Article Text

Abstract
BACKGROUND Topical application of glyceryl trinitrate (GTN) ointment heals chronic anal fissures, providing an alternative to the traditional first line treatment of surgical sphincterotomy.
AIMS To determine the most effective dose of topical GTN for treatment of chronic anal fissures and to assess long term results.
METHODS Seventy consecutive patients with chronic anal fissure, were randomly allocated to eight weeks treatment with placebo, 0.2% GTN three times daily, or GTN starting at 0.2% with weekly 0.1% increments to a maximum of 0.6%, in a double blind study.
RESULTS After eight weeks fissure had healed in 67% of patients treated with GTN compared with 32% with placebo (p=0.008). No significant difference was seen between the two active treatments. Headaches were reported by 72% of patients on GTN compared with 27% on placebo (p<0.001). Maximum anal sphincter pressure reduced significantly from baseline by GTN treatment (p=0.02), but not placebo (p=0.8). Mean pain scores were lower after treatment with GTN compared with placebo (NS). Of fissures healed with placebo 43% recurred, compared with 33% of those healed with 0.2% GTN and 25% healed with escalating dose GTN (p=0.7).
CONCLUSIONS GTN is a good first line treatment for two thirds of patients with anal fissure. An escalating dose of GTN does not result in earlier healing. Significant recurrence of symptomatic fissures and a high incidence of headaches are limitations of the treatment.
- glyceryl trinitrate
- anal fissures
Abbreviations
- GTN
- glyceryl trinitrate
- MRP
- maximum resting anal pressure
- NO
- nitric oxide
Statistics from Altmetric.com
Anal fissure is associated with severe anal pain and bleeding per rectum. The maximum resting anal pressure (MRP), which relates mainly to internal anal sphincter smooth muscle activity, is often raised.1 This may contribute to the pain and localised ischaemia of the traumatised anal lining, perpetuating ulceration and preventing healing.2 Laser Doppler flowmetry,3 and postmortem angiographic studies4 have shown a relatively poorly perfused area at the posterior commisure, where over 90% of fissures occur.
Lateral anal sphincterotomy, which decreases the resting anal sphincter pressure, has been the most favoured surgical procedure for healing fissures.5 However, concerns have been raised about the incidence of faecal incontinence following this procedure.6-8
There is now good evidence that nitric oxide (NO) is one of the most important inhibitory neurotransmitters in the internal anal sphincter.9 ,10 A number of studies have shown that topical application of glyceryl trinitrate (GTN), a NO donor, to the anus, can cause reversible relaxation of the internal sphincter in man,11 and heal fissures.12 However, an acquired tolerance to GTN with continual usage has been reported,13 and this may account for some treatment failures. Nitrate tachyphylaxis is well recognised by cardiologists treating angina pectoris with GTN.14
A recent randomised controlled trial showed that over two thirds of chronic anal fissures can be healed with 0.2% GTN within eight weeks compared with less than 10% with placebo.15 However, the most effective dosage regimen of GTN for fissures has not been determined and the long term results of treatment are not known. In this study we aimed to determine whether higher doses of GTN would result in faster or higher healing rate. As patients do not easily tolerate high doses of GTN we aimed to reach the higher concentrations by gradual weekly increments starting from 0.2% ointment. We postulated that as tolerance develops to the effects of GTN, patients should also become more tolerant to the headaches and other side effects. In addition we have followed up patients after healing to determine the long term efficacy of this treatment.
Materials and methods
Seventy consecutive patients with chronic anal fissure and anal pain attending surgical outpatient clinics were recruited for the study over a 12 month period. All patients had anal fissure of three months duration or longer, with clinical features of chronicity such as fibrosis of the base of the ulcer or an associated sentinel pile. Pregnant women, patients already on nitrate treatment for ischaemic heart disease, patients with fissures due to an underlying identifiable pathology such as Crohn’s disease or HIV, and patients with a history of migraine were excluded. Anal manometry was performed on every patient using an eight channel water perfused catheter or water filled microballoon system; maximum resting anal pressure (MRP) was determined using a station pull through technique and recordings continued for 10 minutes. Anodermal blood flow was measured using a DRT4 laser Doppler flowmeter (Moor Instruments, Devon, UK) by taking the mean of four quadrant readings around the anus.
Patients were randomly allocated to one of three treatment groups in a double blind manner, by a senior pharmacist using computer generated random numbers. The code was kept in the pharmacy department (unknown to the investigators). The GTN ointments were prepared at the hospital pharmacy by diluting commercially available GTN (Percutol, Dominion Pharma, Haslemere, UK) to the required concentration in yellow paraffin. All treatment bottles and ointments looked identical. The three treatment groups were: placebo; 0.2% GTN; and increasing dose GTN starting at 0.2% with weekly increments of 0.1% to a maximum of 0.6% concentration. Patients were shown by the principal investigator how to apply a standard “pea sized” quantity of the ointment (approximately 0.5 ml measured using a hospital syringe) during their first visit. This was applied manually to the skin of the anal verge circumferentially around the anal opening (not intra-anal) three times daily for an eight week treatment course.
Fortnightly assessment was by clinical examination of the fissure, anal manometry, and laser Doppler flowmetry. Patients were given daily diary cards for the eight weeks of treatment, asked to indicate the worst pain experienced each day on linear analogue charts (scale 0 to 10), and were questioned about side effects of treatment. If healing had occurred after an initial eight week period the patients were followed up in the outpatient clinic at three, six, and twelve months, or sooner if recurrent symptoms developed. Treatment failures, or patients who were unable to tolerate treatment with the ointment, were offered surgical sphincterotomy. Those patients who were clearly improving or symptom free despite a persistent fissure, were offered a further six weeks treatment with 0.2% GTN and considered as treatment failures when analysing the results.
Statistical analysis was by one way analysis of variance (ANOVA) to compare the continuous variables in the three groups. The results of the two active treatment groups were compared with one another; each was compared with placebo separately as well as the average of the two being compared with placebo. Binary outcome variables such as healing were analysed using Fisher’s exact test to compare the two active treatments to one another and also the combined average with placebo. A value of p<0.05 was considered significant. We calculated that using parametric tests, a sample size of 17 would allow us to determine a difference in means of one standard deviation between each active treatment and placebo using a 5% significance level and an 80% power. As we expected to analyse some of the data using non-parametric tests, and to allow for failures in completion of treatment, we increased the sample size by 10% to 20 or more patients per group.
Results
Twenty four patients were randomised to each of the two GTN groups and 22 to placebo. One patient initially diagnosed as having a fissure and randomised to 0.2% GTN was found not to have a fissure when attending for the first manometry session and was excluded from subsequent analysis. Another patient who was randomised to increasing dose GTN failed to attend and was uncontactable. One patient randomised to placebo did not tolerate treatment, underwent lateral sphincterotomy, and was considered as a treatment failure when analysing the results. A total of 23 patients therefore in each of the two GTN groups and 22 in the placebo group were available for follow up (table 1). The patients were well matched for age, sex, duration of symptoms, and site of their fissure (table 1).
Patient characteristics
After 10 weeks (eight weeks treatment and two weeks after treatment) the anal fissure had healed in 7/22 (32%) patients on placebo, 15/23 (65%) patients on 0.2% GTN, and 16/23 (70%) patients on escalating dose GTN (p=0.008, Fisher’s exact test, placebo versus combined GTN healing rate). Median time to healing was eight weeks (range 4–10 weeks). Nine of 23 (39%) fissures had healed after six weeks treatment with high dose GTN (fig 1) compared with 5/23 (22%) on 0.2% GTN (p=0.33, Fisher’s exact test). Four of the six anterior fissures in the 0.2% GTN group and 2/3 in the increasing dose GTN group healed at the end of the eight weeks. All of these fissures were in female patients.
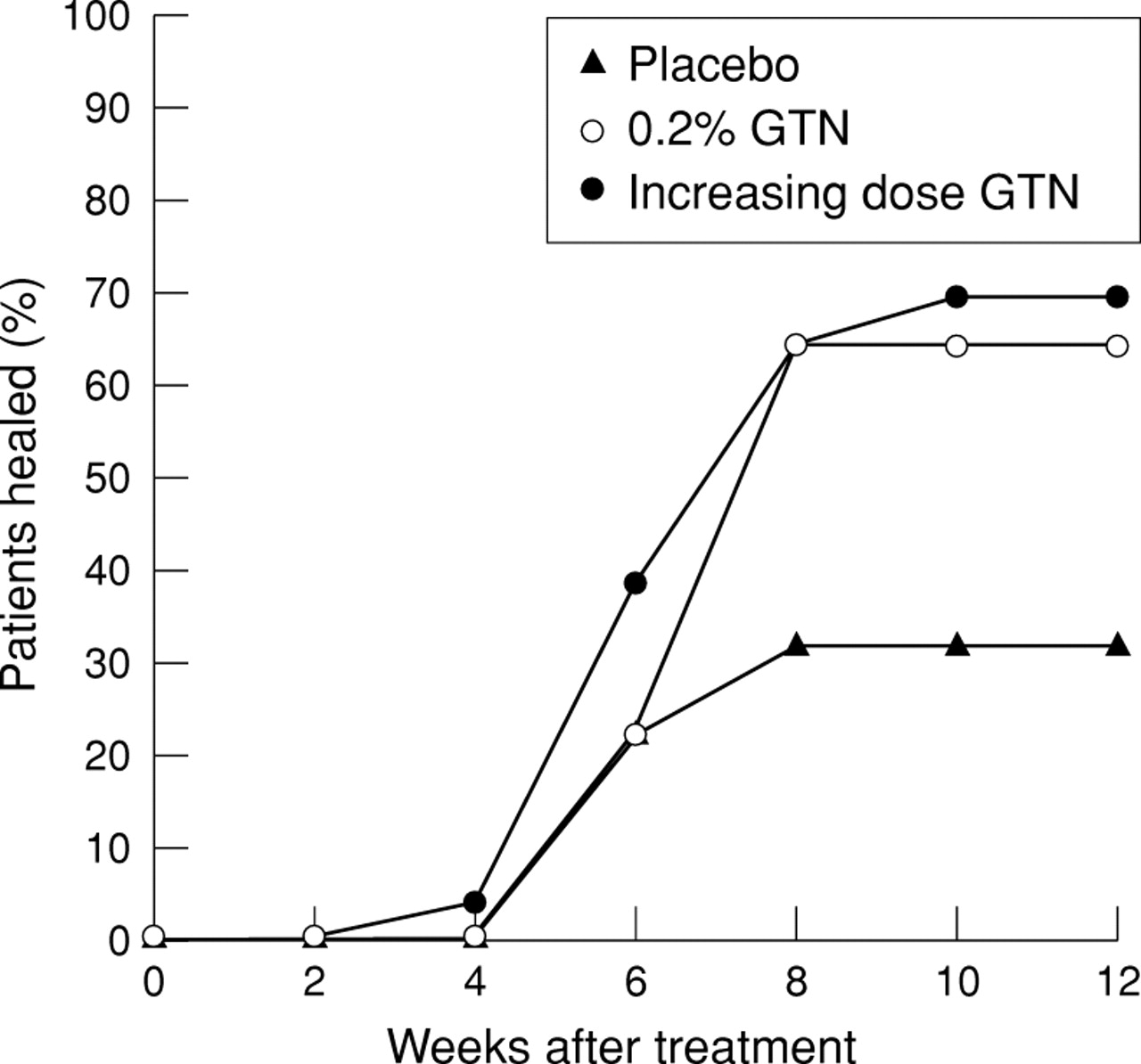
Cumulative healing of fissures.
Headaches were reported by 33/46 (72%) patients on GTN compared with 6/22 (27%) on placebo (p<0.001, Fisher’s exact test). There was no significant difference (p=0.5) in number of patients reporting headaches between the 0.2% GTN group (15/23, 65%) and the increasing dose GTN group (18/23, 78%).
The effect of each treatment on the linear analogue pain score was analysed using analysis of variance. Compared with the pretreatment pain score there was a significant reduction in mean pain score after placebo (p=0.001), after 0.2% GTN (p<0.0001), and after increasing dose GTN (p<0.0001) after two weeks. This reduction in pain was maintained throughout the study in all three treatment groups (fig 2). However, there was no significant difference in the mean pain score between the two GTN groups (p=0.7). Similarly the lower mean pain score after GTN (average of the two GTN groups) compared with that after placebo was not statistically significant (p=0.4).
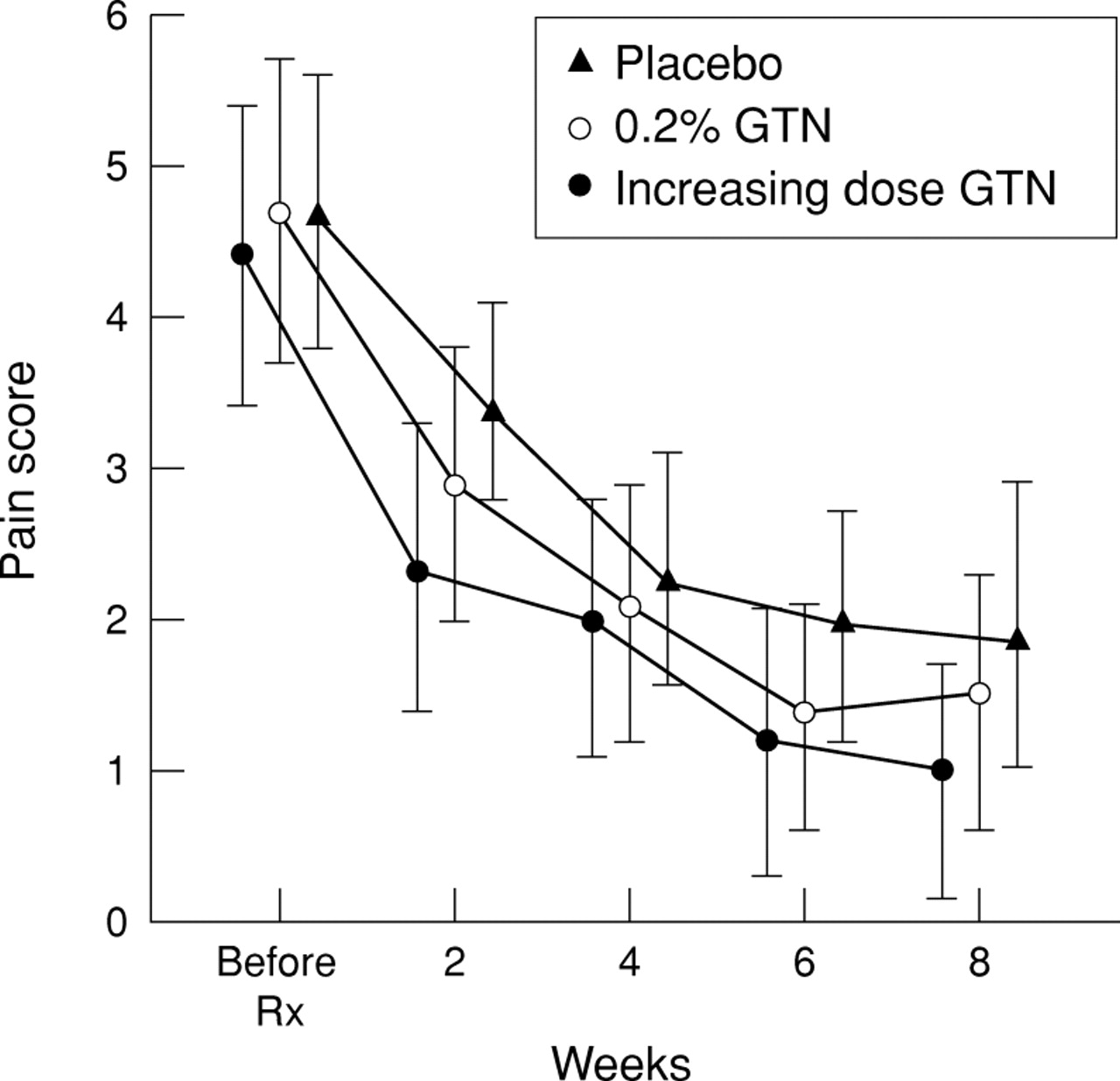
Mean (95% confidence interval) linear analogue pain scores prior to treatment and for subsequent two week periods of treatment between follow ups.
There was a reduction in the maximum resting pressure (MRP) from the pretreatment baseline to the final (week 8) sphincter pressure reading for all three treatment groups (fig 3). However, this change from baseline MRP was significantly (p=0.02, ANOVA) more pronounced after GTN (−32 (15) cmH2O, mean (SD) reduction in MRP) compared with placebo (−19 (19) cmH2O). No significant difference was seen in anodermal blood flow (fig 4) between the two GTN groups (p=0.2, ANOVA), or between placebo and the combined average of the two GTN groups (p=0.5, ANOVA).
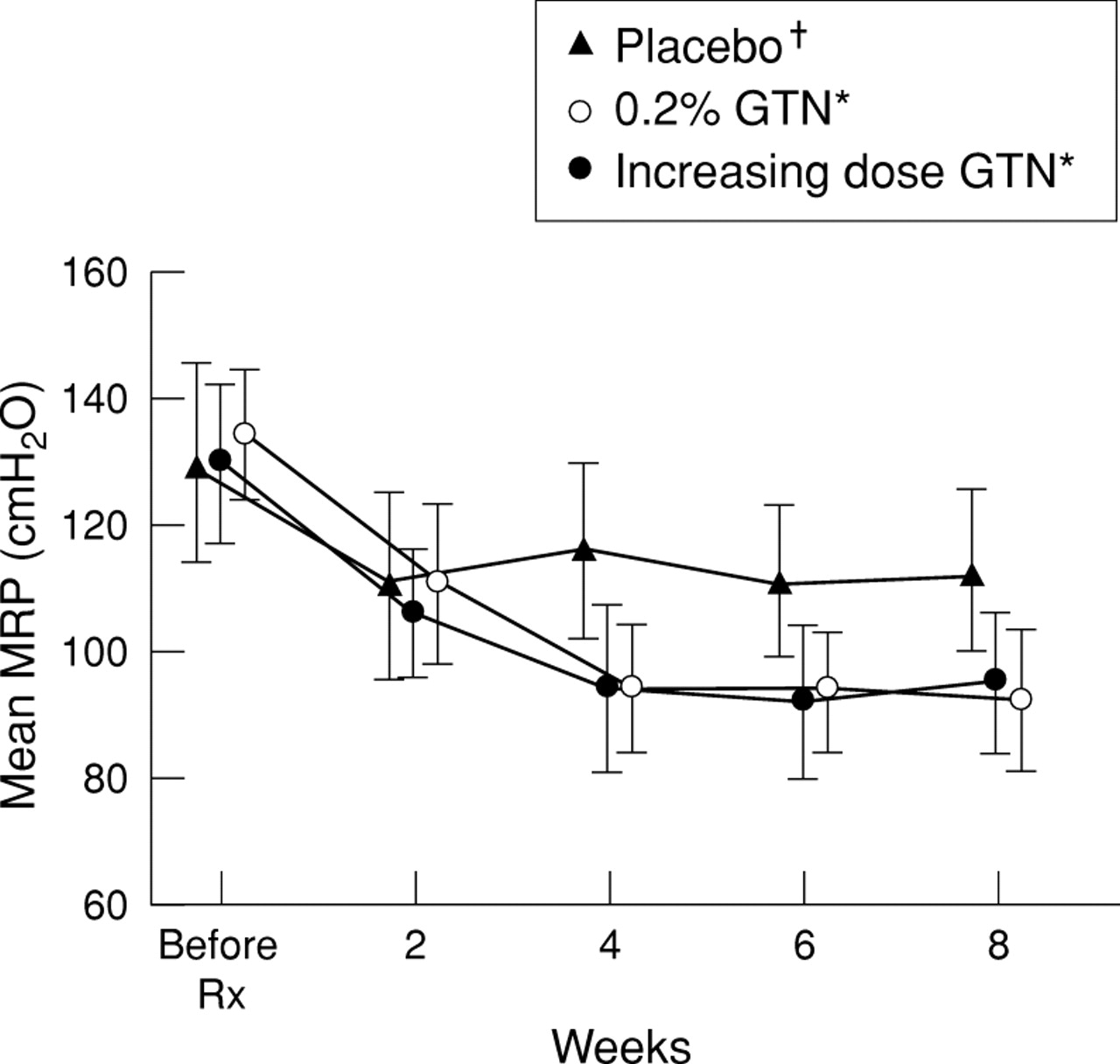
Mean (95% confidence interval) maximum resting pressure (MRP) before treatment and at each fortnightly follow up. *p=0.02, †p=0.8 change from baseline MRP (ANOVA) (placebo v GTN mean MRP: p=0.13; high dose v 0.2% GTN mean MRP: p=0.7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean (95% confidence interval) anodermal blood flow before treatment and after eight weeks.
None of the patients in this series complained of permanent loss of flatus or faecal continence, although overall 6/46 patients receiving GTN noted some temporary loss of flatus control while on treatment with topical GTN.
During the median follow up period of nine months (range 6–14 months), there were 3/7 (43%) symptomatic recurrences of fissure initially healed with placebo, compared with 5/15 (33%) recurrences after initial healing with 0.2% GTN, and 4/16 (25%) after high dose GTN (p=0.7, 0.2% versus escalating dose GTN, Fisher’s exact test).
Discussion
Pharmacological treatment using topical GTN has been shown to be effective for over two thirds of patients with chronic anal fissures.15 Our current study provides further evidence for this finding. It has also confirmed that healing is associated with a sustained reduction in maximum resting anal pressure. We observed a high rate of healing with placebo, consistent with previous reports16 ,17 but differing from the low placebo response rate in a recent study.15 It would seem that many fissures heal spontaneously or due to the continued application of topical ointment. However the extreme pain experienced with this condition demands an active approach to treatment.
This study found that increasing the dose of GTN resulted in faster healing, although the difference between the two doses of GTN did not reach statistical significance. At eight weeks the healing rates with the two different strengths of GTN were identical. An increasing dose of GTN may be useful if pain is extreme or poor compliance is anticipated. Doses of up to 0.6% were tolerated because of the gradual increase in dose.
The pain score fell to a similar degree for all three treatment arms in this study. It would seem that the application of topical ointment alone might reduce pain. In some patients pain decreased or resolved completely, despite the persistence of a fissure. Many of these patients did not want further treatment.
In contrast to previous studies,15-18 topical glyceryl trinitrate did not significantly increase anodermal blood flow. We can only assume that homoeostatic mechanisms responsible for regulation of cutaneous blood flow could have compensated for the vasodilatory effect of GTN.
The observed incidence of recurrent fissures represents one limitation of treatment. Even after a relatively short follow up period approximately one in three fissures recurred. Many of these recurrences were successfully treated with a further course of topical GTN (2/5 recurrences in the 0.2% GTN group and 2/4 recurrences in the high dose GTN group), with patient satisfaction. Topical treatment is ideal for those fissures which do not recur, or those patients who are happy to use repeated treatment. It is not as definitive as surgical treatment, although recurrent fissure can also occur after surgical treatment, and surgical treatment carries with it the risk of usually minor, but occasionally major, incontinence. The incidence of flatus incontinence after sphincterotomy varies between 2.4% and 36%7 ,8 ,19 ,20 and is higher still in some series. The important difference between this and any flatus incontinence experienced after GTN is the permanent or gradually worsening nature of symptoms with sphincterotomy compared with GTN where symptoms are temporary and resolve once treatment is discontinued. In addition, sphincterotomy is associated with faecal soiling in 2–21% of patients and incontinence to solid stool in 0.03–4.9% of patients.7 ,8 ,19 ,20 These more severe degrees of incontinence do not occur with GTN treatment.
The other main problem with topical GTN is the high incidence of headaches. The use of alternative topical agents such as diltiazem21 or bethanechol (unpublished data), which lower resting pressure may produce a solution to this problem.
In conclusion, topical GTN is an effective treatment for a majority of patients with anal fissure. An increasing dose schedule offers only a slight advantage in relation to speed of healing, and does not prevent later relapse. Higher dose preparations do not therefore seem to be indicated. Treatment for recurrence may be required in some patients.
Acknowledgments
We thank Caroline Dore for statistical advice, Claire Chadwick at the pharmacy department of St Mark’s Hospital for randomisation, and the pharmacy departments of Northwick Park and St Mark’s Hospitals for preparing the GTN ointments used in this study. E Carapeti is supported by the Robert Luff Foundation.
Abbreviations
- GTN
- glyceryl trinitrate
- MRP
- maximum resting anal pressure
- NO
- nitric oxide