Article Text

Abstract
Background and aims: C-reactive protein (CRP) levels are often used in the follow-up of patients with inflammatory bowel disease (IBD). The aims of this study were to establish the relationship of CRP levels to disease extent in patients with ulcerative colitis and to phenotype in patients with Crohn’s disease, and to investigate the predictive value of CRP levels for disease outcome.
Methods: CRP was measured at diagnosis and after 1 and 5 years in patients diagnosed with IBD in south-eastern Norway. After 5 years, 454 patients with ulcerative colitis and 200 with Crohn’s disease were alive and provided sufficient data for analysis.
Results: Patients with Crohn’s disease had a stronger CRP response than did those with ulcerative colitis. In patients with ulcerative colitis, CRP levels at diagnosis increased with increasing extent of disease. No differences in CRP levels at diagnosis were found between subgroups of patients with Crohn’s disease as defined according to the Vienna classification. In patients with ulcerative colitis with extensive colitis, CRP levels above 23 mg/l at diagnosis predicted an increased risk of surgery (odds ratio (OR) 4.8, 95% confidence interval (CI) 1.5 to 15.1, p = 0.02). In patients with ulcerative colitis, CRP levels above 10 mg/l after 1 year predicted an increased risk of surgery during the subsequent 4 years (OR 3.0, 95% CI 1.1 to 7.8, p = 0.02). A significant association between CRP levels at diagnosis and risk of surgery was found in patients with Crohn’s disease and terminal ileitis (L1), and the risk increased when CRP levels were above 53 mg/l in this subgroup (OR 6.0, 95% CI 1.1 to 31.9, p = 0.03).
Conclusions: CRP levels at diagnosis were related to the extent of disease in patients with ulcerative colitis. Phenotype had no influence on CRP levels in patients with Crohn’s disease. CRP is a predictor of surgery in subgroups of patients with either ulcerative colitis or Crohn’s disease.
Statistics from Altmetric.com
C-reactive protein (CRP) is one of at least 40 plasma proteins that participate in the acute phase of the inflammatory response. CRP is predominately synthesised in the hepatocytes, although extra-hepatic production has also been demonstrated. Upregulation of this protein is mainly caused by a rise in interleukin 6 (IL6) and, to a lesser extent, by increased IL1β and tumour necrosis factor α (TNFα).1 After binding to its ligand the CRP–ligand complex activates the complement cascade and induces phagocytosis. Thus, CRP plays an important role in the human innate immune system. However, the in vivo effect of this protein is complex and not fully understood.
CRP has become a useful marker for detecting and following up infections and other inflammatory diseases due to its rapid response and short half-life. Medical therapy does not seem to have a direct effect on CRP production in the hepatocytes and changes in CRP response during treatment are caused by the effect of the therapy on the underlying disease.
In clinical practice a CRP assay can be used for different purposes: to identify organic disease, as a guide in differential diagnosis, to monitor disease activity, to select responders to treatment and to predict outcome. However, although CRP levels have been measured for many years in patients with inflammatory bowel disease (IBD), there are several unanswered questions regarding the value of this protein as a clinical marker. An important question is whether CRP may be a predictor of disease outcome during follow-up.
To be able to identify factors at diagnosis associated with serious disease outcome is important in patients with IBD. Such a strategy may help to select patients who may benefit from early use of immunosuppressants and/or biological treatment (top-down strategy). In a study of patients with Crohn’s disease from a referral centre, Beaugerie et al2 found that age, the presence of perianal disease and the initial requirement for steroids were independent predictive factors for a disabling disease course. However, biological markers were not analysed in that study.
The aims of the present study were to evaluate CRP as a diagnostic and predictive marker, both at diagnosis and during follow-up, in a population-based inception cohort of patients with IBD followed for 5 years.
MATERIAL AND METHODS
All new patients diagnosed with IBD or possible IBD were recorded in four geographically well-defined areas in south-eastern Norway from 1 January 1990 to 31 December 1993 (the IBSEN cohort). The total study population on 1 January 1992 was 966 427. All the general practitioners in these areas were invited to participate in the study. A senior gastroenterologist from each hospital was made responsible for the diagnostic procedures and the registration and identification of appropriate cases. A gastroenterologist at a university hospital reviewed the clinical information. The organisation of the study has already been described in detail.3
All patients in the study were invited to a systematic follow-up visit to their local hospital 1 and 5 years (4–6 years) after diagnosis. The purpose of the visits was to re-evaluate the diagnosis and record the clinical course of the disease. The visits included a structured interview, laboratory tests, clinical examination and, if the patient agreed, colonoscopy. When the patient was unable to visit the hospital, the interview was conducted by telephone and supplemented by information from the hospital records. When the patient could not be reached by telephone, the information was based on hospital records alone, provided that these had been recently brought up to date. Medical and surgical treatment was given in accordance with established clinical practice.
Diagnosis and definitions
The diagnosis was based on the presence of symptoms consistent with IBD for more than 4 weeks, excluding infections and other acute or chronic non-IBD conditions.
Initially, the diagnosis of ulcerative colitis, Crohn’s disease, indeterminate colitis and possible IBD were used. The diagnostic criteria have already been reported.4 At the 1 year follow-up the same classification was used, but at the 5 year follow-up the patients were given a definite diagnosis of ulcerative colitis, Crohn’s disease or non-IBD. When a definite diagnosis of either ulcerative colitis or Crohn’s disease could not be made after 5 years, the most likely diagnosis was made on the basis of discussion and consensus between members of the study group.
Proctitis was defined as inflammatory changes up to 15 cm from the anus, proctosigmoiditis as disease involving the rectum and sigmoideum. Left-sided colitis was defined as inflammatory changes up to the splenic flexure, and changes beyond the splenic flexure were defined as extensive colitis.
Patients with Crohn’s disease were retrospectively classified according to the Vienna classification by of age (A1–A2), localisation (L1–L4) and behaviour of disease (B1–B3),5 on the basis of information gathered at diagnosis and 5 years later.
A relapse was defined as an aggravation of symptoms that resulted in the need for more intensive medical therapy or surgery. In the present study surgery was defined as intestinal resection. CRP levels were measured by the same standard methods in all the hospitals and the normal value was ⩽10 mg/l. At diagnosis CRP was measured before medical treatment was instituted.
Statistics
Descriptive statistics are expressed as mean and range or as frequency counts or percentages. Normally distributed data were compared by the Student t test and data that were not normally distributed were analysed by the Mann–Whitney test. Categorical data were analysed by the χ2 test and, when appropriate, Fisher’s exact test. Changes in CRP levels over time were analysed by the paired-sample t test. Associations between two continuous variables were measured by calculating Spearman’s correlation coefficient.
When CRP at diagnosis was analysed as a risk factor for disease outcome, patients were divided into CRP quartiles. The p value for linear-by-linear association was calculated in a cross-table. These analyses were performed both for the main diagnostic groups (ulcerative colitis and Crohn’s disease) and for the subgroups disease extent in patients with ulcerative colitis and disease localisations in patients with Crohn’s disease. When a statistically significant association between CRP and outcome was found, CRP concentration at the 75th percentile was used as a cut-off value for further analysis in a 2×2 table. At 1 year a cut-off value for CRP of 10 mg/l was used. We also conducted a multivariate logistic regression analysis to find which variables were associated with the risk of surgery. Forward selection was used as our model for selection strategy. The categorical variables included in this analysis were: gender, smoking status at diagnosis, and requirement of oral corticosteroids at diagnosis. In addition, for patients with Crohn’s disease stricturing and penetrating disease behaviour at diagnosis were included. Furthermore, the following continuous variables were included: age at diagnosis, CRP level, erythrocyte sedimentation rate (ESR), albumin level, platelet count and haemoglobin level. These analyses were performed separately for patients with ulcerative colitis and Crohn’s disease and for the subgroups disease extent in patients with ulcerative colitis and localisation of disease in patients with Crohn’s disease. Findings were considered significant if p values were below 0.05. All the statistical analyses were performed with SPSS Version 12.0.1 for Windows.
RESULTS
During the inclusion period a total of 843 cases of IBD or possible IBD were identified: 518 patients were diagnosed with ulcerative colitis, 221 with Crohn’s disease, 40 with indeterminate colitis and 64 with possible IBD. Clinical information was available for 739 of the patients (94%) who were alive 5 years later. Of these, 454 patients had a definite diagnosis of ulcerative colitis and 200 a definite diagnosis of Crohn’s disease. Demographic data are summarised in table 1. CRP levels were measured in 371 of 454 (82%) patients with ulcerative colitis at diagnosis, 316 (70%) 1 year later and 450 (99%) 5 years later. The corresponding figures for patients with Crohn’s disease were 176 of 200 (88%) at diagnosis, 161 (81%) 1 year later and 174 (87%) 5 years later. There were no differences in terms of gender, age at diagnosis, frequency of relapse or surgery in the follow-up period between patients whose CRP levels were measured at diagnosis and those whose CRP levels were not available. Furthermore, no difference was found between those with CRP measurements and those without as regards disease extent in patients with ulcerative colitis, and disease localisation and behaviour in patients with Crohn’s disease.
At 1 year, azathioprine was taken by 0.7% of patients with ulcerative colitis and by 6% of patients with Crohn’s disease. Furthermore, azathioprine had been taken by 3% of patients with ulcerative colitis and 22% of patients with Crohn’s disease at some point during follow-up. No patient received biological treatment.
At diagnosis the mean concentration of CRP was 18 mg/l (95% CI 14 to 21 mg/l) in patients with ulcerative colitis and 51 mg/l (95% CI 43 to 60 mg/l) in patients with Crohn’s disease (p<0.001). CRP levels in patients with Crohn’s disease with colonic involvement (L2) were higher than in patients with ulcerative colitis with extensive colitis (mean 54 mg/l, 95% CI 40 to 68 mg/l vs mean 29 mg/l, 95% CI 20 to 37 mg/l, p = 0.002). Patients with Crohn’s disease also showed a stronger CRP response than patients with ulcerative colitis 1 year (mean 51 mg/l vs 18 mg/l, p<0.001) and 5 years (mean 13 mg/l vs 6 mg/l, p<0.001) after diagnosis. No correlation was found between CRP levels at diagnosis and body mass index (BMI) in either patients with ulcerative colitis (r = −0.04) or those with Crohn’s disease (r = −0.16). In the various subgroups of patients with either ulcerative colitis or Crohn’s disease a significant correlation was observed only in those with ulcerative colitis with proctitis (r = 0.24, p = 0.04).
C-reactive protein in patients with ulcerative colitis
The relationship between CRP levels at diagnosis and disease extent are summarised in table 2. An increase in CRP levels with increasing disease extent was observed (p<0.001). However, the differences in CRP levels between patients with left-sided and those with extensive colitis, and between patients with proctitis and those with proctosigmoiditis were not statistically significant (p = 0.80 and p = 0.05, respectively).
CRP levels decreased from the time of diagnosis to the 1 year follow-up in patients with ulcerative colitis (mean 18 mg/l vs 12 mg/l, p = 0.01), with a significant decrease for patients with left-sided (mean 21 mg/l vs 9 mg/l, p = 0.03) and extensive colitis (mean 29 mg/l vs 14 mg/l, p = 0.002). However, no changes in CRP levels were found in patients with proctitis (mean 9 mg/l vs 10 mg/l, p = 0.93) and proctosigmoiditis (mean 9 mg/l vs 16 mg/l, p = 0.20).
Although an increase in CRP levels was seen with increasing extent of disease (p = 0.03) at 5 years, mean and median CRP levels were within the normal range for all subgroups. At 5 years, 195 patients with ulcerative colitis underwent colonoscopy and had CRP levels measured at the same time. No difference in CRP levels was found between patients in endoscopic remission and those with endoscopic inflammation (mean 6 mg/l vs 7 mg/l, p = 0.59).
The CRP levels measured at diagnosis were available for 28 of 34 patients who underwent colectomy during the follow-up period. At diagnosis five patients had proctitis, three proctosigmoiditis, six left-sided colitis and 14 extensive colitis. No significant association was found between CRP levels at diagnosis and colectomy in patients with ulcerative colitis (p = 0.16). An analysis of CRP levels in the subgroups showed a significant association in patients with extensive colitis. In this subgroup patients with CRP levels above the 75th percentile (23 mg/l) at diagnosis had an increased risk of colectomy during the follow-up period (24% vs 6%, OR 4.8, 95% CI 1.5 to 15.1, p = 0.02) (fig 1) and all five patients who underwent colectomy within the first month of diagnosis had CRP levels above 23 mg/l (p<0.001). However, between 1 month and 5 years after diagnosis CRP levels above this cut-off point were not a predictor of surgery (p = 0.50).

In a logistic regression analysis colectomy in patients with ulcerative colitis was associated with age (OR 0.94, 95% CI 0.90 to 0.97, p<0.001) and albumin level (OR 0.90, 95% CI 0.82 to 0.98, p = 0.02) at diagnosis. In the subgroups colectomy was associated with age (OR 0.90 95% CI 0.84 to 0.96, p = 0.003) and CRP level (OR 1.01, 95% CI 1.01 to 1.03, p = 0.04) in patients with extensive colitis. For the other subgroups no risk factors were found.
At 1 year, 23% of the patients with ulcerative colitis had increased CRP levels and CRP levels above 10 mg/l increased the risk of surgery during the subsequent 4 years (OR 3.0, 95% CI 1.1 to 7.8, p = 0.02).
Fifty per cent of the patients with ulcerative colitis relapsed within the first year after diagnosis and 78% during the 5 year follow-up period. No association was found between CRP levels at diagnosis and the risk of relapse for the patients with ulcerative colitis as a whole or for the various ulcerative colitis subgroups.
C-reactive protein in patients with Crohn’s disease
Most patients with Crohn’s disease (75%) had elevated CRP levels at diagnosis. CRP levels in patients with Crohn’s disease are summarised in table 3. No differences in CRP levels were observed between subgroups of patients categorised according to the Vienna classification related to age (A1–A2), localisation (L1–L4) and behaviour (B1–B3) of the disease.
An overall decrease in mean CRP level from 51 mg/l (95% CI 43 to 60 mg/l) to 16 mg/l (95% CI 12 to 19 mg/l) was observed from diagnosis up to 1 year (p<0.001), and a significant decrease in CRP levels was observed for all subgroups.
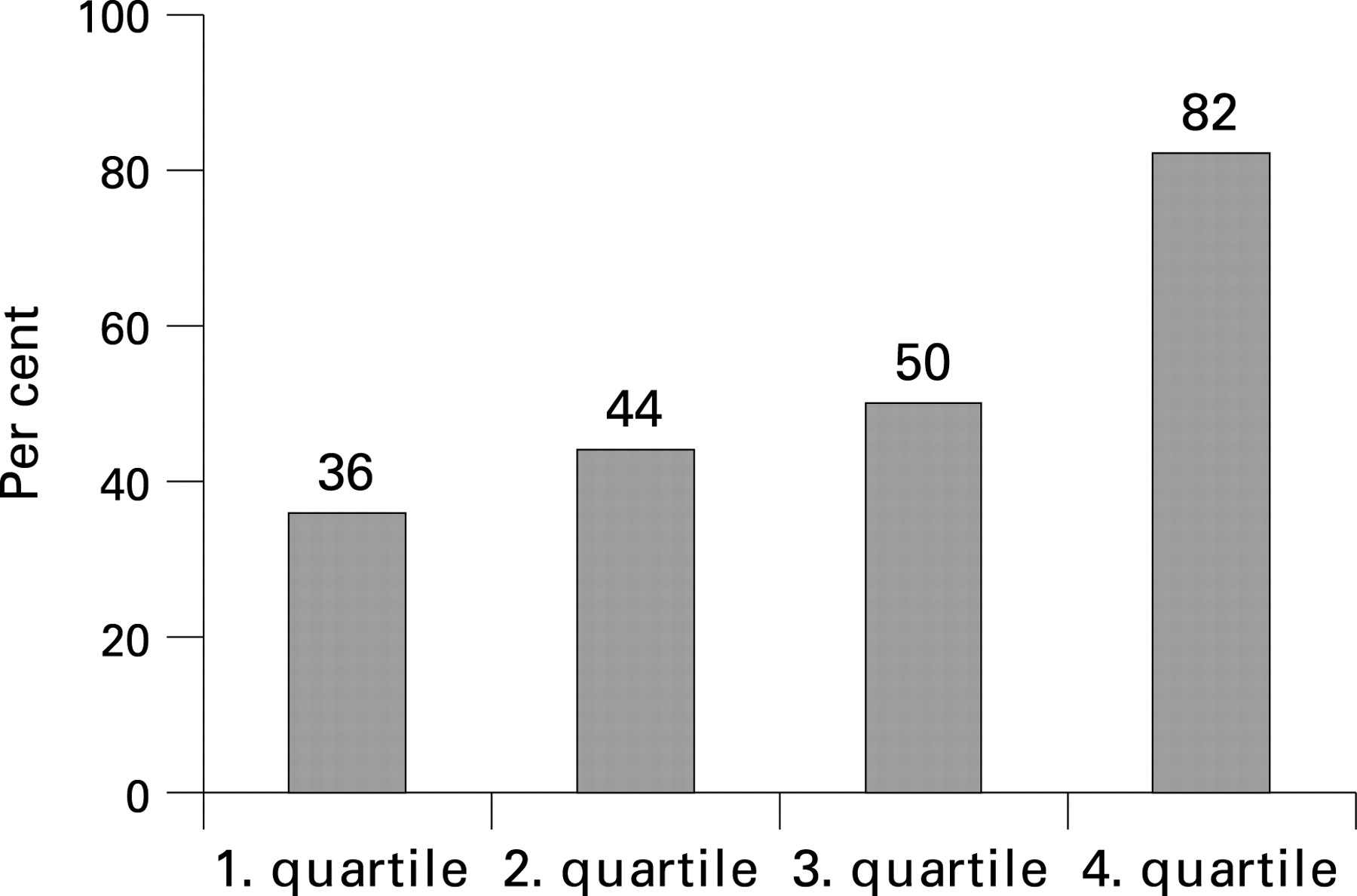
CRP levels at diagnosis were available for 49 of 56 patients who underwent surgery during the follow-up period. The localisation of disease in these patients was L1 in 24 patients, L2 in 12, L3 in 11, and L4 in two. There was no association between CRP levels and risk of surgery for the Crohn’s disease group as a whole (p = 0.71) or for patients with L2 or L3. The number of patients in the L4 group was too small for statistical analysis. In the L1 group a significant linear association was found between CRP levels and risk of surgery (p = 0.03), and when CRP was above 53 mg/l (75th percentile) the risk of surgery increased from 43 to 82% (OR 6.0, 95% CI 1.1 to 31.9) (fig 2). CRP levels above 53 mg/l had the same predictive value for both early (within 1 month) and later surgery.

{kind=link}
{kind=link}
{kind=link}
In a logistic regression analysis, surgery in patients with Crohn’s disease was associated with age (OR 0.97, 95% CI 0.95 to 0.99, p = 0.04), stricturing behaviour (OR 3.10, 95% CI 1.40 to 6.85, p = 0.005) and penetrating behaviour (OR 8.20, 95% CI 2.60 to 25.82, p<0.001) at diagnosis. In the subgroup analysis, surgery in the L1 group was associated with age (OR 0.93, 95% CI 0.87 to 0.99, p = 0.04) and CRP level (OR 1.03, 95% CI 1.01 to 1.05, p = 0.03). For patients in the L2 group age (OR 0.95, 95% CI 0.91 to 0.99, p = 0.04) and penetrating disease behaviour (OR 16.27, 95% CI 2.58 to 102.65, p = 0.003) were significantly associated with surgery. For patients in the L3 group no risk factors were found.
At 1 year, increased CRP levels were found in 34% of the patients with Crohn’s disease. An increased risk of surgery during the subsequent 4 years was found when CRP was above 10 mg/l, but the difference was not statistical significant (OR 2.3, 95% CI 0.9 to 6.1, p = 0.09).
During the first year 52% of the patients relapsed and this figure had risen further at 5 years to 86%. No association was found between CRP levels at diagnosis and relapse for the Crohn’s disease group as a whole or for subgroups according to disease localisation.
DISCUSSION
In this population-based prospective study of CRP in IBD patients, we found a significantly stronger CRP response in patients with Crohn’s disease than in patients with ulcerative colitis. In patients with ulcerative colitis CRP levels were related to disease extent, but in patients with Crohn’s disease we found no difference in CRP levels between phenotypes. In subgroups of patients with ulcerative colitis and Crohn’s disease higher CRP levels increased the risk of surgery.
Although CRP levels have been shown to be a help in differentiating between IBD and non-IBD conditions in both children and adults6–8 it is important to keep in mind that many IBD patients have CRP levels within the normal range at diagnosis. In the present study 71% of patients with ulcerative colitis and 25% with Crohn’s disease had CRP levels within the normal range. This means that, in many patients, measuring CRP at diagnosis would not help to differentiate between IBD and functional disorders. Although higher levels of CRP were found in patients with Crohn’s disease than in those with ulcerative colitis, both at diagnosis and during follow-up, we also observed a large spread and overlap in the serum concentrations between the two conditions. This finding means that CRP measurements are of limited value in differentiating between ulcerative colitis and Crohn’s disease.
Previous studies have shown that patients with Crohn’s disease have a higher CRP production than patients with ulcerative colitis9–11 and also a higher serum concentration of IL6.12 One explanation could be that Crohn’s disease involves a transmural inflammation of the gut wall whereas ulcerative colitis is limited to the mucosa. Mesenteric fat is a major site of IL6 and TNFα synthesis, and an association between CRP levels and BMI has been found in healthy subjects.13–15 An accumulation of intra-abdominal fat has been observed in patients with Crohn’s disease,16 and this fatty tissue may contribute to the difference in CRP production between patients with ulcerative colitis and Crohn’s disease. In a recent study, CRP levels were correlated with radiological findings of increased fat density in patients with ileal involvement, but not in those with inflammation limited to the small bowel wall.17 In the present study, patients with Crohn’s disease with colonic involvement had a stronger CRP response than patients with ulcerative colitis with extensive colitis, indicating that extent of disease is probably not a major factor. Bacteraemia is a potent stimulator of CRP production, but it is not clear whether this mechanism influences CRP production in patients with Crohn’s disease. Individual genetic factors may also contribute to differences in the CRP response. Recently, Florin et al18 found that normal CRP levels were more often associated with ileal involvement and low BMI in patients with Crohn’s disease with a Crohn’s disease activity index (CDAI)⩾200, but in our study there was no such association between CRP levels and BMI at the time of diagnosis.
We observed a decrease in the CRP level over time in patients with ulcerative colitis and those with Crohn’s disease. There is no medical therapy that has been shown to reduce the production of CRP by hepatocytes, so a decrease in CRP concentration must be the result of either a reduction in gut inflammation caused by medical therapy or a natural variation in disease activity, or both.
CRP has been used as a marker of gut inflammation during follow-up of IBD patients, but the association between CRP levels and degree of inflammation is poorly documented.19–21 In the present study, no difference in CRP response was observed between Crohn’s disease subgroups according to the Vienna classification. CRP levels in patients with ulcerative colitis were associated with extent of disease at diagnosis. Five years after diagnosis CRP levels did not differentiate between patients with ulcerative colitis with endoscopic remission and those without remission, which may indicate that CRP is of limited value in predicting disease activity during follow-up. Although an increase in CRP with increasing extent of disease was observed at 5 years, mean and median CRP values were within the normal range in all ulcerative colitis subgroups.
The ability to predict disease outcome in IBD patients is important for both physicians and patients. Boirivant et al22 showed an increased risk of relapse during the second year of follow-up in patients with Crohn’s disease with elevated CRP. In a study where biomarkers were evaluated every 6 weeks in patients with Crohn’s disease, CRP (>20 mg/l) and ESR (>15 mm) were predictive of relapse.23 However, a study by Costa et al24 showed CRP levels to be of no predictive value in either patients with ulcerative colitis or those with Crohn’s disease. Although there are few reports evaluating CRP as a predictor of surgery in patients with ulcerative colitis, a study that included patients with severe ulcerative colitis found that CRP >45 mg/l on day 3 after initiation of intensive medical treatment predicted increased risk of colectomy.25
We found an increased risk of surgery when CRP was above 23 mg/l in patients with ulcerative colitis with extensive colitis at diagnosis. A multivariant analysis confirmed that CRP level was an independent risk factor for surgery in this group. However, CRP level was only predictive for colectomy performed within 1 month. On the other hand, increase CRP levels after 1 year of treatment was a predictor of surgery during the subsequent 4 years.
As far as we know, no study has evaluated CRP as a predictive factor for intestinal resection in patients with Crohn’s disease. In our study a significant association between intestinal resection during follow-up and CRP levels at diagnosis was only observed for Crohn’s disease involving terminal ileum (L1) and this association was confirmed in a multivariant analysis. The risk of surgery increased when CRP at diagnosis was above 53 mg/l, and elevated CRP levels in patients with Crohn’s disease at 1 year increased the risk of surgery during the subsequent 4 years. The increase was not statistically significant, but this could be due to a type II error.
Since few of the patients with ulcerative colitis or Crohn’s disease underwent surgery, the data for the risk of surgery in the various subgroups should be interpreted with caution. We did not find any association between relapse and CRP levels in patients with either ulcerative colitis or Crohn’s disease as a whole or in any subgroup. Further studies should be carried out to evaluate whether highly sensitive CRP assays could be a more sensitive marker of gut inflammation and disease outcome in IBD patients than the CRP assay used in the present study.
In conclusion, this population-based study confirms that CRP levels are higher in patients with Crohn’s disease than in those with ulcerative colitis both at diagnosis and during follow-up. However, a substantial proportion of patients with ulcerative colitis and those with Crohn’s disease had CRP levels at diagnosis within the normal range, with a large overlap in serum concentrations. CRP levels at diagnosis were related to the extent of disease in patients with ulcerative colitis, while in patients with Crohn’s disease no association was found between CRP levels at diagnosis and any of the subgroups according to the Vienna classification. Although CRP levels did not predict relapse in our IBD patients, CRP levels at diagnosis and after 1 year did predict surgery in subgroups of patients with ulcerative colitis or Crohn’s disease.
Acknowledgments
We thank the following members of the Inflammatory Bowel South-Eastern Norway (IBSEN) Study Group of gastroenterologists for participating in this study: Erling Aadland, Aker University Hospital; Erik Aubert, Østfold Hospital Moss; Borgar Flaaten, Notodden Hospital; Tom Schulz, Vest-Agder Central Hospital, Arendal; and Øystein Kjellevold, Blefjell Hospital, Rjukan. We thank the following colleagues for help with statistical analysis: Kathrine Frey Frøslie, Dept. of Biological Statistics, Rikshospitalet University Hospital; Leiv Sandvik, Ullevål University Hospital; and Geir Aamodt, Norwegian Institute of Public Health.
REFERENCES
Footnotes
Funding: The study was supported by the Eastern Norway Regional Health Authority.
Competing interests: None.
Ethics approval: The study was approved by the Regional Ethics Committee, and permission was obtained from the Norwegian Data Registry.
Linked Articles
- Digest