Article Text

Abstract
Background/Aims Studies in animals suggest a physiological role for glucagon-like peptide-1-(7–36)-amide (GLP-1) in regulating satiety. The role of GLP-1 in regulating food intake in man has, however, not been investigated.
Subjects—Sixteen healthy male subjects were examined in a double blind placebo controlled fashion.
Methods The effect of graded intravenous doses (0, 0.375, 0.75, and 1.5 pmol/kg/min) of synthetic human GLP-1 on food intake and feelings of hunger and satiety was tested in healthy volunteers.
Results Graded GLP-1 infusions resulted in a dose dependent reduction in food intake (maximal inhibition 35%, p<0.001 vcontrol) and a similar reduction in calorie intake (32%; p<0.001). Fluid ingestion was also reduced by GLP-1 (18% reduction, p<0.01). No overt side effects were produced by GLP-1, but subjects experienced less hunger and early fullness in the period before a meal during GLP-1 infusion at the highest dose (p<0.05).
Conclusions Intravenous infusions of GLP-1 decrease spontaneous food intake even at physiological plasma concentrations, implying an important role for GLP-1 in the regulation of the early satiety response in humans.
- glucagon-like peptide-1
- satiety
- food intake
- hunger and fullness score
Abbreviations
- GLP-1
- glucagon-like peptide-1
- CCK
- cholecystokinin
Statistics from Altmetric.com
The physiological mechanisms that produce satiety after food intake have not yet been defined. Several peptides secreted from the gastrointestinal tract during eating have been shown to suppress food intake if given before meals.1-3 During recent years, the role of the preabsorptive release of gut peptides (especially cholecystokinin (CCK), bombesin-like peptides, and glucagon-like peptides) in the production of meal-ending satiety has been extensively investigated in animals.3-11
CCK and bombesin-like peptides have also been studied in humans.9 ,10 CCK, the first gut peptide proposed to act as a satiety signal,4 has received the major share of interest in human studies to date, with a dozen reports in the literature.
Glucagon-like peptide-1 (GLP-1), a biologically active product of the post-translational processing of the prohormone proglucagon, is released from enteroendocrine L-cells from the distal gut in response to food intake.12-14 Oral glucose is a stimulus for GLP-1 release, whereas intravenously applied glucose has no effect on endogenous GLP-1. Unexpectedly, later experiments in rats showed that GLP-1 reduced food intake in rats if administered intracerebroventricularly, but had no effect when given peripherally.8 Additional experiments with a specific GLP-1 receptor antagonist that acts specifically to block endogenous peptide and thus affects only physiologically active circuits showed that blockade of endogenous GLP-1 caused healthy already satieted animals to eat more; in fact, the animals more than doubled their food intake. The authors suggested therefore that GLP-1 is a physiological satiety factor.8 The effects of GLP-1 on food intake in humans are not known. Therefore the present study was designed to investigate the effects of intravenous infusions of synthetic human GLP-1 on food intake, meal duration, satiety, and feelings of fullness in healthy male subjects.
Materials and methods
SUBJECTS
A randomised double blind four period latin square design was carried out in 16 healthy men aged 23.6 (0.5) years. The weight of all subjects was within the normal range considering their age, sex, and height.
Each subject gave written informed consent for the study. The protocol was approved by the human ethical research committees of the University Hospitals of Basel and Aarau. Before being accepted, participants were required to complete a medical interview, receive a full physical examination, and participate in an initial laboratory screening. None were taking any medication or had a history of food allergies, disturbances of carbohydrate tolerance, or dietary restrictions.
DOSE-RESPONSE CURVE TO GLP-1
Four treatments, separated by at least seven days, were performed in 16 subjects. The treatments were identical in design (fig 1) except for the intravenous infusion (5% glucose as placebo control or one dose of GLP-1); the order of the experiments was randomised. An identical standard meal was presented to the subjects on each occasion. The meal consisted of orange juice as an appetiser (480 kcal/l), ham sandwiches (60 g bread, 10 g butter, 25 g ham; 266 kcal per sandwich), more orange juice and chocolate pudding (172 kcal/100 g), and coffee with cream and sugar (coffee could be sweetened if desired; therefore both cream and sugar were optional: 12 g cream = 20 kcal, 4.5 g sugar = 18 kcal). No additional food or fluid was allowed during the study. At the end of the experiment, the amount of food eaten and the amount of fluid ingested were measured from which the total calorie intake (food and fluid intake) was calculated.

Daily time course of procedures.
Subjects were free to eat and drink as much as they wished, but the order of food intake had to follow the above schedule. To reduce the participants’ awareness of the amount of food being provided, food was served in excess.
On the day of the experiment, the subjects ate breakfast if this was their normal custom, but no snacks were allowed after 8 00 am. At 12 00 noon, an intravenous infusion of 5% glucose or one dose of synthetic GLP-1 (0.375, 0.75, or 1.5 pmol/kg/min, dissolved in 5% glucose solution) was started and continued for the duration of each experiment. Infusions were delivered by ambulatory infusion pumps through a Teflon catheter inserted into a forearm vein. Participants were able to sit, eat, stand, and walk comfortably while receiving infusions. At 60 minutes after the start of the respective infusion, the test meal was presented and participants were invited to eat and drink as much as they liked.
Beginning at 12 00 noon, the subjects scored their subjective feelings of hunger and fullness at 15 minute intervals throughout the experiments using a visual analogue scale of 0–10 and indicated the scores on a questionnaire. The scales and scores were designed as previously described.15-17 For example, a score of 0 for hunger indicated the subject was not hungry at all, 2 indicated slightly hungry, 5 indicated moderately hungry, 8 indicated very hungry, and 10 indicated absolutely ravenous.
The quantity of food eaten and volume of fluid drunk were measured. The time taken to complete the meal was also measured. From these observations, the average rate of food and fluid intake as well as the calorie intake could be calculated. In the periods before and after eating, blood was drawn at regular intervals in ethylenediaminetetraacetic acid tubes containing aprotinin (1000 KIU/ml blood) for glucose and hormone determinations. Adverse effects were assessed by the attending physician through close observation of the participants; in addition, after each experiment and after all tests had been completed, participants were asked whether they had experienced any adverse effects.
INFUSIONS
The GLP-1 infusions were prepared from a freeze dried synthetic powder. GLP-1 was purchased from Bachem (Bubendorf, Switzerland). The peptide was dissolved in 5% glucose containing 0.5% human serum albumin and prepared under aseptic conditions by the University of Basel Hospital Pharmacy. Aliquots of 50 μg/5 ml were stored at −20°C. Infusion solutions were prepared by diluting appropriate amounts of GLP-1 with 5% glucose containing 0.1% human serum albumin. Control solutions contained albumin in 5% glucose alone; they were indistinguishable in appearance from GLP-1 infusions.
The person in charge of the experiments was unaware of the respective treatment, thereby making it possible to deliver treatments in a double blind fashion.
PLASMA HORMONE AND GLUCOSE DETERMINATIONS
Glucose concentrations were measured by the hexokinase method. Plasma concentrations of insulin, CCK, GLP-1, and leptin were measured as depicted in fig 1. All hormone concentrations were determined by specific radioimmunoassay systems. For insulin and leptin concentrations, commercially available test kits were used.
Plasma immunoreactive CCK concentrations were measured by a sensitive radioimmunoassay17 based on the antiserum OAL656 which recognises the sulphated tyrosine residue of CCK8, but has no relevant cross reactivity with sulphated gastrin (<1%) and does not cross react with unrelated gastrointestinal peptides.18 GLP-1 was measured as previously described.1 ,19 ,20 The detection limit of the GLP-1 assay was 2 fmol/tube. The assay does not have any significant cross reactivity with gastric inhibitory peptide, pancreatic glucagon, glicentin, oxyntomodulin, or GLP-2. Intra-assay and inter-assay coefficients of variation were 3.4 and 10.4% respectively.
STATISTICAL ANALYSIS
The amount of food eaten and the amount of fluid drunk, the corresponding energy intake, and the duration of food consumption were compared between the four treatments by one way analysis of variance using the general linear model procedure of the SAS software package.21 In the event of significant differences, analysis of variance was followed by the Newman-Keuls multicomparison test for pairwise comparisons.22 The same statistical procedure was used to analyse the results of GLP-1 induced changes in plasma hormone concentrations using area under the curve analysis.
Scores for hunger and fullness were compared at the different time points before and after the meal between the different treatments using multiple paired t tests with Bonferroni correction.22
Results
EFFECT OF GRADED INFUSION OF GLP-1 ON FOOD INTAKE
Intravenous infusion of graded doses of synthetic human GLP-1 dose-dependently reduced the amount of food eaten and the amount of fluid consumed (p<0.001 and p<0.01 respectively; table 1). The maximal reduction in food consumption with the highest dose of GLP-1 (1.5 pmol/kg/min) amounted to 35% resulting in a decrease in calorie intake of 32% (p<0.001; table 1).
Effect of graded doses (pmol/kg/min) of human glucagon-like peptide-1 (GLP-1) or 5% glucose on eating behaviour in 16 healthy male subjects
Meal duration during GLP-1 infusions was also dose-dependently decreased compared with that with placebo and reached statistical significance at the highest dose (p<0.05). None of the participants reported any abdominal discomfort or side effects during any infusion of either dose. Furthermore, when questioned at the end of each experiment, none reported any adverse reaction.
EFFECT OF GLP-1 ON EATING BEHAVIOUR
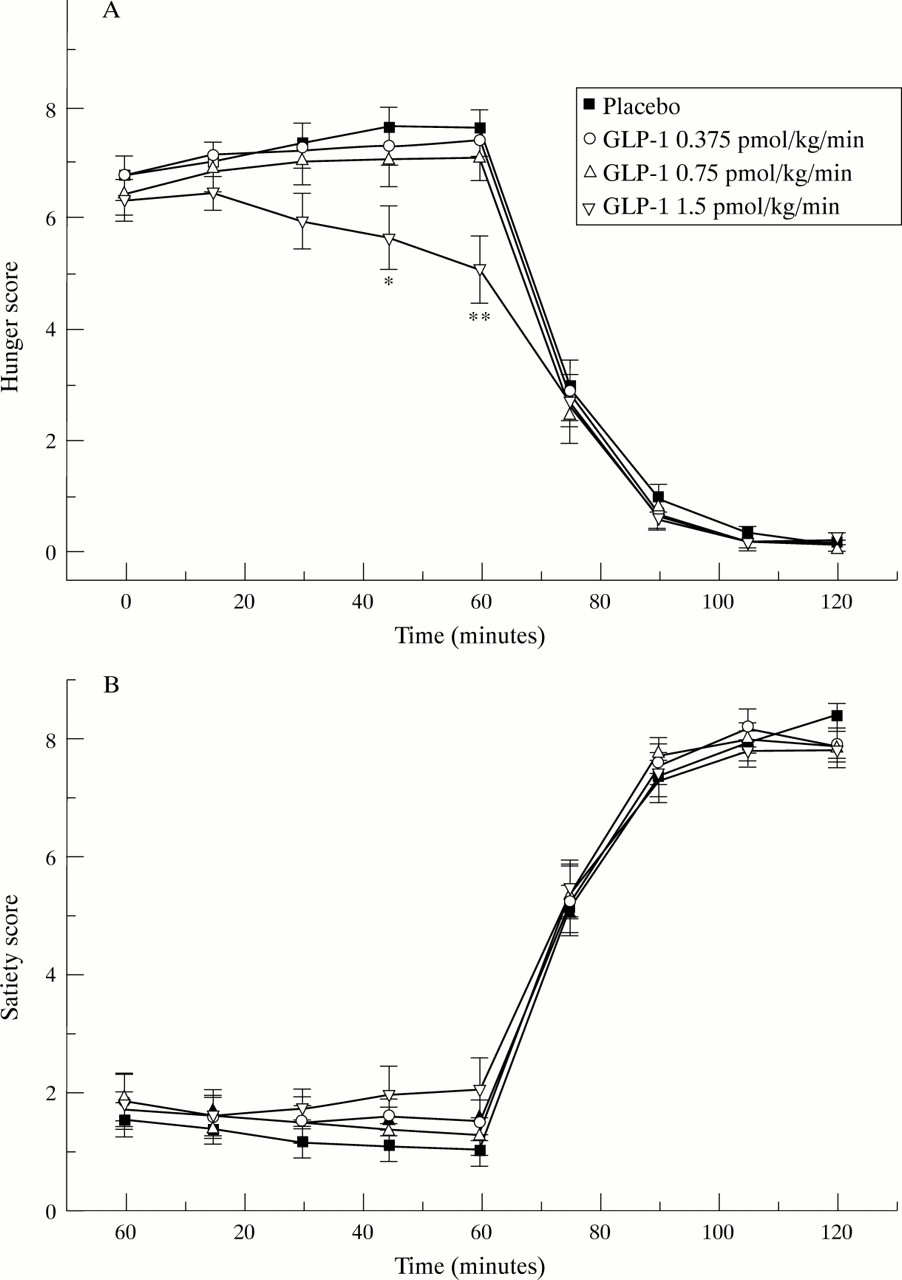
Subjects experienced a reduced degree of hunger and a concomitant feeling of fullness in the period before the meal with increasing doses of GLP-1 infusions. However, the difference reached statistical significance only for the highest dose of GLP-1 with respect to hunger feelings (p<0.05–0.01; fig 2). No statistical differences were observed thereafter in hunger or fullness scores with any treatment after meal intake.

Subjective sensations of hunger (A) and fullness (B) experienced by healthy male subjects before and after food intake during intravenous infusion of 5% glucose (placebo) or one dose (0.375, 0.75, or 1.5 pmol/kg/min) of human glucagon-like peptide-1. Results are expressed as mean and SEM (n = 16). *p<0.05, **p<0.01 v control.
EFFECT OF GLP-1 ON HORMONE LEVELS
Graded doses of exogenous GLP-1 produced dose dependent increases in plasma GLP-1 concentrations (fig 3). The two lower doses produced plasma levels of 3.7 (0.6) and 5.0 (0.6) pmol/l respectively, which can be considered physiological postprandial plasma levels, whereas the highest dose of GLP-1 resulted in supraphysiological plasma concentrations.19 ,20

Immunoreactive glucagon-like peptide-1 (IR-GLP-1) measured in the plasma (pmol/l) in response to graded doses of intravenous GLP-1 or placebo in the preprandial period. Data are expressed as mean and SEM.
In the control experiment, glucose levels and insulin concentrations remained stable in the preprandial period. GLP-1 induced a dose dependent short lasting increase in blood glucose and plasma insulin concentrations; the results are depicted as an insulinogenic index in fig 4. Because changes in plasma glucose are invariably associated with changes in plasma insulin, the insulinogenic index, calculated as the quotient insulin/glucose, more appropriately reflects insulin release.20 Plasma CCK concentrations remained unaltered by any dose of GLP-1 in the preprandial period (fig 4). Finally, leptin levels did not change either with any dose of GLP-1 administered or after food intake (fig 5).

Insulinogenic index (insulin/glucose) and plasma cholecystokinin (CCK) levels (pmol/l) in response to graded doses of glucagon-like peptide-1 (GLP-1) or placebo in the premeal period. Data are expressed as mean and SEM.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leptin concentrations(ng/ml) measured in plasma in response to graded doses of intravenous glucagon-like peptide-1 (GLP-1) or placebo. Data are expressed as mean and SEM.
Discussion
In animals, expression of GLP-1 receptors has been found in the hypothalamus, brainstem, and periventricular area, but not in the cortex.23 Furthermore, GLP-1 receptors have been found in the endocrine pancreas,24 adipose tissue,25and stomach.26 ,27 Moreover, nerves containing GLP-1 have been identified in the brain.28 ,29 As GLP-1 receptors have been shown to be present at sites at which administration of exogenous GLP-1 appears to cause satiety, experiments are now required to determine if the satiety effect of GLP-1 is physiological, and, if so, whether it is a major satiety factor. Recent animal data have provided experimental evidence that GLP-1 can function as a mediator of food induced satiety in rats and mice provided that it is administered directly into the brain. Injection of GLP-1 into the cerebral ventricles of fasted rats inhibited feeding, and this effect was blocked by the GLP-1 receptor antagonist exendin.9-39Furthermore, administration of exendin9-39 alone doubled food intake in satiated rats.8 ,14 These findings prompted the authors to suggest that GLP-1 is a potent physiological regulator of satiety. These initial observations were confirmed by Scrocchi and co-workers30 in normal mice; along this line of investigation, the authors postulated that GLP-1 is a physiological regulator of blood glucose and satiety. To ascertain the physiological importance of the peptide as a regulator of feeding behaviour, they generated mice with a targeted disruption of the GLP-1 receptor gene (GLP-1R). These GLP-1R−/− mice developed normally but exhibited increased levels of blood glucose following an oral glucose challenge together with attenuated levels of circulating insulin.30However, no evidence for abnormal feeding behaviour was observed in GLP-1R−/− mice, so the biological importance of GLP-1 as a neuropeptide remains controversial.
Based on this information, the purpose of this study was to examine the effect of intravenous administration of graded doses of synthetic human GLP-1 on eating behaviour and satiety in healthy male subjects in order to assess a possible physiological role for the peptide in the regulation of food intake. We were especially interested to test whether intravenous administration of the peptide was able to induce satiety effects. This idea was derived from previous studies showing that several peptides normally secreted from the gastrointestinal tract during eating are able to suppress food intake if given before meals.1-3 The results of the present study clearly show that a short term satiety effect can be induced by peripherally infused GLP-1; the results lend further support to the hypothesis that GLP-1 is an endogenous signal involved in the control of food intake in man. The lack of specific GLP-1 receptor antagonists that could be given to humans prevents us for the moment from deciding whether the effects produced by the exogenous administration of GLP-1 (as used in this study) are true physiological effects. However, we have clearly shown that GLP-1 decreases food intake; some of the effects were seen at plasma GLP-1 concentrations observed after a meal.19 ,20 ,31 Along these lines of investigation, Flint and co-workers32 have recently published a similar study. They examined the effect of a single dose of GLP-1 on subjective appetite sensations after an energy fixed breakfast and on spontaneous energy intake at an ad libitum lunch. GLP-1 enhanced satiety and induced early fullness compared with placebo. Furthermore, GLP-1 reduced energy intake. From these observations and our present results, we infer that the effects represent physiological effects of GLP-1.
The mechanism by which GLP-1 inhibits food intake is not clear and could possibly be the result of different actions. Does it mediate its effect directly by binding to peripheral or central receptors or does it act indirectly by releasing other satiety peptides? The questions cannot be answered at the present time as a demonstration of a direct action of GLP-1 would require experiments with a selective GLP-1 receptor antagonist specifically blocking endogenous GLP-1. Is the effect peripheral or mediated by central receptors? Does GLP-1 act as a hormone and does it cross the blood-brain barrier? Turtonet al 8 showed a potent effect on food intake in rats when GLP-1 was administered intracerebroventricularly, whereas intraperitoneal application of the peptide did not have any effect. This observation suggests but does not prove that the action of GLP-1 on food intake is mediated by central rather than peripheral mechanisms. On the other hand, there is experimental evidence to show that intraperitoneal injections of supraphysiological loads of GLP-1 into rats are insufficient to even lower blood glucose levels, indicating rapid degradation of the peptide in the abdominal cavity (P Berghöfer and B Göke, unpublished data). Also, there are experimental data showing that the effect of gut peptides such as CCK in regulating food intake is mediated through stimulation of afferent fibres of the vagus nerve.33 Along this line of argument, Wettergren and co-workers34 have shown that the inhibitory effects of GLP-1 on gastric acid secretion in humans depend on an intact vagal innervation of the stomach as the effect is lost after vagotomy.
Does GLP-1 inhibit food intake by stimulating the release of other peptides known to be involved in the regulation? In the present study, we have measured the effect of GLP-1 on CCK secretion and on plasma leptin concentrations, two peptides that have received a major share of attention with respect to this particular question. The results presented in this study show that CCK is not released after administration of graded doses of GLP-1 before the meal making it unlikely that CCK is the mediator of this response. Leptin, the product of the adipose specific ob gene, regulates food intake and energy expenditure in animals.35-37 No effect of leptin on short term satiety has been shown in humans as yet, but it has been proposed that the postprandial increase in GLP-1 stimulates adipose tissue to secrete leptin and suppress food intake. In our study, plasma leptin concentrations did not change even during a pharmacological GLP-1 infusion (fig 5), confirming the results of Shalev et al.38 The latter finding indicates that food intake suppression induced by GLP-1 is not mediated by leptin. Somatostatin, which has also been proposed to act as a satiety signal, was not measured here, but a previous study has evaluated the effect of intravenous GLP-1 infusion on plasma somatostatin concentration in healthy volunteers and did not show any alteration.39 GLP-1 is associated with gastric emptying in humans19 ,20; it is therefore possible that intravenous administration of GLP-1 activates neural circuits that may cause sensations of fullness by delaying gastric emptying. Additional experiments would be required to test whether changes in gastric function play a role in the suppression of food intake after GLP-1 infusion.
Finally, a non-specific action of GLP-1 can be excluded because no overt side effects were observed in this study. It is noteworthy that GLP-1 reduced food intake to a larger extent than other gut peptides under similar experimental conditions: the maximal reduction in the amount of food eaten was 35% with the highest dose of GLP-1 compared with a maximal effect of gastrin releasing peptide at a high pharmacological dose of 19%11 or a maximal dose of CCK (causing side effects in some volunteers) of 13%.9 A recent study has shown that therapeutic plasma levels of GLP-1 in healthy volunteers were achieved after a single buccal tablet.40 Although the bioavailability of buccal GLP-1 was low, the study indicates a potential therapeutic route of administration for GLP-1. Further studies are required to assess whether GLP-1 could provide a new therapeutic approach to the reduction of food intake in patients with non-insulin dependent diabetes mellitus who are overweight and patients with obesity.
In conclusion, we have shown that graded doses of human GLP-1 that produce plasma GLP-1 concentrations within the physiological range reduce intake of food in non-obese healthy male subjects. The mechanism of action requires clarification. Further investigation is needed to define the physiological role of GLP-1 in the control of human food intake and also to assess its therapeutic potential in reducing food consumption.
Acknowledgments
This work was supported by a grant from the Swiss National Science Foundation (grant No 3200–40604.94/1).
Abbreviations
- GLP-1
- glucagon-like peptide-1
- CCK
- cholecystokinin