Article Text

Abstract
Background and aims: The incidence of gastric cancer in Japan is four times higher than in the UK. It usually arises in a stomach with corpus predominant or pangastritis that has undergone extensive atrophy and intestinal metaplasia. We hypothesised that a Japanese population would have a more severe gastritis with a corpus predominant or pangastritis pattern and a greater degree of atrophy and intestinal metaplasia than that found in the UK. To test this we designed a comparative trial.
Methods: A total of 252 age matched consecutive patients were recruited from the endoscopy services in Leeds and Tokyo. In each centre, 21 patients were prospectively selected from each decennial, between the ages of 20–80 years. All had epigastric discomfort as their predominant symptom. Patients with peptic ulcer, cancer, and oesophagitis were excluded. Five gastric biopsies were examined by two histopathologists using the updated Sydney system. Helicobacter pylori infection was assessed by histology and culture of biopsies and enzyme linked immunosorbent assay and immunoblot of plasma.
Results: Gastritis was found by both pathologists in 59 (47%) UK and 76 (60%) Japanese patients (χ2 test, p = 0.04). In those patients with gastritis, corpus predominant or pangastritis was commoner in the Japanese (63% Japan v 36% in the UK (χ2 test, p = 0.003) Atrophy and intestinal metaplasia were more extensive and severe (Mann-Whitney U test, p<0.001) and chronic inflammation and polymorph activity were also greater, especially in the corpus (Mann-Whitney U test, p<0.001). Fifty three of 59 UK gastritis patients (90%) and 67/76 (88%) (χ2 test, p = 1) Japanese gastritis patients were positive for H pylori. Using a previously described “gastric cancer risk index” among H pylori positive patients, there were significantly more Japanese than UK subjects with a “high risk” score.
Conclusion: In Japanese as opposed to English patients, gastritis is more prevalent and severe with more corpus predominant atrophy and intestinal metaplasia. These differences may partially explain the higher incidence of gastric cancer in Japan.
- IM, intestinal metaplasia
- IQR, interquartile range
- IL, interleukin
- TNF-α, tumour necrosis factor α
- gastritis
- Helicobacter pylori
- population comparison
- gastric cancer risk
Statistics from Altmetric.com
The incidence of gastric cancer varies throughout the world. It is four times more common in Japan than in the UK and occurs at a younger age.1 A variety of aetiological factors have been put forward to account for these differences, including Helicobacter pylori prevalence2 and virulence3as well as dietary4 and genetic5 variations between different populations.
The Correa hypothesis postulates a progression from chronic gastritis to gastric atrophy and intestinal metaplasia (IM), leading to dysplasia and finally cancer.6 Histologically, gastric cancer is classified as either “intestinal” or “diffuse”. Intestinal cancer is commoner and is associated with atrophy and IM while diffuse cancer tends to arise in areas of active inflammation. Both are strongly associated with H pylori infection. The severity and histological appearances of the gastritis are therefore relevant but the pattern of the gastritis seems to be even more important. Patients with a corpus predominant or pangastritis (gastritis affecting the corpus more than the antrum or affecting both equally) have a much higher cancer risk than those with an antral predominant gastritis.7 Corpus gastritis that is associated with loss of parietal cell mass (atrophy) and hypo- or achlorhydria allows faecal-type bacterial species to colonise the stomach and it is thought that these organisms may convert ingested nitrate to nitrite and then to carcinogenic N nitroso compounds.6
It is unclear which factors are responsible for the increased risk of cancer in Japan compared with the UK but it would seem a reasonable hypothesis that whatever the underlying cause the Japanese population should have a more severe gastritis, occurring at an earlier age, and with a corpus, rather than an antral, predominant pattern. Therefore, the aim of this study was to evaluate the pattern and severity of gastritis in patients complaining of dyspepsia in the UK and Japan, matched for age.
PATIENTS AND METHODS
This was a cross sectional comparative study carried out at the General Infirmary at Leeds and the National Cancer Centre Hospital, Tokyo. Three endoscopists (T Gotoda in Tokyo and L Gatta and G Naylor in Leeds) spent two months training together ensuring concordance of patient selection, recruitment and biopsy sites, processing of histological and microbiological specimens, blood sampling, and storage.
Ethics approval for the study was obtained from the local ethics committees. In Leeds, patients were recruited from a “one stop” dyspepsia clinic. Patients gave written consent on the day if they agreed to enter the trial. In Tokyo, patients attending the National Cancer Centre Hospital endoscopy department specifically for investigation of dyspepsia were similarly approached.
In order to calculate sample size, we identified existing data on gastritis for the UK and Japan. Results from a previous Japanese biopsy study8 had shown normal findings (that is, no evidence of gastritis) in 9.5% of an asymptomatic population aged 20–60+ years. Unpublished data from a Leeds population showed 50.5% of patients in a routine endoscopy series to have normal stomachs. No asymptomatic Western population data existed but as previous studies9,10 have demonstrated a lack of correlation between symptoms and histological findings in patients with gastritis, we concluded that this comparison was valid for the purpose of our power calculation. This gave a prevalence of 90.5% and 49.5% for gastritis (of any type) for Japan and Leeds, respectively. Therefore, to detect a difference of 41% in prevalence between the Japanese and English patients with a power of 0.80 and a significance level of 0.05 (alpha two sided), at least 126 patients had to be enrolled from each centre. Twenty one patients from each decennial from 20 to 80 years were therefore recruited from Leeds and Tokyo between May 2000 and April 2002. Inclusion criteria were as follows: age 20–80 years, predominant symptom of epigastric pain and no endoscopic evidence of reflux oesophagitis, peptic ulcer disease, or malignancy (“non ulcer dyspepsia”). Patients were excluded if they had received H pylori eradication therapy in the past or any non-steroidal anti-inflammatory drugs, proton pump inhibitors, antibiotics, or bismuth containing compounds in the previous two weeks or H2 receptor antagonists in the previous two days. At endoscopy, five gastric mucosal biopsies were taken as detailed below. Further antral and body biopsies were taken for H pylori culture. Blood was also taken for H pylori serology.
Histology
Biopsy samples were taken using standard endoscopy biopsy forceps from the five sites specified in the updated Sydney system (fig 1⇓).11
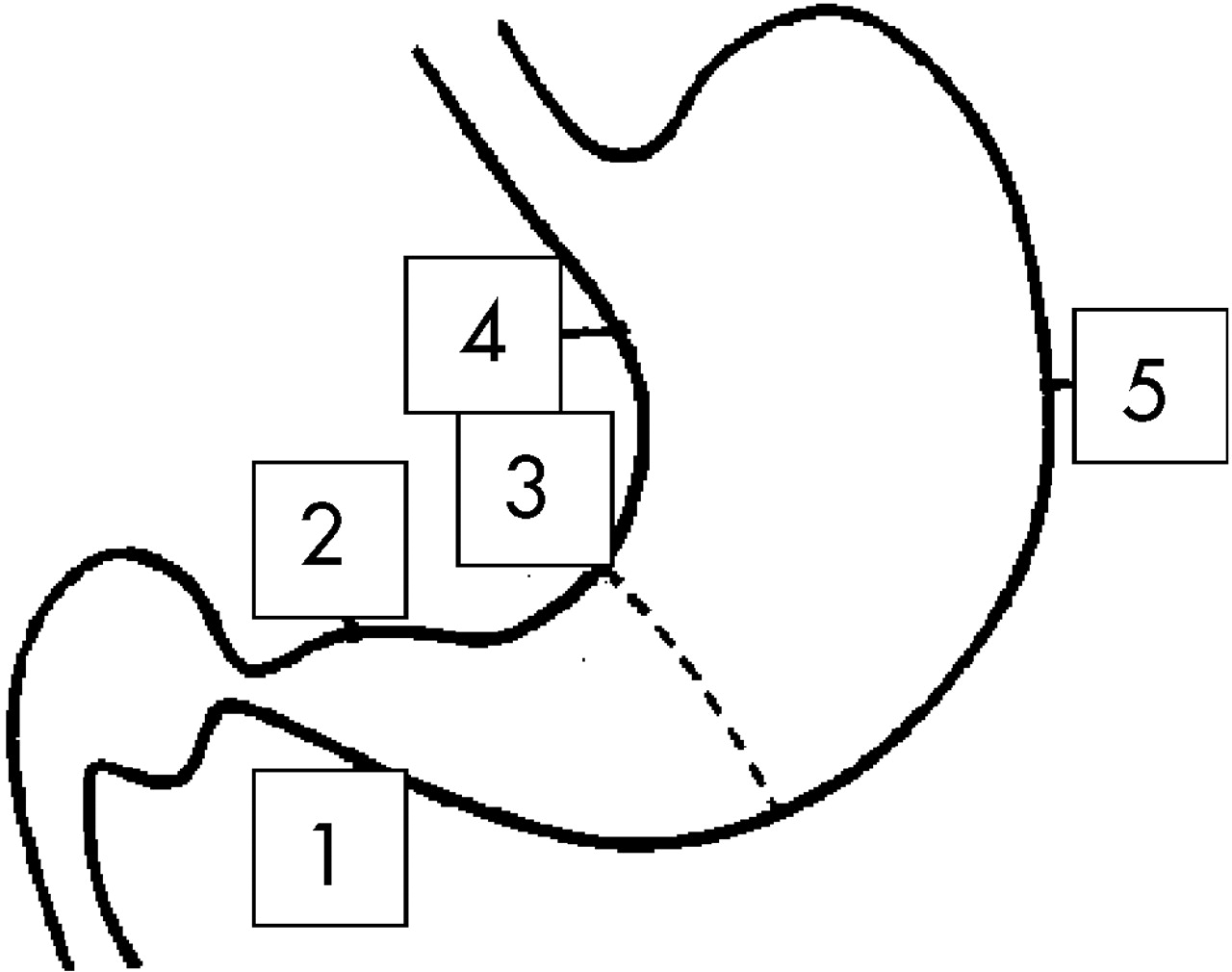
Biopsy sites for the Sydney system: 1, 2 = antrum (approximately 2 cm from the pylorus), 3 = incisura (centre), 4 = lesser curve (mid way between the incisura and cardia), and 5 = greater curve (central, opposite 4).
Samples were placed in 10% formalin and then embedded in paraffin for sectioning. Three sets of slides were made in each centre; one set was stained with haematoxylin and eosin. These were then assessed by the histopathologist in each centre (Professor M Dixon (MD) in Leeds and Professor T Shimoda (TS) in Tokyo). A second set was sent unstained to the other centre where haematoxylin-eosin staining took place and the slides were assessed. The pathologists were blinded as to the age and sex of the subjects but because of differences in laboratory identification of the slides, they were aware of their origin. The graded features were scored as absent, mild, moderate, or severe (0–3) according to the updated Sydney system for polymorph activity, chronic inflammation, IM, and atrophy. Thus two sets of histological data were produced on all of the material from Leeds and Tokyo, one from a Japanese pathologist and one from a “Western” pathologist. In addition, two further sets of slides (one each from Leeds and Tokyo) were stained in Leeds by a modified Giemsa for detection of H pylori (MD). Patients were considered positive for histological gastritis (consensus gastritis) only if it was diagnosed by both pathologists.
Helicobacter pylori
Three methods were used to detect H pylori: histology, culture, and antibody testing. Antral and body biopsy samples were placed immediately into culture medium and then frozen to −70°C. They were cultured on 10% (vol/vol) blood agar at 37°C in variable atmosphere incubators under microaerobic conditions in the separate centres. Cultures (Tokyo) or biopsies (Leeds) where then transported to a single centre (London) to be typed for CagA status and VacA genotype.
Two serological tests were performed on samples from all patients. Firstly, an enzyme linked immunosorbent assay of IgG antibodies against H pylori (HM-CAP; Enteric Products Inc., Westbury, New York, USA) with a value of 1.8 taken as positive (sensitivity 98.7%, specificity 100%). Secondly, an immunoblot kit assay that included VacA and CagA antibody testing as well as diagnosing infection (Helocoblot 2.1; Genelabs Diagnostics, Singapore) (sensitivity 96%, specificity 95%).
Statistical analysis
Demographic data and pattern of gastritis were compared using Pearson’s χ2 test. The Sydney system approach generates four sets of categorical data each, with four possible grades for the five biopsies from individual patients. Statistical analysis of the gastritis data was restricted to those patients in whom both pathologists had agreed the presence of gastritis (consensus gastritis). In order to carry out the statistical comparisons, we converted the grades to numerical values (0–3) and used medians and non-parametric testing, namely the Mann-Whitney U test. Interobserver agreement between the two pathologists was examined using kappa statistics, a chance corrected coefficient of agreement. Differences between proportions and their 95% confidence interval (CI) were calculated using the method recommended by Newcombe and Altman.12 Values of p<0.05 were considered significant. These criteria were determined before commencement of the study. Standard statistical packages were used for the analyses (SPSS version 10.1 (SPSS Science, Chicago, Illinois, USA) and Statsdirect (Statsdirect, Cheshire, UK)).
RESULTS
Demographics
Sex, age, and smoking characteristics of the two patient groups are illustrated in table 1⇓. There was no significant difference in age between the two groups. However, the prevalence of female patients was higher in the Japanese (64.3% (95% CI 55.6–72.1)) than in the UK groups (50% (95% CI 41.4–58.6)), with a difference in prevalence equal to 14.3% (95% CI 2.1–25.9).
Summary of sex and smoking characteristics
Prevalence of gastritis
There was consensus agreement between the two pathologists that 76 (60.3% (95% CI 51.6–68.4)) Japanese and 59 (47.6% (95% CI 39.1–56.3)) UK patients had gastritis, with a difference in prevalence equal to 12.7% (95% CI 0.04–24.5; p = 0.0432). Demographic details for these patients are shown in table 1⇑ and details of the consensus diagnosis per decennial in table 2⇓.
Number of patients in each decennial in whom a consensus diagnosis of gastritis was made by both pathologists
Interobserver agreement between the pathologists
Sydney system scores were compared. Mean kappa coefficients varied from 0.376 to 0.632 (table 3⇓). Agreement was poorest for atrophy and greatest for chronic inflammation. Landis and Koch13 suggest that kappa values >0.20 represent “fair” and >0.40 “moderate” agreement. A previous assessment of interobserver variation in the assessment of gastritis,14 using a comparable scoring system, found kappa scores of 0.1–0.29 for atrophy.
Kappa coefficients of agreement for all patients’ biopsies (Sydney system histology results from a UK and Japanese histopathologist)
Severity of gastritis
Total median scores from all five biopsies were compared between the two patient groups for atrophy, IM, activity, and chronic inflammation in subjects with gastritis. The Japanese median atrophy score was 9 compared with 2 in the UK (median difference 6 (95% CI 5–8); Mann-Whitney U test, p<0.001). Median scores for IM were 1.5 for Japan and 0 for the UK (median difference 0 (95% CI 0–3); Mann-Whitney U test, p<0.01). Median scores for polymorph activity were 8 for Japan and 4 for UK (median difference 4 (95% CI 2–5); Mann-Whitney U test, p<0.001). Median scores for chronic inflammation were 13 for Japan and 9 for the UK (median difference 4 (95% CI 2–5); Mann-Whitney U test, p<0.001). Medians for each decennial are illustrated in fig 2⇓. It can be seen that for each parameter there was a trend to a greater degree of pathological change in each of the age decennials, except for IM in the 20s and 30s where they were the same.

(A–D) Median histology scores for consensus gastritis patients, cumulative scores for all five biopsies. (A) Intestinal metaplasia (IM), (B) atrophy, (C) polymorph activity, and (D) chronic inflammation. (A) Median overall IM scores 1.5 versus 0 (p<0.01). (B) Median overall atropy scores 9 versus 2 (p<0.001). (C) Median overall activity scores 8 versus 1 (p<0.001). (B) Median overall chronic inflammation scores 13 versus 9 (p<0.001).
Pattern of gastritis
Cumulative scores for each patient with gastritis were analysed to assess the pattern of inflammation (antral predominant or corpus/pangastritis). The updated Sydney system11 suggests that chronic inflammation (mononuclear cell infiltration) should be used as the principal tool to assess pattern. The reasoning is that this represents the “degree” of gastritis and also does not have the sampling errors that atrophy and IM are prone to.
Therefore, scores from both pathologists for chronic inflammation were added together for biopsies 1 and 2 (antrum) and compared with the equivalent scores from biopsies 4 and 5 (corpus). If the cumulative scores were 2 or more points greater in the antrum biopsies compared with the corpus biopsies, gastritis was classified as “antral predominant”; if they were 2 or more points greater in the corpus it was classified as “corpus predominant”; or if they were within one point of each other as “pangastritis”.
Sixty three per cent of Japanese patients with gastritis had a corpus predominant or pangastritis compared with 36% in the UK (χ2 test, p = 0.003) (fig 3⇓, table 4⇓).
Pattern of gastritis in UK and Japanese patients

Patterns of gastritis in UK and Japanese patients.
Differences in the nature and severity of gastritis in the antrum and corpus of those patients with consensus gastritis in the two populations were further explored by comparing the cumulative scores for each of the parameters of the updated Sydney system (chronic inflammation, polymorph activity, atrophy, and IM) given by both pathologists for biopsies 1 and 2 (antrum) and biopsies 4 and 5 (corpus). The results are shown in fig 4⇓. Comparisons for each decennial are shown with patients grouped into <50 and >50 for statistical comparison. Chronic inflammation and activity scores were comparable in the antrum but markedly lower in the corpus of the UK patients. This largely explains the greater prevalence of antrum predominant gastritis in UK subjects; Japanese subjects had the same, or even higher, scores for chronic inflammation in the antrum but in general had far more corpus chronic inflammation. The degree of corpus atrophy was more marked in the Japanese patients, especially in the older age groups.

(A–H) Total median scores for atrophy (A, B), intestinal metaplasia (IM) (C, D), polymorph activity (E, F), and chronic inflammation (CI) (G, H) in the antrum (biopsies 1 and 2) and corpus (biopsies 4 and 5). (A) Antral atrophy: median difference age <50 years = 2 (p<0.0001); median difference age >50 years = 3 (p<0.0001). (B) Corpus atrophy: median difference age <50 years = 0 (p = 1); median difference age >50 years = 3 (p<0.0001). (C) Antral intestinal metaplasia: median difference age <50 years = 0 (p = 0.6); median difference age >50 years = 0 (p<0.017). (D) Corpus intestinal metaplasia: median difference age <50 years = 0 (p = 1); median difference age >50 years = 0 (p = 0.01). (E) Antral activity: median difference age <50 years = 1 (p = 0.013); median difference age >50 years = 1 (p = 0.03). (F) Corpus activity: median difference age <50 years = 2 (p = 0.0007); median difference age >50 years = 2 (p<0.0001). (G) Antral chronic inflammation: median difference age <50 years = 2 (p = 0.03); median difference age >50 years = 0 (p = 0.2). (H) Corpus chronic inflammation: median difference age <50 years = 3 (p = 0.001); median difference age >50 years = 3 (p<0.0001). p values for Mann-Whitney U testing.
H pylori associated gastritis
Gastritis patients were assessed for H pylori infection (table 5⇓). Forty six of 59 (78%) UK patients had histological or microbiological (culture) evidence of H pylori infection compared with 54 of 76 (71%) Japanese patients (χ2 test, p = 0.6). However, these values do not include those in whom H pylori may have originally caused inflammation but had subsequently disappeared. If serological evidence is taken into account, 53 of 59 (90%) UK patients and 67 of 76 (88%) of Japanese patients may have been infected at some time (χ2 test, p = 1). Alternatively, if the diagnosis of H pylori infection is taken to require two positive tests, there were 51 (85%) UK and 56 (74%) (χ2 test, p = 0.5) Japanese positives (table 5⇓).
Patients with consensus gastritis: evidence of Helicobacter pylori infection
H pylori negative gastritis
Seventeen gastritis patients (six UK, 11 Japanese) were negative for all modalities of H pylori testing (tables 6⇓, 7⇓). Thirteen of these (four UK, and nine Japanese, all <50 years old) had low levels of gastritis of uncertain significance (median total histology score 3 (interquartile range (IQR) 3–5). Four patients (two UK, two Japanese, all over 50 years) had more marked gastritis (median total histology score 11.5 (IQR 10–15.5)). In these H pylori negative cases, activity scores were low and in general histological changes were more marked in the antrum. However, some of the older patients did have evidence of atrophy and IM in the corpus and it is possible that in these cases both the organism and antibody response had disappeared. Alternative aetiologies such as “chemical” (reactive) or autoimmune gastritis are possible but recent non-steroidal usage was an exclusion criterion and none of the patients had the typical histological appearances of autoimmune gastritis (however, this is known to be very rare in Japan).
Histology scores for the 11 Japanese patients with consensus gastritis who were negative for all forms of Helicobacter pylori testing
Histology scores for the six UK patients with consensus gastritis who were negative for all forms of Helicobacter pylori testing
H pylori pathogenicity
CagA status was assessed using an immunoblot assay. Forty seven (37%, mean age 54 years) UK and 72 (57%, mean age 56 years; χ2 test, p = 0.003) Japanese samples were positive for the 116 kDa protein that corresponds to the presence of the CagA antibody. Histology of the CagA positive patients was compared. There were similar antral activity and chronic inflammation scores in the two populations but greater corpus atrophy, chronic inflammation, and polymorph activity in the Japanese population (fig 5⇓, table 8⇓). The proportions of corpus predominant/pangastritis and antral predominant in CagA positive cases were similar to those found in all cases of gastritis (antral predominant 49% Japan, 67% UK; p = 0.06).
Comparison of histology of cagA positive patients

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of histology of CagA positive patients. CI, chronic inflammation; IM, intestinal metaplasia.
We were able to culture and subtype 53/56 (94%) Japanese H pylori positive patients and 29/51 (57%) UK patients. All 53 Japanese patients were VacA subtype s1m1. Fifty two of 53 Japanese patients were CagA positive although one patient had CagA positive antral and CagA negative body cultures. Eleven of 29 UK patients had VacA s1m1 subtype, 13 were s1m2, and five were s2m2. Overall 26/29 were CagA positive.
Histological differences remained when 52 Japanese and 10 UK patients who were CagA positive and VacA s1m1 on antral biopsy culture were compared. It is apparent that the differences seen for all H pylori gastritis patients are maintained when like is compared with like. Cag and Vac pathogenicity of H pylori does not appear to be the decisive factor explaining the differences in gastritis between the two populations.
Gastric cancer risk scores for H pylori positive patients
In order to further explore the histological data, we used a previously validated gastric cancer risk score, as described by Meining and colleagues.15 They compared gastritis in patients with small early gastric cancers with histologically proven H pylori infection with a control group of H pylori positive duodenal ulcer patients who had a low risk of gastric cancer. Their scoring system was calculated as follows:
Infiltration with chronic inflammatory cells is more pronounced in the corpus mucosa than in the antrum, or is equally distributed = 1 point.
Infiltration with neutrophils ( = “activity” in the Sydney system) is more pronounced in the corpus mucosa than in the antrum, or is equally distributed = 1 point.
Presence of IM in the antrum or corpus = 1 point.
In Meining’s study, the predictive value for the presence of gastric carcinoma was 0.166 for 0 points, 0.464 for 1 point, 0.791 for 2 points, and 0.943 for 3 points.
Histology results of the 45 UK patients and 54 Japanese patients who had histological evidence of H pylori infection were analysed (in keeping with the original study).
The sum of the chronic inflammatory scores for both pathologists for biopsies 1 and 2 (antrum) were compared with the scores for biopsy 4 and 5 (corpus). The same approach was used for activity in the corpus and antrum. Finally, IM in the antrum or corpus reported by either pathologist was noted. Again the results for both pathologists were added together and this value used to establish the cancer risk score.
Comparing the cumulative scores (table 9⇓), there were significantly more Japanese patients with a score of 3, and conversely more UK patients with a score of 0. The proportion of patients with intermediate scores of 1 and 2 were similar in both patient groups.
Comparison of cancer risk scores
DISCUSSION
We believe this to be the first study to prospectively compare the histology of two matched populations from countries with substantially different gastric cancer rates. The selection process excluded patients with macroscopic pathology such as cancer, peptic ulcer, and reflux oesophagitis. Only those with symptoms of “functional” dyspepsia were assessed and the protocol ensured similar age cohorts.
The major weakness of the study is that dyspeptic symptoms were not identical because of differences in culture, language, and health seeking behaviour in the two countries. However, strict adherence to inclusion and exclusion criteria should have minimised this effect; in particular we ensured that the National Cancer Centre patients were attending for investigation of simple dyspepsia and not for possible malignancy. It also proved impossible to “blind” the two pathologists with respect to the source of the material they were examining. The kappa statistics were generally good with the sole exception of antral atrophy in young patients; however, antral atrophy has previously been recognised as a difficult feature to assess.16 A further weakness of the study was that we were unable directly to compare social class between the two countries because a system of social assessment does not exist in Japan. Nor was it considered possible to obtain an accurate dietary history from the Japanese patients.
The cause of the gastritis was predominantly H pylori infection. Other aetiologies are unlikely because of the histological findings, and patients on recent non-steroidal anti-inflammatory drugs were excluded. No patient had the characteristic histological appearance of autoimmune gastritis (a condition that is very rare in Japan anyway) but parietal cell antibodies were not checked.
As this was a cross sectional analysis we must remember that the age of infection with H pylori (assumed to be in childhood) is not known. The rate at which patients were infected and at what age would be important factors in determining the future histological changes.
The difference in prevalence (12.5%) of gastritis between the two groups was lower than anticipated and this reflected the unexpected similarity in H pylori infection rates. This finding is commensurate with the falling rate of infection in the Japanese population. Our results show that gastritis in Japan is histologically more severe, is present at an earlier age, and is more likely to be corpus predominant or pangastritis. Three possible explanations may account for the differences between the two populations: the genetic constitution of the host, the genotype of the infecting organism, and the environment.
Severity of inflammation
Cytokine production is largely responsible for the host’s inflammatory response to H pylori infection and is genetically determined. Interleukin (IL) 1β and tumour necrosis factor α (TNF-α) are proinflammatory cytokines that also inhibit acid production. Polymorphisms of the genes controlling production of these cytokines have been linked to different levels of IL-1β and TNF-α production and have been associated with an increased risk of gastric cancer, chronic atrophic gastritis, IM, and gastric ulcer.5,17–,19
Bacterial factors are also important. Possession of the Cag associated pathogenicity island leads to production of the CagA protein20 and is associated with an increased severity of gastritis and incidence of peptic ulcer disease and gastric cancer.21–,24 Production of the vacuolating toxin VacA, and the genotype of the VacA gene, are also associated with increased pathogenicity.25
Another environmental factor likely to play a role in the severity of gastritis is diet. Diet has long been postulated as an aetiological factor for non-cardia gastric cancer, with nitrate and salt intake both being implicated,1,2,26 while antioxidants such as vitamins A, C, and E may be protective.27 The Japanese diet is higher in salt than a standard Western diet and animal models show that a high salt diet causes an acute gastritis.28
Pattern of gastritis
The pattern of colonisation of the gastric mucosa by H pylori appears to be controlled by acid secretion. Although H pylori is much more tolerant of a low pH than most bacteria, it cannot proliferate in areas of high acid production. A low acid output allows spread of inflammation to the gastric corpus resulting in a further decrease in acid production.29 Acid secretion is directly related to height and weight which determine lean body mass.30
Maximal acid secretion varies widely between individuals and it is likely that patients with a constitutionally lower acid secretion are more likely to develop a corpus predominant or pangastritis. Might different levels of acid production explain the different pattern of gastritis in the two populations? Japanese subjects may have a smaller parietal cell mass but direct comparisons of acid secretion have not been performed. Evidence for lower acid output in patients from the Far East was found in a comparison between a Chinese and Scottish population (both normal and duodenal ulcer subjects). Acid output was higher in the Scottish normal and duodenal ulcer patients and the difference was maintained when the results were corrected for weight.31 The latter study pre-dates the discovery of H pylori so the relative infection rates are unknown. However, the data suggest that variation in the level of acid production in different populations may account for our findings.
Atrophy, intestinal metaplasia, and the role of H pylori
In Japanese patients, atrophy was more severe than in UK patients. The differences were greatest in the corpus of the middle to older age groups. Intestinal metaplasia was more marked in the older Japanese patients. Even when gastritis was caused by similar pathogenic strains (with regard to CagA and VacA), the differences were maintained but there are other virulence factors for which we have not controlled.
More atrophy was seen in the older Japanese who were H pylori histology negative while almost none was seen in their UK counterparts. Serology results suggest that the older Japanese patients with atrophy/IM but no histological evidence of H pylori may have been infected with CagA organisms in the past but had cleared their infection leaving its after effects, as has been described elsewhere.32
Cancer risk
As corpus atrophy and IM are key steps in Correa’s gastritis-metaplasia-dysplasia-carcinoma sequence,5 differences between the two populations show Japanese gastritis to have a “premalignant” pattern in keeping with their increased cancer risk. The carcinogenic factor or factors that tip the balance towards dysplasia and carcinoma are not completely understood but in the hypochlorhydric or achlorhydric stomach faecal-type bacteria proliferate and carcinogenic n-nitroso compounds may be generated by bacterial metabolism of either dietary nitrate or nitrite derived from endogenously converted nitrate.5,33
The pattern of H pylori gastritis in the Japanese was mainly corpus predominant or pangastritis. Conversely, UK patients had an antral predominant pattern that would tend to maintain, or even increase, acid production from the parietal cells of the corpus. The importance of IM and a corpus predominant pattern of chronic inflammation and polymorph activity in determining cancer risk has been demonstrated within a German population.15 We have applied the same scoring system making this the first study to show that such factors apply in two populations with widely different gastric cancer rates.
Summary
This study confirms that in age and symptom matched patients, Japanese subjects do develop a more severe and more corpus predominant gastritis than their UK counterparts. This may account for the increased gastric cancer risk in Japan.
REFERENCES
Footnotes
Published online first 7 April 2006
This research was supported by Astra-Zeneca Pharmaceuticals, the Leeds Infirmary Pathology Department Research Fund, and the Daiwa foundation.
Conflict of interest: None declared.