Article Text

Statistics from Altmetric.com
Achalasia is a primary oesophageal motor disorder characterised manometrically by abnormal lower oesophageal sphincter (LOS) relaxation and oesophageal aperistalsis. Because no treatment can restore the muscular activity of the denervated oesophagus, treatment of achalasia has focused on reducing the pressure gradient across the LOS. Pneumatic dilatation is often used as the first non-surgical treatment given to patients with achalasia, with success rates ranging from 70% to 90%.1-3 Surgical myotomy is usually reserved for patients in whom pneumatic dilatation is unsuccessful.
Recently, Pasricha and colleagues4-7 described endoscopic injections of botulinum toxin into the LOS as an alternative non-surgical treatment for patients with achalasia. Botulinum toxin, a potent inhibitor of acetylcholine release from nerve endings, counterbalances the selective loss of inhibitory neurones in the myenteric plexus resulting in unopposed excitation of the oesophageal smooth muscle by acetylcholine. In a placebo controlled study of 21 patients with achalasia, Pasricha and colleagues6 found an early clinical response in 19 of 21 botulinum toxin treated patients, which was maintained in 14 patients at six months’ follow up. This study did not report the clinical efficacy and objective improvements in oesophageal emptying beyond six months after botulinum toxin treatment. Recently, Annese and colleagues8 compared botulinum toxin injection to pneumatic dilatation, finding a symptomatic response rate of 80% at 12 months in patients receiving two injections of botulinum toxin. However, complete objective assessment beyond six months was reported in only 62% of the initial study population.
Our study aim was to compare the immediate (one month) and long term efficacy (six and 12 months) of botulinum toxin with that of pneumatic dilatation in a randomised group of previously untreated patients with achalasia. Patient symptoms and objective measures of oesophageal function (LOS pressure, oesophageal diameter, and oesophageal emptying) were assessed. Special attention was given to the one year symptom responders to both treatments in order to determine the adequacy of oesophageal decompression.
Materials and methods
PATIENTS
Symptomatic patients with newly diagnosed achalasia based on clinical, radiographic, and manometric criteria from 1995 to 1997 were prospectively evaluated at the Cleveland Clinic Foundation or the University of Alabama at Birmingham. Incomplete LOS relaxation and aperistalsis of the oesophageal body on manometry and the presence of oesophageal dilatation, aperistalsis of the oesophageal body, and narrowed LOS on barium oesophagram were the diagnostic criteria for achalasia. Patients with previous pneumatic dilatation or surgical myotomy were excluded. Additional exclusion criteria included age less than 18 years, achalasia associated with gastric or oesophageal carcinoma, neuromuscular disorder, pregnancy, New York Heart Association functional class III or IV cardiovascular disability, or coagulopathy (prothrombin time more than three seconds prolonged compared with controls). All patients gave informed consent to participate in the study protocol which was approved by the Institutional Review Boards of the participating institutions.
STUDY DESIGN
The study was a randomised trial comparing clinical and objective parameters of improvement in patients treated with botulinum toxin injection with those treated with pneumatic dilatation (fig 1). All patients underwent a standardised pretreatment evaluation consisting of clinical symptom assessment, oesophageal manometry, barium oesophagram, and upper gastrointestinal endoscopy to exclude a secondary cause of achalasia.

Schematic summary of the study protocol comparing pneumatic dilatation with botulinum toxin.
Eligible patients were randomly assigned using a computer generated random number sequence to receive either an injection of 100 units of botulinum toxin or to undergo pneumatic dilatation using a 3.0 cm balloon. Patients with less than 50% symptom improvement one month after treatment received a second injection of 100 units of botulinum toxin or repeat pneumatic dilatation with a larger (3.5 cm) balloon, depending on the initial treatment assignment (there was no treatment crossover). Patients who continued to have less than 50% symptom improvement despite the two interventions and required alternative treatments were considered to be “early failures”, whereas those initially having greater than 50% improvement but later experiencing relapse were classified as “late failures”. Patients who continued to show greater than 50% symptom improvement throughout the 12 month study period and did not require further treatments were considered to be “responders”. Symptom scores were assessed at one, three, six, nine, and 12 months after treatment, oesophageal manometry was repeated one month after treatment, and barium oesophagrams were obtained at one, six, and 12 months after treatment.
SYMPTOM ASSESSMENT
The severity of symptoms was evaluated by a modified symptom score9 consisting of the sum of the scores for dysphagia, regurgitation, and chest pain. The frequency of each symptom was graded on a scale ranging from 0 to 5 (0 = none; 1 = once per month or less; 2 = once per week, up to three to four times a month; 3 = two to four times per week; 4 = once per day; 5 = several times per day). The maximum total score was 15 points for each patient. Patients were interviewed initially and during the follow up visits one, three, six, nine, and 12 months after treatment. Clinical response was defined as a greater than 50% improvement in the total symptom score; failure or relapse was defined as a less than 50% improvement in the total symptom score. We used 50% as the cut off point based on our clinical observations that the overwhelming majority of patients still having more than 50% of their original symptoms consider the treatment a failure and seek alternative treatments. This scoring system is similar, with slight modifications, to that used by Eckardt and colleagues9 where clinical remission was defined by clinical scores less than 4 from a maximum allowed score of 12.
OESOPHAGEAL MANOMETRY
Oesophageal manometry was performed using a low compliance, pneumohydraulic, water infusion system (Arndorfer Medical Specialties, Milwaukee, Wisconsin, USA) and an eight lumen manometric catheter (Arndorfer Medical Specialties). The catheter has four proximal recording ports spaced at 5 cm intervals along its length and another four ports radially oriented (90 degrees) near its tip. The recording sites were connected to an eight channel polygraph (Synectics Medical AB, Stockholm, Sweden). All swallows were monitored using an external microphone. LOS pressure was measured by the station pull through technique and recorded as the mean of four measurements at both mid and end expiration. Data presentation, however, shows mid expiration LOS values as this is the traditional measurement in our laboratory. Completeness of LOS relaxation was assessed as the percentage decrease from mean resting LOS pressure to gastric baseline after wet swallows. Oesophageal peristalsis was recorded 3, 8, 13, and 18 cm above the LOS in response to 5 ml swallows of water at 30 second intervals. Patients with a mean oesophageal body contraction amplitude in the distal two leads greater than 40 mm Hg were diagnosed as having vigorous achalasia. LOS pressures were measured at baseline and one month after treatment. The physicians interpreting the manometry tracings were unaware of the treatment assignment.
BARIUM OESOPHAGRAM
A timed barium oesophagram10 was performed on patients initially and one, six, and 12 months after treatment. While standing, the patient ingested a low density barium sulphate suspension (45% weight in volume) (E-Z-PAQUE; E-Z-EM, Westbury, New York, USA) over 30–45 seconds. Patients were instructed to drink the amount of barium they could tolerate without regurgitation or aspiration (usually between 100 and 200 ml). With the patient upright in a slightly left posterior oblique position, three on one radiographs (35 × 35 cm) of the oesophagus were taken one, two, and five minutes after the last swallow of barium. The distance from the tapered distal oesophagus to the top of the barium column (barium height) and the maximum diameter of the barium column (barium width) at one and five minutes post-ingestion were calculated as previously described.10The five minute barium height and maximum width were used to determine oesophageal emptying and oesophageal diameter, respectively. Subsequent follow up studies used the same initial volume of barium to assess emptying. The radiologists were blinded to the treatment status of all patients.
BOTULINUM TOXIN INJECTION
Upper gastrointestinal endoscopy was performed under conscious sedation using a combination of midazolam and meperidine. The LOS was localised endoscopically by identifying the sphincteric rosette typically seen at the oesophagogastric junction. Botulinum toxin (Allergan Inc., Irvin, California, USA) in five 2 ml aliquots of 20 units (10 units/ml; 100 units total) was injected through a 25 gauge sclerotreatment needle (5 mm long) into the LOS.5 ,6Lyophilised botulinum toxin was stored at −4°C until reconstituted in saline. It was injected immediately after reconstitution to avoid denaturation.
PNEUMATIC DILATATION
Pneumatic dilatation was done using a Rigiflex balloon dilator (Microvasive, Millford, Massachusetts, USA) under fluoroscopic control in the supine position by experienced gastroenterologists who had previously performed more than 100 pneumatic dilatations. Patients fasted for at least eight hours before the procedure. If a tortuous oesophagus was found, the patient was placed on a clear liquid diet for several days before the procedure. All patients were sedated with intravenous midazolam, meperidine, and topical anaesthesia of the pharynx. After upper gastrointestinal endoscopy, a dilator was passed over a guidewire placed in the stomach and positioned across the diaphragmatic hiatus using the radiopaque markers as guides. Correct location was verified fluoroscopically by observing the waist, after balloon inflation pressures of 3–5 psi. The balloon was then inflated for one minute at 9–15 psi, until obliteration of the waist. A gastrografin swallow followed by a barium swallow (if necessary) was performed immediately after the dilatation to test for oesophageal perforation. All patients initially underwent dilatation with a 3.0 cm balloon. Patients not responding within the first month of treatment were redilated with the larger 3.5 cm balloon.
STATISTICAL METHODS
Descriptive statistics are provided as the median and interquartile range for age, symptom score, amplitude, LOS pressure, and barium height and width. Percentage changes from baseline barium height and width were summarised with the mean and 95% confidence intervals. The data were analysed on the basis of intention to treat. The cumulative remission rates of each treatment were estimated by the Kaplan-Meier method and the difference between treatment groups was tested by the log rank test. The difference between LOS pressures initially and at one month was compared using the Wilcoxen signed rank test for paired non-parametric data; the significance level was defined as p<0.05. Friedman repeated measures analysis of variance (ANOVA) on ranks was used to test for differences over time within each treatment group for symptom scores, and barium height and width. The Wilcoxen signed rank test for paired non-parametric data was used for multiple comparisons isolating the individual differences within the group. The Bonferroni correction applied to adjust for multiple comparisons resulted in an adjusted alpha level of 0.01 for the total symptom scores and of 0.0167 for comparisons of the barium height and width. The difference in proportions was evaluated using Fisher’s exact test. The difference in patient characteristics between responders and non-responders within each botulinum toxin and pneumatic dilatation treated group was analysed using the Mann-Whitney test for unpaired non-parametric data.
Results
Of 48 patients enrolled in the study, 24 received botulinum toxin and 24 underwent pneumatic dilatations. The baseline characteristics of age, sex, symptom severity, LOS pressure, oesophageal amplitude, height, and width of barium column were similar for the two groups (table 1). In the botulinum toxin treated group, two patients were excluded from the per protocol analysis; one was lost to follow up and the other declined the second injection of botulinum toxin. In the pneumatic dilatation group, four patients were excluded as a result of perforation with the 3.0 cm balloon (one patient), non-compliance (one patient), lost to follow up (one patient), and protocol violation by using the 4.0 cm balloon (one patient). There were no differences in age, sex, initial LOS pressure, barium height, barium width, or oesophageal amplitude between excluded patients and those who completed the study. Therefore, the number of evaluable patients was 22 for the botulinum toxin and 20 for the pneumatic dilatation group.
Baseline characteristics of patients with achalasia
CLINICAL RESPONSE TO TREATMENT
Figure 2 shows the Kaplan-Meier plot for the two treatment groups. Six patients required pneumatic dilatation with a 3.5 cm balloon, and six required a second injection of botulinum toxin. The remaining patients responded to a single pneumatic dilatation with a 3.0 cm balloon (14 patients) or to botulinum toxin treatment (16 patients). The cumulative one year remission rate was significantly higher (p=0.02) for the pneumatic dilatation group than for the botulinum toxin group. Twelve months after treatment, 14 of 20 (70%) patients treated with pneumatic dilatation and only 7 of 22 (32%) botulinum toxin treated patients were in symptomatic remission (p<0.01). Intent to treat analysis found slightly lower 12 month remission rates for both treatments; however, pneumatic dilatation (58%) continued to show a higher remission rate than botulinum toxin (29%) (p=0.017).
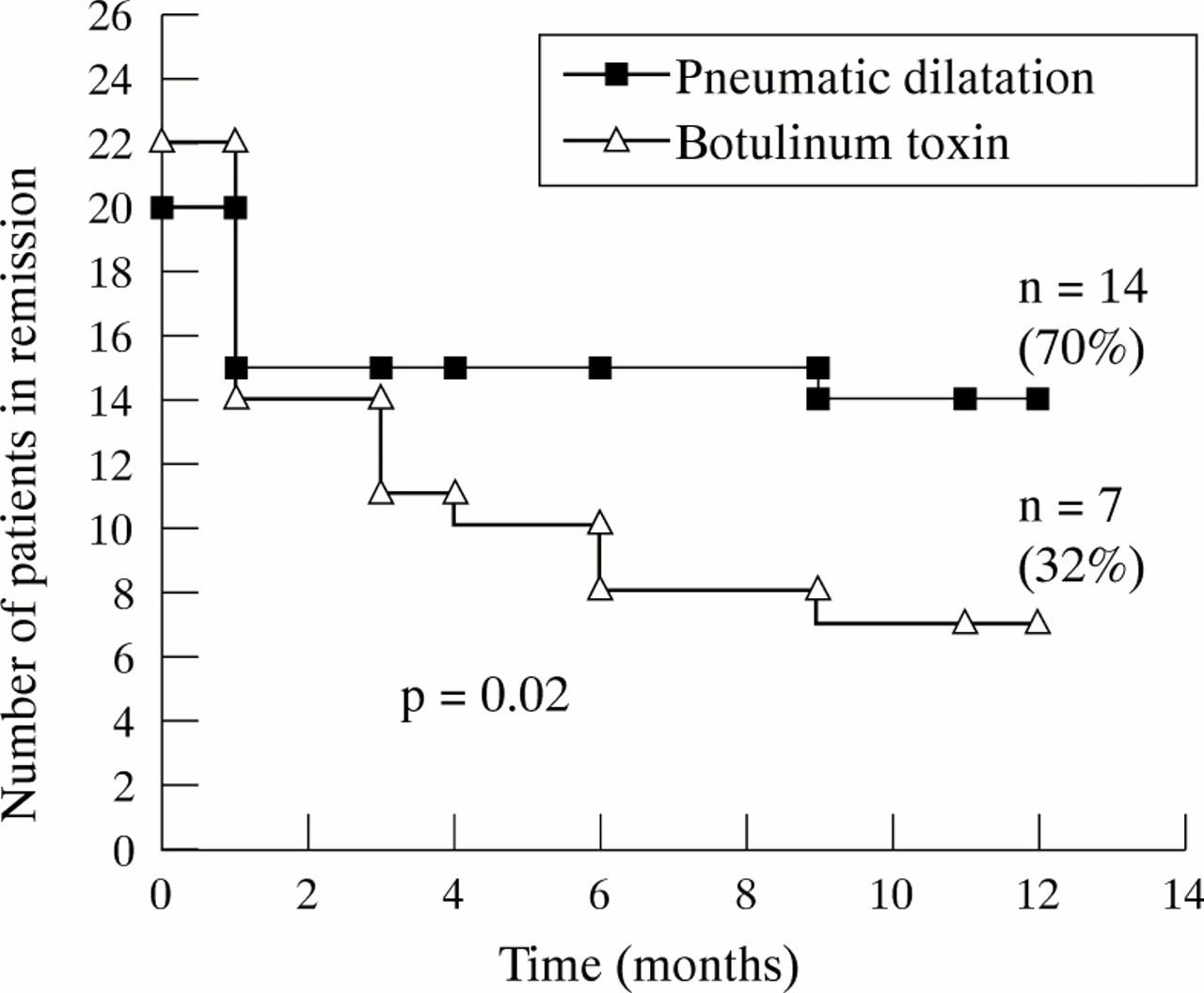
Kaplan-Meier plot showing significantly (p=0.02) higher cumulative one year remission rate for patients treated with pneumatic dilatation compared with botulinum toxin.
There were 21 treatment failures over the 12 month study: six in the pneumatic dilatation group and 15 in the botulinum toxin group. There was no significant difference (p=0.51) in the “early” failure rates (no response to initial treatment) between the pneumatic dilatation (five patients) and botulinum toxin (eight patients) treatments. Significantly (p=0.014) more patients failed “late” (improved initially and then relapsed) in the botulinum toxin treated group (seven patients) than in the pneumatic dilatation group (one patient) (fig 2). In the late failure group, the botulinum toxin treated patients relapsed at three months (three patients), four months (one patient), six months (two patients), and nine months (one patient); in the pneumatic dilatation group, one patient relapsed nine months after treatment. In the patients treated with two injections of botulinum toxin, four of six (67%) patients failed and required definitive treatment with pneumatic dilatation.
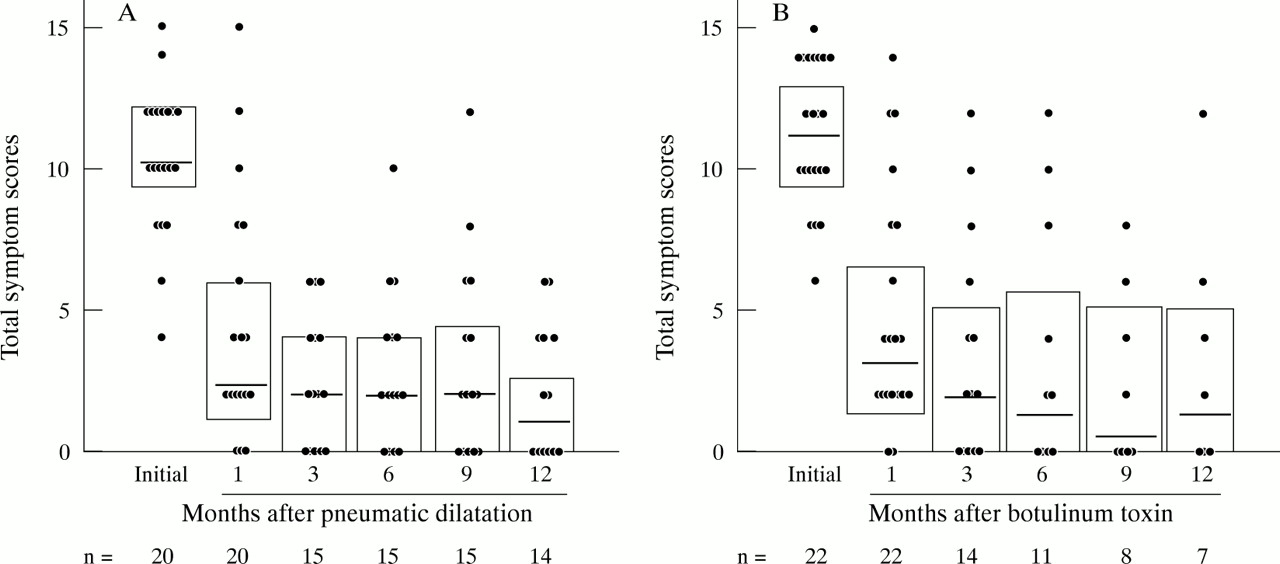
Figure 3 shows the changes in total symptom scores for the two patient groups. In patients treated with pneumatic dilatation, the median (interquartile range) total symptom score decreased significantly (p<0.001) one month after treatment and remained significantly reduced at three, six, nine, and 12 months after treatment (fig 3A). Similarly, patients treated with botulinum toxin had a significant decrease (p<0.001) in median (interquartile range) total symptoms at one, three, six, nine, and 12 months after treatment (fig 3B). In the responding patients, there was no difference in symptom response between groups at the various time intervals. The reduction over time in both groups applied to all three components of the symptom scores: dysphagia, regurgitation, and chest pain.
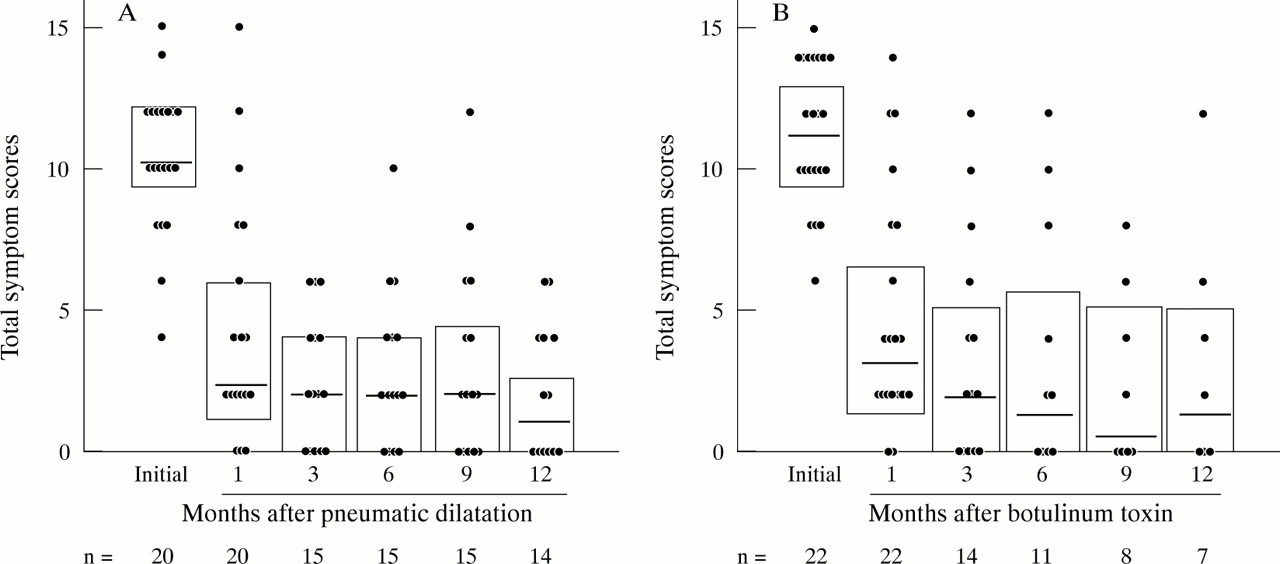
Patient symptom scores initially and at one, three, six, nine, and 12 months after pneumatic dilatation (A) and botulinum toxin treatment (B). The medians and interquartile ranges (25% to 75%) are shown with horizontal lines and boxed in rectangles, respectively. The number of patients (n) remaining in the study is shown for each time interval.
OBJECTIVE OESOPHAGEAL MEASUREMENTS
LOS pressure
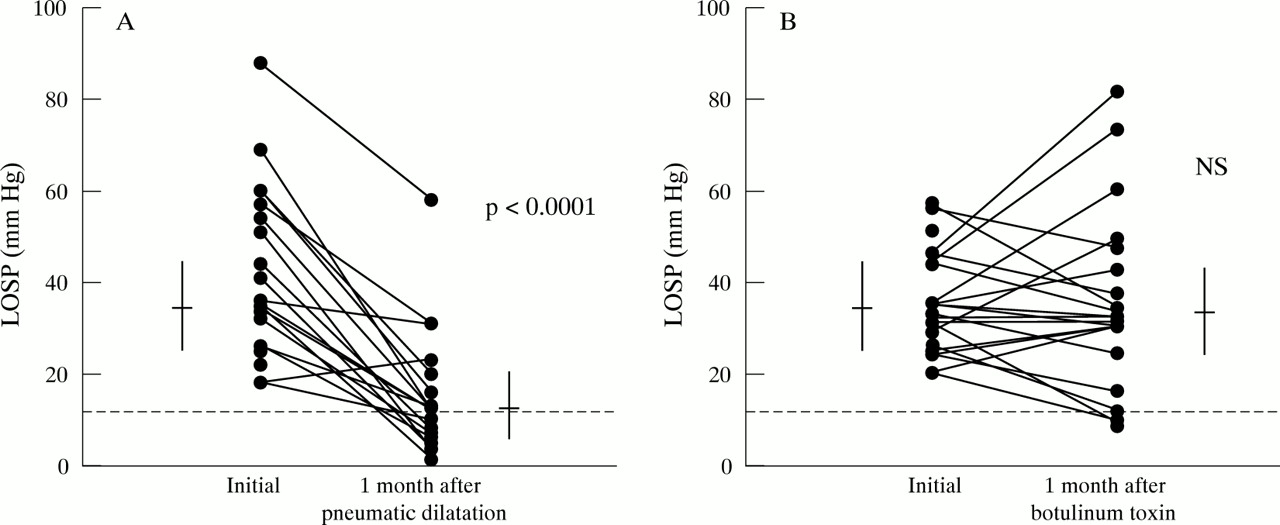
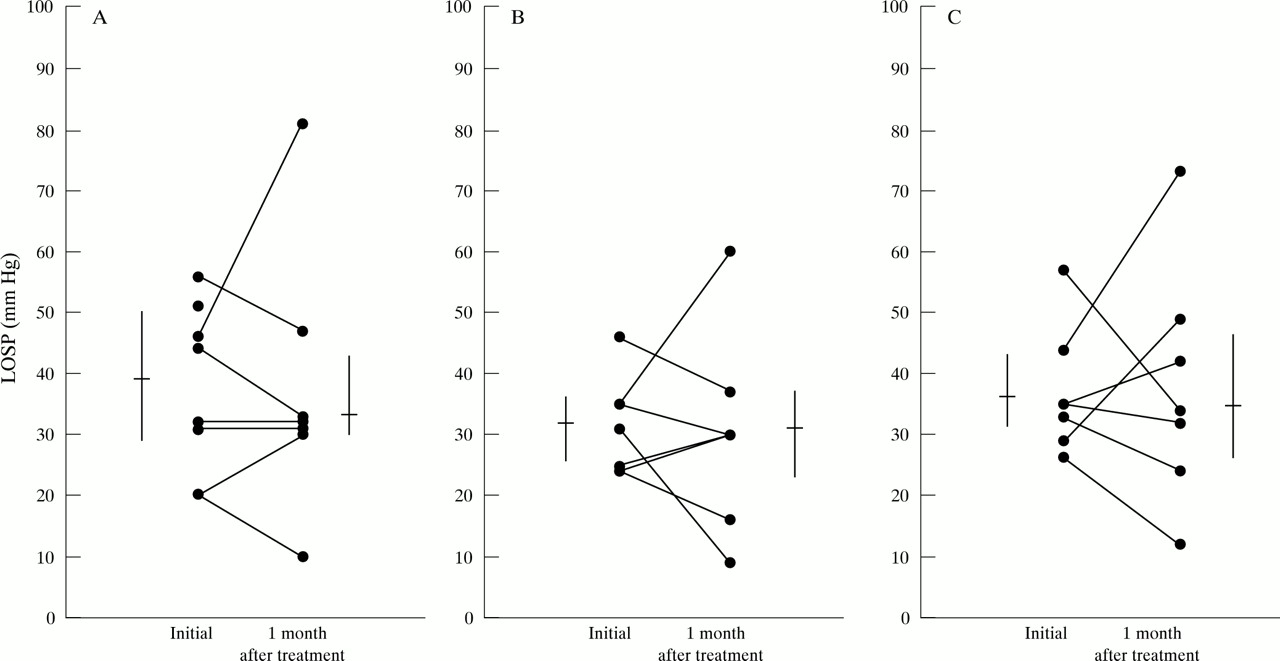
In the pneumatic dilatation group, the median (interquartile range) LOS pressure decreased significantly (p<0.0001) from 35.5 mm Hg initially (26.0 to 55.0 mm Hg) to 12.0 mm Hg (7.0 to 20.0 mm Hg) one month after treatment (fig 4A). In the botulinum toxin group, there was no difference between the initial and one month after treatment LOS pressures: 34.0 mm Hg (26.0 to 44.0 mm Hg) and 32.0 mm Hg (28.5 to 43.2 mm Hg), respectively (fig 4B). In the pneumatic dilatation group, 11 of 20 patients (55%) had reduction of LOS pressures to ⩽12.0 mm Hg, while this occurred in only three of 22 patients (13.6%) treated with botulinum toxin (p<0.01). Subgroup analysis in patients treated with botulinum toxin showed no difference in the median (interquartile range) initial and post-treatment LOS pressures between the early failures, late failures, or those with clinical remission at one year (fig 5 A−C).

Lower oesophageal sphincter pressures (LOSP) initially and at one month after pneumatic dilatation (A) and botulinum toxin treatment (B). The horizontal lines denote group medians and the vertical bars represent interquartile ranges (25% to 75%). The dotted horizontal line represents a lower oesophageal sphincter pressure of 12 mm Hg.

Lower oesophageal sphincter pressures (LOSP) initially and at one month after botulinum toxin treatment in (A) early and (B) late failure groups as well as those in remission at (C) one year.
Oesophageal emptying
The median (interquartile range) oesophageal barium height (cm) at five minutes significantly (p<0.001) decreased after pneumatic dilatation (fig 6A). In the botulinum toxin group, there was a significant (p<0.01) reduction in median (interquartile range) barium height one month after treatment, while there was no difference from baseline values at six and 12 months (fig 6B). At 12 months, seven of 14 (50%) patients treated with pneumatic dilatation had complete oesophageal emptying compared with only two of seven (29%) patients treated with botulinum toxin (p=0.64). There was no difference in mean change from baseline between groups at various time intervals. Despite persistent symptom improvement, four of seven (57%) botulinum toxin treated patients had barium heights similar to their initial untreated values, while this was the case in only two of 14 (14%) patients treated with pneumatic dilatation (p=0.12).
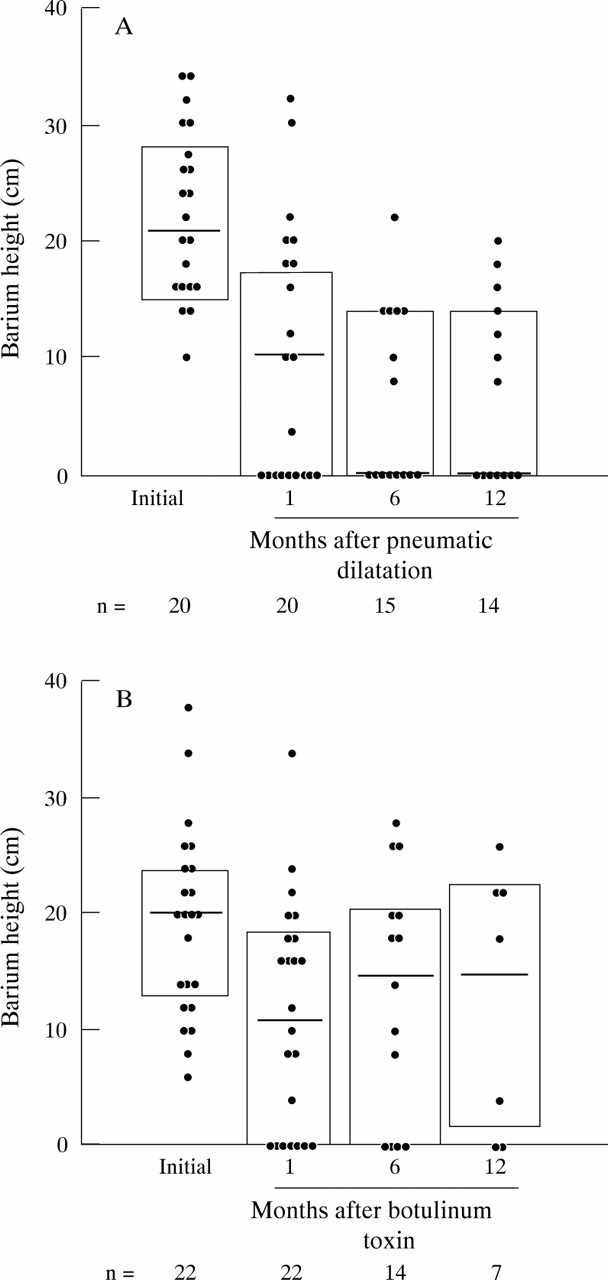
Oesophageal barium column height representing oesophageal emptying initially and at one, six, and 12 months after pneumatic dilatation (A) and botulinum toxin treatment (B). The horizontal lines denote group medians while the vertical bars represent interquartile ranges (25% to 75%). The number of patients (n) remaining in the study is shown for each time interval.
The mean percentage decrease in oesophageal barium height at one, six, and 12 months after pneumatic dilatation (50.2%, 58.4%, 54.6%) was significantly greater than after botulinum toxin (33.6%, 13.5%, 13.4%). Patients treated with pneumatic dilatation had a significantly (p=0.04) greater percentage decrease in oesophageal barium height over the 12 month study period than those in the botulinum toxin group. The degree of change in barium height was stable over the 12 months within the treatment groups and did not change significantly.
The median (interquartile range) oesophageal width (mm) decreased significantly (p<0.001) six and 12 months after pneumatic dilatation (fig 7A). Although there was a decrease in barium width one month after pneumatic dilatation, this did not reach statistical significance. For patients treated with botulinum toxin, there were no differences in the median (interquartile range) oesophageal width over the 12 month study period (fig 7B). There was no difference in mean change from baseline between groups at the one and six month time intervals; however, the 12 month oesophageal width was significantly (p=0.01) lower for patients treated with pneumatic dilatation than in the botulinum toxin treated patients. At 12 months eight of 14 patients (57%) treated with pneumatic dilatation had oesophageal widths within normal limits (less than 25 mm in diameter) compared with only one of seven patients (14%) after treatment with botulinum toxin (p=0.09).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Barium width representing oesophageal diameter initially and at one, six, and 12 months after pneumatic dilatation (A) and botulinum toxin treatment (B). The horizontal lines denote group medians while the vertical bars represent interquartile ranges (25% to 75%). The number of patients (n) remaining in the study is shown for each time interval.
Patients treated with pneumatic dilatation had a significantly (p=0.008) greater overall mean percentage decrease in oesophageal width over 12 months compared with those treated with botulinum toxin: 53.2% and 25.6%, respectively. There was a significant (p=0.01) time dependent improvement in oesophageal width throughout the 12 month study for both treatments; however, this was more notable for patients treated with pneumatic dilatation.
PREDICTORS OF RESPONSE
Post hoc evaluation revealed that neither age, sex, amplitude of oesophageal contractions, nor duration of illness distinguished the responders from non-responders in the botulinum toxin or pneumatic dilatation treated groups; however, there was a trend (p=0.16) towards more favourable outcome in patients with vigorous achalasia for the botulinum toxin treated group.
SUBSEQUENT CLINICAL COURSE
In the botulinum toxin failure group (n=15), patients later improved symptomatically after pneumatic dilatation (eight patients) and Heller myotomy (three patients); three patients were still symptomatic without any other treatments, and one patient was lost to follow up after completing the study. In the pneumatic dilatation failure group (n=6), patients did well after Heller myotomy (two patients), pneumatic dilatation with the 4.0 cm balloon (two patients), and oesophagectomy (one patient), while one patient is still symptomatic and has not undergone any further treatment.
A total of 40 pneumatic dilatations were performed on our patients: 10 in the failed botulinum toxin treated group and 30 in the 24 patients assigned to pneumatic dilatation. Oesophageal perforation occurred in two of 40 (5%) pneumatic dilatations. The perforations occurred during the study in one patient and after exclusion from the study due to symptom failure in the second patient. The two patients with oesophageal perforations underwent surgical repair immediately after perforation was detected and had the perforation oversewed and Heller myotomy performed on the opposite wall of the oesophagus. Both patients had good clinical outcomes.
Discussion
This randomised study compares the efficacy of botulinum toxin injection with pneumatic dilatation in patients with untreated achalasia, while also examining both subjective and objective parameters of oesophageal improvement in all patients over 12 months. At study end, 70% of the pneumatic dilatation treated patients were in symptomatic remission compared with 32% treated with one or two injections of botulinum toxin (p=0.02; fig 2). Additionally, the one year improvement in symptoms in patients treated with pneumatic dilatation paralleled dramatic improvements in LOS pressure, oesophageal emptying, and oesophageal diameter, while the one year subjective improvements reported by patients post-botulinum toxin treatment often did not accompany improvements in these objective measurements.
In our study, the 12 month efficacy of pneumatic dilatation (70%) was slightly higher than that reported by Eckardt and colleagues9 who found a one year remission rate of 59% after a single dilatation using the Brown-McHardy balloon in 54 consecutive patients with achalasia. Using the newer Rigiflex balloon dilators, good to excellent relief of symptoms has been reported in up to 93% of patients with achalasia, usually using graduated balloon dilatations from 3.0 cm to as large as 4.0 cm diameters.11 ,12 In fact, using balloon sizes similar to those in our study (3.0 cm and 3.5 cm), Kadakia and Wong12reported a success rate of 79% with a mean follow up of 47 months. Similar efficacy of pneumatic dilatation (85%) was recently reported by Annese et al.8
At first review, the botulinum toxin efficacy of 32% after 12 months in our study appears much lower than that in previous reports.6-8 ,13 ,14 However, our study is the first to assess the efficacy of initial botulinum toxin treatment after one year. In previous studies, patients who rapidly relapsed after the first botulinum toxin injections received follow up injections at various intervals during the 12 month period and were still defined as successes, possibly resulting in a bias towards botulinum toxin efficacy. Closer scrutiny of efficacy of the initial botulinum toxin injection in these studies reveals failure rates (18% to 32%) similar to those in our study (36%). Furthermore, our six month failure rate of 50% is similar to the 56% and 52% six month failure rates found by Pasricha and colleagues6 and Gordon and Eaker,13 respectively. Recently, Fishman and colleagues14 reported the symptomatic response of 60 consecutive patients with achalasia treated with botulinum toxin and observed a one year response rate of 36% which is comparable to our one year response of 32%. Annese and colleagues8 found an even higher failure rate for botulinum toxin, with symptomatic relapse in seven of eight patients after 12 months. Therefore, the long term efficacy of botulinum toxin, unlike pneumatic dilatation, will require several repeated injections every three to six months in most patients.
Initial studies by Pasricha and colleagues6 and later by Annese and coworkers8 found 60% and 52% mean decreases in LOS pressures one week and one month after botulinum toxin treatment, respectively. However, we found no significant decrease in the mean LOS pressure one month after botulinum toxin treatment compared with initial values (fig 4B). Several possibilities may explain this observation. Firstly, there are slight differences in the concentration of botulinum toxin injected in our study (10 units/ml) compared with those used by Pasricha et al(20 units/ml)6 and Annese et al(25 units/ml).8 However, the total dose of botulinum toxin injected (80 units to 100 units) was similar for all three studies. Could the dilution difference between the studies be responsible for the observed differences in the effect of botulinum toxin on LOS pressure? This possibility is less likely as previous studies, using botulinum toxin in skeletal muscle disorders, did not find that dilution reduced efficacy of the drug. In fact, various dilutions including 10 units/ml, 20 units/ml, 50 units/ml, and 100 units/ml have been used effectively with no change in efficacy of the toxin.15 Furthermore, studies show that only dilutions of the toxin to extremely low concentrations (ng/ml) tend to decrease its stability.16
Secondly, error or variability in manometric measurements of LOS pressure is an unlikely explanation as similar variability did not occur in patients treated with pneumatic dilatation. In fact, the pneumatic dilatation group had a consistent and notable decrease in LOS pressures after treatment (fig 4A), underscoring the efficacy of pneumatic dilatation.
Thirdly, subgroup analysis of the botulinum toxin treated patients comparing pretreatment and post-treatment LOS pressures between patients in remission and those with early failures and late failures found no significant difference between groups (fig 5). This finding suggests that the variability of the LOS pressure data is equally distributed between the outcome groups and did not result in a bias favouring any one group in the botulinum toxin treated patients.
Fourthly, the lack of botulinum toxin efficacy on LOS pressures found in this study is unlikely to be due to differences in LOS pressure measurements at mid versus end expiration reported by Pasrichaet al.6 The analysis of the LOS pressures in our patients both at mid and end expiration, before and after treatment with botulinum toxin and pneumatic dilatation, did not alter the results of our study.
Finally and importantly, our data are consistent with several recent17−19 reports finding no difference in the one or two month post-injection LOS pressure of patients treated with botulinum toxin as compared with pretreatment values. For example, Massey and colleagues19 found no change in the mean (SEM) LOS pressures of eight previously untreated patients with achalasia before and two months post-botulinum toxin injection: 37.0 (4.0) mm Hg and 35.0 (7.0) mm Hg, respectively. Additionally, Kozarek and colleagues17 recently compared the effect of LOS injection of 50 units versus 100 units of botulinum toxin in 32 patients with achalasia. They reported no difference in the LOS pressure post-botulinum toxin compared with pretreatment values for either dose of the toxin (50 units: pretreatment LOSP = 42.7 mm Hg, post-treatment LOSP = 41.1 mm Hg; 100 units: pretreatment LOSP = 47.0 mm Hg, post-treatment LOSP = 41.0 mm Hg).
Barium oesophagram and oesophageal scintigraphy, obtained in the upright position, are commonly used to assess oesophageal emptying in patients with achalasia. In this study, we used a recently validated timed barium oesophagram technique that is simple, widely available, and inexpensive while providing a standardised method for assessing improvement in upright emptying and changes in oesophageal diameter.20 In contrast, oesophageal scintigraphy is much less available, operator dependent, expensive, and evaluates accurately only oesophageal emptying, not diameter. Thus, we believe the barium oesophagram, as a measure of liquid emptying, is more representative of oesophageal function in these patients.
At one year following treatment, pneumatic dilatation was associated with a significant (p<0.001) improvement in oesophageal emptying as assessed by a reduction in both barium height and width; this was not observed in the botulinum toxin treated patients despite having symptom remission. In patients treated with pneumatic dilatation, 50% had complete oesophageal emptying at five minutes and 57% showed a return of oesophageal width to within normal limits; only 29% and 14% respectively of the botulinum toxin treated patients showed similar improvements. Additionally, the percentage decrease in barium height in the pneumatic dilatation treated patients was stable over 12 months, suggesting continued efficacy of pneumatic dilatation during the study. On the other hand, pneumatic dilatation resulted in a time dependent decrease in oesophageal width, which was significantly (p=0.008) greater than that seen in the botulinum toxin group. The discrepancy observed in the improvement of these two measures of oesophageal function should not be surprising. The relief of LOS obstruction should produce an immediate improvement in oesophageal emptying; however, the ability of the dilated oesophagus to return to normal diameter is a function of disease duration, residual elasticity of the organ, and adequacy of oesophageal decompression. We speculate that patients with return to near normal oesophageal function will have prolonged symptom relief.
In previous studies,7 older age and the presence of vigorous achalasia, defined as oesophageal amplitude greater than 40 mm Hg, predicted favourable outcome for patients treated with botulinum toxin. However, our data are consistent with those recently reported from a European multicentre trial21 which found no outcome predictors in botulinum toxin treated patients. We found that age, sex, and duration of illness did not distinguish the responders from the non-responders, although there was a trend towards favourable outcome in patients with vigorous achalasia. Furthermore, our data do not confirm the results of Eckardt and colleagues9 who found that post-pneumatic dilatation LOS pressure of 10 mm Hg or less was the single best factor for predicting favourable long term clinical response.
The discrepancy between the six and 12 month subjective and objective improvement after botulinum toxin raises an intriguing question regarding its possible site of efficacy. Perhaps such disparity may be the result of effects beyond cholinergic neural inhibition. The oesophageal neural network is different from the neuromuscular junction in having not only acetylcholine but also other peptides that closely interact with neural stimulation.22 In fact, studies in the rat smooth muscle found that botulinum toxin induces relaxation by cholinergic as well as by peptidernergic neurones.23Therefore, the assumption that botulinum toxin injected into the LOS of patients with achalasia works similar to those in skeletal muscles by only affecting the acetylcholine containing neurotransmitters, may be too simplistic. Our findings suggest a possible inhibitory effect of botulinum toxin on the oesophageal sensory neurones resulting in improved patient symptoms that are out of proportion to any objective improvements. However, this assumption needs to be substantiated by future studies.
In conclusion, we found that pneumatic dilatation was more effective than botulinum toxin over one year in a randomly treated group of patients with achalasia. Pneumatic dilatation was associated with both symptomatic improvement and frequently a return to near normal oesophageal emptying and diameter. In contrast, even the botulinum toxin treated patients who improved symptomatically over one year did not experience comparable improvements in oesophageal function, suggesting a possible preferential interaction of the toxin on the oesophageal sensory neurones. Therefore, we believe that pneumatic dilatation is the preferred medical treatment for most patients with achalasia. Until we are able to understand better and possibly improve on the neurophysiological action of botulinum toxin, we should reserve this treatment for patients with achalasia (older individuals, comorbid illnesses) who are not candidates for pneumatic dilatation or myotomy. Otherwise, the treatment of healthy achalasia patients with botulinum toxin will require serial injections, efficacy will wane over time due to antibodies, and the treatment does not appear to be cost effective in several preliminary studies.24 ,25
Acknowledgments
We gratefully acknowledge Jean Price and Camille Torbey, MD, for their laboratory support, Kirk Easley, MS, for his statistical guidance and support, and Tom Lang for his editorial assistance. This work was supported by a research grant from the American College of Gastroenterology Institute for Clinical Research and Education.
Abbreviations
- LOS
- lower oesophageal sphincter
- LOSP
- lower oesophageal sphincter pressure
References
Linked Articles
- Commentary