Article Text

Abstract
Background and aims: Transient lower oesophageal sphincter relaxations (TLOSRs) are the major cause of gastro-oesophageal reflux in normal subjects and in most patients with reflux disease. The gamma aminobutyric acid (GABA) receptor type B agonist, baclofen, is a potent inhibitor of TLOSRs in normal subjects. The aim of this study was to investigate the effect of baclofen on TLOSRs and postprandial gastro-oesophageal reflux in patients with reflux disease.
Methods: In 20 patients with reflux disease, oesophageal motility and pH were measured, with patients in the sitting position, for three hours after a 3000 kJ mixed nutrient meal. On separate days at least one week apart, 40 mg oral baclofen or placebo was given 90 minutes before the meal.
Results: Baclofen reduced the rate of TLOSRs by 40% from 15 (13.8–18.3) to 9 (5.8–13.3) per three hours (p<0.0002) and increased basal lower oesophageal sphincter pressure. Baclofen also significantly reduced the rate of reflux episodes by 43% from 7.0 (4.0–12.0) to 4.0 (1.5–9) per three hours (median (interquartile range); p<0.02). However, baclofen had no effect on oesophageal acid exposure (baclofen 4.9% (1.7–12.4) v placebo 5.0% (2.7–15.5)).
Conclusions: In patients with reflux disease, the GABAB agonist baclofen significantly inhibits gastro-oesophageal reflux episodes by inhibition of TLOSRs. These findings suggest that GABAB agonists may be useful as therapeutic agents for the management of reflux disease.
- lower oesophageal sphincter
- oesophageal motility
- baclofen
- gastro-oesophageal reflux disease
- LOS, lower oesophageal sphincter
- TLOSR, transient LOS relaxation
- GABA, gamma amino butyric acid
- GABAB GABA receptor type B
Statistics from Altmetric.com
- LOS, lower oesophageal sphincter
- TLOSR, transient LOS relaxation
- GABA, gamma amino butyric acid
- GABAB GABA receptor type B
Tonic contraction of the lower oesophageal sphincter (LOS) is the principal factor preventing the reflux of gas tric contents into the oesophagus. Transient LOS relaxation (TLOSR) is the major mechanism underlying reflux in normal subjects and patients with reflux disease.1 Control of reflux through pharmacological inhibition of TLOSRs is a conceptually attractive approach to the treatment of reflux disease.
Several pharmacological agents have been shown to inhibit triggering of TLOSRs. These include atropine,2–4 cholecystokininA receptor antagonists,5–7 nitric oxide synthase inhibitors,8 and morphine.9 The most promising class of agents identified to date for the reduction in the rate of TLOSRs however is gamma amino butyric acid receptor type B (GABAB) agonists. GABA is a major inhibitory neurotransmitter within the central nervous system, and GABAB receptors are present at many sites in both the central and enteric nervous systems. Inhibitory GABAB receptors are present on vagal afferent terminals in the dorsal medulla10 and have been shown to inhibit transmitter release in vagal nuclei.11 Such actions are thought to underlie suppression of reflexes controlling respiration12 and gastric relaxation.13 GABAB receptors have also been demonstrated on gastric mechanoreceptors.14 Baclofen, the prototype agent which is currently used primarily for the management of spasticity, was first shown to be a potent inhibitor of TLOSRs in dogs.15 These findings have been subsequently confirmed in ferrets.16 We have shown recently that single oral doses of baclofen inhibit TLOSRs and gastro-oesophageal reflux episodes by over 50% in healthy human volunteers.17
Currently, there are no reported studies of the effect of baclofen on TLOSRs and gastro-oesophageal reflux in patients with reflux disease. Compared with healthy subjects, patients with reflux disease exhibit greater heterogeneity in the mechanisms of reflux and an important minority of patients, predominantly those with severe oesophagitis, appear to reflux largely during periods of absent basal LOS pressure.18,19 It is unclear whether patients with reflux disease would respond to a GABAB agonist in a similar fashion to normal subjects. Therefore, the aim of this study was to investigate the effects of baclofen on LOS function and gastro-oesophageal reflux in patients with reflux disease.
METHODS
Subjects
Studies were performed in 20 patients (15 men, five women; aged 31–73 years (median 56.5)). Body weight ranged from 65 to 102 kg (mean (SEM) 83.68 (2.65) kg). Thirteen patients had Hetzel grade 2 oesophagitis,20 five had grade 3, and two had grade 4 oesophagitis that had been documented by endoscopy within six months before the study. Nine patients had hiatus hernias >3 cm in length. Patients who had undergone previous upper gastrointestinal surgery were excluded. Also, because baclofen lowers the threshold for seizures, patients with a family history of epilepsy were also excluded. Medications that affect gastrointestinal motility and/or acid secretion were stopped for at least four days before each study day. Each patient gave written informed consent, and the protocol was approved by the research ethics committee of the Royal Adelaide Hospital.
Recording methods
Oesophageal manometry was performed with a multilumen manometric assembly (Dentsleeve Pty Ltd, Wayville, South Australia). Lower oesophageal sphincter pressure was measured with a reverse perfused sleeve sensor.21 Gastric pressure was recorded via a side hole located 1 cm distal to the sleeve sensor. Side holes spaced at 3 cm intervals starting at the proximal margin of the sleeve sensor monitored pressure at seven sites along the oesophageal body, and the side hole in the pharynx recorded swallowing. An infusion port was located 11 cm above the sleeve sensor for rapid injection of air boluses into the mid-oesophagus. Each lumen was perfused with degassed distilled water at 0.15 ml/min by a low compliance manometric infusion pump. Oesophageal pH was measured with an antimony electrode (Synectics Medical AB, Stockholm, Sweden) positioned 5 cm above the proximal margin of the LOS.
Data were digitised with a Macintosh computer (Apple Computer Inc., Cupertino, California, USA). The digitised signals were displayed, stored, and analysed using AcqKnowledge software (Biopac Systems, Goleta, California, USA).
Symptom assessment
In order to screen for drug side effects, symptoms of anxiety, sleepiness, desire to eat, hunger, nausea, fullness, dizziness, and tiredness were measured with a validated 100 mm visual analogue scale22 during the measurement period.
Study protocol
The study was of a randomised placebo controlled crossover design. Baclofen 40 mg orally and placebo were studied on separate days at least one week apart. Patients were studied after an overnight fast. A cannula was inserted into a forearm vein for blood sampling. A baseline blood sample was taken for measurement of growth hormone and plasma baclofen levels after which oral baclofen (40 mg) or placebo was given.
Sixty minutes after drug administration, the manometric assembly and pH electrode were passed via an anaesthetised nostril and positioned so that the sleeve straddled the LOS and the pH electrode was 5 cm above the LOS. Patients were allowed 15 minutes to accommodate to the assembly while in the right lateral position. Primary peristalsis was then assessed in response to 10, 5 ml water swallows, and secondary peristalsis was tested with five 20 ml boluses of air rapidly injected into the mid-oesophagus.23
Patients then sat up and ate a 3000 kJ (750 kcal) soft mixed nutrient meal, consisting of savoury minced meat, mashed vegetables, 150 ml milk, and ice cream. After the meal, patients remained sitting and oesophageal manometric and pH recordings were made for three hours. At the end of the study, primary and secondary peristalsis were reassessed as before while patients were in right lateral position.
Pulse rate and blood pressure were recorded every 30 minutes during the study period. Blood samples were taken before dosing and at 30–60 minute intervals after dosing for measurement of plasma levels of baclofen and growth hormone. Symptoms were assessed as described above.
Data analysis
End expiratory basal LOS pressure was referenced to end expiratory intragastric pressure, and was determined at 10 minute intervals as one minute visual means. TLOSRs were defined according to the criteria published previously.24 LOS relaxations that lasted more than 15 seconds which were associated with a swallow within five seconds before or two seconds after the onset of an LOS relaxation were included as TLOSRs.25,26
The amplitude of oesophageal pressure waves at each recording site and the latency of wave onset between adjacent recording sites was determined for both primary and secondary peristalsis. Peak amplitude was referenced to basal end expiratory intraoesophageal pressure. The onset of the major upstroke of the pressure wave was used as the reference point for determination of wave latency. Mean amplitude was calculated for the two proximal and five distal oesophageal recording sites. Amplitude was calculated for all responses irrespective of whether or not they were classified as peristaltic.
Primary peristalsis was classified as successful if a pressure wave of ≥12 mm Hg at the proximal two oesophageal sites and ≥25 mm Hg at the distal five oesophageal sites progressively traversed all of the oesophageal recording sites. The minimum wave latency that defined peristalsis progression was set at 0.5 seconds, corresponding to a peristaltic velocity of 6 cm/s. Secondary oesophageal motor responses were classified according to the criteria for primary peristalsis.23
Acid reflux episodes were defined as a decrease in oesophageal pH below 4 for at least four seconds or, if basal oesophageal pH was already below 4, as a further decrease in pH of at least 1 pH unit. Infrequently, oesophageal pH drifted downwards during a period of several minutes and dropped below pH 4. These pH drifts were included in the analysis of the duration of oesophageal acid exposure but were not scored as reflux episodes. For analysis of the occurrence of acid reflux during TLOSRs, acid reflux was deemed to have occurred if there was an abrupt drop in pH of at least 1 pH unit. Acid clearance was measured from the time that pH fell below 4 to the time at which oesophageal pH increased above pH 4.
The time of onset of the decrease in oesophageal pH was used as the reference time for analysis of the motor events associated with reflux. For each reflux episode, the mechanism of reflux was determined from the patterns of LOS pressure and oesophageal body activity, and their relationship to swallowing and the occurrence of abdominal straining.18,19 These mechanisms were classified as TLOSR, swallow induced reflux (including multiple swallow),26 absent basal LOS pressure, straining, and non-interpretable when pressures were obscured by movement induced artefacts. The presence or absence of oesophageal body common cavities, a manometric indicator of gastro-oesophageal reflux, was also determined during TLOSRs. The rate of spontaneous swallowing was determined by counting the pharyngeal pressure waves.
Plasma levels of baclofen were measured by AstraZeneca R&D, Mölndal.17 Plasma growth hormone levels were measured by radioimmunoassay.
Statistical analysis
The rate of TLOSRs, proportions of TLOSRs associated with reflux and oesophageal body common cavities, rate of reflux episodes, acid exposure time, mean acid clearance time, and proportion of reflux episodes associated with TLOSRs were determined for each patient. Group data are presented as median (interquartile range) and were analysed with the Wilcoxon signed rank test. All other data are presented as mean (SEM). Paired comparisons of LOS pressures, symptom scores, blood pressure, pulse rate, and growth hormone levels were made using repeated measures analysis of variance (ANOVA; Abacus Concepts Inc, Berkeley, California, USA). All other data were analysed using the paired t test. A p value of less than 0.05 was accepted as indicating statistical significance.
RESULTS
The study protocol was well tolerated and all patients completed both phases of the studies.
Basal LOS pressure
Fasting basal LOS pressure during baclofen (5.1 (0.9) mm Hg) was similar to that during placebo (3.1 (0.6) mm Hg) (fig 1). For the first 90 minutes after the meal, basal LOS pressure was also similar during baclofen (3.9 (0.2) mm Hg) and placebo (3.7 (0.2) mm Hg). However, from 90 to 180 minutes, basal LOS pressure during baclofen (7.9 (0.3) mm Hg) was significantly higher than that during placebo (4.6 (0.3) mm Hg; p<0.005) and overall mean postprandial basal LOS pressure during baclofen (5.8 (0.6) mm Hg) was significantly higher than that during placebo (4.1 (0.7) mm Hg; p<0.02).

Effect of baclofen 40 mg orally on basal lower oesophageal sphincter (LOS) pressure. Data are mean (SEM) for each 10 minute interval. p<0.02 (ANOVA).
Transient LOS relaxations
Overall, during baclofen, there were 193 TLOSRs compared with 334 during placebo. Baclofen significantly reduced the rate of TLOSRs from a median of 15 (13.8–18.3) per three hours to 9 (5.8–13.3) per three hours (p<0.0002) (fig 2). Baclofen had no effect on the likelihood of reflux occurring during a TLOSR. During baclofen, reflux occurred with 53.8% (40.9–67.3%) of TLOSRs compared with 41.5% (25.0–75.5%) during placebo. Baclofen had no effect on the proportion of TLOSRs associated with oesophageal common cavities (baclofen 85.2% (75–100) v placebo 100% (91–100)).

Effect of baclofen 40 mg orally on the rate of transient lower oesophageal sphincter relaxations (TLOSRs) during the three hour postprandial period. Each data point represents an individual patient. Lines connect the two study days for each patient. The short horizontal lines indicate median values. p<0.0002.
Gastro-oesophageal reflux
Individual reflux episodes were scored in only 19 patients because oesophageal pH remained at approximately pH 2 in one patient throughout the three hour postprandial recording period on the placebo day. During baclofen, there were 101 acid reflux episodes compared with 174 during placebo. For the postprandial period as a whole, baclofen significantly reduced the rate of reflux episodes by 43% from 7.0 episodes/three hours to 4.0 episodes/three hours (p<0.02) (fig 3). This effect was significant for the second and third postprandial hours.

Effect of baclofen 40 mg orally on the rate of reflux episodes during the three hour postprandial period. Data are median (interquartile range) for each postprandial hour.
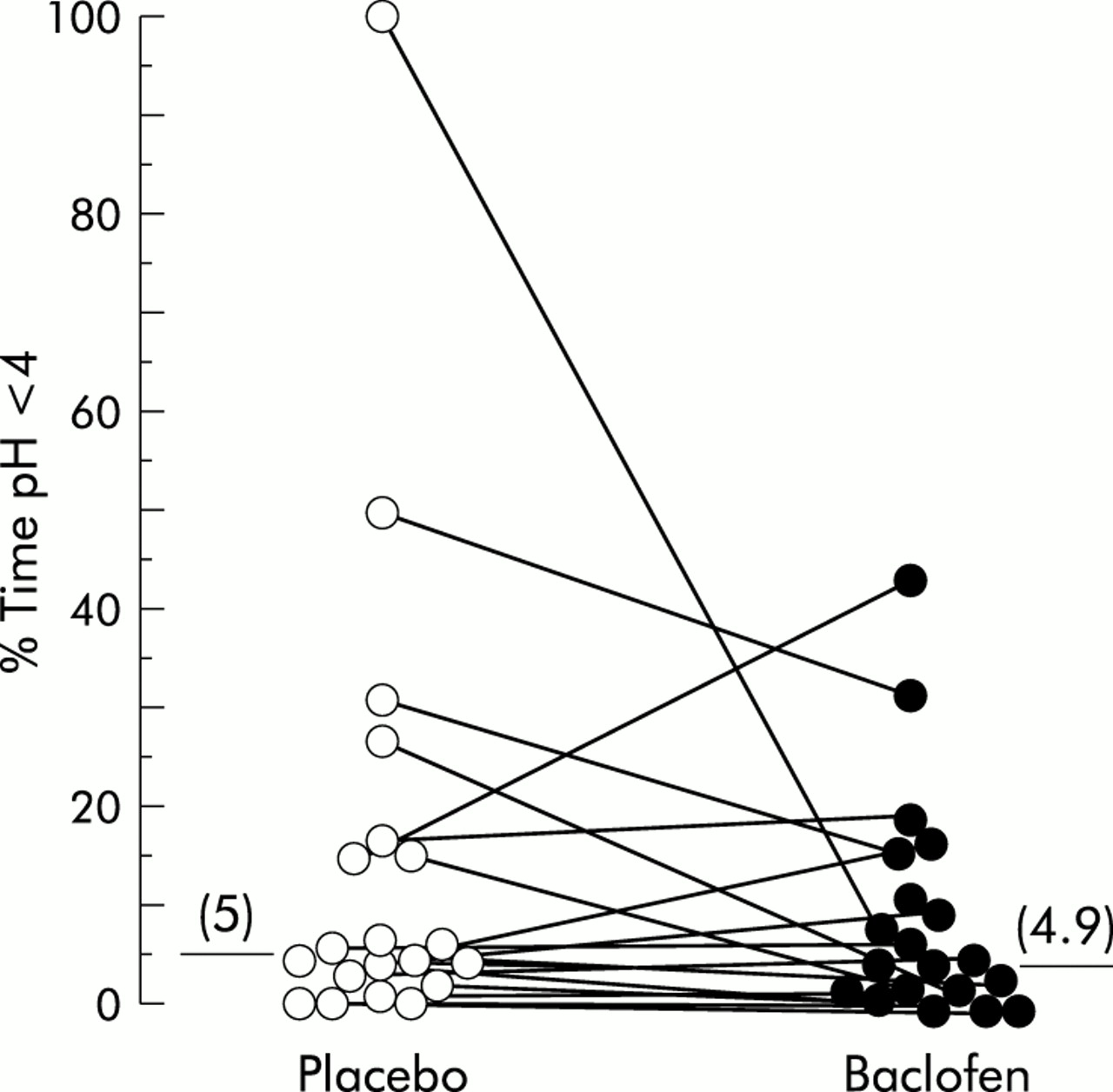
Despite the significant reduction in reflux episodes, baclofen had no significant effect on oesophageal acid exposure. The duration of time that oesophageal pH was <4% during baclofen (4.9% (1.7–12.4)) was similar to that during placebo (5.0% (2.7–15.5)) (fig 4). Oesophageal acid clearance during baclofen (126 s (87–186)) was similar to that during placebo (85 s (57–120)). Oesophageal common cavities occurred with 100% (63.4–100) reflux episodes during baclofen similar to that during placebo (100% (97.5–100)).

Effect of baclofen on oesophageal acid exposure. Data are displayed as individual data points. Horizontal lines indicate median values. Lines connect the placebo and baclofen values for individual patients.
Mechanisms of reflux
On both study days, the majority of reflux episodes occurred during TLOSRs. On a per patient basis, baclofen had no significant effect on the proportion of reflux episodes due to TLOSRs (placebo 81.8% (70.8–86.6), baclofen 93.8% (45–100); p>0.5) (fig 5). However, the total number of reflux episodes that occurred during TLOSRs fell by 44% from 131 on the placebo day to 73 on the baclofen day (p<0.005). There was also a more modest but nevertheless significant fall in the number of reflux episodes that occurred during periods of absent basal LOS pressure (placebo 31 v baclofen 4; p<0.01). Baclofen did not alter the number of reflux episodes that occurred by the other mechanisms of swallow induced LOS relaxation, or straining.
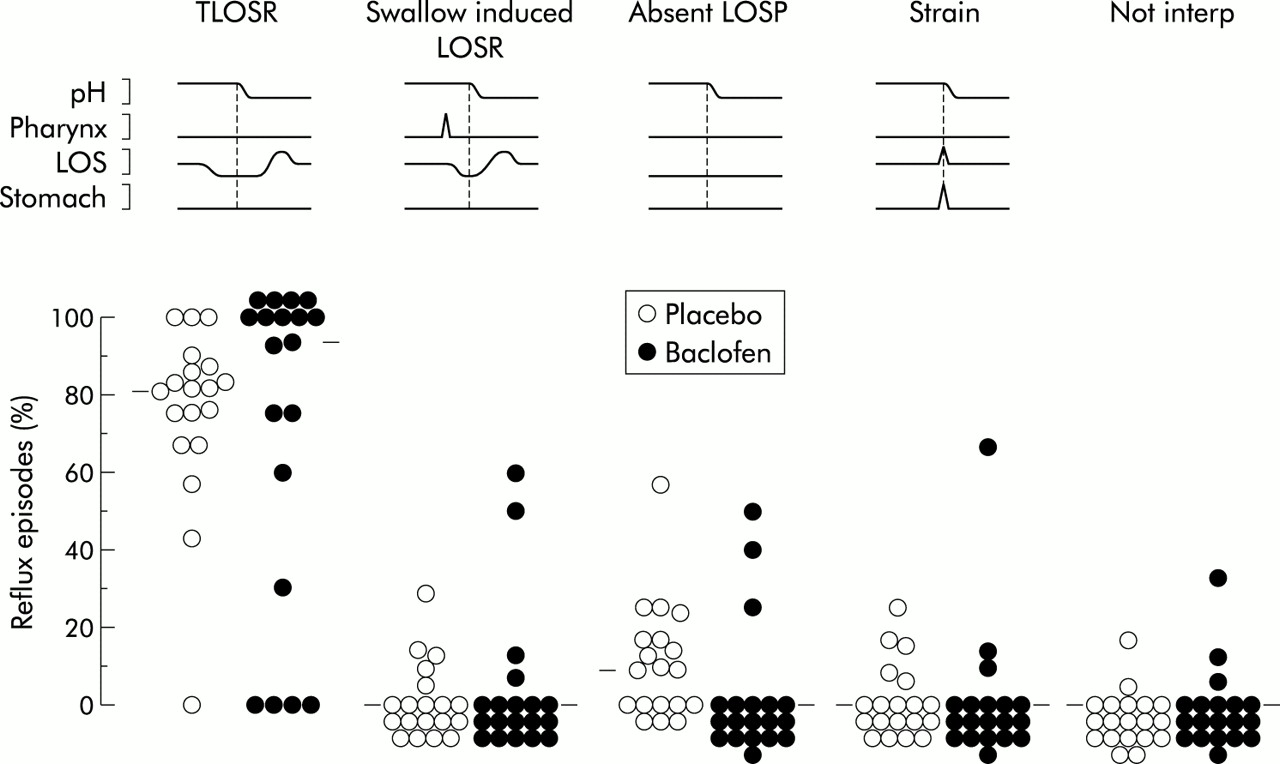
Effect of baclofen on the mechanisms of gastro-oesophageal reflux. Each point represents the proportion of reflux episodes occurring by that mechanism in that patient. Horizontal lines indicate median values. LOS, lower oesophageal sphincter; TLOSR, transient LOS relaxation; LOSP, lower oesophageal sphincter pressure.
Swallowing and oesophageal peristalsis
Baclofen significantly reduced the rate of swallowing from 167 (11.6) to 139 (13.2) per three hours (p<0.05). Baclofen had no significant effect on fasting or postprandial oesophageal peristalsis. The success rates of both primary and secondary peristalsis and distal oesophageal wave amplitude were not affected by baclofen (table 1).
Effect of baclofen on primary and secondary peristalsis
Plasma levels of growth hormone and baclofen
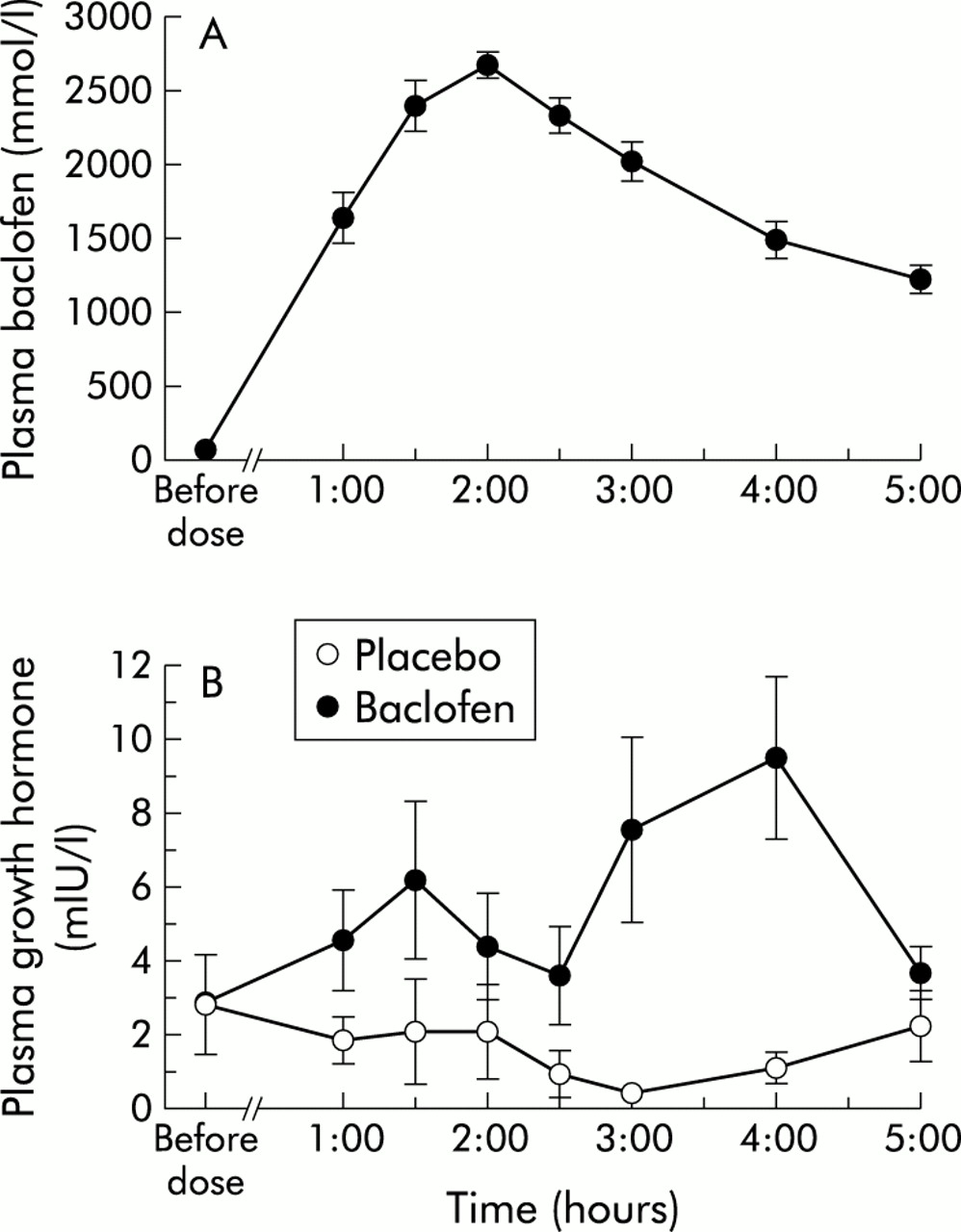
Baclofen increased plasma levels of growth hormone from 2.9 (1.4) mIU/l to a mean peak value of 3.6 (2.7) mIU/l (p<0.0005) (fig 6). Peak levels occurred at about four hours after dosing but the timing varied among subjects. There was no increase in growth hormone on the placebo day. The peak plasma level of baclofen occurred at 120 minutes after dosing (fig 6). Plasma levels had fallen to about one third of peak levels by the end of the study, five hours after dosing.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Plasma baclofen levels (A) and plasma growth hormone levels (B). Data are mean (SEM).
Symptoms and side effects
Over the study period, symptom scores for anxiety, hunger, and desire to eat decreased, and sleepiness, fullness, dizziness, and tiredness increased significantly. There were no overall significant differences in changes in symptom scores between baclofen and placebo.
Vital signs
Baclofen had no effect on blood pressure (baclofen 132 (1)/79 (1) mm Hg, placebo 133 (2)/80 (1) mm Hg) or heart rate (baclofen 68 (1) beats/min, placebo 71 (1) beats/min).
DISCUSSION
TLOSR is the most prevalent mechanism of reflux, and controlling reflux by inhibiting the rate of TLOSRs is therefore physiologically attractive. Recent studies indicate that GABAB receptor agonists are potent inhibitors of TLOSRs, and baclofen is highly effective in normal subjects.17 In patients with reflux disease, the greater heterogeneity of reflux mechanisms, and the presence of other pathogenetic factors such as hiatus hernia and impaired acid clearance, could potentially have a significant impact on the reduction in reflux by inhibition of TLOSRs. To our knowledge, this is the first study to test the effects of baclofen in patients with reflux disease. We demonstrated that baclofen was a potent inhibitor of TLOSRs, reducing the rate by about 40%. This was accompanied by a similar reduction in the rate of reflux episodes.
The reduction in the rate of TLOSRs was significant for each of the three postprandial hours. The magnitude of the reduction however was slightly lower than that seen previously in normal subjects. The reasons for this are not immediately apparent. It has been reported that patients with reflux disease have a higher rate of TLOSRs,9,27 and therefore it might be more difficult to suppress them in this group. Contrary to popular belief, but consistent with previous recent findings in the sitting position,28 we did not find a higher rate of TLOSRs in patients with reflux disease; the rates were almost identical. The lower degree of suppression was also unrelated to differences in the pharmacokinetics of baclofen between the two study groups as plasma levels of baclofen were almost identical to those obtained previously in normal subjects. Patients in this study were substantially older than the normal subjects in our previous study, and growth hormone levels were lower. The latter most likely reflects a primary age related reduction in growth hormone output. However, the possibility that there is an age related downregulation of the GABAB receptor cannot be excluded.
Baclofen also caused a significant increase in basal LOS pressure. A similar but smaller effect has been noted in normal subjects.17 The effect in patients with reflux disease was evident only after the first 90 minutes, but by the end of the monitoring period the increase had reached 100% and was convincingly significant (p<0.02). The reasons for this apparently delayed response are not clear. Perhaps the factors that underlie the postprandial decrease in basal LOS pressure are less easily overcome in patients with reflux disease. Further, the contractile effect of baclofen on basal LOS pressure may have been more easily expressed due to a lower pressure in the reflux patients compared with normal subjects. While the magnitude of the increase was relatively small, it appeared to be functionally important as there was a significant fall in the number of reflux episodes due to absent basal LOS pressure.
The reduction in the rate of TLOSRs was accompanied by a similar reduction (43%) in the rate of reflux episodes. While the effect was not as consistent as the reduction in TLOSRs, the reduction in the rate of reflux episodes was due primarily to a reduction in the rate of those due to TLOSRs with a smaller reduction in those due to absent basal LOS pressure. As with our previous study, there was no change in the proportion of TLOSRs associated with reflux.
The substantial decrease in the rate of reflux episodes was not accompanied by a significant reduction in postprandial oesophageal acid exposure. However, the study was not designed to assess the effects of baclofen on acid exposure but rather the effects on TLOSRs and reflux episodes. Postprandial acid exposure exhibits high intrasubject variability.29 The postprandial setting was chosen for this study because most reflux occurs in the postprandial period30 and meals are an effective trigger of TLOSRs.27,31 Further studies examining the effects of baclofen on 24 hour oesophageal acid exposure are needed to address this issue. Acid exposure is a consequence not only of the rate of reflux episodes but also oesophageal acid clearance. Similar to the previous study in normal subjects, baclofen had no significant effect on oesophageal acid clearance although the median value was almost 50% greater on the baclofen day. It is possible that subtle effects on acid clearance may have counteracted the reduction in reflux episodes in individual patients. Lastly, baclofen has been shown to increase gastric acid secretion.32,33 Potentially, increased acid secretion could have increased the amount or volume of acid in the refluxate. However, this might be expected to either prolong acid clearance or to increase the likelihood of acid reflux occurring during TLOSRs and neither of these effects was seen. Thus at this stage, failure to reduce oesophageal acid exposure remains unexplained.
Although baclofen has central nervous system side effects, these were not detected during the study. The increased scores for several symptoms such as sleepiness, dizziness, and tiredness over the recording period presumably reflect the normal postprandial increase in these symptoms that is experienced by many people. In our previous study,17 two subjects, both of relatively low body weight (<60 kg), reported significant sleepiness that persisted until the following day. No patient experienced this effect, perhaps because we excluded patients weighing less than 60 kg.
What are the implications of the findings for the role of GABAB agonists in the treatment of reflux disease? The reduction in the rate of TLOSRs and reflux episodes supports the concept that this approach is appropriate in patients who reflux predominately through the mechanism of TLOSR. The lack of effect on oesophageal acid exposure requires further assessment with a more representative measure of oesophageal acid exposure such as 24 hour ambulatory oesophageal pH monitoring.
Acknowledgments
We thank Sara Leandersson for analysis of plasma baclofen levels. This study was supported by AstraZeneca R&D, Mölndal, Sweden.
REFERENCES
Linked Articles
- FILLER
- Commentary