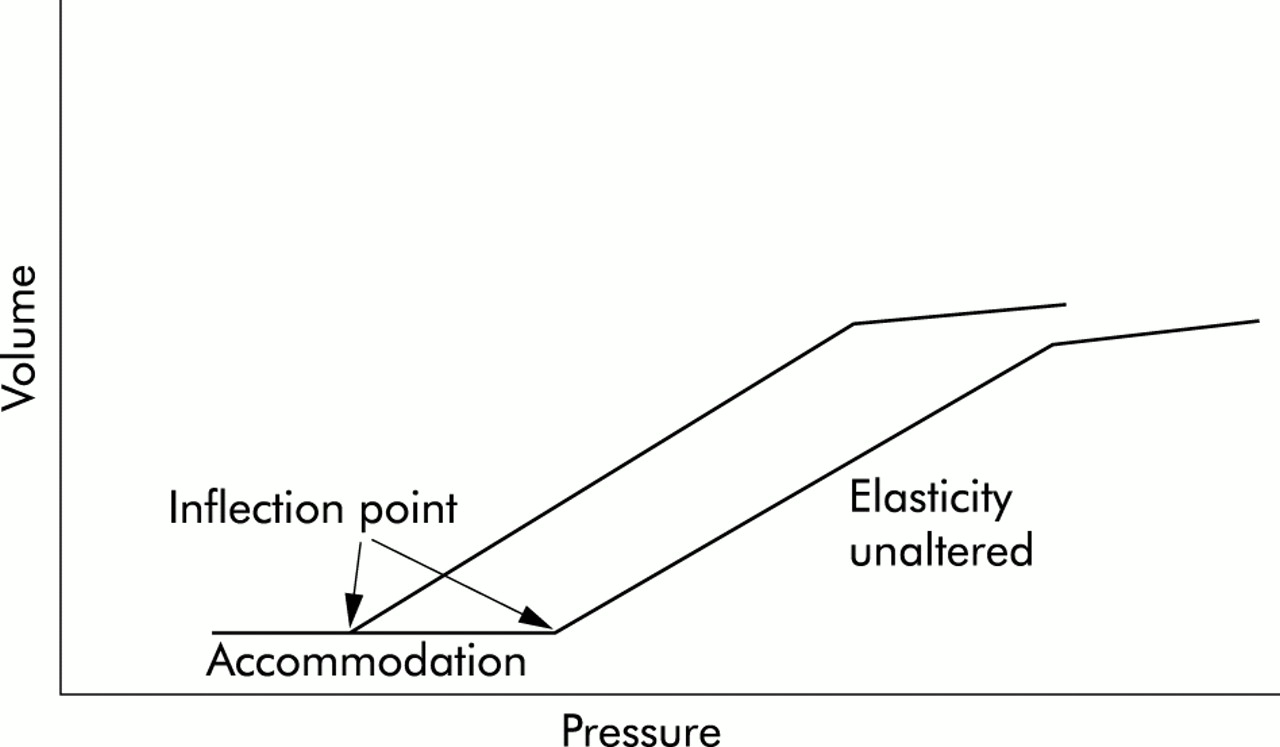
Viscus compliance curves: a shift to the left of the curves is reflected in a change in inflection point (tone) although the elasticity (slope) is unaltered.
Wall tension
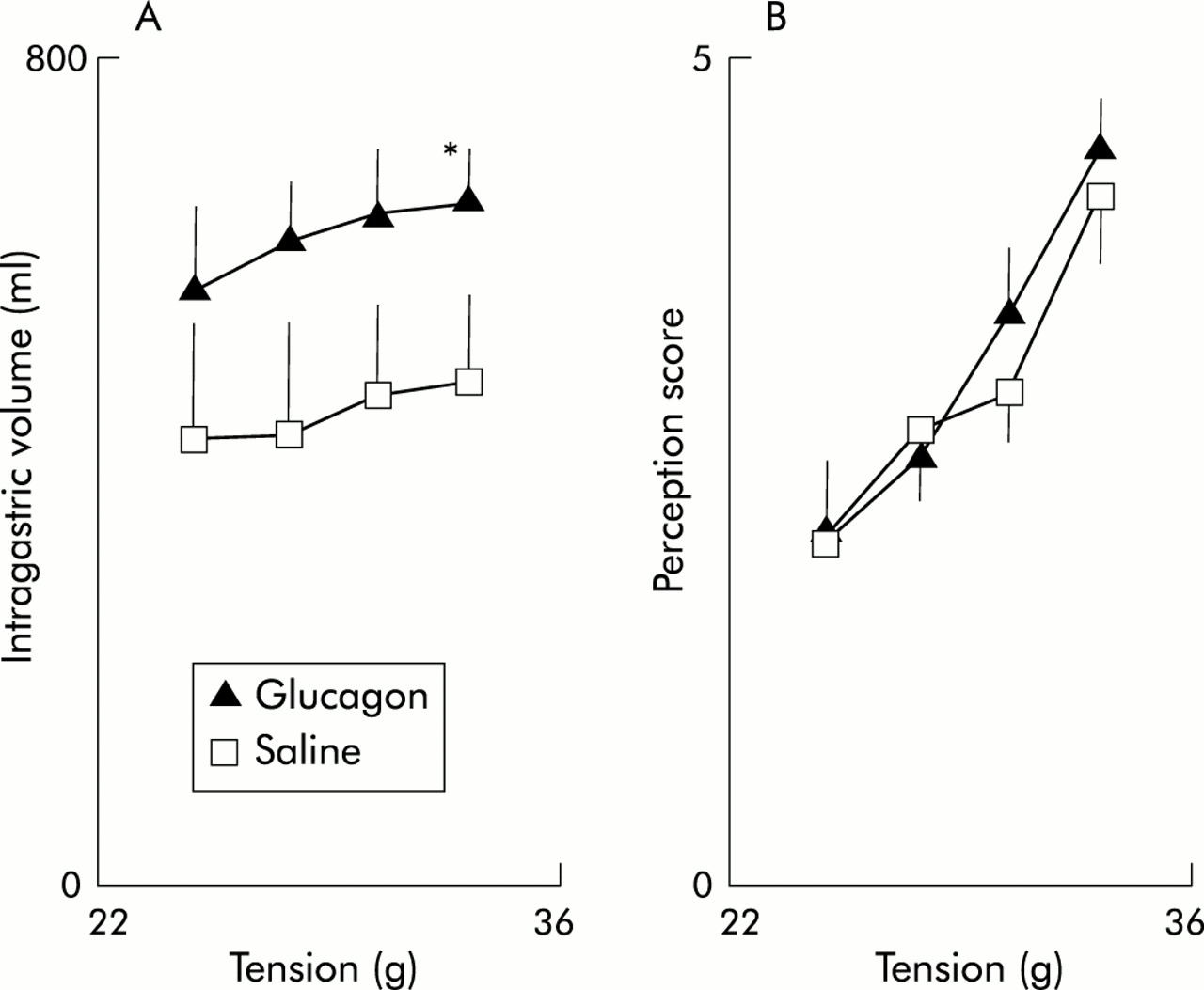
Wall tension has been calculated using the law of Laplace (T≈P×r), derived with a slight difference in the formula for the actual shape of the balloon (for example, cylinder, sphere) in the viscus segment tested. This measurement assumes several factors which are unknown in most studies performed in humans. It was claimed that measurement of tension would be more relevant to the investigation of sensory changes7 but correlation of sensation in response to tension based stimuli may not be significantly better than pressure based stimuli (fig 2).

Erroneous interpretation of sensations based on effects of glucagon compared with saline when distension is based on different parameters. However, the linear relationships for perception (C) and volume (A) (r=0.82; r=0.86; p<0.05), and tension (B) (r=0.96; p<0.005) are all significant and not qualitatively different. *p<0.05, **p<0.01. Reproduced with kind permission from Distrutti and colleagues.7
An alternative method, which has been used to measure rectal wall tension, is impedance planimetry.8 In these studies increased wall tension was associated with greater sensation of the need to defecate but, as shown in fig 3, similar increases in sensation were observed with increases in distension pressure.7
Use of tensostat as distending device provided data suggesting that, even in the relaxed state, perception was unchanged by glucagon. *p<0.05 versus saline. Reproduced with kind permission from Distrutti and colleagues.7
It has been suggested that the simplified law of Laplace can be used to estimate wall tension during barostat studies of hollow organs, and that this level of wall tension determines the level of perception during distension studies.7 Nevertheless, this formula makes a number of assumptions, which are not necessarily fulfilled by the experimental conditions. The assumptions include: the wall of the viscus is infinitely thin; the intraluminal balloon and viscus have a perfectly defined (for example, spherical) shape that can be defined mathematically; and the pressure external to the viscus is known and is evenly distributed. Most importantly, Laplace formulae do not take into account the modulatory effects of changes in the contractile state of the viscus, which may occur reflexly or in response to neurohumoral or pharmacological modulation, and which are superimposed on the compliance of the hollow organ. The limitations in current assessments of tension with tensostat or barostat were recently discussed by Gregersen9 who emphasised the error in the assumption that tension is equal throughout the proximal stomach (that is, isotropic), particularly in view of the complex and variable geometry of the stomach within and between individuals (fig 4). These differences in geometry render invalid a theoretical attribution of shape (for example, spherical, ellipsoid, or more complex shapes).

Single photon emission computed tomography (SPECT) images of the stomach, demonstrating differences in shape in health and disease, making calculations of volume difficult.
Hypersensitivity, hyperalgesia, allodynia
These terms, which were originally used in reference to somatic sensation, have been adapted to studies of visceral sensation. Hypersensitivity refers to increased sensation of stimuli. In practice, this is appraised by measurement of threshold volumes or pressures for first sensation or pain. Alternatively, it refers to the increased scores of symptoms (including pain) in response to standard stimuli. Hyperalgesia refers to increased pain sensation in response to a certain stimulus. Allodynia refers to the appreciation that a stimulus, which was previously not perceived as being painful, becomes painful.
VISCERAL HYPERSENSITIVITY IN FUNCTIONAL GASTROINTESTINAL DISORDERS
Studies indicate that patients with IBS have a heightened sensitivity to distension in the gastrointestinal tract.10–13 The evidence to support this hypothesis includes the presence of excessive sensitivity to balloon distension in the rectosigmoid and anorectum10–12 and lower thresholds for sensation to rectal gas, stool, and discomfort, which is most evident in diarrhoea predominant IBS.11,12 In addition, increased rectal sensitivity has been shown to be associated with increased motor responsiveness11 and, finally, patients with IBS have different cerebral areas of activation in response to rectal distension, as shown by positron emission tomography imaging.13
Hypersensitivity in functional dyspepsia is associated with normal gastric compliance,14,15 abnormal gastric accommodation,14–17 and hyperalgesia.18 The cofactors of this hypersensitivity are likely to be wall tension and the function of visceral afferents. Impaired gastric accommodation has been associated with the symptoms of weight loss and early satiety17 but in our experience the patient's symptoms do not allow a clear prediction of the presence or absence of impaired gastric accommodation.16 However, all systematic studies suggest that there is a cohort of functional dyspepsia patients who have normal gastric emptying, compliance, and accommodation and the most attractive hypothesis is that they experience symptoms secondary to hypersensitivity.
It cannot yet be concluded that increased perception, as it is currently assessed, is a biological marker for IBS. “Thresholds” for sensations are not sufficiently discriminant, and multifactorial analyses that evaluate sex, age, viscus compliance, somatic sensitivity, associated myofascial, or other psychosomatic (for example, somatisation) disorders need to be assessed in clinical subgroups of IBS.
The testing of upper gastrointestinal, colonic, or rectal sensation has not moved into clinical practice for a number of reasons, chiefly the invasive nature of testing, and the absence of standardised and validated tests.
MEASUREMENT OF VISCERAL SENSITIVITY IN HUMANS
Visceral sensitivity has been studied in humans for over a decade.10–12,14–16,18 It is now considered that patients with IBS and functional dyspepsia have increased visceral sensitivity detected by decreased pain and sensation thresholds to distension. The discussion that follows draws on evidence acquired from studies of the stomach or colorectum to provide a framework for understanding the methods, assumptions, and pitfalls in testing the visceral hypersensitivity hypothesis in humans. Table 1 summarises the types of tests and main pitfalls.
Tests of visceral hypersensitivity and main pitfalls
Thresholds
Several groups have reported on the use of threshold volumes and pressures in assessing the hypersensitivity of functional dyspepsia and IBS, and as a means to assess the effects of visceral sensation modulators. In IBS, the proportion of patients with increased sensitivity ranges from 30% to 85% across different series, questioning whether this is a biological marker of IBS.
The simple ascending method of limits has been found to be equivalent to the more complicated random staircase method to determine the thresholds for sensations.19 Compliance measurements can be accomplished during the same ascending method of limits but this method requires repetitive questioning at each step of the pressure distensions and may introduce elements of fatigue or perceptual bias. Preliminary data, presented in abstract form, have shown that threshold assessments correlate weakly with current symptoms and with responses to therapy; thus, for example, the correlations between thresholds and symptoms are typically in the 0.3–0.4 range 20. Moreover, Riberdy-Poitras and colleagues21 showed poor responsiveness of rectal sensory thresholds despite clinical response to tricyclic antidepressants in patients with IBS.
PHASIC DISTENSIONS AND VISUAL ANALOGUE SCALE (VAS) OF SENSATION
Studies by Ford and colleagues22 were instrumental in developing the alternative method for studying the sensation of colonic stimuli by applying a limited number of stimuli and a VAS to quantify intensity of sensation to gas, pain, and urgency. This approach was intended to reduce the perceptual bias that is more likely with repetitive questioning and distensions. Ford and colleagues22 validated responsiveness of the method to varying stimulus intensity and psychosensory modulation. These studies showed that increasing levels of distension of a colonic balloon produce a progressive increase in the symptom scores of gas and pain. These studies applied predefined pressure based stimuli to the balloon, anchoring the values above a baseline operating pressure to attempt to correct for differences in dimension, anatomy, or location of the balloon within the viscus. Moreover, the method took two other precautions: firstly, randomisation of the order of the three or four distensions, to avoid an order effect. Secondly, the investigators assessed the influence of the state of tension or anxiety of the individual on reported sensation, by assessing the level of tension immediately before applying the sensory test and accounting for it in the statistical analysis of sensation scores.
These initial studies also validated the responsiveness of the sensations of gas and pain to psychosensory modulation (relaxation and mental stress) during distensions of the sigmoid and transverse colon. Psychosensory modulation alters the perception of distension. Thus this method is responsive to changing environments or perturbations.
Others at the Mayo Clinic have documented the responsiveness of the sensations of gastric and colonic distensions during pharmacological modulation with α2 adrenoceptor agents.23–27
Cerebral projection of visceral sensation
Indirect observations suggest that changes in cerebral function can alter the overall sensation experienced in response to bowel manipulation. Thus the sensation of the colon in humans is susceptible to physiological and pharmacological perturbations. In such studies evaluation of the effects of stress provide models for understanding interactions between psychosocial, motor, and sensory disorders in IBS. For example, psychosensory modulation resulted in changed sensation at a given stimulus in healthy subjects.22 Colonic contraction after meal ingestion may alter sensation in animals28; similarly, enhancement of colonic tone during hyperventilation has been shown to increase sensation in humans.29 The α2 adrenergic mechanism appears to be quite important in modulating colonic compliance and sensation23 but, as in the stomach, colonic sensation may be altered independently of the physical properties of the colonic wall.
Much attention has recently been paid to the question of the central projection of visceral stimuli. Price30 has reviewed the ascending pathways, subcortical, and cortical centres involved in somatic sensation, and the cascade of interrelated events that bring into activation several of the centres involved in the various dimensions of sensation. Thus nociceptive input results in nociceptive sensations through the somatosensory cortical centres S1 and S2, as well as arousal of autonomic areas, such as the reticular formation, hypothalamus, and amygdala, which contribute to the autonomic and appetite responses to pain perception. Together these experiences of somatosensory and autonomic nature contribute to the sensation of immediate pain unpleasantness which is associated with activation of the anterior cingulate cortex (ACC). Secondary activation of the prefrontal cortex is associated with the second order appraisal of the pain and a secondary pain affect.
While there is not complete consensus on the centres activated during visceral (gut) sensations, many of these same centres are shown to be activated during experimental pain. Thus some very intriguing studies suggest that patients with IBS have a propensity to activation of the dorsolateral prefrontal cortex rather than the ACC during anticipation of rectal distension or during actual rectal distension.13,31,32 These observations were not observed in healthy subjects13 or in patients with predominant fibromyalgia and associated IBS symptoms.32 One interpretation of these data is that attention and vigilance, activated in anticipation of rectal distension as well as in response to pain, result in activation of the frontal areas in IBS. Brain imaging studies have shown that among those patients with predominant fibromyalgia and concomitant IBS, there is a preferential increase in cerebral blood flow during somatic rather than rectal stimulation and vice versa; patients with overlap and predominant colonic symptoms show increased blood flow during rectal than somatic stimuli.32
Several other factors or covariates can influence the observed change in regional cerebral blood flow. Vigilance and attention alter regional brain activation with non-visceral (somatic) pain perception. Thus the level of attention modulates activation of the primary somatosensory cortex during somatic pain stimulation.33 Moreover, Ploghaus and colleagues34 showed that anticipation of somatic pain was associated with prefrontal activation while actual pain characteristically increased the blood flow through the caudal ACC.
The perceived unpleasantness of a visceral sensation may also influence the site of activation.35 Thus there is greater activation in the ACC than in the somatosensory cortex when stimuli of an unpleasant nature are being perceived. By applying a somatic stimulus and changing the level of unpleasantness by concomitant hypnosis, Rainville and colleagues35 demonstrated that there was greater activation in the ACC but not in the somatosensory cortex.35
The intensity of experienced pain also influences activation of the insula and thalamus.36 Sex differences in cerebral blood flow in response to stimulation with noxious heat stimuli applied to the left volar forearm have been reported by Paulson and colleagues.37 Thus females had greater activation of the thalamus, anterior insula, and prefrontal cortex compared with males. Finally, facial expression can also change brain activation. Blair and colleagues38 have shown that sadness resulted in activation of the left amygdala and temporal pole whereas anger was associated with activation of the orbital frontal and ACC.
Thus the centres associated with gut sensations are partly understood but cerebral imaging studies to date have not incorporated pharmacological ligands which are essential for a better understanding of the mediators involved in sensory pathways and the causes of visceral afferent dysfunction.
CONTROVERSIAL INTERPRETATION OF VISCERAL SENSATION DATA
This section addresses a number of controversial issues pertaining to visceral sensation. Such controversial statements and interpretations include the assumption that if a drug alters perception without a change in compliance, it must do so by altering visceral afferent function. Other examples include the assertion that wall tension determines the level of sensation in a viscus and that relaxation results in reduced perception.
Compliance and perception
Interpretation of perception data in response to pharmacological perturbations has incorporated measurements of organ compliance. Thus when compliance is unchanged but sensation is altered, it has been implied that afferent nerve function has been affected. This is illustrated by the example of octreotide, which alters sensation without changing compliance,39–42 suggesting that its effect must be on afferent nerve function. However, octreotide also reduces postprandial colonic tone, suggesting that it may blunt reflex contraction to physiological stimuli.43 More relevant to the interpretation of sensation is the potential of the effect of the drug on baseline or postprandial tone as this is usually the background state of contraction at which the sensation occurs in patients.
There is moreover much variation in the literature pertaining to the method of performance of compliance measurements.44 These variations relate to the actual distension paradigms and perhaps, more importantly, to the mathematical methods to analyse the pressure-volume curves.
Preliminary reports by Bharucha and colleagues45 suggest that the standard method used for the last decade (2–4 mm Hg steps, one minute distensions, with one minute intervals between distensions, measuring volume during the second half of the minute of distension) cannot be appreciably improved by prolonging the distension period, or the interval between distensions. This is important as it also suggests that the ascending method of limits can be used simultaneously with the determination of thresholds for first sensation, urgency, and pain.
The optimal mathematical model for summarising the compliance curve involves estimation of the initial “cushion” in which pressure increments do not result in increased volume (true compliance), and a separate estimate of the elastic properties of the viscus, as indicated from the slope of the linear portion of the pressure-volume relationship. At the very least, the compliance measurement should summarise the entire curve with a parameter such as the pressure at half maximum volume in the standard ramp distension sequence. This allows assessment of the effects of medications such as clonidine on colonic compliance,23 and the lack of effect of a 5-HT3 antagonist on compliance of the rectum.27
Tension
The relationship between tension in the wall and sensation7 is also complex and, as indicated in the previous discussion, requires more thorough study. When a compliance curve is shifted to the left or right with no change in volume but a change in pressure, a simple application of Laplace's law would suggest that there has been a change in wall tension. Such a change may not be identified if only the slope of a linear model is applied to the compliance curve. It is still unclear from animal observations (fig 5) whether the sensory apparatus is a tension, pressure, or volume receptor (fig 6), and whether it is in series or in parallel.46,47 Further basic research is needed to help interpretation of observations in whole organs.
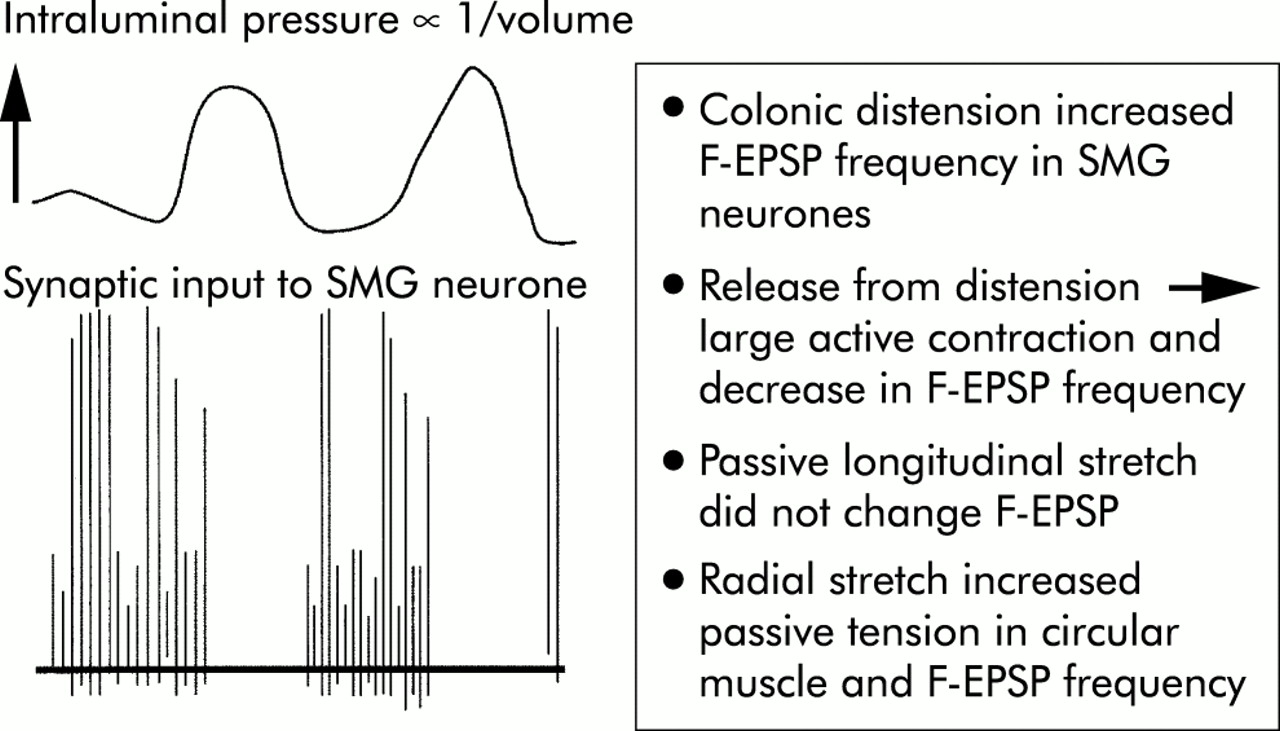
Plot of the relationship between intraluminal pressure, with firing of colonic mechanosensory afferents, and synaptic input recorded by a mesenteric ganglion neurone. Data suggest in parallel tension receptors in circular muscle. F-EPSP, fast excitatory postsynaptic potential; SMG, superior mesenteric ganglion. Reproduced with kind permission from Miller and Szurszewski.46

Model of the effects of distension, relaxation, and contraction on sensory activation. Reproduced with kind permission from Camilleri and colleagues.47
Isovolumetric stimulation: relaxation versus antinociception
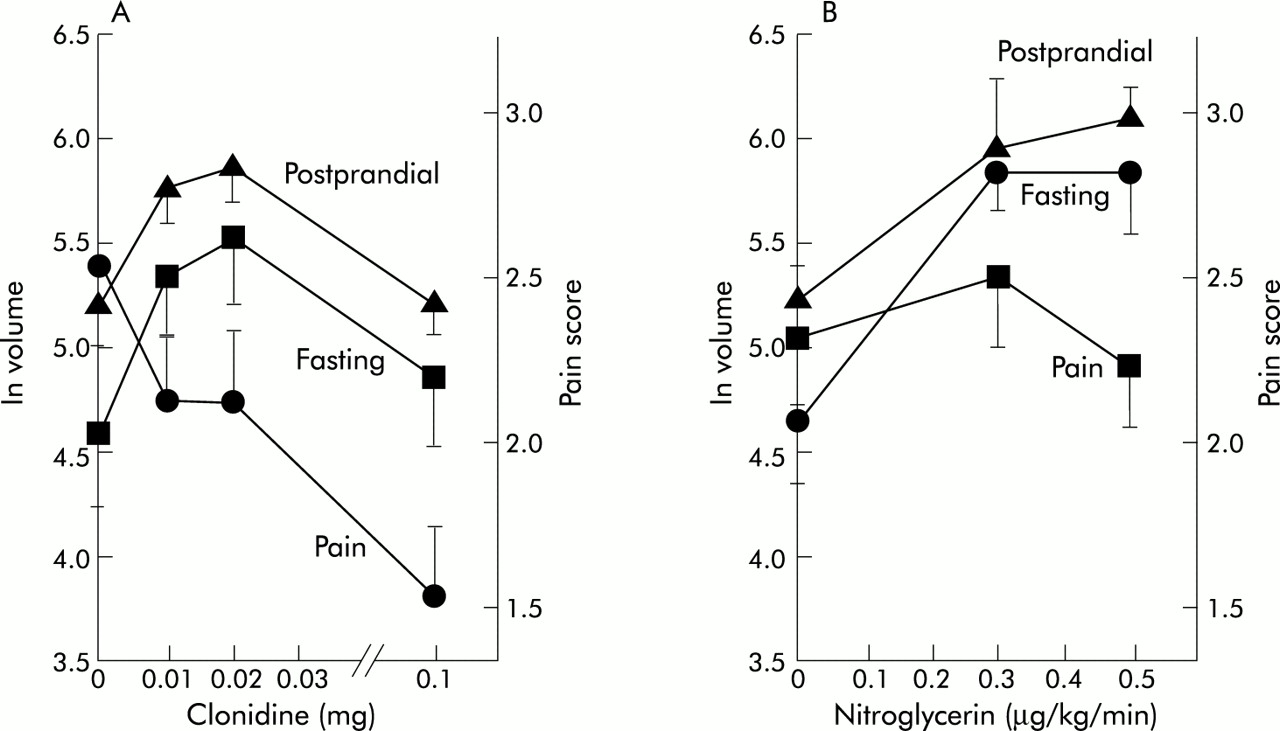
Another pitfall in the interpretation of data in the literature pertains to observations with isovolumetric stimuli. These volume based mechanical stimuli are vulnerable to misinterpretation. Thus changes in wall tension or relaxation will result in greater volumes required to achieve the threshold of sensation; volume based mechanical stimuli are vulnerable because changes in compliance or relaxation will be associated with greater volumes to achieve threshold but no such change in the pressure thresholds. In a study of IBS patients, Delvaux and colleagues48 demonstrated that alosetron was associated with increases in the perception threshold and pain threshold to volume distensions of the colon. However, there was no significant difference in pressure thresholds, suggesting an absence of an antinociceptive action of alosetron. Differences between relaxatory and antinociceptive actions were demonstrated quite convincingly in comparisons between the effects of nitroglycerin and clonidine in gastric physiology in humans.24 Both classes of medications result in relaxation of the stomach during fasting and postprandially but whereas clonidine reduced the sensation of pain in a dose dependent manner, no such effect of nitroglycerin was observed (fig 7). In fact, healthy volunteers exposed to nitroglycerin tended to have a greater sensation of bloating.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effects of clonidine (A) and nitroglycerin (B) on gastric tone and sensation. Note both agents relax the stomach but pain scores are reduced only with clonidine. Reproduced with permission from Kim and colleagues.17
Future diagnostic evaluation of visceral sensation
Currently, most of the tests involve intubation of the viscus of interest and application of mechanical stimuli such as balloon distension with monitoring of either perception scores on a VAS, threshold perceptions, or changes in cerebral blood flow. These approaches have been necessary at all levels of the gastrointestinal tract. Several groups have attempted to develop a liquid nutrient or non-nutrient load test16,49 to identify patients with hypersensitivity due to functional dyspepsia. About 50% of patients with functional dyspepsia16,49 can tolerate a lower volume prior to the development of satiety. Moreover, measurement of the volume ingested does not differentiate hypersensitivity of the afferent apparatus from changes in gastric compliance, volume, or tone.
Thus a non-invasive approach to measurement of gastric accommodation would allow further interpretation of the satiety test. The combination of volume measurements, as with the non-invasive SPECT measurement of the accommodation response,17,50 with a simple drink test and measurement of symptoms such as satiety, pain, nausea, fullness, and bloating 30 minutes after ingestion of the maximum volume of nutrient or non-nutrient liquid17,49,51 might provide a clinically applicable means to assess both accommodation and sensation responses. Symptoms associated with impairment of accommodation might be amenable to gastric relaxation therapy whereas a normal accommodation response with increased symptoms would more likely require a visceral analgesic approach. For example, a recent study with alosetron demonstrated that the accommodation volume was not altered but the aggregate symptom score and particularly nausea and bloating were reduced by alosetron.52 These data suggest that the mechanism of action is not mediated through the effect of the agent on gastric relaxation postprandially but by the actions on afferent function, possibly including chemosensitive afferents, as previously suggested by Feinle and Read.53
Nevertheless, with all sensation testing it is important to recall that psychological influences can be potential confounders in the perception and reporting of sensations54 and have to be evaluated in the interpretation of sensation data.
CONCLUSIONS
The surge of interest in the study of augmented visceral sensitivity has enhanced our understanding of several disease states. The relevance of the concept will depend on proof that symptoms are attributable to altered sensitivities and that therapies aimed at correction of hypersensitivity result in clinical benefit. Prerequisites for such correction are improved, preferably non-invasive, diagnostic tests and more thorough understanding of the transmitters or mediators involved in visceral hypersensitivity. Novel or selective approaches to target those transmitters would be feasible if the tools for measurement of the pharmacological actions of the therapies can be based on validated experimental medicine methods in health and disease.
Acknowledgments
This study was supported in part by grants RO1-DK54681-03 and K24-DK02638-03 (Dr M Camilleri) and by General Clinical Research Center grant (No RR00585) from the National Institutes of Health. I wish to thank Mrs Cindy Stanislav for excellent secretarial assistance.