Article Text

Abstract
Management strategies for reflux disease are very different from those for dyspepsia and so differentiating between patients with “true” dyspepsia and those whose primary symptom is heartburn is a key step in their management. This separation has become more clear during the last decade as insights into reflux disease and dyspepsia have improved. It is likely that the use of short self administered questionnaires in routine clinical care will improve the reliability of separation of reflux induced symptoms from true dyspepsia.
- diagnosis
- dyspepsia
- reflux disease
Statistics from Altmetric.com
SUMMARY
Management strategies for reflux disease differ substantially from those applicable to dyspepsia and so separation of these two problems is a key step in their management. This separation is less simple than has been believed in recent years, as endoscopy is an insensitive test for reflux disease, revealing clearcut oesophagitis in only approximately 40% of patients with troublesome reflux induced symptoms. Oesophageal pH monitoring also has significant limitations for diagnosis, being not only less sensitive than widely believed but also relatively expensive, uncomfortable, inconvenient, and inaccessible. Fortunately, in the majority of patients, patterns of reflux induced symptoms are distinctive for this problem. Reliable recognition of reflux induced symptoms requires insightful symptom analysis. Of special importance is the finding that the word “heartburn” is poorly understood by patients; instead, this cardinal symptom of reflux disease is recognised better if it is described in simple words. It is likely that the use of short self administered questionnaires in routine clinical care will improve the reliability of separation of reflux induced symptoms from true dyspepsia, as defined by the Rome group.
INTRODUCTION
The strong clinical logic for separation of patients with “true” dyspepsia, as currently defined by the Rome group (see articles by Agréus (see page iv2) and by Talley (see page iv72) in this supplement), from those whose primary symptom is heartburn has become more clear during the last decade as insights into reflux disease and dyspepsia have improved. Predominant heartburn was previously included within formal definitions of dyspepsia and, as a result, many practitioners continue to do this, which is unfortunate as clinical strategies are fundamentally different for heartburn and dyspepsia.
HEARTBURN AND DYSPEPSIA
The relatively high diagnostic specificity of heartburn for gastro-oesophageal reflux disease as well as its high prevalence1,2 provide the clinical logic for separating this symptom from other upper abdominal/lower retrosternal symptoms. By contrast, other upper abdominal/lower retrosternal symptom patterns grouped under the umbrella of the current definition of dyspepsia have very little, if any, diagnostic specificity for the various disorders that cause dyspepsia. Identification of heartburn patients allows them to be treated with existing effective therapies and well formulated management strategies for reflux disease, with a high expectation of success.1 As other articles in this supplement indicate, management methods for reflux disease differ substantially from those that are appropriate for the majority of dyspeptic patients, regardless of whether these management strategies use totally empirical therapy or therapy that is based on the results of endoscopy.
DEFINITIONS OF REFLUX DISEASE
Definitions and terminology are a source of confusion for gastro-oesophageal reflux disease, although less so than with dyspepsia. A recent workshop held in Genval, Belgium, defined gastro-oesophageal reflux disease as “being present in all individuals who are exposed to the risks of physical complications of gastro-oesophageal reflux, or who experience clinically significant impairment of health-related well being (quality of life) due to reflux related symptoms, after adequate reassurance of the benign nature of their symptoms”.1 This definition makes a pragmatic distinction between individuals whose reflux induced symptoms are troublesome enough to justify defining reflux as a disease, and the many individuals in the general population who experience a clinically insignificant level of reflux induced symptoms.
ENDOSCOPIC DIAGNOSIS OF REFLUX DISEASE
As with peptic ulcer disease, the major advances in the understanding and treatment of reflux disease that have occurred in the last 20 years have been enabled by the development of flexible endoscopy. Patients with clearcut endoscopic reflux oesophagitis were the first focus of research, as the endoscopic appearances of the oesophageal mucosa could be used as “hard” criteria for definition of the disease and recognition of therapeutic effects.3 Unfortunately, the criteria used for recognition and grading of reflux oesophagitis in these studies were not standardised nor formally validated for clinical relevance or observer variation. This lack of standardisation and validation hampers comparisons across clinical trials, and also detracts from the value of the routine diagnostic use of endoscopy. An international working group has been addressing this problem with the proposed,4 and now the final,5 version of the Los Angeles classification which grades endoscopic oesophagitis into four levels of severity (grades A–D) according to the radial extent of the oesophagitis. This grading of the severity of oesophagitis is determined independently of the presence of Barrett's oesophagus or other complications of oesophagitis. The working group considered the minimum criteria needed for reliable diagnosis of reflux oesophagitis and judged that minimal changes such as erythema, oedema, and friability could not be recognised reliably at present with conventional endoscopic equipment and techniques.6 The group has therefore concluded that minimal changes should not be used as indicative of reflux oesophagitis.5 As a result, the Los Angeles classification scores only the extent of oesophageal erosion or ulceration, collectively referred to as mucosal breaks.
It has long been recognised that many patients have troublesome reflux induced symptoms in the absence of endoscopic oesophagitis but it is only recently that large scale studies have been performed on this patient group.7–13 The term “endoscopy negative reflux disease” was defined at the Genval Workshop as applying to individuals who satisfy the definition of gastro-oesophageal reflux disease but who have neither Barrett's oesophagus nor definite endoscopic oesophageal mucosal breaks.1 The recent large studies have shown that such patients constitute from just over half to around two thirds of patients with reflux disease.8–10,12–14 This statistic has a very important message for the practicalities of separation of reflux disease from dyspepsia. It defines endoscopy as an insensitive test for reflux disease and emphasises the need to use other strategies to recognise this problem from among the broad group of patients presenting with upper abdominal/lower retrosternal symptoms. It should certainly not be concluded that functional dyspepsia is the diagnosis in patients who have classical heartburn and other reflux induced symptoms but a negative endoscopy. Frequently this has been the case. The diagnosis of endoscopy negative reflux disease depends primarily on symptom evaluation, sometimes with the assistance of oesophageal pH monitoring. A test of therapy is then the most logical approach to evaluate this diagnosis. These strategies are expanded on below and in other articles in this supplement.
RECOGNITION OF REFLUX INDUCED SYMPTOMS
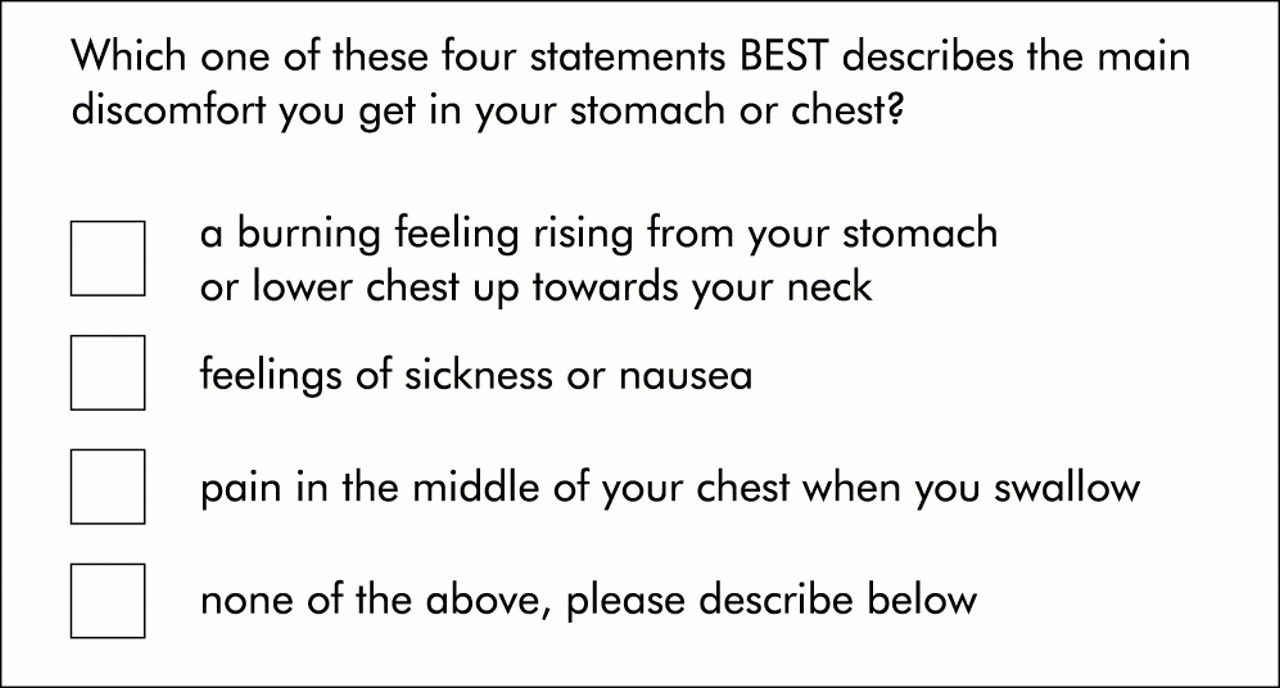
Given that a high proportion of patients with reflux disease will not be recognised by endoscopy, symptom evaluation must be the primary diagnostic method for reflux induced symptoms. Fortunately, the pattern of such symptoms is usually distinctive. As heartburn is the hallmark symptom, reliable recognition of this is of greatest importance. It has been found that patients frequently do not understand what is meant by the word “heartburn” and that physicians are not adequately aware of this.1 This communication difficulty is illustrated particularly well by a study that sought to enroll patients with functional dyspepsia.15,16 Predominant heartburn was an explicitly stated exclusion criterion, consistent with the current definition of dyspepsia. After patients had been screened by a routine clinical interview and endoscopy, 196 patients were judged to have functional dyspepsia. Of these, 188 completed a self administered questionnaire that was under evaluation for the diagnosis of reflux disease. The results of this questionnaire were used only to provide additional descriptive information about the patients enrolled. The most important question is that shown in fig 1. This description was designed to describe the sensation of heartburn without using this word. Of the 188 patients who completed this questionnaire, 42% selected the word picture of heartburn as best describing their main discomfort, despite the fact that they had not been considered to have predominant heartburn when enrolled.16 Data from oesophageal pH monitoring (see below) and omeprazole therapy, which were part of the protocol of this study, support the view that at least a substantial proportion of patients who selected the word picture for heartburn were suffering from endoscopy negative gastro-oesophageal reflux disease.
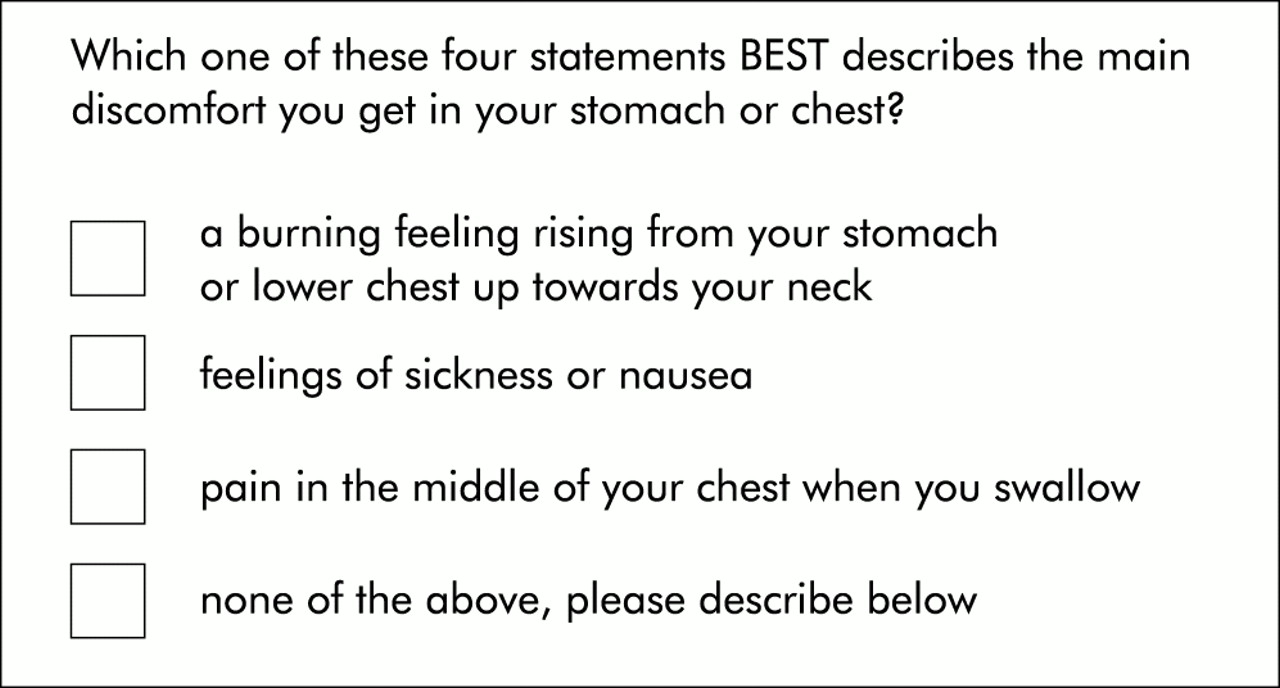
Question designed to determine whether heartburn was a predominant symptom (patients were instructed to tick only one box).
There is demonstrated benefit for symptom screening to go beyond reliable recognition of heartburn, as other aspects of the symptom patterning of reflux disease are also quite distinctive. The clustering of symptoms during the postprandial period and their prompt relief by antacids appear to be the most useful additional positive diagnostic criteria.16,17
Studies of screening for reflux induced symptoms indicate that this poses practical difficulties, even for clinicians who have a special interest in gastroenterology. Because of these difficulties, a validated formally structured but simple questionnaire designed for completion by the patient, and which derives an overall diagnostic score, is an attractive approach. Such a questionnaire could provide a reproducible expert structure for symptom evaluation. Assessments of two diagnostic questionnaires of this type support their utility,16,17 and other studies are underway to further validate and refine a questionnaire suitable for routine clinical practice which evaluates both the diagnosis and severity of symptoms. The word “predominant” is an important qualifier to keep in mind when symptoms are being evaluated as it ensures attention is focused on the symptom that is the primary concern of the patient. Given that mild heartburn occurs at some time within three months in a substantial minority of the general population,2 this symptom would be expected to occur just by chance alone in many patients whose symptoms arise primarily from another problem, including functional dyspepsia. The reverse is also likely to be true—that is, a proportion of patients whose primary problem is reflux disease will also have functional dyspepsia, given the high prevalence of this problem.
IMPORTANT TECHNICAL CONSIDERATIONS FOR OESOPHAGEAL PH MONITORING
Twenty four hour oesophageal pH monitoring is a useful technique for assessing “problem” patients but it is impractical and unnecessary as a mainstream diagnostic approach.1 This type of testing is resource consumptive, and somewhat uncomfortable and inconvenient for patients. It is also not usually widely available. The diagnostic sensitivity and specificity of oesophageal pH monitoring as routinely performed are also considerably less than is widely believed for endoscopy negative patients.1,18–21 In this setting, the major aim is to determine, in an individual patient, whether symptoms are caused by gastro-oesophageal reflux. The usual approach is to rely on the 24 hour oesophageal acid exposure value, expressed as the percentage of time that oesophageal pH is less than 4. The difficulty with this approach is that the amount of acid reflux that occurs in patients with endoscopy negative reflux disease is, on average, less than that in patients who have clearcut reflux oesophagitis.1,18,19 Because of this, 24 hour acid exposure values are within the normal range in a substantial minority of patients with definite reflux disease, and in others the acid exposure values are in the grey zone between normal and abnormal.1,18,19,21 When oesophageal pH monitoring is performed twice in endoscopy negative patients, the diagnosis of normal/abnormal acid exposure will change in approximately one third of patients, dependent on the cut off level set between normal and abnormal acid exposure values.18,19
Measurement of acid exposure values only tests indirectly whether a troublesome symptom is reflux induced. Oesophageal pH monitoring allows a direct evaluation of the association of symptoms with individual reflux episodes by having the patient signal the occurrence of symptoms with the pH monitor symptom event marker. This more sophisticated use of oesophageal pH monitoring substantially improves sensitivity and specificity21 but it is technically demanding for the patient and doctor and so tends to be used relatively infrequently.1
The practical limitations of oesophageal pH monitoring for recognition of patients with reflux disease reinforce the importance of extracting the maximum diagnostic value from assessment of symptom patterns. The limitations of oesophageal pH monitoring also make a test of therapy an attractive option after symptom assessment, with oesophageal pH monitoring being reserved for “problem” patients.1
INSIGHTS FROM OESOPHAGEAL PH MONITORING IN DYSPEPSIA
There has been little critical evaluation of what can be learnt from the use of oesophageal pH monitoring in patients who are considered to have dyspepsia, and in whom no explanatory endoscopic abnormality has been found. Given that the clinical use of oesophageal pH monitoring is for the diagnosis of reflux disease, this method of testing should give an estimate of the proportion of patients with reflux disease misclassified as having functional dyspepsia. When oesophageal pH monitoring is used in this way, the results should be interpreted critically, taking into account information given earlier in this review indicating that oesophageal pH monitoring falls far short of being a diagnostic gold standard for reflux disease.
Twenty four hour oesophageal pH monitoring was performed in 128 of 196 patients considered to have functional dyspepsia (data on file, AstraZeneca, Mölndal, Sweden) in the study by Lauritsen and colleagues,15 also described by Carlsson and colleagues,16 and referred to previously above. These data are shown in fig 2 according to the subsequent symptom evaluation by questionnaire. Of the patients with predominant heartburn, the proportions with definite, probable, and normal oesophageal acid exposure were almost identical to those found in the large study of endoscopy negative reflux disease by Lind and colleagues (fig 3).11 Interestingly, even in patients confirmed to have true dyspepsia according to the Rome definition (see articles by Agréus [see page iv2] and by Talley [see page ix72] in this supplement), definite and possibly abnormal levels of acid exposure18,19,21 were seen in a substantial minority (fig 3). Unfortunately, the pH monitor symptom event marker was not used in this study and therefore there are no data on the association of symptom episodes with individual reflux episodes.

Twenty four hour oesophageal acid exposure data for 123 patients from the study by Lauritsen and colleagues,15 from whom pH data were available (data on file, AstraZeneca, Mölndal, Sweden).

Twenty four hour oesophageal acid exposure data for 451 patients who had troublesome heartburn but no oesophageal mucosal breaks.11
The study by Small et al evaluated patients with 24 hour oesophageal pH monitoring.22 Although this is presented as a study on functional dyspepsia, endoscopy negative patients with predominant heartburn were included, being referred to confusingly as patients with “reflux-like dyspepsia”. These patients are redefined for the purposes of this article as heartburn patients. It needs to be appreciated that a substantial minority of the patients enrolled in this study did not meet the current Rome criteria for functional dyspepsia. Table 1 shows data on oesophageal acid exposure for the entire patient group, underlining the importance of reflux disease in patients with no clearcut endoscopic abnormality and upper abdominal/lower retrosternal symptoms. Of special interest is the symptom event marker evaluation of the association of symptoms with reflux episodes reported for patients in whom acid exposure was within normal limits.22 The 80 patients in this category were divided into those with severe or moderate heartburn (n=44) and those with mild or no heartburn (n=36). Figure 4 shows that a substantial minority of the patients with prominent, if not predominant, heartburn had high rates of association of symptoms with reflux episodes, despite their normal acid exposure values.
Data on 100 patients from the study of Small and colleagues.22 Those with abnormal acid exposure were classified as having reflux disease, regardless of their symptom pattern

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Graphical presentation of data on the association of individual symptom episodes with acid reflux events for patients who had normal levels of oesophageal acid exposure.22 Patients were subdivided according to whether they had moderate or severe heartburn, or mild or no heartburn. A substantial minority of patients with predominant heartburn had a relatively high level of association of symptoms with reflux.
THE PLACE OF OESOPHAGEAL PH MONITORING IN THE ROUTINE CLINICAL MANAGEMENT OF DYSPEPSIA
Oesophageal pH monitoring has provided useful insights into the contribution of reflux disease to symptoms in patients diagnosed as having functional dyspepsia. These insights however do not justify the routine use of oesophageal pH monitoring in this patient group. Instead the outcomes of these studies emphasise the need for a carefully structured screening of endoscopy negative patients for their predominant symptom pattern. If this is heartburn, then the next step should be a trial of therapy based on the diagnosis of endoscopy negative reflux disease. Oesophageal pH monitoring should be reserved for particularly difficult cases after a trial of therapy.
REFERENCES
Footnotes
-
Conflict of interest: This symposium was sponsored by AstraZeneca, makers of omeprazole. The author of this paper has received sponsorship for travel and an honorarium from AstraZeneca.