Article Text

Abstract
Treatment modalities for gastro-oesophageal reflux disease (GORD) mirror the pathophysiology of the disease. Since acid plays a key role in GORD-associated mucosal lesions, proton pump inhibitors (PPIs) are the dominant GORD treatment, being the most potent inhibitors of acid secretion available. However, the clinical effectiveness of PPIs varies with the specific symptoms being treated; they are more effective for heartburn than for regurgitation than for extra-oesophageal symptoms. An alternative therapeutic approach to GORD is to prevent the most fundamental cause of reflux symptoms, reflux itself, which most commonly occurs by transient lower oesophageal sphincter relaxation (TLOSR). Among potential pharmaceutical agents developed to target TLOSRs, the most advanced are GABAB (γ-aminobutyric acid) agonists, which experimentally reduce the occurrence of TLOSRs by about 40% in both animal and human studies. However, the effectiveness of GABAB agonists in clinical trials of patients with GORD with an incomplete response to PPI treatment has been modest. In part, this is probably attributable to the difficult problem of patient selection in these trials. Identifying patients by partial response to PPI treatment results in a heterogeneous population, including those with persistent weakly acidic reflux, patients with visceral hypersensitivity and those with functional heartburn, dyspepsia, or chest pain. From the clinical data available, the best treatment results and, hence, the patients most likely to benefit from reflux inhibitors, are those with persistent reflux, most commonly manifest as persistent regurgitation despite PPI treatment.
- Gastro-oesophageal reflux disease
- drug development
- proton pump inhibitors
- gastro-oesopahgeal junction
- antireflux therapy
- autonomic nervous system
- dysphagia
- oesophageal pH monitoring
- oesophageal physiology
- oesophageal reflux
- motility disorders
Statistics from Altmetric.com
- Gastro-oesophageal reflux disease
- drug development
- proton pump inhibitors
- gastro-oesopahgeal junction
- antireflux therapy
- autonomic nervous system
- dysphagia
- oesophageal pH monitoring
- oesophageal physiology
- oesophageal reflux
- motility disorders
Key messages: gastro-oesophageal reflux disease pathophysiology
-
Gastro-oesophageal reflux disease (GORD) is a complex motility disorder with both physiological and anatomical causes and a wide variety of clinical manifestations.
-
Proton pump inhibitors compensate for excessive gastro-oesophageal reflux by reducing the acidity of gastric juice but their effectiveness varies with the specific reflux syndrome treated; oesophagitis > heartburn > regurgitation or chest pain > extra-oesophageal manifestations.
-
An alternative approach to GORD treatment is to reduce the occurrence of reflux, which is possible through pharmacological inhibition of transient lower oesophageal sphincter relaxations (TLOSRs).
-
TLOSRs are the most common mechanism by which reflux occurs but the most common distinguishing feature of patients with GORD is in the consequences of TLOSRs rather than their numerical excess.
Introduction
Gastro-oesophageal reflux disease (GORD) is complex. It is probably best to conceptualise GORD as a group of syndromes rather than as a single entity. Such was the conclusion of the Montreal Consensus Group in formulating the definition, ‘a condition which develops when the reflux of stomach contents causes troublesome symptoms and/or complications’ (figure 1).1 Oesophagitis is a different condition than symptomatic regurgitation, which, in turn, is a very different problem than reflux-cough syndrome. All fit the overarching definition of GORD, but each has a unique set of pathophysiological determinants. A corollary to this, somehow lost in translation, is that treatments for reflux disease may be highly effective for some reflux syndromes and completely ineffective for others. In other words, contrary to prevailing opinion, reflux disease is not defined by responsiveness to proton pump inhibitor (PPI) treatment. Rather, the most ubiquitous feature is reflux itself because all else follows from that. Hence, the appeal of pharmacological reflux inhibition. The aim of this overview is to appraise the recent successes and failures of that approach.
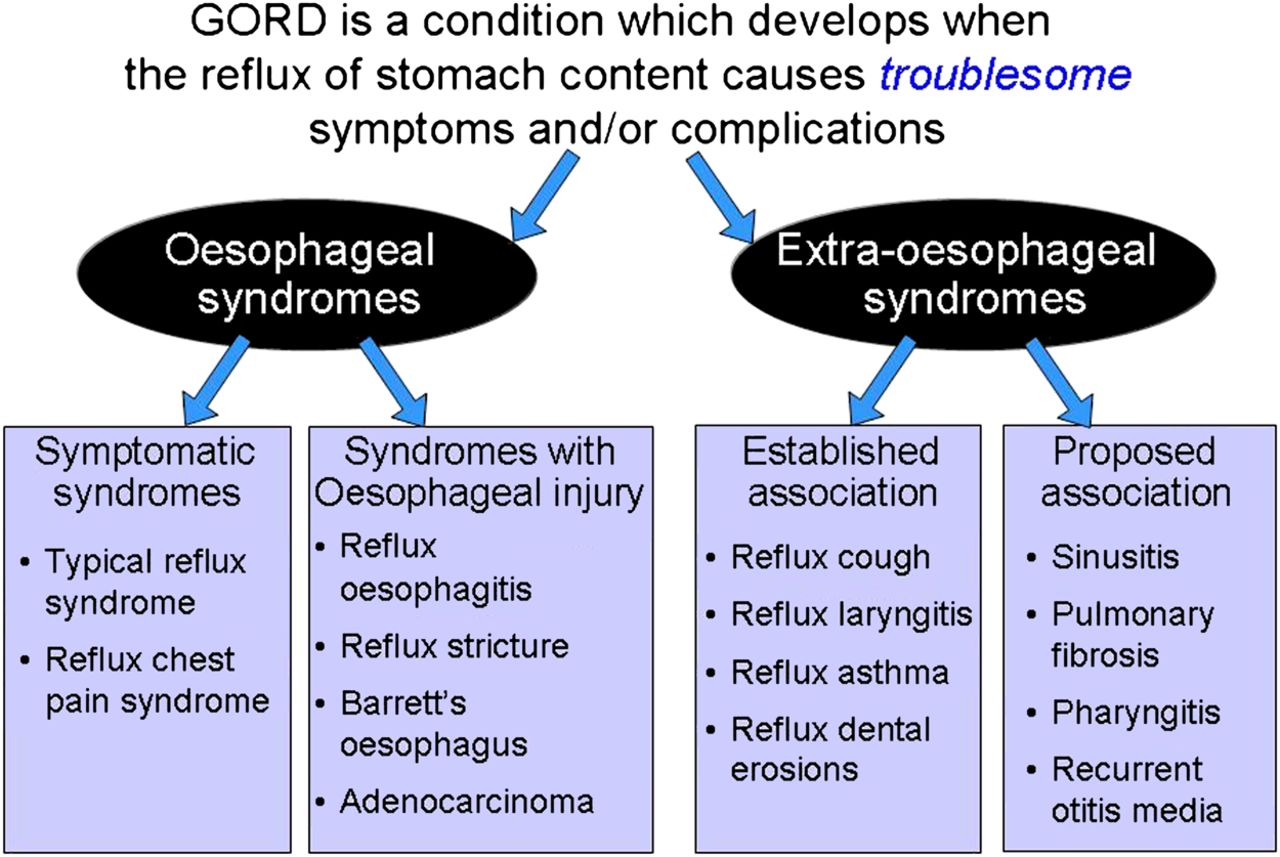
The Montreal definition of gastro-oesophageal reflux disease. The overarching definition encompasses both oesophageal and extra-oesophageal syndromes which can be based on a symptom complex, endoscopic findings, or epidemiological association. The level of established causality with the established and proposed associated conditions is highly variable.
GORD pathophysiology and limitations of PPI treatment
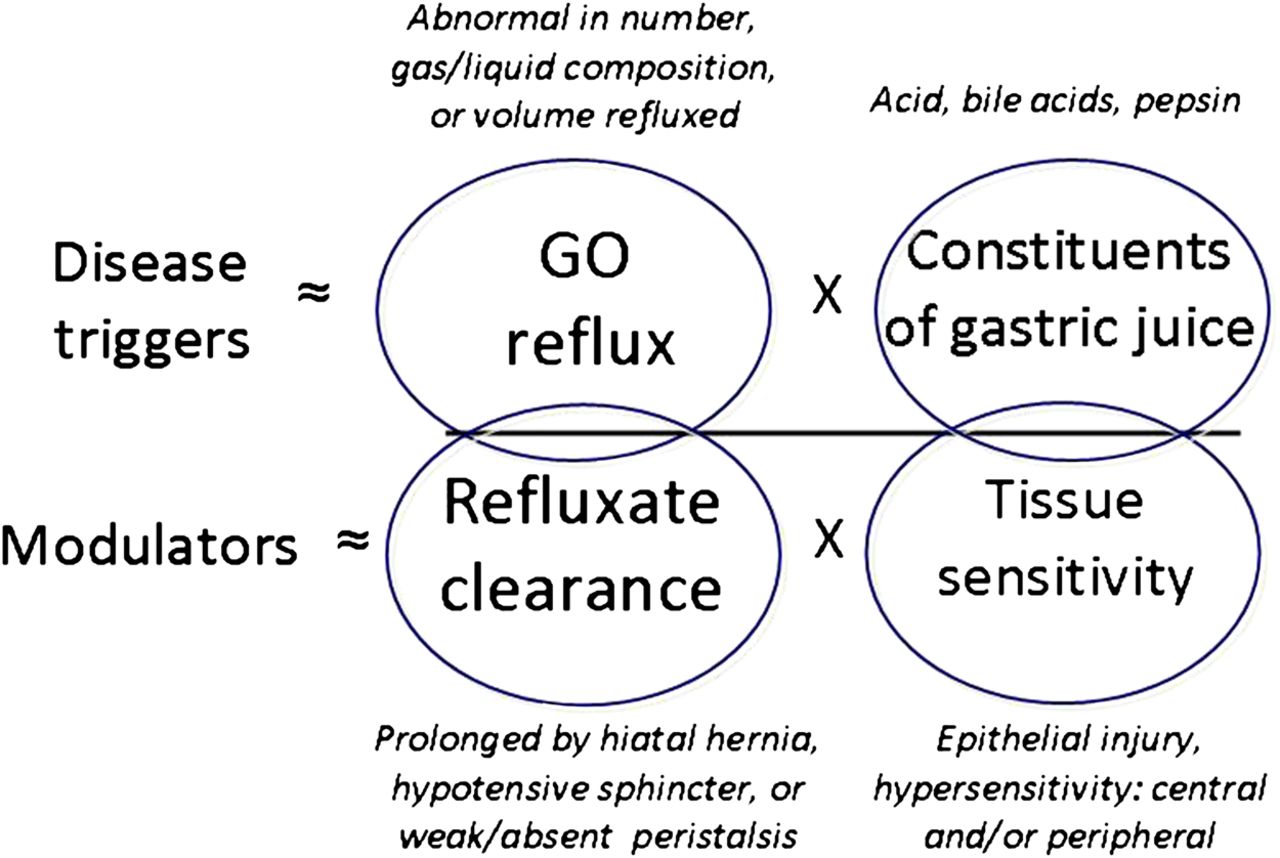
Fundamental to the Montreal definition of GORD is that gastro-oesophageal reflux is the root cause of the disease. However, while that may be the unifying concept among all of the encompassed GORD syndromes, it is not the only pathophysiological determinant to consider. In fact, as detailed in figure 2, there are four major pathophysiological determinants: gastro-oesophageal reflux, refluxate constituents, refluxate clearance and mucosal sensitivity, be that mediated peripherally or centrally. Any of these may dominate the pathophysiology of a particular GORD syndrome. Indeed, most patients with heartburn do not have oesophagitis even before treatment and this lack of connection becomes more exaggerated with atypical GORD symptoms.2 The dominant feature distinguishing oesophagitis from symptomatic heartburn is not reflux but, rather, impaired refluxate (acid) clearance attributable to the effects of a hiatal hernia or weak peristalsis.3 ,4 Prolonged acid clearance correlates with both the severity of oesophagitis and the presence of Barrett's metaplasia.5 ,6 The efficacy of acid clearance is particularly impaired in those patients with non-reducing hiatus hernia who exhibit reflux of fluid from the hernia during deglutitive relaxation.7 ,8 Conversely, patients with symptomatic heartburn without oesophagitis tend to exhibit heightened mucosal sensitively, probably related to mucosal factors such as dilated intercellular spaces, as a distinguishing feature.9

Conceptual model of the pathophysiology of gastro-oesophageal reflux disease (GORD). The fundamental abnormalities are of excess reflux events and prolonged clearance. However, the effect of reflux in eliciting symptoms is linked to the toxicity of gastric juice even though this is usually normal in patients with GORD. Acid clearance and mucosal sensitivity modulate the effect of reflux events by prolonging the exposure of the oesophageal mucosa to refluxate and making the mucosa fundamentally more sensitive. Each of these elements may be targeted by GORD treatments. However, the most attractive target is the reflux event itself because all else follows from that.
Generally speaking, GORD treatments target individual elements of GORD pathophysiology as conceptualised in figure 2. As might be expected, pharmaceutical treatments have minimal effect in improving acid clearance, but lifestyle modifications such as avoiding post-prandial recumbency and anti-reflux surgery to eliminate hiatus hernia do target this mechanism.10 Visceral sensitivity is gaining recognition as an important element of reflux pathophysiology, and is increasingly considered to be an important modulator of reflux symptom severity and, in the case of reflux cough, a key pathophysiological feature.11 However, thus far, treatments targeting this mechanism are rudimentary and non-specific.12 On the other hand, the lethality of gastric juice to oesophageal epithelial cells, a key event in the pathogenesis of oesophagitis, proved to be an excellent pharmacological target. Consequently, the dominant pharmacological GORD treatments (PPIs) work by inhibiting acid secretion. Somewhat paradoxically, gastric acid secretion is usually normal in patients with GORD and the dominance of acid as a pathophysiological determinant diminishes with syndromes other than oesophagitis. The therapeutic implications of that observation are summarised in figure 3 comparing the efficacy of PPIs in treating oesophagitis with their efficacy in treating GORD syndromes other than oesophagitis. Evident in the figure, PPI efficacy progressively diminishes when moving from oesophagitis to symptomatic heartburn, regurgitation,14 ,15 chest pain,16 cough17 and laryngitis.13 Improving these therapeutic outcomes will probably require finding an alternative treatment strategy and, given its fundamental significance, reflux inhibition is an attractive candidate. Reflux inhibition is potentially achieved pharmacologically by augmenting lower oesophageal sphincter (LOS) pressure or by reducing the number of transient lower oesophageal sphincter relaxations (TLOSRs).

Summary of proton pump inhibitor efficacy for potential manifestations of gastro-oesophageal reflux disease (GORD) as assessed in randomised controlled trials. In each case, data among trials are averaged to derive estimates of placebo effect and therapeutic gain (the degree to which the active treatment improved over the benefit seen with placebo). The blue bars represent the placebo effect and the green bars the therapeutic gain beyond the placebo effect seen with proton pump inhibitors (PPIs). PPI data are grouped by brand and dose, taking some liberties for simplification. However, it should be noted that the only disease manifestation in which a dose–response curve has been demonstrated by a randomised controlled trial is in the healing of oesophagitis. At the other extreme, in the case of hoarseness, controlled trial data are sparse and the only large trial (which was done in patients without oesophagitis or frequent heartburn) failed to show benefit of PPI versus placebo.13 LA; Los Angeles. NERD; nonerosive reflux disease; OGD; oesophagogastroduodenoscopy.
Compelling evidence exists that TLOSRs are the most common mechanism for reflux during periods of normal LOS pressure (>10 mm Hg). Transient LOS relaxations occur independently of swallowing, persist for longer periods than swallow-induced LOS relaxations (>10 s) and are not accompanied by peristalsis.18 ,19 Furthermore, TLOSR is an integrated motor response involving LOS relaxation and also crural diaphragmatic inhibition, contraction of the costal diaphragm and prolonged longitudinal muscle contraction in the distal oesophagus19–21 (figure 4). The TLOSR reflex is abolished by vagotomy.22

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schematic diagram of the transient lower oesophageal sphincter relaxation reflex. Proximal gastric distension stimulates vagal afferents through intraganglionic lamellar endings (IGLEs) that function as tension receptors in the myenteric plexus. After relay through the nucleus solitaries and dorsal motor nucleus of the vagus, vagal efferents mediate lower oesophageal sphincter (LOS) relaxation, distal oesophageal shortening and crural diaphragm inhibition. Not shown in the diagram but reported from animal studies is concomitant costal diaphragm contraction.22
TLOSRs as a mechanism of reflux
Conceptualised as the impediment to reflux, the oesophagogastric junction (OGJ) is a high-pressure zone at the distal end of the oesophagus that isolates the oesophagus from the stomach. However, OGJ anatomy is complex. The oesophagus traverses the diaphragmatic hiatus and joins the stomach in a nearly tangential fashion. Thus, there are several potential contributors to OGJ competence (or incompetence): the intrinsic LOS, the aperture of the diaphragmatic hiatus, the contraction of the crural diaphragm against the oesophagus and the muscular architecture of the gastric cardia that constitutes the distal aspect of the OGJ high-pressure zone. LOS pressure varies widely among normal individuals and fluctuates throughout the day, decreasing in the post-cibal state and increasing during sleep and with the migrating motor complex.23 The genesis of LOS tone is a property of both the smooth muscle of the sphincter and its extrinsic innervation.24 At a given moment, myogenic factors, intra-abdominal pressure, gastric distension, peptides, hormones, various foods and many drugs affect LOS pressure. Vagal modulation is mediated through myenteric plexus neurons that can stimulate either LOS contraction or relaxation. Surrounding the LOS at the level of the squamocolumnar mucosal junction is the diaphragmatic hiatus, a teardrop shaped canal that is normally about 2 cm long on its major axis, formed by the right crus of the diaphragm. Recent physiological investigations have advanced the ‘two-sphincter hypothesis’ for maintenance of OGJ competence, suggesting that both the intrinsic LOS and the extrinsic crural diaphragm serve a sphincteric function. Independent control of the crural diaphragm can be demonstrated during oesophageal distension, vomiting and belching when electrical activity in the crural diaphragm is selectively inhibited despite continued respiration.25 ,26 This reflex inhibition of crural activity is eliminated with vagotomy.22
A multitude of investigations have concluded that there are three dominant mechanisms of OGJ incompetence: (1) TLOSRs with or without anatomic abnormality; (2) LOS hypotension, again with or without anatomic abnormality; or (3) anatomical distortion of the OGJ inclusive of (but not limited to) hiatus hernia.23 ,27–29 Which reflux mechanism dominates depends upon a number of factors. While TLOSRs typically account for up to 90% of reflux events in normal subjects or patients with GORD without hiatus hernia, more heterogeneous mechanisms are found in patients with hiatus hernia, with reflux episodes frequently occurring in the context of LOS hypotension, straining and even swallow-associated LOS relaxation.28 ,30 These observations support the hypothesis that the functional integrity of the OGJ is dependent on both the intrinsic LOS and extrinsic sphincteric function of the diaphragmatic hiatus. In essence, the occurrence of gastro-oesophageal reflux requires two ‘hits’ to the OGJ. Patients with a normal OGJ require inhibition of both the intrinsic LOS and the crural diaphragm for reflux to occur; physiologically, this occurs only in the setting of a TLOSR. In contrast, patients with hiatal hernia or a widely dilated hiatus may exhibit pre-existing compromise of the hiatal sphincter. In that setting reflux can occur during a TLOSR and also with LOS hypotension or even deglutitive LOS relaxation. Complicating the situation further, prolonged high-resolution manometric studies show that some patients with GORD spontaneously switch from a non-hernia to a hernia OGJ conformation and that while TLOSRs dominate in the non-hernia conformation, non-TLOSR mechanisms become twofold more common in the hernia conformation.31
The dominant stimulus for TLOSRs is distension of the proximal stomach; not surprising given that transient LOS relaxation is the physiological mechanism for belching.32 The frequency of TLOSRs is also increased by assuming an upright posture.33 Transient LOS relaxation can be experimentally elicited by a standardised meal, gaseous distension of the stomach, or distension of the proximal stomach with a barostat bag. An interesting variation on this is with achalasia, an ‘experiment of nature’ in which there is selective dysfunction of the inhibitory post-ganglionic myenteric plexus neurons. Stimulated by gastric distension, patients with achalasia exhibit a motor response similar to a TLOSR (distal oesophageal shortening, crural diaphragm inhibition, distal oesophageal and LOS after-contraction), but selectively lacking LOS relaxation.34 Another modifier of the distension response is hiatus hernia, which lowers the threshold for experimentally eliciting TLOSRs. The degree to which TLOSR frequency is augmented by gastric distension is directly proportional to the size of hiatus hernia, suggesting that the associated anatomical alteration affects the function of the afferent mechanoreceptors responsible for eliciting this reflex.35 The most likely candidate for the afferent receptor is the intraganglionic lamellar ending.36 Intraganglionic lamellar endings are found at the receptor end of vagal afferents innervating the gastric cardia and fire in direct proportion to applied tension.37 The vagal afferent mechanoreceptors in the gastric cardia then project to the nucleus tractus solitarii in the brainstem and subsequently to the dorsal motor nuclei of the vagus. Finally, dorsal motor nucleus neurons project to inhibitory neurons localised within the myenteric plexus of the distal oesophagus.
Of note, prolonged manometric recordings have not consistently demonstrated an increased frequency of TLOSRs in patients with GORD compared with normal controls.33 About half of the studies show an increased TLOSR frequency in patients with reflux while the other half show no difference between patients with reflux and control subjects. Quite possibly, the difference pertains to the specific reflux populations studied, with an increased TLOSR frequency attributable to a greater proportion of individuals with hiatus hernia included in the study population. However, a consistent observation, in all but one of these investigations, was that the frequency of acid reflux (as opposed to gas reflux) during TLOSRs was greater in patients with GORD. Furthermore, a study using a radioactive clip to localise the OGJ, and technetium pertechnetate to localise the pool of recently secreted acid, showed that this pool or ‘pocket’ tends to localise within the hiatus or even above the diaphragm in patients with GORD.38 All of these observations suggest that the more consistent feature is a qualitative difference in the consequences of a TLOSR rather than the frequency of TLOSRs in patients with GORD compared with non-GORD individuals. Physiological data have demonstrated increased compliance of the OGJ to be a fundamental abnormality in patients with GORD with or without hiatus hernia.39 With all other physical variables held constant, increased OGJ compliance leads to an increased volume of both gas and liquid flow across the relaxed OGJ.40 Consequently, while a TLOSR is likely to result in a mainly gas reflux in a normal person, the same physiological event can to lead to reflux of liquid into the proximal oesophagus and even regurgitation of liquid into the hypopharynx in a person with GORD.41 ,42 If the increased compliance is coupled with the increased intra-abdominal pressure due to abdominal obesity then the effects of increased compliance are magnified further by an increased gastro-oesophageal pressure gradient.43
In summary, TLOSRs are undoubtedly of major significance in the pathogenesis of GORD. However, it is not a simple matter of numerical excess. While there may be a numerical excess in selected individuals and in patients with hiatus hernia, the more prevailing abnormality is in the consequences of TLOSRs. In normal individuals, this is an exquisitely designed reflex leading to the selective venting of gas from the stomach while simultaneously constraining fluid reflux. Individuals with reflux disease, on the other hand, lose this content selectivity and reflux larger volumes of both gas and fluid. This leads to proximal oesophageal exposure to gastric reflux and acid regurgitation to a much greater degree than seen in normal individuals. Numerous physiological investigations have concluded that proximal reflux events are more likely to be associated with heartburn and/or chest pain.44 Box 1 summarises qualitative differences between patients with GORD and control subjects that affect the physiological consequences of TLOSRs.
Anatomical and/or mechanical factors implicated in gastro-oesophageal reflux disease pathogenesis that tend to diminish the dominance of transient lower oesophageal sphincter relaxation (TLOSR) as a mechanism of reflux
-
‘Patulous hiatus’
-
Compromised oesophagogastric junction (OGJ) pressure augmentation during respiration
-
Increased reflux events related to ‘abdominal strain’
-
Intermittent transition to hiatus hernia
-
-
Increased OGJ compliance
-
Increased volume of reflux with increased oesophageal distension, more proximal spread and regurgitation
-
Loss of air/water discrimination during reflux owing to the increased opening diameter of the OGJ
-
-
Hiatus hernia
-
Reflux and ‘superimposed-reflux’ during deglutitive lower oesophageal sphincter relaxation, leading to prolonged acid clearance while supine and a mechanism of reflux not encountered in normal individuals
-
Lower threshold for experimentally eliciting TLOSRs with gastric distension
-
Impaired acid clearance
-
-
Obesity
-
Increased intra-abdominal pressure, which both promotes the formation of hiatus hernia and increases the volume of reflux owing to the augmented abdominal to mediastinal pressure gradient
-
Key messages: clinical trial experience with reflux inhibitors
-
GABAB (γ-aminobutyric acid) antagonists and mGluR5 (metabotropic glutamate receptor 5) agonists reduce transient lower oesophageal sphincter relaxation (TLOSR) frequency by about 40%, with associated reduction in reflux events and oesophageal acid exposure in both control subjects and patients with gastro-oesophageal reflux disease (GORD).
-
Proof-of-principle trials of reflux inhibitors suggest clinical efficacy as monotherapy in patients with GORD previously shown to be responsive to proton pump inhibitor (PPI) treatment.
-
The largest reflux inhibitor clinical trial experience is with the GABAB agonist, lesogaberan, used as add-on treatment for patients partially responsive to PPIs and, though significant, the therapeutic gain was slight relative to placebo.
-
The best clinical response to reflux inhibitor treatment was seen for the symptoms of heartburn and regurgitation, precisely the symptoms most tightly physiologically coupled to TLOSRs.
-
All major development programmes for reflux inhibitors have been suspended and the path forward is uncertain.
Reflux inhibition
Given that reflux of acid or non-acid gastric content during TLOSRs leads to reflux symptoms, pharmacological reduction of TLOSRs represents an attractive therapeutic target. The first evidence supporting the feasibility of this concept was reported by Mittal et al using atropine in healthy subjects.45 Despite profound reduction of LOS pressure, atropine reduced the frequency of reflux episodes following meal ingestion by reducing the number of TLOSRs, thereby implicating muscarinic receptors in the TLOSR pathway. Since then, both preclinical and human studies have identified numerous neurotransmitters and receptors involved in the TLOSR reflex as potential drug targets, including nitric oxide, glutamate, cannabinoids, γ-aminobutyric acid (GABA), cholecystokinin, morphine and acetylcholine.46 ,47 However, mainly because of safety concerns, only GABAB receptor agonists and metabotropic glutamate receptor 5 (mGluR5) antagonists have reached the stage of clinical development and evaluation in humans.
Preclinical data have abundantly demonstrated the potency of GABAB receptor agonists to reduce the number of TLOSRs.48 Baclofen, already in clinical use as a skeletal muscle antispasmodic agent, was the first GABAB agonist shown to effect a 60% reduction in postprandial reflux episodes due to blockade of TLOSRs.49 Since then, baclofen's potential as a reflux inhibitor has been confirmed in both healthy subjects and patients with GORD by reducing the number of reflux events (acid and weakly acidic), oesophageal acid exposure, bile reflux and reflux symptoms.49–57 However, baclofen crosses the blood–brain barrier and is frequently associated with central nervous system side effects such as drowsiness, dizziness, lightheadedness and headache, severely limiting its clinical utility in GORD. Moreover, baclofen has a short half-life requiring frequent dosing and potentially compromising patient compliance. Two pharmacological strategies that have been used to overcome these shortcomings are (1) the development of peripherally restricted GABAB agonists (AZD9343 and lesogaberan (AZD3355))58 ,59 and (2) using a transported prodrug of R-baclofen in a sustained-release formulation (arbaclofen) to minimise fluctuations in serum concentration.60 Clinical evaluation progressed furthest with the peripherally restricted GABAB agonists. Tested in healthy subjects, both lesogaberan and AZD9343 reduced the number of reflux episodes, reduced the rate of TLOSRs, increased resting LOS pressure and were better tolerated than baclofen.61 ,62
In addition to GABAB agonists, mGluR5 antagonists have also been shown to reduce reflux and TLOSRs in animal models,63 ,64 leading to their development for human use (ADX10059 and AZD2066). AZD2066 was shown to reduce the number of TLOSRs by 27% and reflux events by 51% in healthy subjects.65 No data on TLOSRs suppression are available for ADX10059, but it has been shown to be well tolerated and to reduce reflux episodes in healthy subjects.66
Clinical trial experience with TLOSR inhibition
Given the preclinical data summarised above, the concept of reflux inhibition through suppression of the TLOSR reflex was taken forward for further clinical development by three independent initiatives: lesogaberon by AstraZeneca, arbaclofen placarbil by Xenoport and ADX10059 by Addex Pharmaceuticals. However, the profound dominance of PPIs in the therapeutic arena of GORD greatly complicated the trial design. Should reflux inhibitors be used in the trial as monotherapy or co-therapy along with PPIs? Should clinical response to PPI treatment be an inclusion criterion, an exclusion criterion, or something in between? By what symptom profile should patients be selected for clinical trials? Should patients qualify for clinical trials on the basis of physiological testing implicating TLOSRs as the basis for their symptoms? If so, while taking PPIs or not? Furthermore, while consensus existed among experts in defining these issues, there was no consensus in resolving them. Nonetheless, the outcome of the trials must be weighed in light of the way in which these problems were dealt with.
The most robust development programme was for lesogaberan, which was tested in two double-blind, placebo-controlled, randomised phase II studies as add-on treatment to PPIs. Entry criteria were that patients experience continuing GORD symptoms despite 6 weeks of continuous PPI treatment at approved doses. Eligibility was based on upper gastrointestinal symptoms listed in the Reflux Disease Questionnaire.67 Taking their existing PPI regimen, they needed to report at least 3 days with ‘a burning feeling behind the breastbone’ (heartburn) and/or ‘unpleasant movement of material upwards from the stomach’ (regurgitation) of at least mild intensity; patients with ‘pain in the centre of the upper stomach’ of intensity equal to or greater than that of heartburn, without fulfilling the regurgitation inclusion criteria, were excluded. No endoscopy or physiological testing was performed.
In the first study, patients were randomised to either lesogaberan or placebo for 4 weeks.68 A positive response was defined as no more than one mild episode of heartburn or regurgitation of no more than mild intensity in the past 7 days. At the end of the study, the lesogaberan group had a significantly larger proportion of responders than the placebo group (16% vs 8%). The number of symptom-free days was larger for patients taking lesogaberan than for the placebo group for both heartburn (37% vs 23%) and regurgitation (38% vs 25%). Adverse events of mostly mild to moderate intensity (mainly diarrhoea, transient episodes of paraesthesia, nausea, fatigue) were reported in 45% of patients receiving lesogaberan compared with 37% in the placebo group, indicating that the drug was well tolerated.
In the second study, entry criteria were slightly different and higher lesogaberan dosages were evaluated in 661 patients.69 To qualify, patients needed to recall having heartburn or regurgitation of at least moderate intensity for at least 3 of the past 7 days while taking their ‘individually optimised’ PPI regimen. Treatment response was defined as having ‘at least 3 additional days of no more than mild symptoms on average per week’ during treatment compared with baseline. Response rates were 21%, 26%, 24% and 26% for the lesogaberan 60, 120, 180 and 240 mg doses, respectively and 18% for placebo. While these changes were significant, they corresponded to less than 1 extra day a week of no more than mild symptoms and were deemed insufficient to be clinically important. Six patients taking lesogaberan developed reversible transaminitis, with alanine transaminase levels more than five times the upper limit of normal.70 The results of these two trials led to the termination of the development programme for lesogaberan.
Unlike lesogaberan, arbaclofen was evaluated as monotherapy for GORD. In a first, proof-of-principle study, the reflux-inhibitory effect of single doses of arbaclofen versus placebo were physiologically tested in 44 patients who were required to have at least 20 reflux episodes on impedance/pH monitoring while lying in a right lateral decubitus position after ingesting a high fat standardised meal. Each participant was studied with one dose of arbaclofen and placebo. Of note, 336 patients meeting the symptom burden entry criteria (GORD symptoms at least three times a week, concomitant PPI use not specified) were screened to identify 58 patients suitable for randomization, amounting to 83% screening failures.71 The primary outcome of the study was the number of reflux episodes recorded by pH-impedance monitoring during a 12 h period after arbaclofen or placebo treatment during which two high-fat meals were consumed. Arbaclofen significantly reduced the number of reflux episodes from 60.9 for placebo to 50.5 for all doses of arbaclofen (17% reduction). The reduction in heartburn events during the 12 h period was also significant (12.9 vs 16.7 for placebo).
This led to a larger subsequent study of 156 patients with GORD with heartburn and/or regurgitation on ≥3 days a week. Participants either had no history of PPI use or a history of at least partial response to PPI treatment. Regardless, patients took no PPIs for 2 weeks before randomization, and arbaclofen (20, 40 mg or 60 once daily, 30 mg twice daily) was tested as monotherapy against placebo for 4 weeks.72 The primary outcome variable was change from baseline in the weekly frequency of heartburn over 4 weeks of treatment; arbaclofen was found to be no better than placebo in achieving this. However, in an exploratory subgroup analysis, it was shown that arbaclofen was effective in the PPI-responsive subgroup but not in the PPI-naïve group, which was characterised by a very high placebo-response rate. The percentage of PPI-responsive patients reporting complete relief of heartburn during the last week of treatment was higher in each arbaclofen treatment group with the largest effect in the 30 mg twice-daily group (50% of days vs 6% for placebo). However, a large phase IIB study (as yet unreported) failed to confirm this finding and further development of arbaclofen stopped.
The third putative reflux inhibitor to consider is ADX10095, a selective mGluR5 negative allosteric modulator. The clinical strategy for these trials was similar to that of arbaclofen with an interesting twist. It, too, was studied as monotherapy in patients with GORD characterised by their responsiveness to PPIs, but rather than seeking partial responders, complete responders were studied after having been withdrawn from PPI treatment. In a first, proof-of-concept study, two groups of 12 patients with GORD underwent 24 h pH-metry on 2 consecutive days following treatment with placebo or ADX10095 (50 or 250 mg three times daily).73 Standardised high-fat meals were provided for breakfast, lunch and supper and patients followed a regimented activity protocol. The primary efficacy variable was the percentage of time with an oesophageal pH <4; comparison of ADX10059 with placebo showed that this was achieved with the 250 mg, but not the 50 mg dose.
These findings were confirmed in larger randomised clinical trial involving 103 similarly characterised patients with GORD.74 Two weeks of treatment with 120 mg ADX10059 twice daily as monotherapy showed a significant increase in GORD symptom-free days and heartburn-free days, a reduction in antacid use and an improvement of total symptom score compared with placebo. The mean number of GORD symptom-free days improved by approximately 2 days, from 0.5 days at baseline to 2.5 days at week 2 in the treatment group compared with an improvement of approximately 1 day from 0.7 days at baseline to 1.7 days at week 2 in the placebo treatment group. By contrast, when ADX10059 was used as add-on treatment to PPIs (trial published only in abstract form), this primary end point was not met, emphasising the importance of this detail in study design.75 However, despite good safety and tolerability in short-term trials, longer-term testing for a parallel indication for migraine headache encountered an unacceptably high incidence of increased hepatic transaminase and the compound was withdrawn from further development.76
Summary and future directions
In summary, the development of reflux inhibitors is a classic example of a bench-to-bedside development project that did not meet expectations. The foundations of the effort, description of the physiology of TLOSRs as an important mechanism of reflux, logically led to attempts at pharmacologically inhibiting this reflex. Preclinical models and pilot data from healthy volunteers and selected patients offered promising results. However, the therapeutic gain observed in patients with GORD was rather small and even difficult to demonstrate. Consequently, these findings together with hints of hepatotoxicity in some cases have left us with no active development initiatives in this domain.
Might this have turned out differently? Were these results a consequence of flawed study design…or were they a matter of inflated expectations? In retrospect, it seems more a matter of inflated expectations. Consider first the most basic question—in the long shadow of PPIs, what is the real unmet need in GORD therapeutics? Figures 1 and 3 emphasise that the unmet need is in symptom control, not mucosal healing. Furthermore, the problem of unresolved symptoms becomes particularly profound when the causal linkage between target symptoms and reflux is uncertain and controversial. Delving into the domain of refractory symptoms, figure 2 emphasises another concept, that this is not a one-size-fits-all disease. True, TLOSRs are the instigating mechanism for many reflux events, but equally true is that the consequences of those reflux events depend on a multitude of independent variables including central or peripheral hypersensitivity and the anatomical degradation of the OGJ manifest by laxity at the hiatus and hiatus hernia. Furthermore, those reflux symptoms in which physiology is not dominated by abnormal sensitivity or clearance are often mediated by acid, precisely the therapeutic domain dominated by PPIs. All these considerations tend to constrict the target patient population for reflux inhibitor treatment. Clearly, not the message that a pharmaceutical firm faced with huge drug development costs wants to hear.
So, if mainstream reflux disease is ceded to the world of antacids and acid inhibitors, what is the ideal patient population for reflux inhibitor treatment? To answer this, we can learn from the lesogaberan, arbaclofen and ADX10059 studies. In the lesogaberan studies, the study populations, defined by their refractoriness to PPI treatment, were probably enriched with patients with functional heartburn and/or functional dyspepsia. Selection of patients solely based on reflux symptoms will unavoidably result in a heterogeneous and ‘contaminated’ population. Indeed, in a study of patients with GORD symptoms possibly related to gastro-oesophageal reflux assessed using pH-impedance monitoring while on PPI, only 37% were found to have symptoms related to either acid or non-acid reflux.77 Interestingly, the symptoms most commonly associated with weakly acidic reflux were regurgitation and cough. These findings reinforce the fact that while the overall treatment effect may be minimal, the best effect would probably be for regurgitation and burping. Taking this further and acknowledging the difficulty of doing so, the outcome of the lesogaberan trials might have been more impressive if patient selection had been based on positive pH-impedance monitoring rather than on ‘refractory’ heartburn. If so, the ‘baby might have been thrown out with the bath water’.
From the arbaclofen and ADX10059 trials we learn that response to PPI treatment is probably a predictor of response to a reflux inhibitor as monotherapy, particularly if the patients were shown to have an abnormally great number of reflux events by physiological monitoring. However, the magnitude of the reflux inhibition treatment effect is unlikely to exceed that of PPIs. In the end, these observations steer us towards patients troubled by persistent regurgitation despite PPI treatment (probably as add-on treatment) or patients with excessive burping (with or without acid suppressive treatment) as candidates for reflux inhibitors.
In conclusion, there is probably a therapeutic role for TLOSR inhibition but it is not broadly defined ‘refractory disease’, as initially envisioned. Rather, it needs to be disease that is refractory on the basis of TLOSRs and this is a much more finite target population. No reflux inhibitors remain in active development programmes but, hopefully, this is not the end of the story.
Acknowledgments
PJK receives research support from the US Public Health Service (R01 DC00646).
References
Footnotes
-
Competing interests PJK is a paid consultant for AstraZeneca, Eisai, EndoGastric Soultions, Ironwood Pharmaceuticals, Reckitt Benchiser, Torax and Xenoport. He receives grant support from the US National Institute of Health (R01 DC00646) and Reckitt Benchiser. GB serves on an advisory board and speakers bureau for Shire-Movetis. He is a paid consultant for Reckitt Benchiser and Shire-Movetis.
-
Provenance and peer review Commissioned; externally peer reviewed.